")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 16
The Effectiveness of Chemical Cautery and Electrosurgery on Anogenital Wart: Systematic Review
Authors Mawardi P , Kamilah L , Fauziyyah Heryadi F, Arrosyid A
Received 10 July 2023
Accepted for publication 20 September 2023
Published 5 October 2023 Volume 2023:16 Pages 2773—2780
DOI https://doi.org/10.2147/CCID.S426851
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Prasetyadi Mawardi, Lian Kamilah, Fanny Fauziyyah Heryadi, Azhar Arrosyid
Department of Dermatology and Venereology, Faculty of Medicine, Sebelas Maret University/Dr Moewardi General Hospital, Surakarta, Indonesia
Correspondence: Prasetyadi Mawardi, Department of Dermatology and Venereology, Faculty of Medicine, Sebelas Maret University/Dr Moewardi General Hospital, Surakarta, Central Java, Indonesia, Tel +6281229750211, Email [email protected]
Introduction: Anogenital warts (AGW) is one of the sexually transmitted infections (STIs) caused by human papillomavirus (HPV). Treatment modalities of AGW yield low clearance and recurrence rate, so that chemical cautery with trichloroacetic acid (TCA) and electrosurgery are widely used to remove the lesions without any severe side effects.
Objective: To investigate the efficacy of chemical cautery with TCA and electrosurgery in AGW based on clinical trials or case series.
Methods: The systematic review was reported according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) but not registered to the International Prospective Register of Systematic Review (PROSPERO). To acquire proper and accurate information from relevant literature, two databases PubMed and the Cochrane Library were searched from January 2013 to March 2023.
Results: Thirteen studies were included in this systematic review, comprising seven articles on chemical cautery and six electrosurgery articles. The highest cure rate of chemical cautery with TCA was 94.1% while electrosurgery was 100%. A relatively low recurrence rate during 1 year follow-up was observed in electrosurgery with 14.6%, whereas the chemical cautery was 27.6%.
Conclusion: Electrosurgery for AGW treatment had higher cure rate with lower recurrence rate compared to chemical cautery with TCA. Numerous adverse effects of electrosurgery were reported include bleeding and scar formation as high risk of HPV infection.
Keywords: anogenital warts, chemical cautery, electro cautery, electrosurgery, trichloroacetic acid
Introduction
Anogenital warts (AGW) or condyloma acuminata, is one of the sexually transmitted infections (STIs) resulting from human papillomavirus (HPV) which manifest as fibroepithelial hyperplasia of skin or mucous membrane. Anogenital warts are a fairly common condition in sexually active adults with an annual incidence rate of 2%.1 Anogenital wart treatment aims to eradicate lesions and prevent their recurrence with minimal side effects. The therapeutic modality is classified into pharmacological such as chemical cautery with trichloroacetic acid (TCA) and non-pharmacological such as electrosurgical excision.2
The highly recommended therapy for AGW is chemical cautery by using TCA with a concentration of 70–100%. It is easy to apply with minimal side effects such as pain and burning sensation. Previous studies reported that chemical cautery using TCA was effective for superficial lesions with the cure rate ranging from 70% to 80% and recurrence rate was 36%.3 Another commonly used modality treat AGW is electrosurgery. It is effective for small warts on penis, vagina or rectal region, but big lesions must be avoided, as it may lead to a scar formation. A randomized controlled trial study stated that the cure rate of electrosurgery for AGW treatment was 94% at the sixth week.4 Appropriate management is required to the effectiveness and reduce the recurrence rate as well as side effects. Hence, we conducted this systematic review to compare the efficacy of chemical cautery using TCA to electrosurgery in AGW.
Methods
This systematic review was according to the Preferred Reporting Items for Systematic Review and Meta-Analysis (PRISMA) and no registered to the International Prospective Register of Systematic Review (PROSPERO).
Search Strategy
The search was conducted for studies assessing chemical cautery using TCA for AGW treatment from January 2013 to March 2023, with the following keywords: ((Anogenital warts) OR (Genital warts) OR (Condyloma acuminata) OR (Human papillomavirus) OR (HPV)) AND ((chemical cautery) OR (trichloroacetic acid) OR (TCA)) AND ((Therapy) OR (Treatment)), ((Anogenital warts) OR (Genital warts) OR (Condyloma acuminata) OR (Human papillomavirus) OR (HPV)) AND ((Electrosurgery) OR (Electrosurgical)) AND ((Therapy) OR (Treatment)) (Table 1). The investigators independently searched throughout several databases including PubMed and the Cochrane Library. Decisions were recorded through Microsoft Excel.
 |
Table 1 MeSH Terms Retrieved in Articles |
Study Eligibility Criteria
In terms of studies eligibility, we only included studies which met the inclusion criteria, namely (1) type of study (clinical trials, randomized control trial, case series); (2) study population (anogenital warts patients, age <18 years old and >18 years old); (3) intervention (chemical cautery, electrosurgery); and (4) outcomes (cure rate, recurrence rate, side effects). Meanwhile, the exclusion criteria were irretrievable full text and language other than English.
Data Extraction
A predetermined outcome sheet in Microsoft Excel was used to include the following data to be extracted: (1) author and year of publication; (2) study design; (3) study location; (4) time to follow-up; (5) study population (number of population, sex, mean age, number of lesions, and site of lesion); (6) intervention (type of intervention and duration); (7) outcome (cure rate and recurrence rate). Cure rate as the main outcome, was defined as lesions which were successfully eliminated or when the size of the wart reduced but did not disappear. Moreover, recurrence rate was defined by the presence of new warts after achieving complete response.
Results
Search Selection and Characteristics
Literature search flow details were described in Figure 1.5 A total of 982 articles were found upon initial search, removed 70 duplicates then screened and retrieved 913 articles. After being assessed for eligibility, 13 studies were included in this systematic review consisting of retrospective study (n=6), randomized control trial (n=5), and quasi-experimental (n=2). The most common retrospective study was conducted in 629 patients and total of 945 patients were included in this study (346 patients received chemical cautery using TCA and 598 patients treated with electrosurgery). The mean age of this subject was 34.27 years old. The duration of chemical cautery treatment range from 2 to 24 weeks.
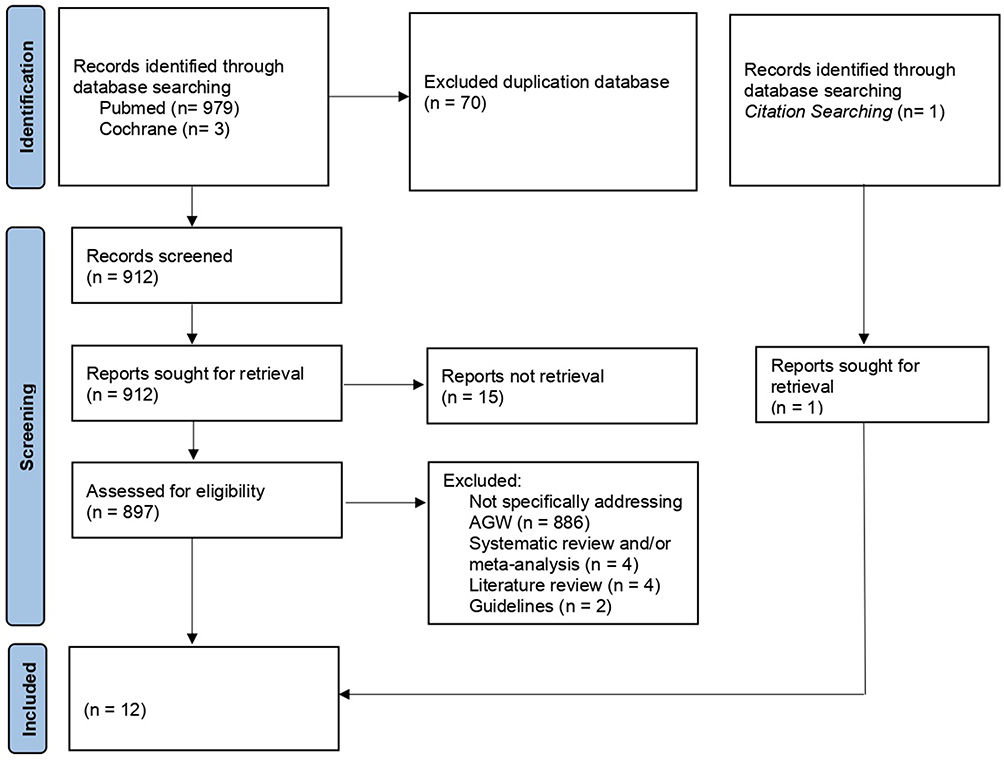 |
Figure 1 PRISMA chart. Adapted from Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. International Journal of surgery. 2021; 88: 105906. Creative Commons.5 |
Study Outcomes
The summary of the outcome of each study was listed in Table 2 and Table 3. The cure rate of chemical cautery of TCA varied ranging from 20% to 94.1% while the cure rate of electrosurgery was between 28% and 100%. The recurrence rate of chemical cautery and electrosurgery after 1-year follow-up was 27.6% and 14.6% respectively. Numerous adverse effects of electrosurgery were reported include bleeding and scar formation with the most common adverse effect was pain sensation. Meanwhile, the most common reported adverse effect of chemical cautery with TCA were pain and burning sensation.
 |
Table 2 Articles Addressing of Trichloroacetic Acid (TCA) |
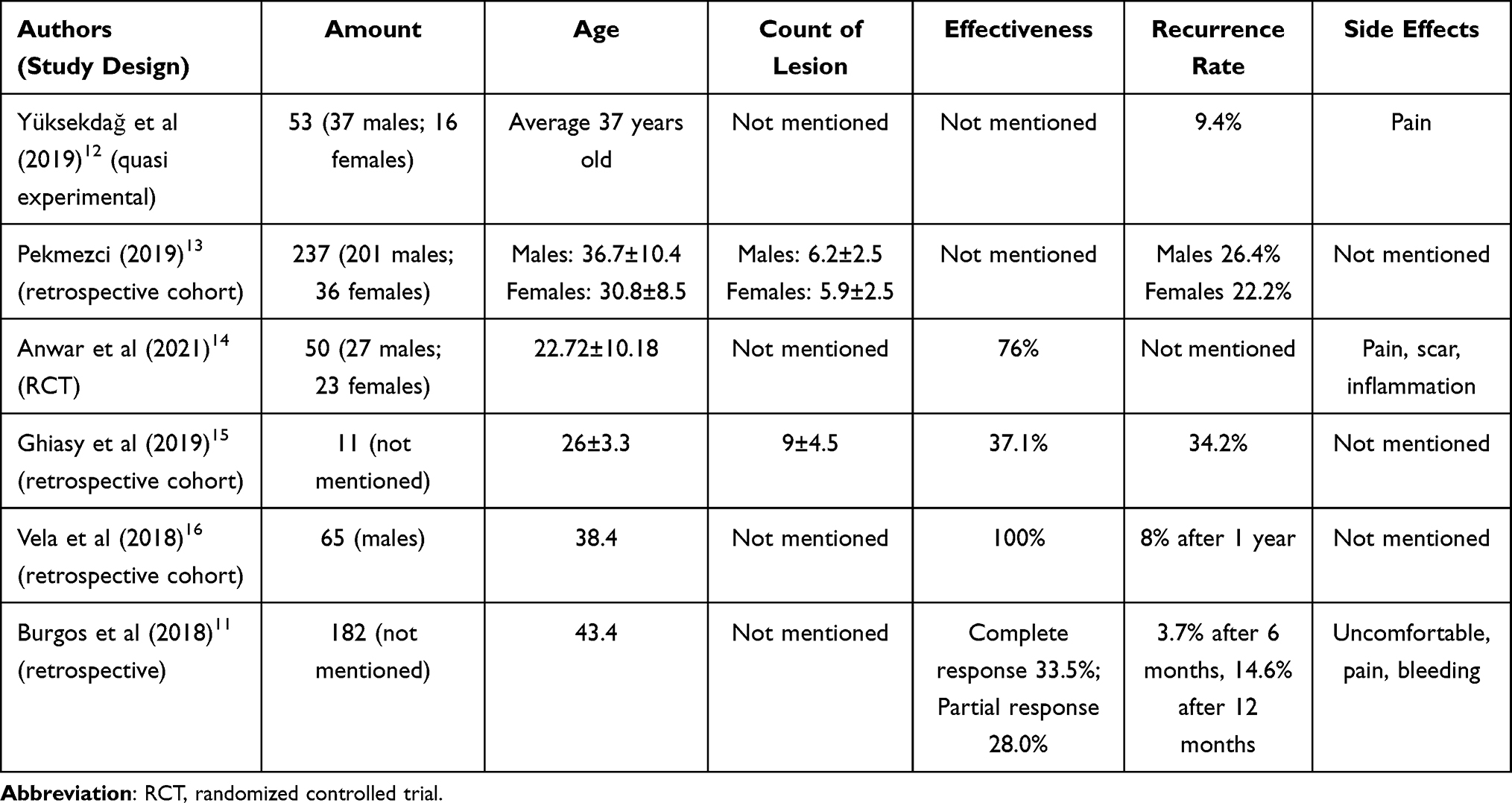 |
Table 3 Articles Addressing of Electrosurgery |
Discussion
The management of patients with AGW focuses on eliminating wart and precancerous lesions. The therapeutic modalities are topical therapy, systemic therapy, and destructive and surgical therapy.17 Topical therapy can be carried out by administering podophyllin, podophyllotoxin, 5-fluorouracil, imiquimod, and cidofovir.18 Podophyllin and podophyllotoxin is an antimitotic agent, 5-fluorouracil is DNA and RNA synthesis inhibitor, imiquimod is immunomodulator, and cidofovir is antiviral.19–24 Apart from topical therapy, AGW management can also be done with ablative techniques such as destructive therapy and surgery. Destructive and surgical therapy for HPV can be performed through trichloroacetic acid (TCA), cryotherapy, carbon dioxide (CO2) lasers, photodynamic therapy (PDT), and excision surgery.22,23 Destructive and surgical therapy have the same main mechanism of action, which is to induce tissue damage and thereby remove AGW lesions.25–27 Administering retinoids, cimetidine, interferon, or vaccines are systemic therapy for HPV.28 Retinoid is an antioxidative and keratolytic agent, cimetidine is an immunomodulator, interferon is an immunomodulator and could suppress cell proliferation, and vaccine is a prophylactic measure.29–31
Trichloroacetic acid acts as a cytotoxic agent causing coagulation of superficial tissue to cauterize damaged tissue.22,23 Trichloroacetic acid is one of the recommended clinic-based treatments. It is one of the chemical peels-based methods used in AGW management. It is usually used in high concentration preparations of 80–90%.32,33 For superficial skin lesions it may use pure TCA 10–30%, or in a combination form, such as TCA 15% combined with lactic acid 10%, or TCA 15% combined with salicylic acid (SA) 15% and lactic acid 15%. Trichloroacetic acid works by forming coagulation of epidermal proteins and keratinocytes.33 Higher concentrations of TCA solutions result in better clinical improvement.34 However, in this systematic review, it was discovered that a high level of effectiveness was not found to be associated with higher TCA concentrations or longer duration of therapy, whereas 70% TCA for 3 months had a greater effectiveness rate (94.1%) compared to that of TCA 100% with a duration of 6 months (82.2%). This effectiveness was also influenced by the number of lesions and the TCA application technique. Application technique is very important because the depth of penetration depends on the quantity of application. TCA is commonly used in several consecutive applications.13,33
Anogenital wart therapy using TCA commonly required several consecutive applications.35 Although it has a fairly high effectiveness, the recurrence rate in TCA therapy is also quite high, reaching 36%.36 In this systematic review, the recurrence rate ranged from 2.9% to 33%. These recurrence rates were time-dependent, in which, higher recurrence was found in a longer duration of follow-up time of 6 months, and higher TCA concentrations (100%). The recurrence rate at the same lesion site reached 61.1%.11 The study also discovered that the most common side effects of TCA were discomfort, burning sensation, pain and bleeding. These side effects relate to post-application peeling.33
Electrosurgery utilizes alternating current to produce different types of waveforms producing a combination of excision and coagulation that usually requires local anesthesia. Direct contact with skin causes coagulation and drying without carbonization (electrodesiccation), while air gaps (usually 1–3 mm) are used to cause rapid heating and carbonization of tissue (electrofulguration). The dry tissue that subsequently appears is removed by curettage.37 Another approach utilizes high-frequency alternating electric currents that pass through the lesions causing immediate tissue damage.38
The effectiveness rate of electrosurgery in AGW is very high, reaching 94–100%.32 This study obtained an effectiveness rate between 33.5% and 100%. The highest level of effectiveness was found in male subjects and mean age of 38.4 years. Among other therapeutic modalities for AGW, surgery is the most effective treatment to reduce the risk of recurrence after complete clearance.39 The electrosurgery was higher when compared to that of TCA in a 1-year follow-up period. The recurrence rate of electrosurgery in a 1-year follow-up period was 8%, while the TCA recurrence rate for the same follow-up period was 27.6%.
Electrosurgery has a higher effectiveness rate and lower recurrence rate compared to TCA. However, electrosurgery has more severe side effects when compared to TCA, in which bleeding predominantly occurs in electrosurgery. In addition, an RCT study reported that electrosurgery has a lower tolerance level when compared to TCA (79.4% vs 85.5%). Other benefits of using TCA are that it is easier and cheaper because it does not require local anesthesia or complicated technical equipment so that it can be performed on an outpatient basis, and TCA does not cause tissue evaporation which may increase the risk of HPV exposure for clinicians performing the procedure.40
Several factors have been correlated to AGW recurrence including the patient’s immune defense. The inability of the immune system to recognize an incoming or descending virus can be explained by the nature of the virus lifecycle. HPV infects basal cells and expresses of the early viral genes which are responsible for replication, transcription and stimulation of cell proliferation. In addition, the late gene that allows replication and encapsulation of viral DNA, and capsid structural proteins is expressed in the granular layer. During natural infection, viral antigens are not effectively presented to the immune system, nor can they be expressed at levels detectable by the immune system. This may lead to ineffective T cell activation leading to a lack of immunological ignorance and/or tolerance of virus-infected cells.41 Another study reported that patients with genitourinary infections are prone to AGW recurrence due to repeated stimulation of the skin and mucosa by various pathogens resulting in an increase of HPV colonization. The number of skin lesions are an independent influencing factor for AGW recurrence which causes declinine in the immune system to inhibit and eradicate HPV by T lymphocyte cells.42
Conclusion
In conclusion, electrosurgery has a better effectiveness as well as lower recurrence rate. However, electrosurgery can cause more serious side effects, has more complex applications and increases the risk of exposure to HPV for clinicians conducting the procedure.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Qayum A, Majid Paracha M, Sagheer F. Effectiveness of topical 100% trichloroacetic acid in treatment of anogenital warts in male patients. Fortune J Heal Sci. 2022;05(01):37–42.
2. Ball SLR, Winder DM, Vaughan K, Hanna N, Levy J, Sterling JC. Analyses of human papillomavirus genotypes and viral loads in anogenital warts. J Med Virol. 2011;83(8):1345–1350. doi:10.1002/jmv.22111
3. Khan A. Genital warts, etiology, signs, treatment and prevention. Am J Biomed Sci Res. 2019;5(4):307–308. doi:10.34297/AJBSR.2019.05.000934
4. Patel H, Wagner M, Singhal P, Kothari S. Systematic review of the incidence and prevalence of genital warts. BMC Infect Dis. 2013;13(1):39–42. doi:10.1186/1471-2334-13-39
5. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. Int J Surg. 2021; 88: 105906.
6. Asgari A, Taheri A, Babae A. A comparison of two treatment methods, trichloroacetic acid, and laser therapy, in the wart treatment: a randomized double-blind clinical trial in a University Hospital in Tehran, Iran. Ann Mil Heal Sci Res. 2023;20(4):5–9.
7. Recanati MA, Kramer KJ, Maggio JJ, Chao CR. Cantharidin is superior to trichloroacetic acid for the treatment of non-mucosal genital warts: a pilot randomized controlled trial. Clin Exp Obstet Gynecol. 2018;45(3):383–386. doi:10.12891/ceog4112.2018
8. Lotfabadi P, Yazdanpanah MJ. Liquid nitrogen cryotherapy versus 70 % trichloroacetic acid in the treatment of anogenital warts: a randomized controlled trial. Iranian J Dermatol. 2015;18(4):151–155.
9. Mawardi P, Febrianto B, Yuliarto D, Sumandjar T. Comparing the efficacy of chemical cautery to cryosurgery on CD4 + Status of HIV patients with condyloma acuminata. Clin Cosmet Investig Dermatol. 2021;14(1):1453–1458. doi:10.2147/CCID.S328667
10. Denise M, Silva S, Arruda D, Helena R, Crestana S, Aparecida C. Photodiagnosis and photodynamic therapy HPV-induced condylomata acuminata treated by photodynamic therapy in comparison with trichloroacetic acid: a randomized clinical trial. Photodiagnosis Photodynamic Therapy. 2021;35(1):4–9.
11. Burgos J, Martin-castillo M, Landol S, Dinares MC, Villar J, Navarro J. Effectiveness of trichloroacetic acid vs electrocautery ablation for the treatment of anal high-grade squamous intraepithelial lesion in HIV-infected patients. J Acquir Immune Defic Syndr. 2018;79(5):612–616. doi:10.1097/QAI.0000000000001847
12. Yüksekdağ S, Firat A, Unal E. The outcome of combined electro-fulguration and surgical excision techniques in the management of anogenital condylomas. Turk J Color Dis. 2019;29(1):188–192.
13. Pekmezci E. Higher lesion numbers result in higher recurrence rates: a retrospective cohort study in condylomata acuminata treated with electrocauterization. Georgian Med News. 2019;1(289):51–55.
14. Anwar A, Rafiq Z, Salam S. Comparison of efficacy of electrocautery vs cryotherapy in the treatment viral warts. J Fatima Jinnah Med Univ. 2021;15(1):177–180. doi:10.37018/PZCW5103
15. Ghiasy S, Fallah-karkan M, Razzaghi MR, Ranjbar A, Rahavian A. Is holmium laser an appropriate modality to treat. Laser Appl Med Sci Res Cent. 2019;10(1):70–74. doi:10.15171/jlms.2019.11
16. Vela S, Videla S, Ornelas A, Revollo B, Clotet B, Sirera G. Effectiveness of physically ablative and pharmacological treatments for anal condyloma in HIV-infected men. PLoS One. 2018;65(1):1–11.
17. Leszczyszyn J, Łebski I, Lysenko L, Hirnle L, Gerber H. Anal warts (condylomata acuminata) - current issues and treatment modalities. Adv Clin Exp Med. 2014;23(2):307. doi:10.17219/acem/37083
18. Johnson C, Goddard L, Jacob SE. Podophyllotoxin in dermatology. J Dermatol Nurses Assoc. 2018;10(1):53–56. doi:10.1097/JDN.0000000000000373
19. Blondy S, David V, Verdier M, Mathonnet M, Perraud A, Christou N. 5-Fluorouracil resistance mechanisms in colorectal cancer: from classical pathways to promising processes. Cancer Sci. 2020;111(9):3142–3154. doi:10.1111/cas.14532
20. Prince GT, Cameron MC, Fathi R, Alkousakis T. Topical 5-fluorouracil in dermatologic disease. Int J Dermatol. 2018;57(10):1259–1264. doi:10.1111/ijd.14106
21. Diamantis L, Barletts T. Safety, efficacy & recurrence rates of imiquimod cream 5% for treatment of anogenital warts. J Dermatology. 2009;14(5):1–7.
22. Rossi A, Cantisani C, Melis L, Iorio A, Scali E, Calvieri S. Imiquimod 5% cream use in dermatology, side effects and recent patents. Recent Pat Inflamm Allergy Drug Discov. 2012;6(5):130–136. doi:10.2174/187221312800166859
23. Nickles MA, Sergeyenko A, Bain M. Treatment of warts with topical cidofovir in a pediatric patient. Dermatol Online J. 2019;25(5):1–5. doi:10.5070/D3255044063
24. Byung H. Cidofovir intralesional injection for recalcitrant common warts: a comparison with sodium tetradecyl sulfate intralesional injection. Ann Dermatol. 2020;32(4):273–279. doi:10.5021/ad.2020.32.4.273
25. Sterling JC, Gibbs S, Haque Hussain SS, Mohd Mustapa MF, Handfield-Jones SE. British Association of Dermatologists’ guidelines for the management of cutaneous warts 2014. Br J Dermatol. 2014;171(4):696–712. doi:10.1111/bjd.13310
26. Mawardi P. Tatalaksana human papillomavirus. In: Listiawan MY, Indah J, Darmawan N, Muh E, editors. In: All About a Human Papillomavirus. First Edition.surakarta. UNS Press; 2022:71–83.
27. Wang HW, Zhang LL, Miao F, Lv T, Wang XL, Huang Z. Treatment of HPV infection- associated cervical condylomata acuminata with 5-aminolevulinic acid-mediated photodynamic therapy. Photochem Photobiol. 2012;88(3):565–569. doi:10.1111/j.1751-1097.2011.01060.x
28. Oren-Shabtai M, Snast I, Noyman Y, Lapidoth M, Sherman S, Mimouni D. Topical and systemic retinoids for the treatment of cutaneous viral warts: a systematic review and meta-analysis. Dermatol Ther. 2021;34(1):1–2. doi:10.1111/dth.14637
29. Jafarzadeh A, Nemati M, Khorramdelazad H, Hassan ZM. Immunomodulatory properties of cimetidine: its therapeutic potentials for treatment of immune-related diseases. Int Immunopharmacol. 2019;70(5):156–166. doi:10.1016/j.intimp.2019.02.026
30. Leung AKC, Barankin B, Leong KF, Hon KL. Penile warts: an update on their evaluation and management. Drugs Context. 2018;7(1):1–14. doi:10.7573/dic.212563
31. Scheinfeld N. Current update on the treatment of genital warts. Dermatol Online J. 2013;19(6):321–332. doi:10.5070/D3196018559
32. Gilson R, Nugent D, Werner RN, Ballesteros J, Ross J. 2019 European guideline for the management of anogenital warts in adults. Int J Med. 2019;1(1):1–20.
33. Small R, O’Hanlon K. Chemical Peels. In: Usatine RP, Pfenninger JL, Stulberg DL, editors. Small RBT-D and CP in OP. Philadelphia: W.B. Saunders; 2012:259–273.
34. Pezeshkpoor F, Banihashemi M, Yazdanpanah MJ, Yousefzadeh H, Sharghi M, Hoseinzadeh H. Comparative study of topical 80% trichloroacetic acid with 35% trichloroacetic acid in the treatment of the common wart. J Drugs Dermatol. 2012;11(11):66–69.
35. Godley MJ, Bradbeer CS, Gellan M, Thin RN. Cryotherapy compared with trichloroacetic acid in treating genital warts. Genitourin Med. 1987;63(6):390–392. doi:10.1136/sti.63.6.390
36. Abdullah AN, Walzman M, Wade A. Treatment of external genital warts comparing cryotherapy (liquid nitrogen) and trichloroacetic acid. Sex Transm Dis. 1993;20(6):344–345. doi:10.1097/00007435-199320060-00008
37. Thurgar E, Barton S, Karner C, Edwards SJ. Clinical effectiveness and cost-effectiveness of interventions for the treatment of anogenital warts: systematic review and economic evaluation. Health Technol Assess. 2016;20(24):1–486. doi:10.3310/hta20240
38. Grimnes S, Martinsen OG. Selected Applications. In: Grimnes S, editor. Martinsen ØGBT-B and BB Third E. Oxford: Academic Press; 2015:405–494.
39. Barton S, Wakefield V, Mahony O, Edwards C. Effectiveness of topical and ablative therapies in treatment of anogenital warts: a systematic review and network meta-analysis. BMJ Open. 2019;9(10):027765. doi:10.1136/bmjopen-2018-027765
40. Burgos J, Martin-Castillo M, Landolfi S, Dinares MC, Villar J, Navarro J. Brief report: effectiveness of trichloroacetic acid vs. electrocautery ablation for the treatment of anal high-grade squamous intraepithelial lesion in HIV-infected patients. J Acquir Immune Defic Syndr. 2018;79(5):612–616.
41. Zhan M, Tong Z, Chen S, Miao Y, Yang Y. Establishing a prediction model for recurrence of condyloma acuminatum. Eur J Med Res. 2022;27(1):1–9. doi:10.1186/s40001-022-00816-7
42. O’Brien PM, Campo M. Papillomaviruses: a correlation between immune evasion and oncogenicity? Trends Microbiol. 2003;11(7):300–305. doi:10.1016/S0966-842X(03)00145-8
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.