")
Back to Journals » Clinical Interventions in Aging » Volume 18
The Effect of Tele-Savvy on Sleep Quality and Insomnia in Caregivers of Persons Living with Dementia
Authors Brewster GS , Higgins M, McPhillips MV, Bonds Johnson K, Epps F, Yeager KA, Bliwise DL, Hepburn K
Received 13 June 2023
Accepted for publication 1 December 2023
Published 14 December 2023 Volume 2023:18 Pages 2117—2127
DOI https://doi.org/10.2147/CIA.S425741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Glenna S Brewster,1 Melinda Higgins,1 Miranda Varrasse McPhillips,2 Kalisha Bonds Johnson,1 Fayron Epps,1 Katherine A Yeager,1 Donald L Bliwise,3 Kenneth Hepburn1
1Nell Hodgson Woodruff School of Nursing, Emory University, Atlanta, GA, USA; 2University of Pennsylvania, School of Nursing, Philadelphia, PA, USA; 3Division of Sleep Medicine, Emory University School of Medicine, Atlanta, GA, USA
Correspondence: Glenna S Brewster, 1520 Clifton Road, NE, Atlanta, GA, 30322-4027, USA, Tel +1 404.712.9164, Email [email protected]
Introduction: Sleep disturbance is prevalent in caregivers of persons living with dementia (PLwD). Tele-Savvy, a 7-week virtual psychoeducational intervention, enhances caregivers’ competence and self-care, and reduces depression. While not explicitly designed to do so, Tele-Savvy can potentially improve caregivers’ disturbed sleep. The present study aimed to examine the longitudinal effects of Tele-Savvy on caregivers’ sleep quality and insomnia.
Methods: This was a secondary data analysis of a 3-arm randomized control trial [Tele-Savvy (active treatment), Healthy Living (attention control), and usual care (waitlist control)]. Multilevel mixed modeling with intent-to-treat principles tested for group, time, and group-by-time effects. Effect sizes were estimated for all changes from baseline to the initial 6-month post-intervention point. Following completion of the 6-month post-randomization delay, we examined combined outcomes for Tele-Savvy.
Results: Participants (n=137; mean age 64.7 years) were predominantly female (68.6%) and White (68.6%). We found no initial group-by-time effects for the Pittsburgh Sleep Quality Index (PSQI) and the Insomnia Severity Index (ISI). For the combined Tele-Savvy group, there was a statistically significant improvement in ISI scores across time (p=0.050). The combined Tele-Savvy effect size for PSQI was d=0.126 and ISI was d=0.310.
Discussion: Tele-Savvy resulted in a significant long-term reduction in insomnia symptoms in this sample of caregivers of PLwD and demonstrated a positive trend for improvement in their sleep quality. Since sleep disturbance is so prevalent among caregivers of PLwD, the inclusion of sleep health education into psychoeducation caregiver interventions may yield even better outcomes for caregivers.
Plain Language Summary: Many caregivers of persons living with dementia have poor sleep. Tele-Savvy is a 7-week intervention that was delivered online to caregivers improved their caregiving skills and self-care and reduced their depressive symptoms; thus, Tele-Savvy may possibly improve their sleep problems. This study aimed to examine the effects of Tele-Savvy on caregivers’ sleep quality and insomnia over 6 months. Caregivers were randomly assigned to Tele-Savvy (intervention), Healthy Living (comparison intervention), and usual care (no initial intervention). One hundred and thirty-seven caregivers, predominantly female, who were on average 64.7 years, participated in this study and completed measures of insomnia and sleep quality. Insomnia symptoms improved and there was a positive trend for improved sleep quality across time for caregivers who received Tele-Savvy. Since so many caregivers have sleep problems, including sleep health education as a part of other caregiver interventions may lead to even better outcomes for caregivers.
Keywords: psychoeducational intervention, Alzheimer’s disease, circadian rhythm, cognitive behavioral therapy for insomnia, depression
Introduction
Of the more than 16 million caregivers/care partners of persons living with dementia (PLwD),1 92% report some type of sleep disturbance.2–4 Sleep disturbances include prolonged sleep latency, frequent nighttime awakenings often with difficulty falling back asleep, inconsistent sleep and wake times, changes in rapid eye movement and non-rapid eye movement sleep, short sleep duration, and poor sleep quality.5–7 Compared to age-matched non-caregivers, caregivers get approximately two and a half fewer hours of sleep each week—less than the recommended minimum daily sleep duration of 7 hr.8 For caregivers, poor sleep is generally associated with hypertension,9 obesity,10 type-2 diabetes,10 and neurodegeneration.11 Poor sleep is also associated with greater depressive symptoms12,13 and care burden,14,15 poorer quality of life,14 and increased inflammatory blood biomarkers.16,17 Since sleep disruption can be devastating for caregivers,18,19 they need interventions to address their sleep disturbance.
Despite the high prevalence of sleep disturbances in PLwD caregivers, few sleep-focused interventions exist for this group. In a recent meta-analysis, Gao, Chapagain, and Scullin8 reported on 13 interventions noting their impact on sleep duration and sleep quality. They found that behavioral interventions, such as sleep hygiene education, stimulus control, and light chronotherapy, were associated with better post-intervention sleep quality. At the same time, numerous psychoeducational interventions not explicitly focusing on sleep have been developed for and tested with caregivers.
One psychoeducational intervention is the well-established Savvy Caregiver program (SCP).20,21 Social cognitive theory22,23 and stress process24,25 model which recognize that the stress that often accompanies caregiving and threatens caregiver health have guided the development of SCP. Savvy Caregiver Program is delivered in-person by trained facilitators over 6 weeks in 2-hr group sessions. The SCP curriculum proposes that caregiving plays a clinical role that requires specific skills and knowledge. SCP teaches caregivers how to assess the capacities of the PLwD they are caring for, determine what assistance will be effective, and apply the proper support to maintain their emotional well-being, and self-care strategies. Specific topics in SCP include staging dementia, tailoring tasks and activities to fit with dementia stages, identifying community resources, and caregiver self-care. Some self-care activities include how to use techniques like yoga, meditation, and breathing exercises. The program increased caregiver mastery and promoted successful caregiving and self-care behaviors using instruction, practice, coaching, and debriefing techniques.20 SCP was adapted to be fully online as Tele-Savvy. Tele-Savvy increased caregivers’ competence, decreased their perceived stress and depressive symptoms, and improved caregiver wellbeing.26,27
Tele-Savvy may still have considerable relevance for sleep disturbance in PLwD as it reduced caregiver stress and depressive symptoms and improved caregiver self-care.26,28–32 Since stress and depressive symptoms are associated with poor sleep outcomes.4,31,33–37and acts of self-care such as meditation and relaxation are related to having better sleep,38–40 it is feasible to posit that a reduction in stress and depressive symptoms with enhanced self-care may improve sleep. In this paper, we examine the effect of Tele-Savvy on caregivers’ sleep quality and insomnia symptoms.
Methods
Design
This was a secondary data analysis of a randomized, controlled trial with three groups:
- Tele-Savvy (active intervention). Tele-Savvy consists of seven weekly, 75–90-min group videoconferences, and daily brief email-delivered “video lessons”.26 Group meetings allowed for the discussion of activities that were attempted during the preceding week with an emphasis on successes and challenges, introduction of new material, and guided discussions. An email was sent to caregivers with a link to a daily video lesson that was housed in Canvas.41 The content of the video lessons focused and expanded on the weekly topics. Caregivers could watch and re‐watch videos at their convenience. Caregivers also received a manual and a workbook.
- Healthy Living (attention control). Caregivers in the Healthy Living group had the same amount and length of weekly group videoconferences and daily brief email-delivered “video lessons” as caregivers in the TeleSavvy group.26 Healthy Living is based off Go4Life by the National Institute on Aging and covered topics like healthy nutrition, stretching, balancing, and aerobic and resistance exercises.42,43 The group's videoconferences were equivalent to that in Tele‐Savvy. Similarly, the caregivers received daily instructional videos and written materials similar to those in Tele‐Savvy, which were housed on the Canvas platform41 and caregivers could watch and re‐watch videos at their convenience. Caregivers also received a manual and a workbook.
- Usual Care (waitlist control). Caregivers randomized to Usual Care were encouraged to continue to provide care for the PLwD through their customary means. These caregivers were asked not to enroll in an extended caregiver education program during the 6-month period.
Neither Tele-Savvy nor Healthy Living addressed sleep. More information on the parent study design is found in a previous publication.26
Participants
Participants were informal caregivers (family/friends) of PLwD. Participants had to provide an average of 4 hr of assistance per day to a PLwD. The caregiver did not have to live with the PLwD; however, the caregiver could not plan to move the PLwD to a residential community in the 6 months after beginning the study. Participants were excluded if they were involved in another caregiver training study or had previously participated in SCP. Each participant had to have access to a computer or a mobile device with an adequate internet connection, microphone, and speakers and be able to use email. Participants also needed to be able to read, speak, and understand English, and have no uncorrectable vision or hearing deficits that might have impeded participation.
Randomization
After completing the informed consent process, the study statistician randomly assigned the participants on a 2:2:1 ratio to immediate participation in the Tele-Savvy intervention, immediate participation in the Healthy Living condition, or usual care condition. Participants in the Healthy Living and usual care conditions were offered Tele-Savvy after a six-month data collection visit. Three hundred and eleven caregivers participated in the study, which ran July 2017 through December 2020 (see previous publication for complete CONSORT chart).26,42 The study was approved by the Emory IRB (IRB00092812) and preregistered on clinicaltrials.gov (NCT03033875). The study complied with the Declaration of Helsinki.
Measures
Caregivers were asked to provide information about their socioeconomic status, age, length of caregiving, and co-residence with recipient as well as self-reports on their emotional well-being and sense of caregiving competence (these are described in a prior report).26
Sleep was assessed at baseline, at 3 months, and at 6 months.
Sleep Quality: Sleep quality was assessed with the Pittsburgh Sleep Quality Index (PSQI).44 The PSQI is a 19-item instrument, which measures seven different components of sleep including subjective sleep quality, sleep latency (ie, how long it takes to fall asleep), sleep duration, habitual sleep efficiency (ie, the percentage of time in bed that one is asleep), sleep disturbances, use of sleeping medication, and daytime dysfunction.44 Each of the seven components is weighted on a 0–3 interval scale. The global PSQI score is calculated by totaling the seven component scores, providing an overall score ranging from 0 to 21, where lower scores denote better sleep quality; a score greater than five indicates poor sleep quality.44 The psychometric properties of the PSQI have been documented in multiple studies.45,46 The PSQI was used in this study to provide a broad perspective on disordered sleep, one that encompasses, but is not limited to, the self-report of poor sleep. In our sample, the PSQI had a Cronbach’s alpha=0.762.
Insomnia: Insomnia was assessed with the Insomnia Severity Index (ISI).47 The ISI is a 7-item self-report questionnaire, which evaluates the nature, severity, and impact of insomnia in the last month.47 Each item is rated using a 5-point Likert scale (eg, 0 = no problem; 4 = very severe problem), resulting in a total score ranging from 0 to 28. Previous studies have reported adequate psychometric properties.47,48 ISI is widely used as an outcome in behavioral intervention studies for insomnia. In our sample, the ISI had a Cronbach’s alpha=0.908.
Dataset for these analyses: The sleep measures (PSQI and ISI) were added after the study was underway, thus the analyses presented here focuses on a subset of 137 caregivers, as well as the 80 caregivers including caregivers from the waitlist control and attention control groups (for the combined effects). To avoid confounding intervention effects due to the impact of the pandemic, data collected after the COVID-19 shutdown in March 2020 were removed.
Analysis
At the time of each interview, a trained research staff member entered the data directly into the dedicated project tablet computer, which was saved on Emory’s secure REDCap platform. Descriptive statistics and frequency distributions were examined to identify outliers and ensure integrity of merged files. For all multi-item scales, internal consistency was examined using Cronbach’s alpha and associated statistics (eg, item-total correlations).
Multi-level mixed-effects models (MLM) with random (participant) effects (ie random intercepts) were used to test for the effects of group, time, and group*time factor interactions. To test the differences between the three randomized groups, Intent-to-Treat (ITT) principles were followed with all available data included in the models for all caregivers who completed the PSQI and ISI at baseline and follow-up visits. To compare the Tele-Savvy intervention group (n=51) to the Healthy Living (n=59) and usual care (n=27) groups, the first 3 time points (baseline and 3- and 6-months) were used to test for differences between the three-group longitudinal trajectories. For the merged groups (n=80) after receipt of the Tele-Savvy intervention, the MLM models initially included both group and time effects. However, neither the group nor group-by-time effects were statistically significant, so group was dropped from the models and only the time effect was tested for the merged changes over time.49 Sidak Type-I error rate adjustment (which has higher power than Bonferroni) was applied for multiple pairwise comparisons between the 3 time points and groups. SPSS v.27 was used for all analyses at the 5% significance level.50 For the sample size of n=137 for the three group, 3 time point comparisons, we were powered at 80% and 5% level of significance to detect moderate-to-large effect sizes for the group (f=0.269), time (f=0.304) and group-by-time (f=0.304) factors; and for the n=80 merged groups after the Tele-Savvy intervention, we were powered to detect moderate-to-large time effects (f=0.356); power analyses completed using PASS 2023.
Results
The 137 caregiver ages ranged from 31 years to 87 years with an average age of 64.7 (standard deviation (SD) −10.4) years. The average age of the PLwD was 74.9 (9.7) years. Most of the caregivers were female (68.6%), White (68.6%), caring for a spouse (65%), not employed (57.7%), had less than a BA/BS college degree (57.7%), and lived in either an urban (33.3%) or suburban area (43.0%). A slight majority of caregivers did have help from someone else (54.0%). More than a third (39.4%) were caring for others besides the PLwD. See Table 1. Additionally, most of these caregivers (115, 83.9%) lived with the PLwD, had been caring for the PLwD between 0 and 13 years with a median of 2 years.
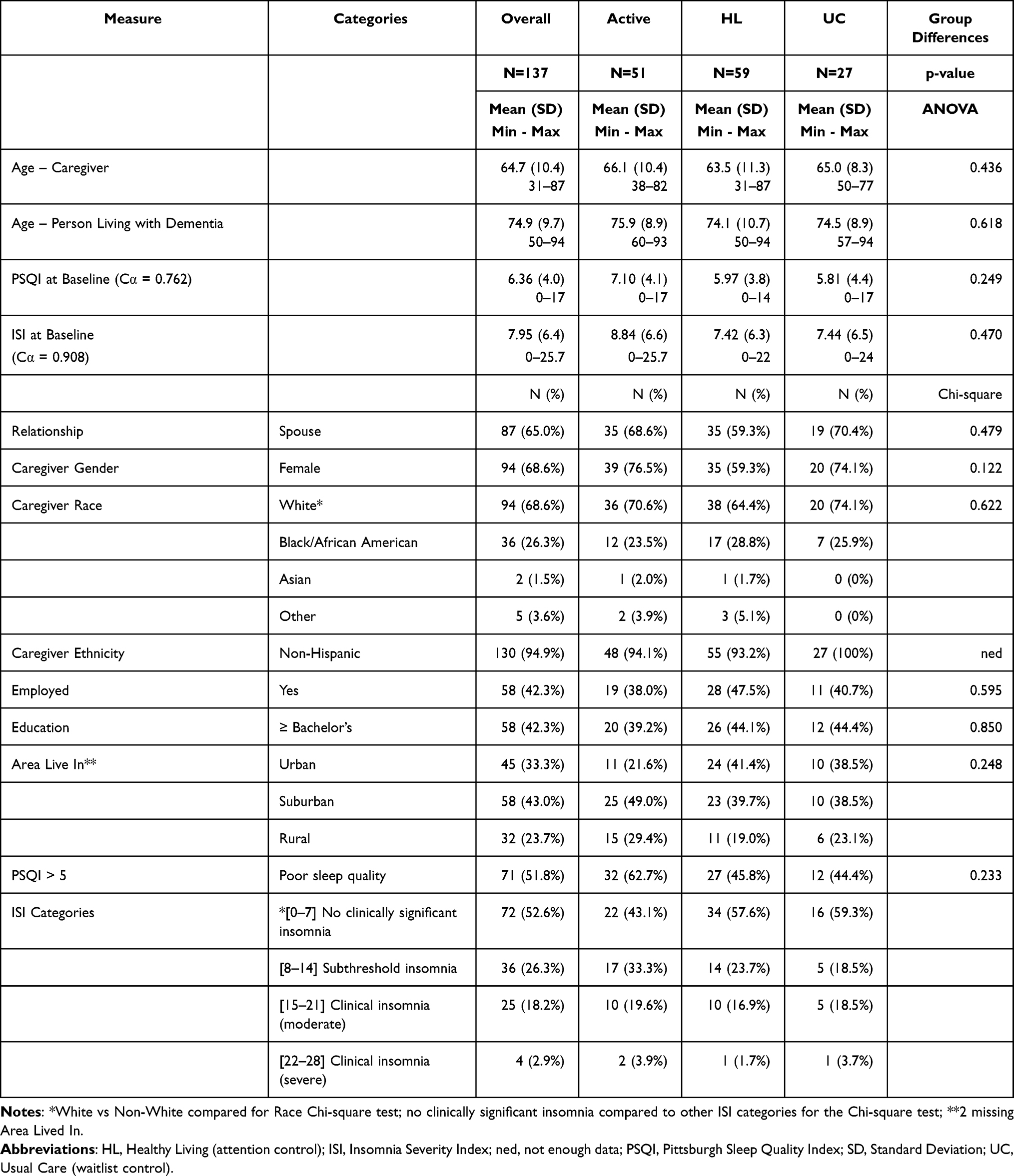 |
Table 1 Demographics – Baseline Cohorts 1–23: Overall and by Group |
The PSQI scores ranged from 0 to 17 with an average at baseline of 6.36 (4.0) with slightly more than half (51.8%) of the participants scoring greater than 5 on the PSQI.44 See Table 1. The three sleep quality components that scored the worst out of the 7 PSQI component scores were daytime dysfunction due to sleepiness, sleep disturbances, and poor duration of sleep. The ISI scores ranged from 0 to 25 with an average of 7.95 (6.4) at baseline with nearly half (47.4%) having subthreshold insomnia or worse (Table 1).
When we conducted MLM models of group, time, and group-by-time effects for PSQI and ISI, none of the model effects were significant (Table 2). However, there were noticeable differences between the immediate Tele-Savvy group that showed decreasing PSQI scores (improving sleep quality) from baseline, whereas the trends for the Healthy Living and usual care groups showed increasing PSQI scores (worsening sleep quality) (Table 2 and Figure 1 top). In fact, the immediate Tele-Savvy group’s PSQI scores reflected a small-to-moderate effect improvement (Cohen’s d = −0.298) from baseline to 3 months (Table 2). The Healthy Living and usual care groups’ PSQI scores increased (got worse) on average with the PSQI scores increasing the most in the usual care group (Table 2 and Figure 1 top). However, even with the improvements seen for the immediate Tele-Savvy group, more than half the caregivers still had PSQI scores > 5, indicating poor sleep quality, after 6 months. For ISI, there was a small effect size improvement (decreased ISI) from baseline to 3-month (d = 0.202) for the pairwise effect sizes for the immediate Tele-Savvy group, suggesting that there was improvement in insomnia symptoms from baseline (Table 2). Like PSQI, the pairwise changes in ISI scores for the Healthy Living and usual care groups increased (got worse) over time (Table 2 and Figure 1 bottom).
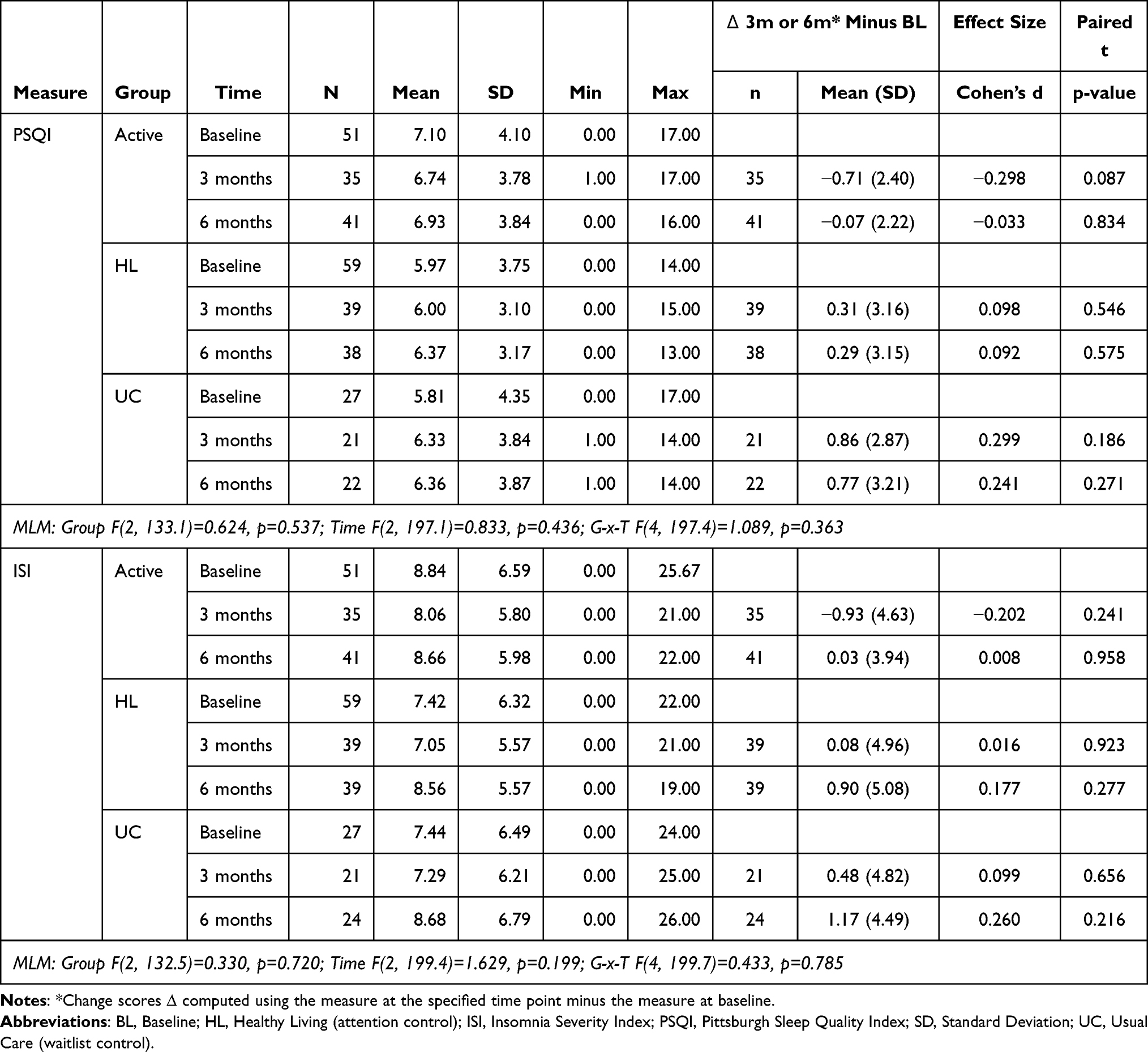 |
Table 2 PSQI and ISI Measures by Group and Time Point (from Baseline to 3 Months to 6 Months) |
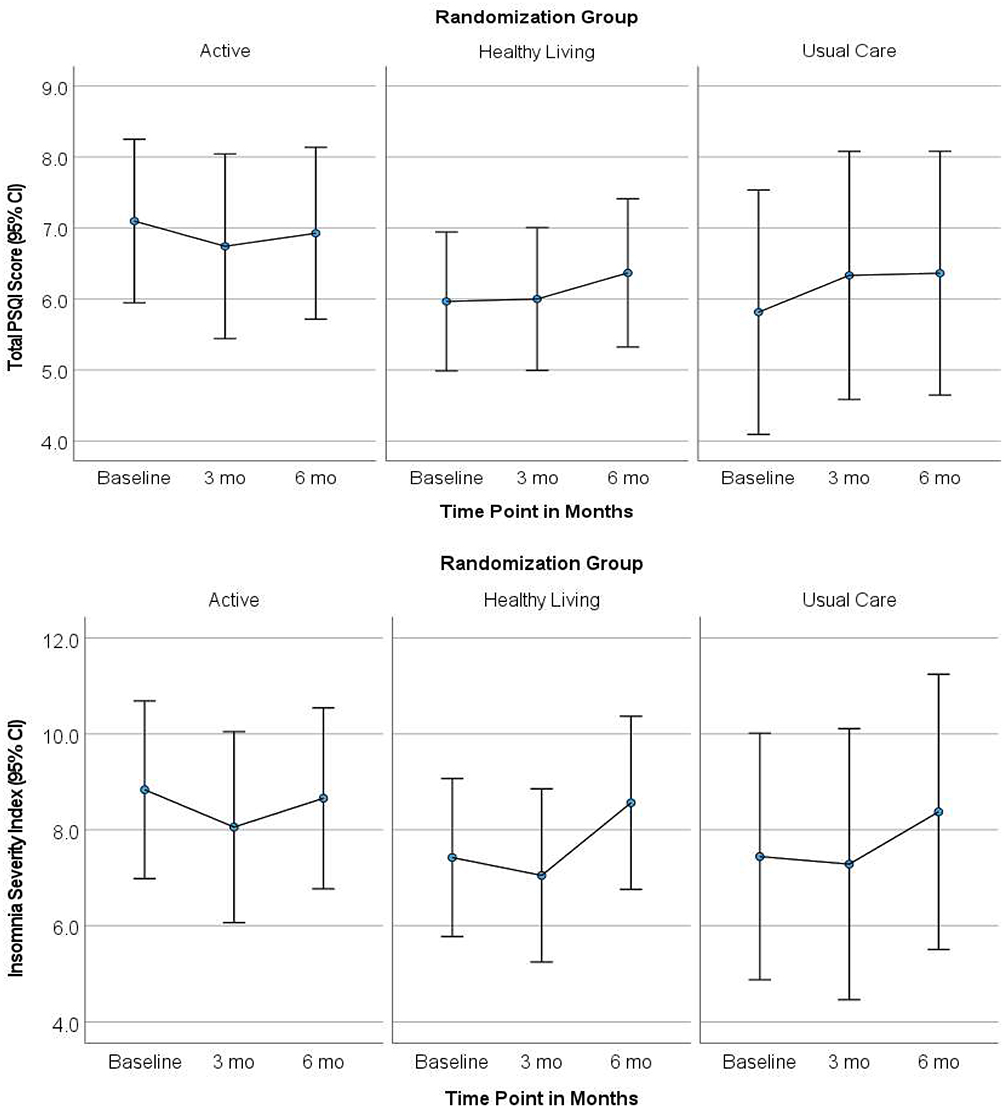 |
Figure 1 [TOP] PSQI, and [BOTTOM] ISI by Group and Time Point. |
To estimate the overall effect of the Tele-Savvy intervention, we merged the results of the immediate Tele-Savvy group (baseline to 6-month) with the results from the Healthy Living and usual care groups after they received the intervention (6-month to 12-month) (Table 3). For these merged results (n=80, Table 3 and Figure 2), the PSQI results showed decreasing scores over time (Figure 2 LEFT) but the time effect was not statistically significant (p=0.474, Table 3). Even though the time effect was not significant, the percentage of caregivers with PSQI scores > 5 decreased from 57.5% at baseline immediately before receipt of the Tele-Savvy intervention to 49.2% 6 months later. ISI scores also decreased over time (Figure 2 RIGHT) with a significant time effect (p=0.050, Table 3) for differences across the time points, with a small-to-moderate effect size for the improvements from baseline to 6-month (d = −0.310).
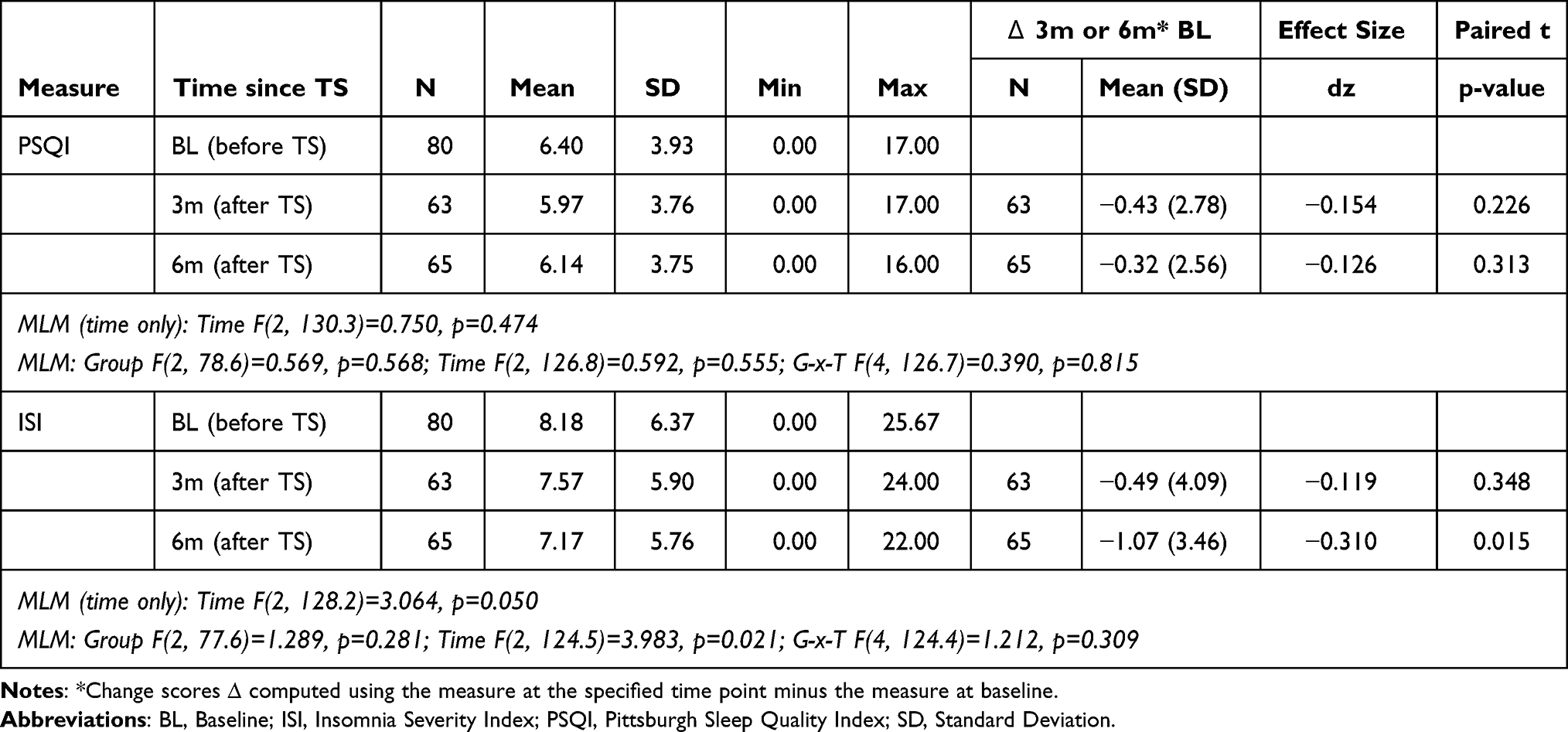 |
Table 3 Merged Tele-Savvy Results for PSQI and ISI |
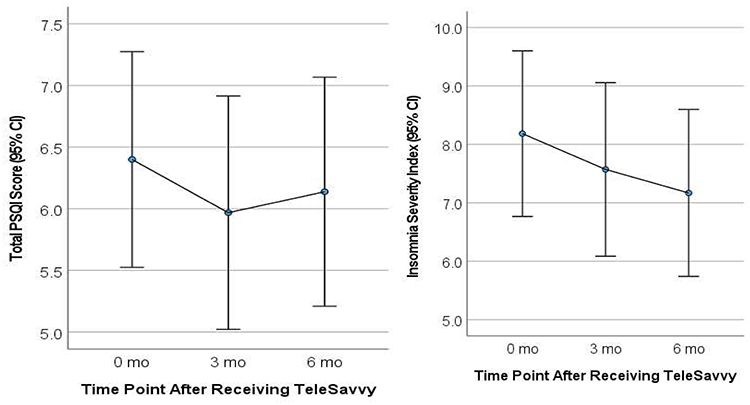 |
Figure 2 [LEFT] PSQI and [RIGHT] ISI by Time since Receiving Tele-Savvy for all participants who received Tele-Savvy. |
Discussion
This study examined the impact of Tele-Savvy, a psychoeducational intervention, compared to Healthy Living and usual care on sleep quality and insomnia symptoms. In the main analysis, we found no group, time nor group-by-time effects for PSQI and ISI. We did, however, find that, in the between-group analysis, participants in the Healthy Living and usual care control groups reported trends of worsening sleep symptoms and insomnia symptoms compared to the Tele-Savvy group. Considering the combined caregivers’ experience of Tele-Savvy participation (after everyone received the intervention), we found a significant improvement (with moderate effect size) in ISI scores for the combined group of subjects who took part in Tele-Savvy. Likewise, we found a positive but non-significant trend (with small effect size) in the improvement of sleep quality symptoms of these participants. These results provide encouraging evidence that the Tele-Savvy intervention may be protective of worsening sleep quality and helpful in preventing or reducing insomnia symptoms.
Results were comparable to those found with other psychoeducational interventions. Caregivers who received the Resources for Enhancing Alzheimer’s Caregiver Health intervention, which provided educational materials on self-care and a computerized telephone support system reported a non-significant improvement in their sleep quality.51 Similarly, caregivers in “Building Better Caregivers”, a 6-week behavioral intervention group workshop for stress reduction, self-efficacy, and social support, did not have an improvement in their sleep at 6 months post-intervention but had an improvement at 12 months post-intervention.52 Our results differ from those reported by Forney, Gajer, Williams, Schneider, Koenig, McCulle, Karlebach, Brotman, Davis, Ault, and Ravel53 who found that a video-based coping skills training intervention with added telephone coaching had no effect on subjective sleep quality. Similarly, caregivers who received the Interprofessional Virtual Healthcare Neighborhood (a 16-week online educational intervention) did not experience any significant changes in sleep quality or quantity, with both the intervention and the usual care groups experiencing reductions in their insomnia severity scores.54
It is possible that psychoeducation interventions like Tele-Savvy might improve caregiver sleep because it improves caregiver competence, reduces depressive symptoms and perceived stress, and improves caregiver self-care.26,27 Knowing how to care for the PLwD and feeling less stressed could enhance caregivers' ability to fall asleep quicker and have less wake after sleep onset.31 Moreover, Tele-Savvy focuses on self-care and discusses relaxation and yoga meditation, practices that have been shown to improve sleep in many studies.55–57 Practicing relaxation techniques during the day or before bed could have reduced caregivers’ stress level thus making it more conducive to sleep better.
While caregivers may be sleeping better due to feeling more competent, and less stressed and depressed, without the techniques of how to improve their sleep, there may be a floor effect regarding how much improvement can result from psychoeducational interventions as exemplified in this study with caregivers still having poor sleep quality, on average, at the end of the intervention. Since disturbed sleep is so pervasive in the caregiving population, sleep education and behavioral sleep techniques should be integrated into caregiver psychoeducational interventions. For example, a four-session behavioral intervention delivered either in a group setting or individually which consisted of sleep hygiene, stimulus control, sleep compression strategies, education about community resources, stress management, and techniques to reduce PLwD disruptive behaviors, resulted in improved sleep quality and sleep efficiency for caregivers immediately after the 3-months intervention.58 A similar behavioral sleep intervention for caregivers combining relaxation, stimulus control, and sleep hygiene with personal goal setting also resulted in improved subjective sleep quality post-intervention, but the effect was not statistically significant.59
There were limitations to the study. The study used subjective self-reported assessments for sleep over the past week or month. It did not assess sleep daily via diary, so may miss the variability often reported in caregiver sleep. Also, objective assessment of sleep quality metrics such as from actigraphy could have allowed for broader assessment of caregiver sleep.
Conclusion
This study provides evidence that Tele-Savvy, a psychoeducational intervention, can reduce insomnia and protect caregivers from worsening sleep quality. Researchers should continue to test the effect of psychoeducational interventions on sleep outcomes and incorporate behavioral sleep education into psychoeducational interventions being developed for caregivers.
Data Sharing Statement
The author does not intend to share individual deidentified participant data.
Funding
Agency: National Institute on Aging Grant/Award Numbers: R01AG054079 (PI: Hepburn, Griffiths), K23AG070378 (PI: Brewster), K23AG065452 (PI: Epps) .
Disclosure
Dr Glenna Brewster reports grants from National Institute on Aging, during the conduct of the study. Dr Donald L Bliwise reports personal fees from CliniLabs, personal fees from Eisai, personal fees from Ferring, personal fees from Huxley, personal fees from Idorsia, personal fees from Merck, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Gaugler J, James B, Johnson T, et al. 2022 Alzheimer’s disease facts and figures. Alzhei Demen. 2022;18(4):700–789.
2. Fonareva I, Oken BS. Physiological and functional consequences of caregiving for relatives with dementia. Int Psychogeriatr. 2014;26(5):725–747. doi:10.1017/S1041610214000039
3. Peng HL, Lorenz RA, Chang YP. Factors associated with sleep in family caregivers of individuals with dementia. Perspect Psychiatr Care. 2019;55(1):95–102. doi:10.1111/ppc.12307
4. Wilcox S, King AC. Sleep complaints in older women who are family caregivers. J Gerontol B Psychol Sci Soc Sci. 1999;54(3):P189–98. doi:10.1093/geronb/54b.3.p189
5. Castro CM, Lee KA, Bliwise DL, Urizar GG, Woodward SH, King AC. Sleep patterns and sleep-related factors between caregiving and non-caregiving women. Behav Sleep Med. 2009;7(3):164–179. doi:10.1080/15402000902976713
6. Fonareva I, Amen AM, Zajdel DP, Ellingson RM, Oken BS. Assessing sleep architecture in dementia caregivers at home using an ambulatory polysomnographic system. J Geriatr Psychiatry Neurol. 2011;24(1):50–59. doi:10.1177/0891988710397548
7. McKibbin CL, Ancoli-Israel S, Dimsdale J, et al. Sleep in spousal caregivers of people with Alzheimer’s disease. Sleep. 2005;28(10):1245–1250. doi:10.1093/sleep/28.10.1245
8. Gao C, Chapagain NY, Scullin MK. Sleep duration and sleep quality in caregivers of patients with dementia: a systematic review and meta-analysis. JAMA Netw Open. 2019;2(8):e199891. doi:10.1001/jamanetworkopen.2019.9891
9. Grandner M, Mullington JM, Hashmi SD, Redeker NS, Watson NF, Morgenthaler TI. Sleep duration and hypertension: analysis of > 700,000 adults by age and sex. J Clin Sleep Med. 2018;14(6):1031–1039. doi:10.5664/jcsm.7176
10. Antza C, Kostopoulos G, Mostafa S, Nirantharakumar K, Tahrani A. The links between sleep duration, obesity and type 2 diabetes mellitus. J Endocrinol. 2021;252(2):125–141. doi:10.1530/JOE-21-0155
11. Sprecher KE, Koscik RL, Carlsson CM, et al. Poor sleep is associated with CSF biomarkers of amyloid pathology in cognitively normal adults. Neurology. 2017;89(5):445–453. doi:10.1212/WNL.0000000000004171
12. Creese J, Bédard M, Brazil K, Chambers L. Sleep disturbances in spousal caregivers of individuals with Alzheimer’s disease. Int Psychogeriatr. 2008;20(1):149–161. doi:10.1017/S1041610207005339
13. Rongve A, Boeve BF, Aarsland D. Frequency and correlates of caregiver-reported sleep disturbances in a sample of persons with early dementia. Am Geriatr Soc. 2010;58(3):480–486. doi:10.1111/j.1532-5415.2010.02733.x
14. Cupidi C, Realmuto S, Lo Coco G, et al. Sleep quality in caregivers of patients with Alzheimer’s disease and Parkinson’s disease and its relationship to quality of life. Int Psychogeriatr. 2012;24(11):1827–1835. doi:10.1017/S1041610212001032
15. Ali S, Bokharey IZ. Maladaptive cognitions and physical health of the caregivers of dementia: an interpretative phenomenological analysis. Int J Qual Stud Health Well-Being. 2015;10:28980. doi:10.3402/qhw.v10.28980
16. Mausbach BT, Ancoli-Israel S, von Känel R, et al. Sleep disturbance, norepinephrine, and D-dimer are all related in elderly caregivers of people with Alzheimer disease. Sleep. 2006;29(10):1347–1352. doi:10.1093/sleep/29.10.1347
17. von Känel R, Mausbach BT, Ancoli-Israel S, et al. Sleep in spousal Alzheimer caregivers: a longitudinal study with a focus on the effects of major patient transitions on sleep. Sleep. 2012;35(2):247–255. doi:10.5665/sleep.1632
18. Vitaliano PP, Murphy M, Young HM, Echeverria D, Borson S. Does caring for a spouse with dementia promote cognitive decline? A hypothesis and proposed mechanisms. J Am Geriatr Soc. 2011;59(5):900–908. doi:10.1111/j.1532-5415.2011.03368.x
19. Wulff K, Gatti S, Wettstein JG, Foster RG. Sleep and circadian rhythm disruption in psychiatric and neurodegenerative disease. Nat Rev Neurosci. 2010;11(8):589–599. doi:10.1038/nrn2868
20. Hepburn K, Lewis M, Tornatore J, Sherman CW, Bremer KL. The Savvy Caregiver program: the demonstrated effectiveness of a transportable dementia caregiver psychoeducation program. J Gerontol Nurs. 2007;33(3):30–36.
21. Kally Z, Cote S, Gonzalez J, et al. The savvy caregiver program: impact of an evidence-based intervention on the well-being of ethnically diverse caregivers. J Gerontol Soc Work. 2013;57:1–13.
22. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Advan Behav Res Ther. 1978;1(4):139–161. doi:10.1016/0146-6402(78)90002-4
23. Bandura A. Human agency in social cognitive theory. Am Psychol. 1989;44(9):1175–1184. doi:10.1037/0003-066X.44.9.1175
24. Folkman S. Personal control and stress and coping processes: a theoretical analysis. J Pers Soc Psychol. 1984;46(4):839–852. doi:10.1037/0022-3514.46.4.839
25. Folkman S, Lazarus RS, Gruen RJ, DeLongis A. Appraisal, coping, health status, and psychological symptoms. J Pers Soc Psychol. 1986;50(3):571–579. doi:10.1037/0022-3514.50.3.571
26. Hepburn K, Nocera J, Higgins M, et al. Results of a randomized trial testing the efficacy of tele-savvy, an online synchronous/asynchronous psychoeducation program for family caregivers of persons living with dementia. Gerontologist. 2021;2021:1.
27. Griffiths PC, Kovaleva M, Higgins M, Langston AH, Hepburn K. Tele-savvy: an online program for dementia caregivers. Am J Alzheimers Dis Other Demen. 2018;33(5):269–276. doi:10.1177/1533317518755331
28. Brewster GS, Epps F, Dye CE, Hepburn K, Higgins MK, Parker ML. The effect of the “great village” on psychological outcomes, burden, and mastery in African American caregivers of persons living with dementia. J Appl Gerontol. 2020;39(10):1059–1068. doi:10.1177/0733464819874574
29. Zhao Y, Feng H, Hu M, et al. Web-Based interventions to improve mental health in home caregivers of people with dementia: meta-analysis. J Med Internet Res. 2019;21(5):e13415. doi:10.2196/13415
30. Cheng ST, Au A, Losada A, Thompson LW, Gallagher-Thompson D. Psychological interventions for dementia caregivers: what we have achieved, what we have learned. Current Psychiatry Reports. 2019;21(7):59. doi:10.1007/s11920-019-1045-9
31. Sanprakhon P, Chaimongkol N, Lach HW. Integrative stress reduction program for family caregivers of persons with advanced dementia: a randomized-controlled trial. West J Nurs Res. 2023;45(11):1017–1026. doi:10.1177/01939459231201251
32. Almutairi RR, Zauszniewski JA. sleep quality and depressive symptoms in caregivers of persons with dementia: a systematic review. Issues Ment Health Nurs. 2023;44(6):538–550. doi:10.1080/01612840.2023.2205535
33. Simpson C, Carter P. Short-term changes in sleep, mastery & stress: impacts on depression and health in dementia caregivers. Geriatric Nurs. 2013;34(6):509–516. doi:10.1016/j.gerinurse.2013.07.002
34. Mezick EJ, Matthews KA, Hall M, et al. Intra-individual variability in sleep duration and fragmentation: associations with stress. Psychoneuroendocrinology. 2009;34(9):1346–1354. doi:10.1016/j.psyneuen.2009.04.005
35. McCurry SM, Teri L. Sleep disturbance in elderly caregivers of dementia patients. Clin Gerontol. 1995;16(2):51–65. doi:10.1300/J018v16n02_05
36. Rowe MA, McCrae CS, Campbell JM, Benito AP, Cheng J. Sleep pattern differences between older adult dementia caregivers and older adult noncaregivers using objective and subjective measures. J Clin Sleep Med. 2008;4(4):362–369. doi:10.5664/jcsm.27238
37. Peng LM, Chiu YC, Liang J, Chang TH. Risky wandering behaviors of persons with dementia predict family caregivers’ health outcomes. Aging Mental Health. 2018;22(12):1650–1657. doi:10.1080/13607863.2017.1387764
38. Gibson R, Helm A, Ross I, Gander P, Breheny M. ”I think I could have coped if I was sleeping better”: sleep across the trajectory of caring for a family member with dementia. Dementia. 2023;22(5):1038–1056. doi:10.1177/14713012231166744
39. Werner A, Kater M-J, Schlarb AA, Lohaus A. Sleep and stress in times of the COVID-19 pandemic: the role of personal resources. Appl Psychol. 2021;13(4):935–951. doi:10.1111/aphw.12281
40. Hall MH, Casement MD, Troxel WM, et al. Chronic stress is prospectively associated with sleep in midlife women: the SWAN sleep study. Sleep. 2015;38(10):1645–1654. doi:10.5665/sleep.5066
41. Instructure; 2020. Available from: https://www.instructure.com/canvas/.
42. Kovaleva M, Nocera JR, Hepburn K, et al. Attention control in a trial of an online psychoeducational intervention for caregivers. Res Nurs Health. 2022;45(3):337–349. doi:10.1002/nur.22208
43. National Institute on Aging. Go4Life; 2011. Available from: https://www.ncoa.org/resources/go4life/.
44. Buysse D, Reynolds C, Monk TH, Berman S, Kupfer DJ. The Pittsburgh sleep quality index - a new instrument for psychiatric practice and research. Psych Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
45. Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F. Test-retest reliability and validity of the Pittsburgh sleep quality index in primary insomnia. J Psychosom Res. 2002;53(3):737–740. doi:10.1016/S0022-3999(02)00330-6
46. Song MJ, Kim JH. Family caregivers of people with dementia have poor sleep quality: a nationwide population-based study. Int J Environ Res Public Health. 2021;18(24):13079. doi:10.3390/ijerph182413079
47. Bastien CH, Vallières A, Morin CM. Validation of the insomnia severity index as an outcome measure for insomnia research. Sleep Med. 2001;2(4):297–307. doi:10.1016/S1389-9457(00)00065-4
48. Jiménez-Gonzalo L, Romero-Moreno R, Pedroso-Chaparro MDS, et al. Psychometric properties of the insomnia severity index in a sample of family dementia caregivers. Sleep Med. 2021;82:65–70. doi:10.1016/j.sleep.2021.03.036
49. Hedeker D, Gibbons RD. Longitudinal Data Analysis. Hoboken, N.J: John Wiley & Sons, Inc; 2006.
50. Corp I. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp; 2020.
51. Elliott AF, Burgio LD, Decoster J. Enhancing caregiver health: findings from the resources for enhancing alzheimer’s caregiver health II intervention. Am Geriatr Soc. 2010;58(1):30–37. doi:10.1111/j.1532-5415.2009.02631.x
52. Lorig K, Ritter PL, Laurent DD, Yank V. Building better caregivers: a pragmatic 12-month trial of a community-based workshop for caregivers of cognitively impaired adults. J Appl Gerontol. 2019;38(9):1228–1252. doi:10.1177/0733464817741682
53. Forney LJ, Gajer P, Williams CJ, et al. Comparison of self-collected and physician-collected vaginal swabs for microbiome analysis. J Clin Microbiol. 2010;48(5):1741–1748. doi:10.1128/JCM.01710-09
54. Fowler CN, Kott K, Wicks MN, Rutledge C. Self-efficacy and sleep among caregivers of older adults with dementia effect of an interprofessional virtual healthcare neighborhood. J Gerontol Nurs. 2016;42(11):39–47. doi:10.3928/00989134-20160901-02
55. Innes KE, Selfe TK, Brown CJ, Rose KM, Thompson-Heisterman A. The Effects of meditation on perceived stress and related indices of psychological status and sympathetic activation in persons with alzheimer’s disease and their caregivers: a pilot study. Evid Based Complement Alternat Med. 2012;2012:927509. doi:10.1155/2012/927509
56. Jain FA, Nazarian N, Lavretsky H. Feasibility of central meditation and imagery therapy for dementia caregivers. Int J Geriatr Psychiatry. 2014;29(8):870–876. doi:10.1002/gps.4076
57. Paller KA, Creery JD, Florczak SM, et al. Benefits of mindfulness training for patients with progressive cognitive decline and their caregivers. Am J Alzheimers Dis Other Demen. 2015;30(3):257–267. doi:10.1177/1533317514545377
58. McCurry SM, Logsdon RG, Vitiello MV, Teri L. Successful behavioral treatment for reported sleep problems in elderly caregivers of dementia patients: a controlled study. J Gerontol B Psychol Sci Soc Sci. 1998;53:2.
59. Simpson C, Carter PA. Pilot study of a brief behavioral sleep intervention for caregivers of individuals with dementia. Res Gerontol Nurs. 2010;3(1):19–29. doi:10.3928/19404921-20090731-02
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.