")
Back to Journals » Clinical Ophthalmology » Volume 17
The Effect of Sodium Hyaluronate Eye Drops 2, 4 or 6 Times a Day on Signs and Symptoms of Dry Eye Disease
Authors Muñoz-Villegas PDC , Sánchez-Ríos A, Olvera-Montaño O
Received 3 August 2023
Accepted for publication 29 September 2023
Published 6 October 2023 Volume 2023:17 Pages 2945—2955
DOI https://doi.org/10.2147/OPTH.S433709
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Patricia del Carmen Muñoz-Villegas,1,2 Alejandra Sánchez-Ríos,1 Oscar Olvera-Montaño1
1Regional Medical Affairs Department, Laboratorios Sophia, S.A. de C.V, Zapopan, Jalisco, Mexico; 2Centro de Investigación en Matemáticas A.C. (CIMAT), Unidad Aguascalientes, Aguascalientes, Mexico
Correspondence: Patricia del Carmen Muñoz-Villegas, Regional Medical Affairs Department, Laboratorios Sophia, S.A. de C.V, Paseo del Norte 5255, Guadalajara Technology Park, Zapopan, Jalisco, 45010, Mexico, Tel +52 (33) 3301 4200, Email [email protected]
Purpose: A randomized clinical trial was run to evaluate the effectiveness of a preservative-free 0.4% sodium hyaluronate eye drop (LOF) in different dosage schemes to alleviate signs and symptoms of dry eye disease (DED).
Methods: A total of 116 subjects with mild-to-moderate DED were included, and 111 completed the study (from which 67.6% were female and 65.3% were users of oral contraceptives). Patients were randomly assigned to instill a drop of LOF either 2 (BID), 4 (QID) or 6 (6TD) times a day (at least 3 hours apart) for 30 days. The clinical parameters and symptom endpoints were Ocular Surface Disease Index (OSDI), tear break-up time (TBUT), ocular surface staining, and conjunctival hyperemia. Other parameters evaluated were chemosis, best corrected visual acuity, and the incidence of adverse events (AE).
Results: There was a significant reduction in OSDI scores by day 30 in all groups. The recovery of the OSDI score back to normal values was observed in 51.4% of patients treated (50%, 48.6%, and 55.6% in BID, QID, and 6TD, respectively, p = 0.822). Similar improvement was observed for TBUT, 50.5% of patients increased this variable to > 10 seconds (39.5%, 51.4%, and 61.1%, p = 0.175), and for ocular surface staining, ≥ 72% showed Grade 0. There were no significant differences among posology groups regarding ocular surface staining, conjunctival hyperemia, or any safety parameters. No overall improvement in OSDI and TBUT to normal values was noted for 31 patients (21 were female and 71.4% users of contraceptive drugs).
Conclusion: The ophthalmic use of preservative free LOF, 2, 4 or 6 times a day, may alleviate clinical parameters and symptoms in 50% of patients with mild-to-moderate DED after a one-month treatment. This improvement seemed to be less ubiquitous in patients within reproductive age and using oral contraceptives.
Trial Registration: This trial is registered at clinicaltrials.gov (NCT0704531).
Keywords: contraceptives, dry eye disease, ocular surface disease index, sodium hyaluronate, tear break-up time
Introduction
Dry eye disease (DED) is a multifactorial disease characterized primarily by instability of the tear film that can be due to insufficient amount of tear production and/or poor quality of tear film,1,2 which may induce ocular signs and symptoms that decrease visual-related quality of life.1
DED is prevalent in up to 50% of the population, and its incidence is associated with a considerable amount of risk factors such as age, race, meibomian gland dysfunction, contact lens use, Sjögren syndrome and other systemic diseases, regular visual display use, environmental factors, nutritional deficiencies, etc.2,3 Sex is also a very significant risk factor for the development of DED, being more frequent in females than males.4 Furthermore, androgen deficiency is associated with both aqueous-deficient and evaporative dry eye.5 The decrease in serum androgen levels during menopause, pregnancy, and lactation, as well as the use of estrogen-containing oral contraceptives, have been proposed as a cause of primary lacrimal gland deficiency. Oral contraceptive use has been associated with increased symptoms of DED and contact lens intolerance in some studies.4–7
Regardless of the etiology or classification of DED, ocular lubricants are traditionally the therapeutic tool most frequently used, even in mild cases of this condition. Such is the case for Lagricel® Ofteno (Laboratorios Sophia, S.A. de C.V., Zapopan, Jalisco, Mexico), composed of high molecular weight 0.4% sodium hyaluronate preservative-free, has mucoadhesive properties responsible for increasing corneal residence time in addition to its humectant features.8,9 Sodium hyaluronate exhibits non-Newtonian properties that allow it to lubricate while offering a good tolerability profile and efficaciously improving DED symptoms.10,11
Ocular lubricants may be formulated as preservative free eye drops, avoiding the need of substances such as benzalkonium chloride and their disruptive proinflammatory effects on the ocular surface of the eye, tear film stability, as well as their toxicity on the corneal and conjunctival epithelium.12–14 Even though ocular lubricants do not modify underlying causes of DED, they are successful at attenuating ocular symptoms and therefore improving the everyday lives of those who use them.13–15
This study aims to provide evidence of the effectiveness of preservative-free 0.4% sodium hyaluronate eye drops at three different dosage schemes to alleviate clinical parameters and symptoms back within the range of normalcy in patients with mild-to-moderate DED after one month’s treatment.
Participants and Methods
Trial Design
This randomized, parallel assignment, prospective study was an open-label trial. This study was run in Mexico and registered at clinicaltrials.gov as NCT04704531. An ethics committee in each center reviewed and approved the study’s protocol and informed consent form (see Acknowledgments section). The research was conducted in compliance with the Declaration of Helsinki and in accordance with Good Clinical Practices Standards. All patients who participated in this study provided written and signed informed consent before their inclusion. Patients were recruited between January 2022 and June 2022 (FPFV: 2022–01-03 and LPLV: 2022–06-08).
Participants
Inclusion criteria contemplated male and female patients (age ≥18 years old) presenting mild-to-moderate DED diagnosis, defined as having an Ocular Surface Disease Index (OSDI) score between 13 and 32 plus one of the following: TBUT < 10 seconds, corneal staining with more than 5 dots, or conjunctival staining with more than 9 dots.1 Exclusion criteria included requiring implementation of the treatment scheme described in the step 2 management recommendations of the TFOS DEWS II,1,2 patients with eye parasitic infections, anterior blepharitis, conjunctivitis, Demodex infestation, unresolved ocular trauma, healing disorders of the ocular surface, presence of any illness that could interfere with study parameters (eg retinal diseases or glaucoma), history of penetrating keratoplasty, best corrected visual acuity (BCVA) of 20/200 or worse in either eye, previous history of any ophthalmic surgical procedure within 3 months before baseline, history of contact lens use, and pregnancy, breastfeeding or patients of childbearing age under no birth control treatment.
Interventions and Evaluations
A total of one hundred sixteen patients were randomized to instill a drop of 0.4% sodium hyaluronate preservative-free eye drops (Lagricel® Ofteno [LOF]) in the inferior conjunctival sac of both eyes 2 (BID), 4 (QID) or 6 times per day (6TD) (at least 3 hours apart) for 30 days. Follow-up visits took place on days 15 and 30 after randomization (day 1). A safety call was carried out 3 days after the final visit (33rd ± 1 day).
The study would be considered as discontinued if either the principal investigator or patient judged that it was not in the latter’s best interest to continue or if a female patient became pregnant.
Randomization and Masking
Patients were randomized following a 1:1:1 ratio to LOF. This was an open-label trial, in which the treatment assignment was not withheld from patients, researchers nor other sponsoring team members. However, subjects’ selection and evaluation bias were minimized by random assignment to posology groups. Randomization numbers were generated uniformly distributed using a computer software (SAS Institute, Inc., Cary, NC, USA).
Outcomes
The restoration of the parameters affected by DED was defined by the reduction of the OSDI score back to normal values (<13), the improvement of TBUT ≥10 seconds, and/or the presence of no epithelial staining (grade 0) after a one-month treatment period in at least one group.1,2,16
The OSDI questionnaire is the most widely used test in DED clinical trials. It measures frequency of symptoms in several environmental settings and vision-related quality of life. It has demonstrated to assess clinically important differences in DED research.17 The presence of epithelial defects was evidenced by corneal fluorescein and conjunctival lissamine green staining (CFS and CLGS, respectively), and conjunctival hyperemia evaluation was also performed at each follow-up visit. Safety was assessed by the presence of chemosis, BCVA evaluated through the Snellen chart, and the incidence of adverse events. TBUT with fluorescein was used to assess tear film stability.18 Surface dye staining was classified with a scale from 0 to V in accordance with the percentage of the affected area (Oxford scale). The tip of the dye strip was moistened with tetracaine (Ponti Ofteno®, Laboratorios Sophia S.A. de C.V.), and fluorescein (BioGlo, HUB Pharmaceuticals LLC) or lissamine green (Green Glo, HUB Pharmaceuticals LLC) was applied by contact in the lower conjunctival fornix. After instillation of dye, patients were asked to blink gently 2 times to allow adequate staining. CFS was observed immediately after the blinking (slip-lamp under the combination of a yellow filter and the highest cobalt blue illumination). CLGS was observed at least 1 minute but no more than 4 minutes after instillation of dye (slip-lamp under dimmed white light),19–21 Meanwhile the conjunctival hyperemia was classified following the Efron Scale.22,23 For AE, causality, relatedness assessment and severity were analyzed.24,25 The study schedule at each visit included (in the following order): OSDI (basal and day 30), BCVA, anterior biomicroscopy, FCS, TBUT, CLGS, intraocular pressure (IOP, using a calibrated Goldmann applanation tonometer), posterior ophthalmoscopy under mydriasis, and AE evaluation. In each site, all evaluations were performed by the same investigator.
Finally, since measurements obtained from right and left eyes are usually correlated, data from right eyes was used to give a single data point per patient for ophthalmic variables.26–28
Statistical Analysis
Statistical evaluations were carried out using the R statistical software package (The R Foundation for Statistical Computing; http://www.R-project.org). All data is expressed as mean ± standard deviation (SD) unless indicated otherwise. Sample size calculation was estimated to test the reduction in OSDI score after 30 days of treatment, with an expected change of 20%, at a level of significance of p < 0.05, and with a statistical power of 80%.29,30 Statistical analyses were performed with analyses of variance (ANOVA) for continuous data. The 95% confidence interval (CI) of these differences was computed. The categorical variables were analyzed using p × q contingency tables, and the differences were calculated with Pearson’s Chi-square test. Spearman correlation coefficient was used to evaluate the association among all considered variables at baseline that might explain changes in DED, based on previously published literature.14,31 All statistical analyzes performed in this study contemplated a p < 0.05 as significant.
Results
Characteristics of the Participants
A total of 116 patients were included in this study (intent-to-treat population), of which five discontinued their participation because of major protocol deviations (3/5, 60%) and follow-up loss (2/5, 40%). Therefore, 111 patients (38, 37 and 36, in BID, QID and 6TD, respectively) completed the entire protocol without deviations up to day 33 ± 1. Demographic and baseline characteristics were similar among each posology group, showing no significant differences, see Table 1. The mean age ± SD was 36.5 ± 13.5 years (range of 67 years), and 67.6% of patients were female, of which 65.3% were users of oral contraceptives. All subjects in each posology group were diagnosed with mild-to-moderate DED (see Participants and Methods section).
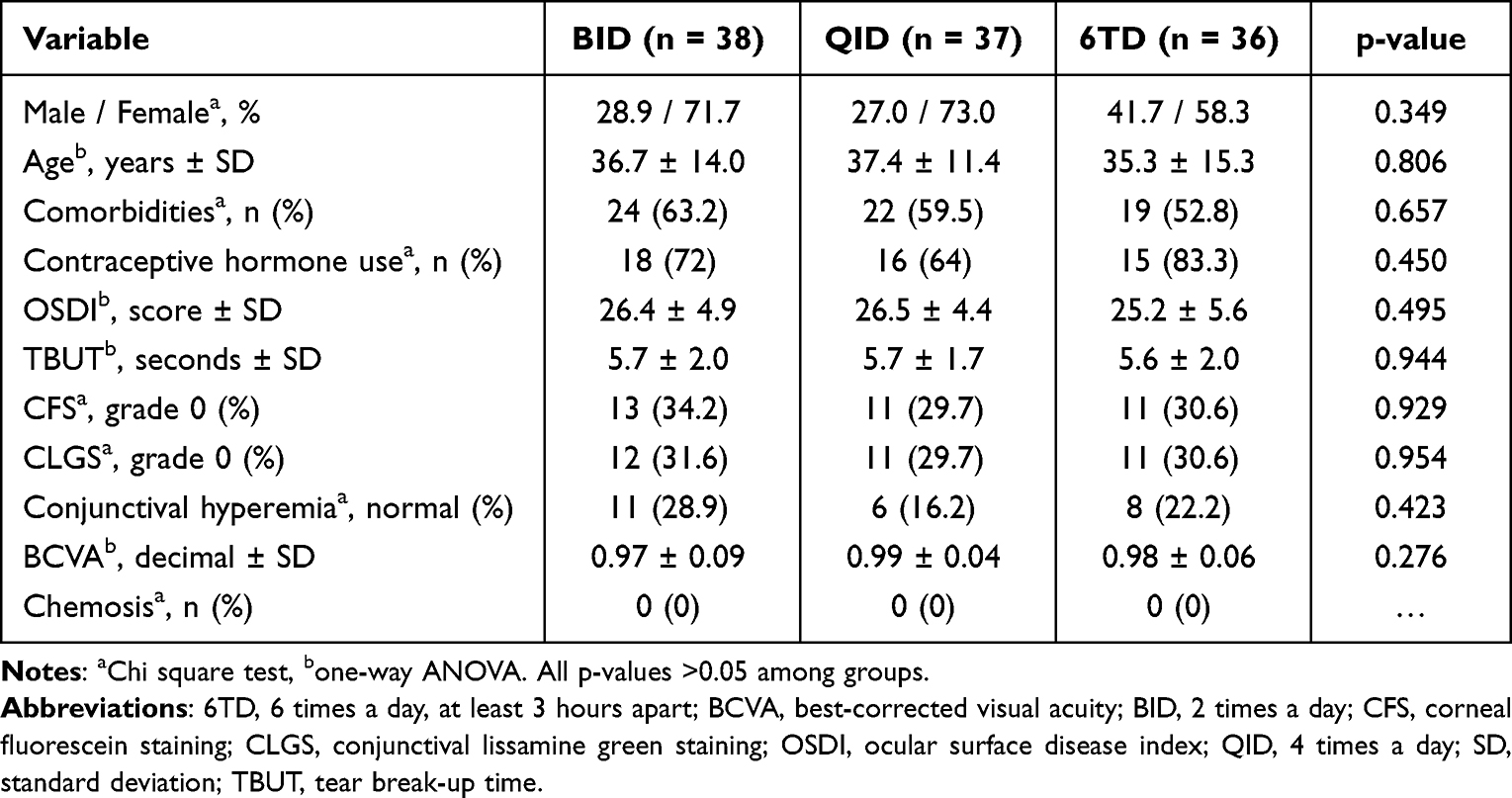 |
Table 1 Initial Characteristics of Each Posology Group |
The results of all correlations are shown in Figure 1. The correlation between age, BCVA, CFS, CLGS and conjunctival hyperemia was significant. There was a moderate positive correlation between CFS and CLGS (Rho = 0.58, p < 0.0001), conjunctival hyperemia with CFS (Rho = 0.54, p < 0.0001), and conjunctival hyperemia with CLGS (Rho = 0.49, p < 0.0001). A weak negative correlation between age and BCVA was observed (−0.39, p < 0.0001).
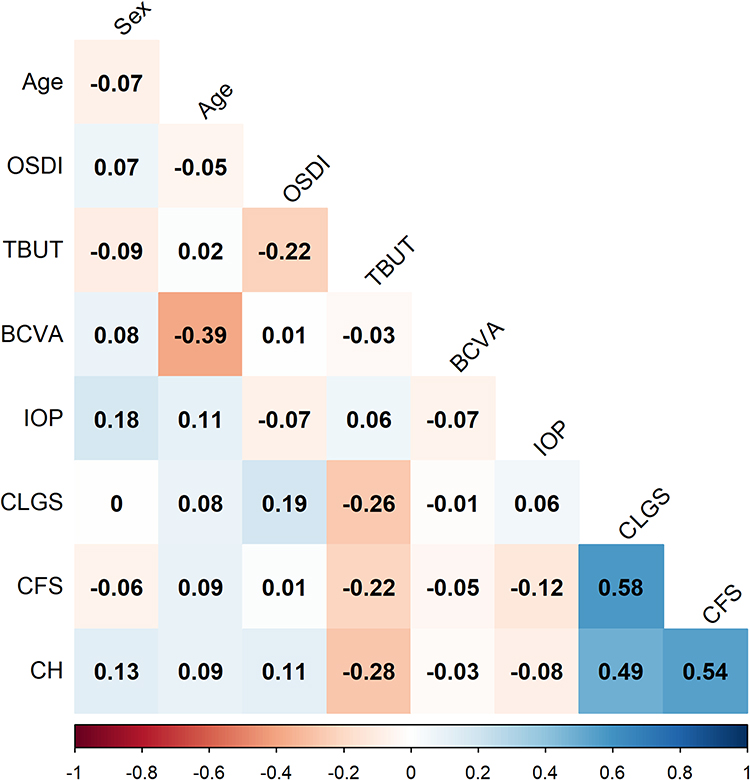 |
Figure 1 Matrix of correlations at baseline (n= 111). The r value is colored from the lowest obtained value (Rho= −0.39) as red, to Rho= 0.58 colored as blue. Abbreviations: BCVA, best corrected visual acuity; CFS, corneal fluorescein staining; CLGS, conjunctival lissamine green staining; IOP, intraocular pressure; OSDI, ocular surface disease index; TBUT, tear break-up time. |
Ocular Surface Disease Index (OSDI)
There was a significant reduction in OSDI score after one month of treatment in all groups (factor visit, p < 0.0001, 95% CI [−16.04, −13.21]), this analysis showed that all posology groups had a similar score reduction (no significant differences were found, p = 0.736), see Figure 2. The mean change ± SD from baseline to day 30 was −14.7 ± 6.6 for BID, −15.2 ± 7.9 for QID, and −13.9 ± 7.2 for 6TD. The final OSDI score was 11.7 ± 5.7 for BID vs 11.2 ± 6.5 for QID and 11.3 ± 4.6 for 6TD (p = 0.923).
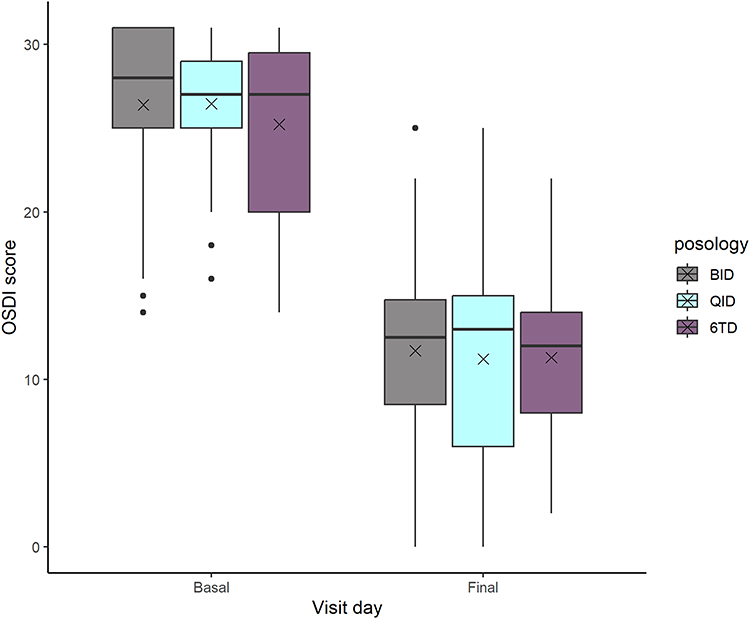 |
Figure 2 OSDI score, change after 30 days of treatment (n= 111). The decrease in all posology groups was statistically significant at final visit vs basal value (p< 0.0001). However, there was no significant difference in the score among groups. The cross indicates the mean, the outliers are designed with a full circle. |
At day 30, a reduction in OSDI score of 54.6 ± 23.4% (versus baseline score) was observed in BID, vs 56.2 ± 24.9% for QID, and 52.7 ± 20.9% for 6TD posology. The recovery of the OSDI score to normal values (<13 points) was detected in 51.4% of patients treated (50%, 48.6%, and 55.6% in BID, QID and 6TD, respectively). There was no significant difference among groups (Chi-square, p = 0.822), see Table 2.
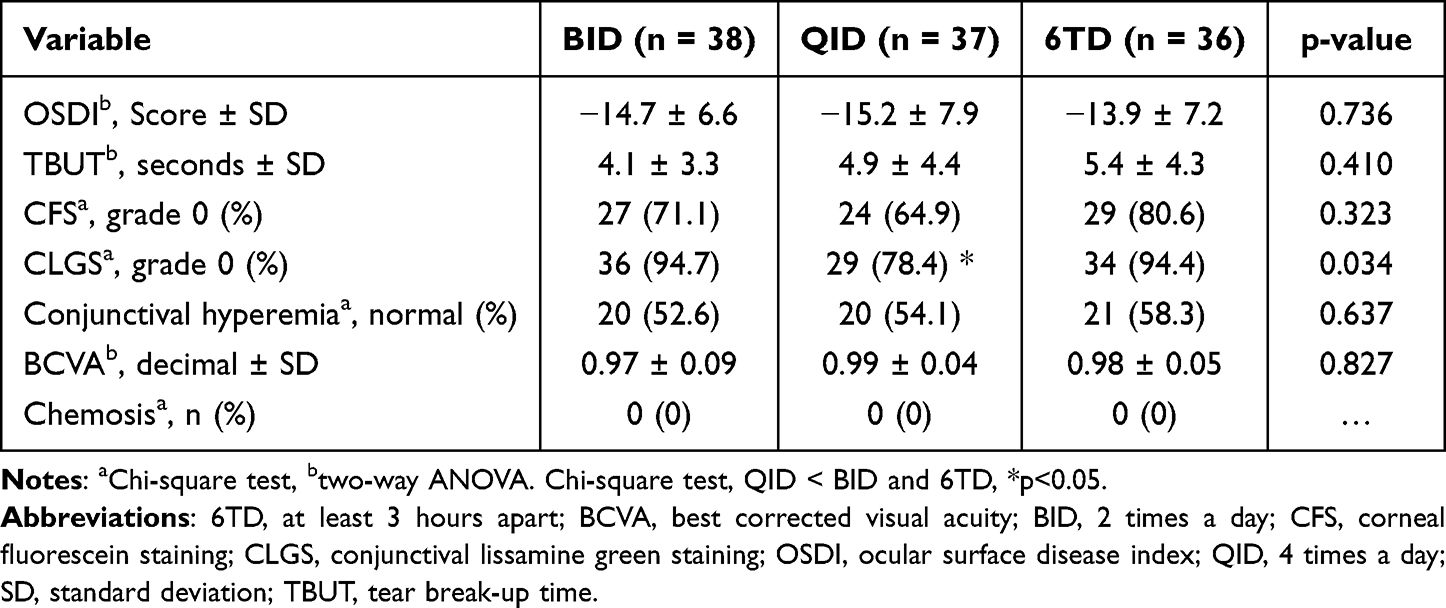 |
Table 2 Change from Baseline at 30-Day Follow-Up Visit |
Tear Break-Up Time (TBUT)
After 15 days of treatment, the mean TBUT was 9.0 ± 3.5 seconds for BID, 8.8 ± 2.7 seconds for QID, and 9.03 ± 3.1 seconds for the 6TD group. By day 30, the BID group had a mean TBUT of 9.8 ± 3.7 seconds for BID, 10.6 ± 4.3 seconds for QID, and 10.9 ± 4.3 seconds for 6TD group. This represented an increase of 4.1 ± 3.3 seconds for BID, 4.86 ± 4.4 seconds for QID, and 5.4 ± 4.3 seconds for the 6TD group compared to their respective baseline values. The findings of population analysis identified comparable values, with no significant differences among groups (factor posology, p = 0.693). However, the factor visit was significant (Day 30 vs day 15, p < 0.0001, 95% CI [3.78, 5.78]). Between-factor interaction was not significant (posology × visit day; p = 0.743), see Figure 3. The TBUT recovered to normal values (>10 seconds) in 50.5% of patients at the final visit; 39.5% for BID, 51.4% for QID, and 61.1% for the 6TD group. No significant differences were observed among groups (Chi-square, p = 0.175), see Table 2.
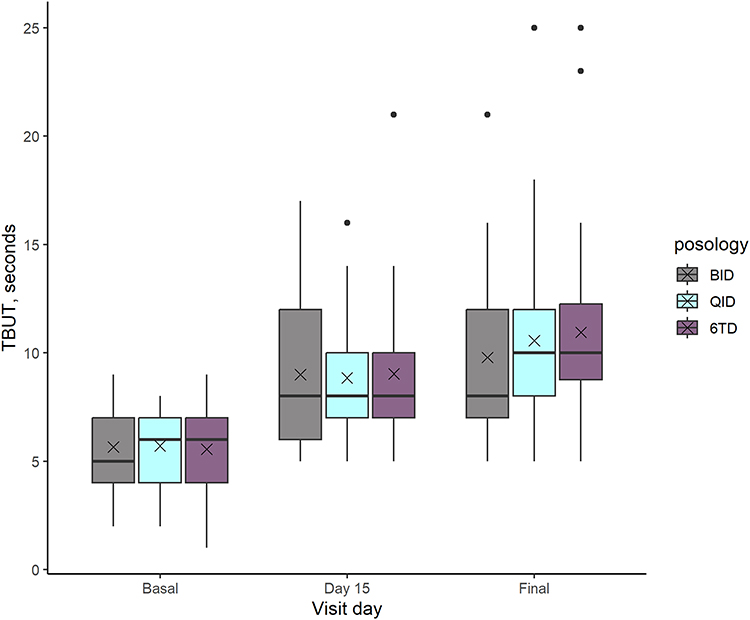 |
Figure 3 TBUT with fluorescein in seconds (n= 111). The increase in all groups was statistically significant after 15 and 30 days (p< 0.0001) compared to basal value. Though there was no significant difference in TBUT among groups. The cross indicates the mean, the outliers are designed with a full circle. |
Corneal Fluorescein and Conjunctival Lissamine Green Staining (CFS)
Compared to baseline, there was a significant increase in the CFS grade 0 (absent) cases in all dosages, the BID group had an increment of grade 0 to 47.4% of patients by day 15 and 71.1% by the final visit. For the QID group, it was 54.1% and 64.9%, respectively, while for the 6TD group it was 55.6% and 80.6%, respectively. There was no significant difference among groups for change from baseline at any time point (Chi-square, p-values; 0.330 and 0.320 at day 15 and day 30, respectively). The CFS converted to normal values (grade 0, no staining) in 72.1% of patients at the final visit, see Table 2.
The improvement of CLGS was similar in all groups (Chi-square, p = 0.702). The BID group had a grade of 0 in 63.2% of patients by day 15 and 94.7% by the final visit. For the QID group, posology it was 59.2% and 78.4%, respectively, and for the 6TD group it was 63.9% and 94.4%, respectively. At the final visit, the CLGS showed more significant improvements in the BID and 6TD groups than in the QID group (Chi-square, p = 0.034). The CLGS converted to normal values (grade 0, no staining) in 89.2% of patients at final visit, see Table 2.
Conjunctival Hyperemia
At day 15, there was a narrow reduction of conjunctival hyperemia in all groups. For the BID group, 39.5% had a grade 0 (normal), vs 48.6% and 33.3% for QID and 6TD, respectively. By the final visit, 52.6%, 54.1% and 58.3% for BID, QID and 6TD, respectively, showed grade 0 of conjunctival hyperemia. No significant differences were observed among groups at any time point (Chi-square, p-values; 0.605 and 0.637 at day 15 and day 30, respectively). The conjunctival hyperemia recovered to normal values in 55% of patients at the final visit, see Table 2.
Lastly, at the final visit, 30% of the patients had an OSDI score <13 and a TBUT ≥10 seconds. A total of 31 patients did not improve their OSDI and TBUT back to normal values, of which 21 were female and 71.4% being users of hormonal contraceptive drugs.
Safety
Chemosis
No patients presented chemosis before or after their respective posology group administration.
Best-Corrected Visual Acuity (BCVA)
The BCVA (decimal) did not change significantly from baseline to final visit in any of the groups (factor visit, F(2324) = 0.836, p = 0.434). However, there were significant differences for the mean value of BCVA among groups (factor posology, p = 0.003, 95% CI [0.01, 0.04]). The mean BCVA for the QID group was statistically better than the BID group; nevertheless, this may not be clinically relevant, see Table 2.
Adverse Events (AE)
During the intent-to-treat (ITT) analysis (n = 116) 31% (36/116) of the randomized patients reported at least one related, unexpected-AE. Of the total, 43.3% were described for BID, 28.3% for QID and 28.3% for 6TD posology groups. All of them were classified as mild. According to their causality assessment, 21.7% of AE were possible, 76.7% probable or likely, and 1.6% unlikely, without differences among posology groups (Chi-square, p = 0.159). The most common class of reported AE was blurry vision (18.3%), followed by product residue presence (16.7%), and abnormal sensation in eye (13.3%), without significant differences among groups (Chi-square, p = 0.583).
Discussion
The results of this study demonstrate that the topical use of 0.4% sodium hyaluronate 2, 4, or 6 times a day may alleviate clinical parameters and symptoms, as confirmed by TBUT and OSDI scores back within the range of normalcy in 50% of patients with mild-to-moderate DED after one month’s treatment. Additionally, this improvement seems to be less completely in woman within reproductive age range and using hormonal contraceptives.
LOF, an ocular lubricant composed of sodium hyaluronate apart from their rheological properties, exhibits mucoadhesive properties, makiing it ideal for DED, a disease that results in visual disturbance and tear-film instability.8,32,33 Lubricant eye drops are commonly prescribed pro re nata (PRN), or “as needed”; however, some studies have demonstrated that a fixed dose QID can improve DED symptoms more efficiently than a PRN scheme.14,34,35 The literature indicates that most lubricants may have similar efficacy in the management of DED. However, some inconsistencies in both study designs and dosing control in several trials represent a variability in lubricant application, ranging from 2 to over 6 instillations per day, and possibly correlating with DED severity when more applications were needed.36 In the current study, three dosing schemes were tested, BID, QID and 6TD in order to determine the impact of instillation frequency in signs and symptoms affecting patients with mild-to-moderate DED.
In DED, numerous tests are used to classify the disorder and to track change over time or with treatment, each test is impacted by the test performed previously.37 The analyzed variables included OSDI, TBUT, CFS, CLGS and conjunctival hyperemia. No correlation between OSDI, TBUT and sex was observed. Nevertheless, significant correlations among CFS, CLGS and conjunctival hyperemia were noted. Several studies showed a discordance between signs and symptoms of DED,14,31,38 while in our study a few statistically significant correlations were found only among signs of DED.
For all groups, the OSDI score was reduced by the end of the treatment period, in comparison to baseline values. The mean change from baseline to day 30 was −14.7 for BID, −15.2 for QID, and −13.9 for the 6TD group. Furthermore, OSDI was recovered to normal values (<13 points) in 51.4% of treated patients, with no significant difference among dosing schemes. Perhaps, patients with a more severe clinical presentation of DED show an additional beneficial effect from an increased frequency in eye drop administration.
For TBUT, recovery to normal values (>10 seconds) took place in 50.5% of patients by the final visit. CFS was restored to normal values (grade 0, no staining) in 72.1% of patients by the final visit, and CLGS reverted to grade 0, no staining, in 89.2%. Finally, 55% of patients presented absence of conjunctival hyperemia by the final visit.
No differences among groups were found for any of the evaluated parameters. It is worth mentioning that every patient included in this study improved their OSDI score and at least one of the evaluated signs (TBUT, CFS, CLGS, or conjunctival hyperemia) when compared to baseline, even when not all of them reached normal values. These results agree with those of Szczesna et al, who evaluated the effectiveness of common ocular lubricant treatment after one month of use.14
Regarding safety evaluations, no patients presented chemosis before or after their respective treatment. Concerning BCVA, the statistical differences observed among posology groups were without clinical relevance. For the AE evaluation, the most common class of reported AE was blurry vision, followed by the presence of product residue and abnormal sensation in eye, without differences among groups. These are expected AE related to eye drops in general, but these do not entail any additional safety risk associated with the formulation employed in this study.
Preclinical studies have identified the relationship between testosterone regulation and the expression of thousands of genes in the lacrimal and meibomian glands of ovariectomized and orchiectomized mice, suggesting that sex steroids may induce sex-specific effects in the lacrimal and meibomian glands.39–41
Furthermore, the presence of receptors for both male and female sex hormones in human corneal epithelial cells obtained at autopsy of both genders has been established previously through reverse transcription-polymerase chain reaction.42 This substantiates the fact that preclinical findings could extend to a clinical setting where hormonal levels and their modification through oral contraceptives may impact the signs and symptoms related to dry eye.41 Galiano et al demonstrated that postmenopausal women are at risk for DED, and that low levels of sex steroids such 17-β-oestradiol, oestrone and total testosterone, are related to the development of evaporative dry eye.4
There are not many available clinical studies focused on evaluating the role of oral contraceptives in dry eye prevalence and/or response to treatment. However, in a study published by Wróbel-Dudzinska et al, in which 312 university students were evaluated for dry eye prevalence and risk-factor preponderance, a total of 219 were women, of which nearly 22% (47 out of 219) declared oral contraceptive use, the authors considered oral contraceptive use a risk for dry eye.43
In the current study, a total of 67.6% of included patients were female, and most of them within reproductive age (65.3% were users of oral contraceptives), with an approximate mean age of 40 years. When considering both signs and symptoms related to DED, at the final visit, 30% of the patients had both an OSDI score <13 and a TBUT ≥10 seconds. Of the 31 patients who did not improve their OSDI and TBUT to normal values, 21 were female and 71.4% of them were users of oral contraceptives.
Sharma et al published a study in which 50 women using oral contraceptives were compared to 50 controls, measuring serum testosterone and dehydroepiandrosterone levels as well as clinical signs related to dry eye such as Schirmer’s test and TBUT. The results obtained demonstrated a decrease in androsterone levels in women using oral contraceptives when compared to the similar-age group where no hormonal treatment was used. Furthermore, both tear secretion (13 vs 31 mm/5 min, respectively) and stability (11.9 vs 13.6 sec, respectively) were significantly reduced in the study group.44
Also, Boga et al evaluated 36 normally menstruating and 36 oral contraceptive-using women. Daily, for a total of 40 days, the subjects answered the Instant Ocular Symptoms Survey, with the purpose of evaluating the presence and variability of dry eye symptoms over a complete menstrual cycle compared in the two groups previously described. The results found a significant increase in symptomatology on day 2 of the cycle, as well as significantly higher general symptom scores for the oral contraceptive group.45
The present study’s results agree with these previous findings, with an even higher percentage of oral contraceptive users diagnosed with dry eye. Among the many risk factors associated with DED, oral contraceptive use has been proposed as a cause of increased symptoms of dry eye and contact lens intolerance. Even though the relationship between estrogen supplementation in premenopausal women and its effects on the ocular surface is still to be confirmed, the association between oral contraceptives and DED has been described anecdotally.5,6
Furthermore, there is precedent of the clinical relationship between oral contraceptive use and dry eye.44,45 Beyond this, the data obtained in this study put forth the fact that women within reproductive age and exposed to oral contraceptives were less prone to improve both for signs and symptoms related to DED than other population groups treated for this condition with 71.4% of patients who did not improve OSDI and TBUT to normal values being users of hormonal contraceptives.
Some of the weaknesses of this study include the fact that it was not designed specifically for the evaluation of this correlation, and no control group of women without the use of oral contraceptives was included. Moreover, only mild-to-moderate DED patients were included, which could have limited the contrast of benefits of applying ocular lubricants less or more frequently than the standard QID scheme. The lack of a placebo (saline) control group should limit the observed changes in symptoms and signs over the month of treatment due to the treatment effect of the eye drop. However, it has been previously reported that sodium hyaluronate eye drops may be superior to saline for the treatment of DED.46–48 The fact that the use of TBUT with fluorescein may be influenced by the amount of colorant deposited, while noninvasive automated measures are reported to provide unbiased results, could also be considered a limitation.14,49
Conclusion
In conclusion, the topical use of preservative-free 0.4% sodium hyaluronate 2, 4 or 6 times a day may alleviate clinical parameters and symptoms, as demonstrated by TBUT and OSDI scores back within the range of normalcy in 50% of patients with mild-to-moderate DED after one month’s treatment. This improvement seems to be less ubiquitous in patients within reproductive age range and using oral contraceptives.
Future DED studies recruiting premenopausal women exposed to oral contraceptives could shed light on the clinical impact this disease has on such population, as well as the extent of beneficial effects that ocular lubricant treatment may present on both signs and symptoms.
Abbreviations
6TD, 6 times a day; AE, adverse events; BCVA, best-corrected visual acuity; BID, 2 times a day; CFS, corneal fluorescein staining; CLGS, conjunctival lissamine green staining; DED, dry eye disease; FPFV, first patient first visit; LPLV, last patient last visit; OSDI, ocular surface disease index; QID, 4 times a day; TBUT, tear break-up time.
Data Sharing Statement
The dataset generated during and/or analyzed for the current study is available in the Open Science Framework (https://osf.io) repository as DOI 10.17605/OSF.IO/YDRZQ.
Acknowledgments
Phase II clinical study to evaluate the efficacy of multidose Lagricel® Ofteno ophthalmic solution applied in three different dosage schemes as treatment to mild-to-moderate dry eye (NCT0704531) was conducted in six centers in Mexico (Jalisco, Mexico City, Veracruz, and Yucatan). The study protocol and informed consent form were approved by their respective Institutional Review Boards as follows: Instituto Tecnológico de Estudios Superiores de Monterrey, Comité de ética en investigación de la escuela de medicina del Instituto Tecnológico y de Estudios Superiores de Monterrey, Centro de Investigación Clínica Acelerada S.C., Hospital la Misión, Sociedad Administradora de Servicios de Salud S.C., and Comité de Clínica Bajío CLINBA S.C.
We thank the participants in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Laboratorios Sophia, S.A. de C.V. (Zapopan, Jalisco, Mexico). MVP, SRA, and OMO are employees of Laboratorios Sophia, S.A. de C.V. The sponsor provided support in the form of salaries for authors (MVP, SRA, and OMO), this does not alter our adherence to the Good Publication Practice guidelines for pharmaceutical companies (GPP3) policies on sharing data and materials. The authors report no other conflicts of interest in this work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Craig JP, Nichols KK, Akpek EK, et al. TFOS DEWS II Definition and Classification Report. Ocul Surf. 2017;15(3):276–283. doi:10.1016/j.jtos.2017.05.008
2. Stapleton F, Alves M, Bunya VY, et al. TFOS DEWS II Epidemiology Report. Ocul Surf. 2017;15(3):334–365. doi:10.1016/j.jtos.2017.05.003
3. Baudouin C, Messmer EM, Aragona P, et al. Revisiting the vicious circle of dry eye disease: a focus on the pathophysiology of meibomian gland dysfunction. Br J Ophthalmol. 2016;100(3):300–306. doi:10.1136/bjophthalmol-2015-307415
4. Gagliano C, Caruso S, Napolitano G, et al. Low levels of 17-β-oestradiol, oestrone and testosterone correlate with severe evaporative dysfunctional tear syndrome in postmenopausal women: a case–control study. Br J Ophthalmol. 2014;98(3):371–376. doi:10.1136/bjophthalmol-2012-302705
5. Sullivan DA, Rocha EM, Aragona P, et al. TFOS DEWS II Sex, Gender, and Hormones Report. Ocul Surf. 2017;15(3):284–333. doi:10.1016/j.jtos.2017.04.001
6. Warren DW, Azzarolo AM, Huang ZM, et al. Androgen Support of Lacrimal Gland Function in the Female Rabbit. Int J Med. 1998:89–93. doi:10.1007/978-1-4615-5359-5_11
7. Versura P, Giannaccare G, Campos EC. Sex-Steroid Imbalance in Females and Dry Eye. Curr Eye Res. 2015;40(2):162–175. doi:10.3109/02713683.2014.966847
8. Weng J, Fink MK, Sharma A. A Critical Appraisal of the Physicochemical Properties and Biological Effects of Artificial Tear Ingredients and Formulations. Int J Mol Sci. 2023;24(3):2758. doi:10.3390/ijms24032758
9. Kathuria A, Shamloo K, Jhanji V, Sharma A. Categorization of Marketed Artificial Tear Formulations Based on Their Ingredients: a Rational Approach for Their Use. J Clin Med. 2021;10(6):1289. doi:10.3390/jcm10061289
10. You IC, Li Y, Jin R, Ahn M, Choi W, Yoon KC. Comparison of 0.1%, 0.18%, and 0.3% Hyaluronic Acid Eye Drops in the Treatment of Experimental Dry Eye. J Ocular Pharmacol Therapeutics. 2018;34(8):557–564. doi:10.1089/jop.2018.0032
11. Pisárčik M, Bakoš D, Čeppan M. Non-Newtonian properties of hyaluronic acid aqueous solution. Colloids Surf a Physicochem Eng Asp. 1995;97(3). doi:10.1016/0927-7757(95)03097-W
12. Walsh K, Jones L. The use of preservatives in dry eye drops. Clin Ophthalmol. 2019;13. doi:10.2147/OPTH.S211611
13. Ribeiro MVMR, Barbosa FT, Ribeiro LEF, Sousa-Rodrigues CF, Ribeiro EAN. Effectiveness of using preservative-free artificial tears versus preserved lubricants for the treatment of dry eyes: a systematic review. Arq Bras Oftalmol. 2019;82(5). doi:10.5935/0004-2749.20190097
14. Szczesna-Iskander DH, Muzyka-Wozniak M, Llorens Quintana C. The efficacy of ocular surface assessment approaches in evaluating dry eye treatment with artificial tears. Sci Rep. 2022;12(1):21835. doi:10.1038/s41598-022-26327-3
15. Jones L, Downie LE, Korb D, et al. TFOS DEWS II Management and Therapy Report. Ocular Surface. 2017;15(3). doi:10.1016/j.jtos.2017.05.006
16. Rodriguez-Garcia A, Babayan-Sosa A, Ramirez-Miranda A, et al. A Practical Approach to Severity Classification and Treatment of Dry Eye Disease: a Proposal from the Mexican Dry Eye Disease Expert Panel. Clin Ophthalmol. 2022;16:1331–1355. doi:10.2147/OPTH.S351898
17. Wolffsohn JS, Arita R, Chalmers R, et al. TFOS DEWS II Diagnostic Methodology report. Ocular Surface. 2017;15(3). doi:10.1016/j.jtos.2017.05.001
18. Akpek EK, Amescua G, Farid M, et al. Dry Eye Syndrome Preferred Practice Pattern®. Ophthalmology. 2019;126(1):286–P334. doi:10.1016/j.ophtha.2018.10.023
19. Bron AJ. Methodologies to Diagnose and Monitor Dry Eye Disease: report of the Diagnostic Methodology Subcommittee of the International Dry Eye WorkShop (2007). Ocul Surf. 2007;5(2):108–152. doi:10.1016/S1542-0124(12)70083-6
20. Bron AJ, Evans VE, Smith JA. Grading Of Corneal and Conjunctival Staining in the Context of Other Dry Eye Tests. Cornea. 2003;22(7):640–650. doi:10.1097/00003226-200310000-00008
21. Eom Y, Lee JS, Keun Lee H, Myung Kim H, Suk Song J. Comparison of conjunctival staining between lissamine green and yellow filtered fluorescein sodium. Canadian J Ophthalmol. 2015;50(4):273–277. doi:10.1016/j.jcjo.2015.05.007
22. Singh RB, Liu L, Anchouche S, et al. Ocular redness – I: etiology, pathogenesis, and assessment of conjunctival hyperemia. Ocul Surf. 2021;21:134–144. doi:10.1016/j.jtos.2021.05.003
23. Efron N. Grading scales for contact lens complications. Ophthalmic Physiological Optics. 1998;18(2):182–186. doi:10.1016/S0275-5408(97)00066-5
24. Dang TT, Nguyen TH, Ho TB. Causality Assessment of Adverse Drug Reaction: controlling Confounding Induced by Polypharmacy. Curr Pharm Des. 2019;25(10):1134–1143. doi:10.2174/1381612825666190416115714
25. Naranjo CA, Busto U, Sellers EM, et al. A method for estimating the probability of adverse drug reactions. Clin Pharmacol Ther. 1981;30(2):239–245. doi:10.1038/clpt.1981.154
26. Armstrong RA, Davies LN, Dunne MCM, Gilmartin B. Statistical guidelines for clinical studies of human vision. Ophthalmic Physiological Optics. 2011;31(2):123–136. doi:10.1111/j.1475-1313.2010.00815.x
27. Karakosta A, Vassilaki M, Plainis S, Elfadl NH, Tsilimbaris M, Moschandreas J. Choice of Analytic Approach for Eye-Specific Outcomes: one Eye or Two? Am J Ophthalmol. 2012;153(3):571–579.e1. doi:10.1016/j.ajo.2011.08.032
28. Armstrong RA. Statistical guidelines for the analysis of data obtained from one or both eyes. Ophthalmic Physiological Optics. 2013;33(1):7–14. doi:10.1111/opo.12009
29. Pinto-Fraga J, López-de la Rosa A, Blázquez Arauzo F, Urbano Rodríguez R, González-García MJ. Efficacy and Safety of 0.2% Hyaluronic Acid in the Management of Dry Eye Disease. Eye Contact Lens. 2017;43(1):57–63. doi:10.1097/ICL.0000000000000236
30. Chow SC, Wang H, Shao J. Sample Size Calculations in Clinical Research. Chapman and Hall/CRC; 2007; doi:10.1201/9781584889830
31. Bartlett J, Keith M, Sudharshan L, Snedecor S. Associations between signs and symptoms of dry eye disease: a systematic review. Clin Ophthalmol. 2015;1719. doi:10.2147/OPTH.S89700
32. Abatangelo G, Vindigni V, Avruscio G, Pandis L, Brun P. Hyaluronic Acid: redefining Its Role. Cells. 2020;9(7):1743. doi:10.3390/cells9071743
33. Liao YH, Jones SA, Forbes B, Martin GP, Brown MB. Hyaluronan: pharmaceutical Characterization and Drug Delivery. Drug Deliv. 2005;12(6):327–342. doi:10.1080/10717540590952555
34. Asbell P, Vingrys AJ, Tan J, et al. Clinical Outcomes of Fixed Versus As-Needed Use of Artificial Tears in Dry Eye Disease: a 6-Week, Observer-Masked Phase 4 Clinical Trial. Investigative Ophthalmol Visual Sci. 2018;59(6):2275. doi:10.1167/iovs.17-23733
35. Baiza-Durán LM, Muñoz-Villegas P, Sánchez-Ríos A, Olvera-Montaño O. Efficacy and Safety of an Ophthalmic DMPC-Based Nanoemulsion in Patients with Dry Eye Disease: a Phase I/II Randomized Clinical Trial. J Ophthalmol. 2023;2023:1–9. doi:10.1155/2023/1431473
36. Pucker AD, Ng SM, Nichols JJ. Over the counter (OTC) artificial tear drops for dry eye syndrome. Cochrane Database Sys Rev. 2016;2016(2). doi:10.1002/14651858.CD009729.pub2
37. Nichols KK, Mitchell GL, Zadnik K. The Repeatability of Clinical Measurements of Dry Eye. Cornea. 2004;23(3):272–285. doi:10.1097/00003226-200404000-00010
38. Johnson ME. The Association Between symptoms of Discomfort and signs in Dry Eye. Ocul Surf. 2009;7(4):199–211. doi:10.1016/S1542-0124(12)70187-8
39. Sullivan DA, Jensen RV, Suzuki T, Richards SM. Do sex steroids exert sex-specific and/or opposite effects on gene expression in lacrimal and meibomian glands? Mol Vis. 2009;15:1553–1572.
40. Schirra F, Suzuki T, Richards SM, et al. Androgen Control of Gene Expression in the Mouse Meibomian Gland. Investigative Ophthalmol Visual Sci. 2005;46(10):3666. doi:10.1167/iovs.05-0426
41. Truong S, Cole N, Stapleton F, Golebiowski B. Sex hormones and the dry eye. Clin Exp Optom. 2014;97(4):324–336. doi:10.1111/cxo.12147
42. Suzuki T, Kinoshita Y, Tachibana M, et al. Expression of sex steroid hormone receptors in human cornea. Curr Eye Res. 2001;22(1):28–33. doi:10.1076/ceyr.22.1.28.6980
43. Wróbel-Dudzińska D, Osial N, Stępień PW, Gorecka A, Żarnowski T. Prevalence of Dry Eye Symptoms and Associated Risk Factors among University Students in Poland. Int J Environ Res Public Health. 2023;20(2):1313. doi:10.3390/ijerph20021313
44. Sharma A, Porwal S, Tyagi M. Effect of oral contraceptives on tear film in reproductive age group women. Int J Reprod Contracept Obstet Gynecol. 2018;7(3):860. doi:10.18203/2320-1770.ijrcog20180410
45. Boga A, Stapleton F, Briggs N, Golebiowski B. Daily fluctuations in ocular surface symptoms during the normal menstrual cycle and with the use of oral contraceptives. Ocul Surf. 2019;17(4):763–770. doi:10.1016/j.jtos.2019.06.005
46. Ang BCH, Sng JJ, Wang PXH, Htoon HM, Tong LHT. Sodium Hyaluronate in the Treatment of Dry Eye Syndrome: a Systematic Review and Meta-Analysis. Sci Rep. 2017;7(1):9013. doi:10.1038/s41598-017-08534-5
47. Yang YJ, Lee WY, jin KY. A Meta-Analysis of the Efficacy of Hyaluronic Acid Eye Drops for the Treatment of Dry Eye Syndrome. Int J Environ Res Public Health. 2021;18(5):2383. doi:10.3390/ijerph18052383
48. Johnson ME, Murphy PJ, Boulton M. Effectiveness of sodium hyaluronate eyedrops in the treatment of dry eye. Graefe’s Arch Clin Exp Ophthalmol. 2006;244(1):109–112. doi:10.1007/s00417-005-0028-1
49. Abdelfattah NS, Dastiridou A, Sadda SR, Lee OL. Noninvasive Imaging of Tear Film Dynamics in Eyes With Ocular Surface Disease. Cornea. 2015;34(Supplement 10):S48–S52. doi:10.1097/ICO.0000000000000570
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.