Back to Journals » Advances in Medical Education and Practice » Volume 13
The Effectiveness and Student Perceptions of Peer-Conducted Team-Based Learning Compared to Faculty-Led Teaching in Undergraduate Teaching
Authors Huilaja L, Bur E, Jokelainen J, Sinikumpu SP, Kulmala P
Received 14 January 2022
Accepted for publication 21 April 2022
Published 18 May 2022 Volume 2022:13 Pages 535—542
DOI https://doi.org/10.2147/AMEP.S358360
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Md Anwarul Azim Majumder
Laura Huilaja,1,* Eeva Bur,2,* Jari Jokelainen,3 Suvi-Päivikki Sinikumpu,1 Petri Kulmala2,4
1Department of Dermatology and Medical Research Center Oulu, PEDEGO Research Unit, University of Oulu and Oulu University Hospital, Oulu, Finland; 2Faculty of Medicine, University of Oulu, Oulu, Finland; 3Infrastructure for Population Studies, Faculty of Medicine, University of Oulu, Oulu, Finland; 4Department of Pediatrics and Medical Research Center Oulu, PEDEGO Research Unit, University of Oulu and Oulu University Hospital, Oulu, Finland
*These authors contributed equally to this work
Correspondence: Laura Huilaja, Email [email protected]
Background: Today’s professionals need to be capable of independent information retrieval, teamwork, and lifelong learning. To meet these demands, more active learning methods are needed in university teaching. Team-based learning (TBL) is a learner-centered method which enables activation of students in large classes.
Objective: The aim of this study was to compare a method combining peer teaching and TBL (peer-conducted TBL; pTBL) with faculty-led seminar teaching. More precisely, students’ opinions about teaching methods and immediate and long-term learning outcomes were aimed to compare.
Methods: A faculty-led design was compared to a pTBL design when teaching pediatric and dermatological allergy in a seminar setting for 5th year medical students. For that purpose, students were randomly split into two learning groups. In a faculty-led seminar (n = 44 students) the instructor first lectured on each subject; then, named students from each group were asked to present clinical cases given to them beforehand and them raising questions were answered. In a pTBL group (n = 50) student’s prior knowledge was first tested. Then, randomly selected, pre-prepared students took a tutors role in a seminar and presented clinical case to be solved in groups by all students. Students’ performance was equally tested after both sessions and 5– 6 months afterwards. Students’ opinions were asked by an electronic survey.
Results: In this study, pTBL was significantly preferred over faculty-led learning (mean grade 8.5 vs 6.5). Those participating in pTBL group studied pre-learning material more actively than those in faculty-led group. However, there was no difference in learning outcomes (immediate or long term) between the groups.
Conclusion: Students prefer teaching method in which they are self in active role. Combining TBL and peer teaching may further increase the accumulation of non-academic skills like expertise and proficiency.
Keywords: peer teaching, team-based learning, active learning
Introduction
The use of active learning methods have been increasing in health education in last decade1,2 and those have been used when teaching other disciplines as well.3–5 In these methods, the main role shifts from the teacher to the students to be more engaged in their learning.6 In addition, the importance of teamwork is increasing in working life, and it is evident that future professionals will need efficient team working skills as well.7
Team-based learning (TBL) is a structured, learner-centered activating learning method – in which learner is an active participant, not a subject – that can be used in larger or smaller classes.8,9 It utilizes the flipped classroom method and includes in-class testing of previous knowledge.9 TBL aims to give better tools for students to master and then apply information to solve real-life problems. It is also meant to guide students to interpret and evaluate data and think more critically. Working in teams is essential in TBL, and everyone must be engaged in the process; in TBL, students gain better tools to work as valuable members of a team.9,10 It has been shown that TBL increases student engagement,1 since in TBL, any member of the team can be randomly chosen to present the team’s answer.9,10 TBL has been shown to be an effective instructional technique, yielding better or equal academic performance compared to another instructional method.1
Peer teaching offers good opportunity to practice teaching and teamwork skills and commerce.11 In addition, it enables learners and teachers to be on a similar level educationally (=cognitive congruence), compared to faculty-led teaching.12 Peer teachers have familiarized themselves with the same material as peer learners and are thus able to express topics in a more understandable manner than faculty teachers who are not at the same social and educational standing as students. Recent meta-analysis showed that peer-assisted medical learning was especially efficient in teaching practical skills.13 Moreover, peer teaching has been reported to increase self-confidence among students and to create better learning environment and atmosphere in class.14
During the last decade, variable types of seminars have been more and more used as a form of instruction in medical education in Finnish universities instead of standard historical approach of teaching.15 Typically, seminars are mainly instructor-led and consist of short presentations prepared by groups of 5–12 students on the subject given. In addition to that, invited experts and the instructor of the seminar deliver their lectures on the subject. This design makes most students passive listeners and can increase the number of free-riders among the students. A faculty-led seminar day does not require every student to be prepared or motivate them to internalize the information given, and immediate reflecting is often lacking as well. Therefore, the achieved individual learning is likely to be superficial. Students have expressed their dissatisfaction and doubt towards seminars and the benefit obtained from them compared to traditional lectures, due to the large group size (there are approximately 100–150 students per class in Finnish medical schools) in both of these methods.15
Since more activating learning methods have been widely introduced in medical teaching, and peer teaching is also known to have a positive effect on the learning environment,12 our aim was to design a modified, peer-conducted TBL-based seminar setting (pTBL). This setting was applied in teaching of pediatric and dermatological allergology for fifth-year undergraduate medical students, and learning outcomes and students perceptions were compared to a faculty-led seminar design.
Materials and Methods
The Design of the Study and Arrangements of Instruction
Pediatrics and dermatology are designed as part of the 5th academic year curriculum at the University of Oulu, Finland. In the beginning of the academic year, all fifth-year medical students are split into two learning groups. One group attends the 10-week course on pediatrics during the fall semester and the other during the spring semester. The course on dermatology and allergology is taught for the entire group of fifth-year students in between. Seminars on a variety of subjects have been among the teaching methods used in both courses, including one combined seminar on pediatric and dermatological allergology for the students of the entire academic year. For the present study, during the academic year 2015–2016, this allergology instruction was first carried out as a faculty-led seminar design for one-half of the 5th academic year students (n = 44), and then as a modified, peer-conducted-TBL (pTBL) design for the other half of the students (n = 50). Equal time on task was used in both designs. Both seminars were supervised by the same two instructors (LH and PK; both had previous experience on implementing TBL in medical education). Both groups had received similar education in previous four years of medical studies (including 1–2 small group instructions conducted with TBL method).
For the advance assignment, all students received identical material to study and prepare themselves for the seminar. Learning objectives were defined and provided for all students to help them to focus on relevant issues while studying.
The Protocol of Faculty-Led Seminar
In the faculty-led design, the fourty-four students were split into groups (Figure 1). The groups prepared a short digital presentation of a clinical patient case (clinical history, diagnosis, treatment and follow-up) in advance, with clinical details provided to them by the instructors. During the seminar day, the instructor first lectured briefly on each subject; then, named students from each group were asked to give their presentations. The other students listened to the presentations and the instructors answered any questions that arose.
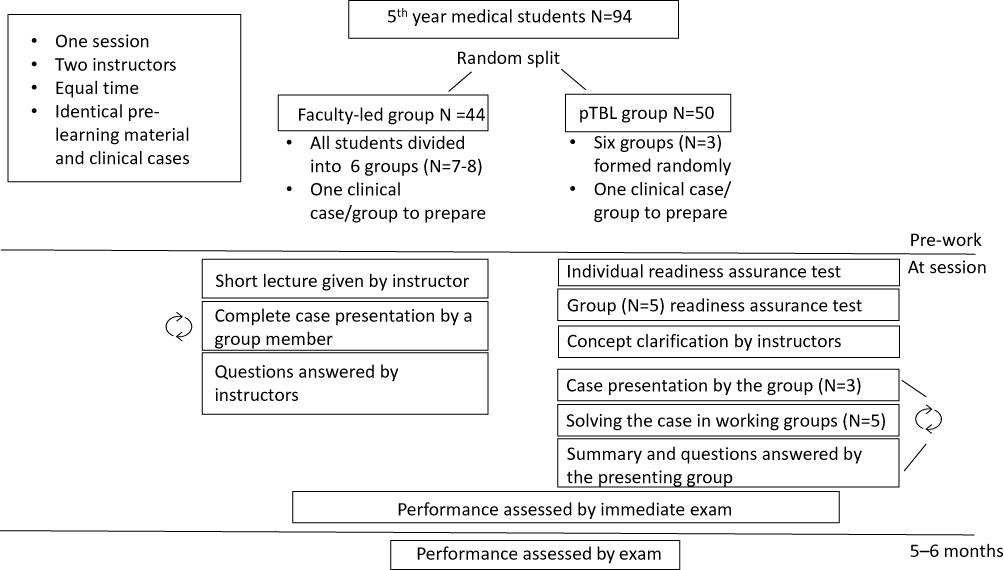 |
Figure 1 Study groups and arrangement of the instruction in faculty-led and peer-conducted team based learning (pTBL). |

The Protocol of pTBL Seminar
In the pTBL design, in line with the TBL method,9 the seminar day began with a test based on the advance material. The test was first done as individuals and then in groups. After completion of the test, relevant concepts and questions were clarified by the instructors. Before the seminar, six groups of three students had been randomly selected to prepare a short digital presentation of a clinical patient case in advance (Figure 1). The cases were the same as in the seminar carried out using faculty-led design, although presented in a manner enabling problem-solving and thus ie, diagnose was not provided. Furthermore, these case-presenting students were instructed to prepare themselves to be able to act as experts during the case presentation. The presenting expert students instructed the other students to solve the case in their teams (five students in each team). The working teams had all medical information sources available on their laptop computers, tablets and cell phones. The aim was to find a well-founded answer for each multiple-choice question provided by the presenting group in all teams in a time-limited manner. Simultaneous answers for each question were required from each team. Individual students were randomly picked from the audience to present and argue their team’s answer. Thereafter, the presenting expert group showed the right answer to the case including the examinations needed, diagnosis and treatment. Finally, the expert group presented a short summary on the clinical subject of their case based on the learning outcomes of the seminar. The role of the expert students included answering all the questions from the working audience, further emphasizing and imitating the role of a medical expert in real-life situations. If they could not answer the questions correctly, they consulted the instructors (LH and PK). The other role of the instructors was to oversee the fluent flow and schedule of the seminar and to bear responsibility for the correct content of the seminar.
Learning Outcomes and the Students’ Perceptions
In both seminars, the students took an exam at the end of the day to test what they had learned. In addition, to test assimilation and long-term learning, the students had another multiple-choice test 5–6 months after the seminar day. Since the second test was carried out as part of the fifth-year final exam at the end of the spring semester, it was not possible to run the test in its entirety, but the questions asked were chosen among the ones used in the first test.
After the seminar, all the participating students were asked to answer an online survey regarding the teaching method used in the seminar (Table 1). Those participating in the first faculty-led design received the link for the questionnaire right after the seminar. Unfortunately, the delivery of the link to the questionnaire to those participating in the pTBL design was delayed for two months before a technical problem on the delivery of the link was discovered.
 |
Table 1 Participants’ Opinions Regarding the Teaching Method |
Statistical Methods
Results are given as proportions and means. Chi-Square test was used to analyze the difference in students’ opinions and gender balance (Table 1) and students’ t-test was used to compare the test performance between the groups (Table 2). P-value <0.05 was considered statistically significant.
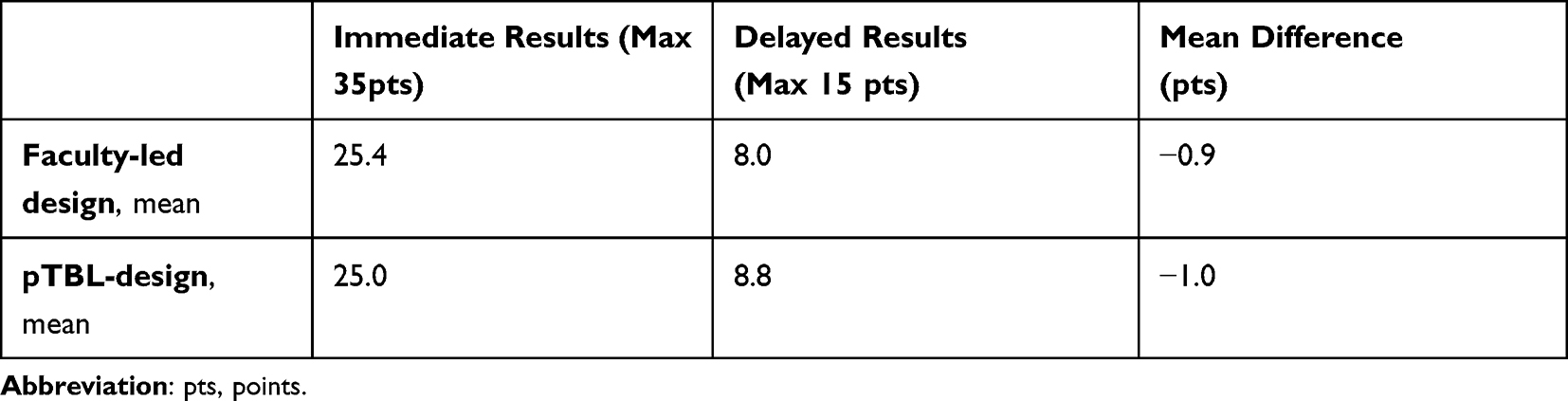 |
Table 2 Students’ Performance in Exams Related to the Topic Covered in the Seminar |
Results
Previous Experience of Methods Used and Overall Grade
Students’ perceptions survey was answered by 98–100% (N = 43–44/44) in the faculty-led group and 58–62% (N = 29–31) in pTBL group (Table 1). Almost all students in the faculty-led group (n = 42/44) reported that they had previously participated in instruction conducted in the same way. One third (n = 10/31) of the students in the pTBL group reported they had no previous experience of TBL design in seminar setting. The overall grade for the seminar day was significantly higher in the pTBL group than in the group taught with faculty-led design (p < 0.001): In the pTBL group, the mean grade (range 1–10) was 8.5 (SD = 0.8; range 7–10) and in the faculty-led group, 6.5 (SD = 1.8; range 2–9).
The results in the faculty-led group were divided, but half (n=22/44; 50.0%) of the students thought the seminar day was at least “somewhat better” than just lecturing. In the pTBL group, none thought that the faculty-led lecturing method would have been better. Majority of students (n=21/31; 67.7%) in the pTBL group answered that pTBL was a “significantly better” method than the faculty-led seminar design (Figure 2). In students’ opinion, the pTBL method made it more difficult to free-ride compared to the faculty-led group (Table 1).
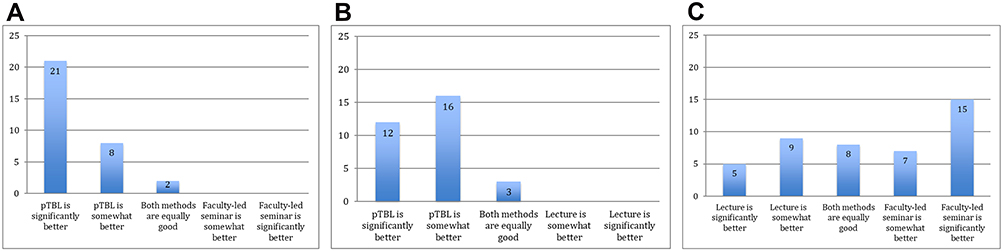 |
Figure 2 Comparison of different teaching methods based on students’ opinions. (A) pTBL compared to faculty-lead seminar and (B) pTBL compared to lectures by those participated to peer-conducted team-based learning (pTBL) (n=31) (C) Faculty-led seminar compared to lectures by those participated to faculty-led seminar (n=44). |
Advance Material
In the pTBL group, more students (n = 27/31; 87.1%) studied the advance material either “thoroughly” or “a little” than in the faculty-led design (n=29/44; 65.9%). In both groups, majority of the students thought that the extent of the advance material was adequate and that it was useful. There was no statistically significant difference between the groups in thoughts about usefulness of the material (useful vs not useful, p = 0.054). However, most students (n = 20/31; 64.5% in pTBL-design and n = 21/44; 47.7% in faculty-led design, respectively) reported that studying the advance material was somewhat arduous (Table 1).
Learning Process and Learning Outcomes
In the pTBL group, almost all (93.5%) of the students answered that the method helped their learning whereas fewer students (74.4%) in the faculty-led group thought so (Table 1). However, this difference did not reach statistical significance (p = 0.084). Students’ learning was assessed by an identical multiple-choice exam after both seminar days. Mean scores did not differ between these groups (25.4/35 in faculty-led group vs 25.0/35 in pTBL, p = 0.51). To study more permanent learning results, some of the questions were repeated after 5–6 months and these results were compared to the results of the first exam. Students from both groups got equally lower scores in the latter exam (mean difference −0.9 in faculty-led group vs −1.0 in pTBL group, p = 0.86) (Table 2).
Discussion
TBL can flip the teaching design so that it takes better advantage of students’ own potential and knowledge.9 To give students even more responsibility in the learning process and to gain advantage of peer-teaching,12 we designed a modified TBL-method (pTBL) in which peers served as teachers.
In our study we found that the pTBL method was significantly preferred (mean grade 8.45 vs.6.52) as an instruction method among fifth-year medical students over faculty-led learning when studying pediatric and dermatological allergology. This is in line with recent systematic review reporting that learners prefer TBL over other, often more traditional forms of instruction.1 A Turkish study described that a majority of fifth-year medical students felt that the TBL method helped them meet the learning objectives better and gave them a better understanding on the subject.16 However, there are some studies that have reported neutral or diminished preference of TBL over lectures.1 Previously, Fatmi et al17 described mixed learner reactions towards TBL, possibly due to the increased student workload during pre-class preparation. However, in our study most of the students found the volume of the advance material suitable and felt that studying it was not very demanding. We admit that we cannot exclude the possibility of the “novelty effect” of preferred pTBL: during the time this study was performed, TBL was used only in 1–2 instruction sessions in our faculty and “novelty effect” has been reported to be particularly influential in experiments involving one or only few sessions as in our study.18 However, it is of note that albeit “novelty effect” is generally considered to be favorable for a new method, too much novelty can hamper learning so “novelty effect” is not unambiguous.18,19
As a method, TBL promotes active learning opportunities and engages participants, thus promoting deeper understanding and better knowledge retention.9 To assess the learning outcomes between the faculty-led and pTBL-design two separate tests were performed for both groups. Nevertheless, we did not find any difference between the groups in the test results, either immediately after the teaching or when recalling after 5–6 months. This is in line with a meta-analysis reporting that outcomes of students taught by peers do not differ from those taught by faculty.20 However, we speculate that our multiple-choice questions were not the best possible way to monitor in-depth learning, and this may have concealed the differences. Maybe a mixed-method approach with more qualitative analysis would have led to different outcomes. Since the TBL method has given better results, especially in those who have previously scored lower points in exams,21,22 it would have been beneficial to compare students’ scores to their overall performance. Unfortunately, this was not possible due to the university’s regulations. However, it is of note that despite our finding that pTBL did not enhance students’ performance, majority of the students preferred pTBL learning compared to the faculty-led seminars they had previously attended. However, there was no statistically significant difference between the groups in their perceptions about the method’s benefits to their learning. Most probably this is due to the small group size in our study. Thus, TBL seems to foster a positive attitude towards learning, which, in turn, is essential to achieve the principle of life-long learning.23
For today’s professionals, it is not enough to just adopt information; there is also a high demand for managing good intercourse skills.24 As an instruction method, TBL offers a possibility to learn a variety of general skills besides the exact concepts taught. TBL potentially supports students’ team-working and communication skills. In addition, it enhances problem-solving skills and capability to resolve conflicts. Peer teaching, in turn, has been shown to increase teaching and intercommunication skills.11 Therefore, combining these two methods would likely amplify learning of these essential skills in medical education as shown in recent meta-analysis.13 Although all these skills are crucial in real-world settings, they are not usually measured or evaluated while analyzing TBL as an instruction method.1,9 To properly study the accumulation of these skills, a more longitudinal setting than ours is needed.
There are several strengths in our study. Firstly, both study groups had gone through similar curricula so the groups have no significant background differences and were balanced by gender. However, due to this we were unable to analyze the effect of methods used during prior curricula, which may have diminished our findings.25 Secondly, all students participated to both tests measuring learning outcomes. Unfortunately, most probably due to the delayed delivery, not all in pTBL group answered the questionnaire about students’ perceptions leading to lower response rate in pTBL group compared to faculty led group. Better response rate may have led to different findings if only those students who were most active and thus liked pTBL answered to our questionnaire.
In conclusion, students considered pTBL as a feasible learning method. pTBL increased students’pre-learning, but led to similar learning outcomes compared to the faculty-led seminar. Based on our study, the advantages of peer teaching can be successfully combined with the TBL-method, letting students work as experts in the TBL design. TBL increases both knowledge and skills beyond testing. The outcomes in pTBL equal to those in faculty-led teaching, and in addition peer-teaching involves students even more, which may further broaden the skills achieved. Thus, pTBL is a good variation of TBL to be implemented in higher education. New studies with more extensive setting (ie, whole course instead of one instruction) and longer follow-up are needed to fully understand the effects of pTBL teaching in higher education.
Abbreviations
TBL, team-based learning; pTBL, peer-conducted team-based learning; SD, standard deviation.
Acknowledgments
Mr Risto Bloigu’s expert help with the statistical analysis is gratefully acknowledged.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Reimschisel T, Herring AL, Huang J, Minor TJ. A systematic review of the published literature on team-based learning in health professions education. Med Teach. 2017;39(12):1227–1237. doi:10.1080/0142159X.2017.1340636
2. Alberti S, Motta P, Ferri P, Bonetti L. The effectiveness of team-based learning in nursing education: a systematic review. Nurse Educ Today. 2021;97:104721. doi:10.1016/j.nedt.2020.104721
3. Castro LF, Peuker S, Mott J. Application of team‐based learning for teaching food analysis. J Food Sci Educ. 2021;20(2):78–87. doi:10.1111/1541-4329.12223
4. Alamoudi AA, Al Shawwa LA, Gad H, Tekian A. Team-based learning versus traditional didactic lectures in teaching clinical biochemistry at king abdulaziz university; learning outcomes and student satisfaction. Biochem Mol Biol Educ. 2021;49(4):546–559. doi:10.1002/bmb.21501
5. Simkins SP, Maier MH, Ruder P. Team-based learning (TBL): putting learning sciences research to work in the economics classroom. J Econ Educ. 2021;1:1–10.
6. Hrynchak P, Batty H. The educational theory basis of team-based learning. Med Teach. 2012;34(10):796–801. doi:10.3109/0142159X.2012.687120
7. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. Lancet. 2010;376(9756):1923–1958. doi:10.1016/S0140-6736(10)61854-5
8. Parmelee DX, Hudes P. Team-based learning: a relevant strategy in health professionals’ education. Med Teach. 2012;34(5):411–413. doi:10.3109/0142159X.2012.643267
9. Burgess A, van Diggele C, Roberts C, Mellis C. Team-based learning: design, facilitation and participation. BMC Med Educ. 2020;20(Suppl 2):461–y. doi:10.1186/s12909-020-02287-y
10. Parmelee D, Michaelsen LK, Cook S, Hudes PD. Team-based learning: a practical guide: AMEE guide no. 65. Med Teach. 2012;34(5):275. doi:10.3109/0142159X.2012.651179
11. General Medical Council (Great Britain). Good Medical Practice. General Medical Council London; 2013.
12. Lockspeiser TM, O’Sullivan P, Teherani A, Muller J. Understanding the experience of being taught by peers: the value of social and cognitive congruence. Adv Health Sci Educ Theory Pract. 2008;13(3):361–372. doi:10.1007/s10459-006-9049-8
13. Brierley C, Ellis L, Reid ER. Peer-assisted learning in medical education: a systematic review and meta-analysis. Med Educ. 2021;56(4):365–373. doi:10.1111/medu.14672
14. Kassab S, Abu-Hijleh MF, Al-Shboul Q, Hamdy H. Student-led tutorials in problem-based learning: educational outcomes and students’ perceptions. Med Teach. 2005;27(6):521–526. doi:10.1080/01421590500156186
15. Mäkelä M, Möller R, Stphens C, et al. Educating Doctors for the Future – Evaluation of Undergraduate Medical Education in Finland. Finnish Education Evaluation Centre; 2018:1–112.
16. Altintas L, Altintas O, Caglar Y. Modified use of team-based learning in an ophthalmology course for fifth-year medical students. Adv Physiol Educ. 2014;38(1):46–48. doi:10.1152/advan.00129.2013
17. Fatmi M, Hartling L, Hillier T, Campbell S, Oswald AE. The effectiveness of team-based learning on learning outcomes in health professions education: BEME guide no. 30. Med Teach. 2013;35(12):1608. doi:10.3109/0142159X.2013.849802
18. Tsay CH, Kofinas AK, Trivedi SK, Yang Y. Overcoming the novelty effect in online gamified learning systems: an empirical evaluation of student engagement and performance. J Comput Assist Learn. 2020;36(2):128–146. doi:10.1111/jcal.12385
19. Boeve-de Pauw J, Van Hoof J, Van Petegem P. Effective field trips in nature: the interplay between novelty and learning. J Biol Educ. 2019;53(1):21–33. doi:10.1080/00219266.2017.1418760
20. Rees EL, Quinn PJ, Davies B, Fotheringham V. How does peer teaching compare to faculty teaching? A systematic review and meta-analysis. Med Teach. 2016;38(8):829–837. doi:10.3109/0142159X.2015.1112888
21. Tan NC, Kandiah N, Chan YH, Umapathi T, Lee SH, Tan K. A controlled study of team-based learning for undergraduate clinical neurology education. BMC Med Educ. 2011;11(1):91. doi:10.1186/1472-6920-11-91
22. Punja D, Kalludi SN, Pai KM, Rao RK, Dhar M. Team-based learning as a teaching strategy for first-year medical students. Australas Med J. 2014;7(12):490–499. doi:10.4066/AMJ.2014.2244
23. Inuwa IM. Perceptions and attitudes of first-year medical students on a modified team-based learning (TBL) strategy in anatomy. Sultan Qaboos Univ Med J. 2012;12(3):336–343. doi:10.12816/0003148
24. Kääpä P, Hoffren J. Generic competences in medical undergraduate education. Duodecim. 2010;126(14):1720–1729.
25. Frame TR, Cailor SM, Gryka RJ, Chen AM, Kiersma ME, Sheppard L. Student perceptions of team-based learning vs traditional lecture-based learning. Am J Pharm Educ. 2015;79(4):51. doi:10.5688/ajpe79451
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.