")
Back to Journals » Risk Management and Healthcare Policy » Volume 15
The Effect of Social Norms on Physicians’ Intentions to Use Liver Cancer Screening: A Cross-Sectional Study Using Extended Theory of Planned Behavior
Received 22 November 2021
Accepted for publication 27 January 2022
Published 9 February 2022 Volume 2022:15 Pages 179—191
DOI https://doi.org/10.2147/RMHP.S349387
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Qingwen Deng,1,2 Wenbin Liu1
1Department of Health Management, School of Public Health, Fujian Medical University, Fuzhou, 350122, People’s Republic of China; 2School of Public Health, Fudan University, Shanghai, 200032, People’s Republic of China
Correspondence: Wenbin Liu, Tel +86 13799983766
, Email [email protected]
Background: Liver cancer is a globally acknowledged threat to public health, and there is a critical and urgent need to determine factors associated with the use of liver cancer screening and to further promote its use.
Purpose: To examine whether the extended theory of planned behavior (TPB) incorporating social norms predicts physicians’ intentions to use liver cancer screening and to identify the associated factors quantitatively, using contrast-enhanced ultrasound (CEUS) as an example.
Methods: A research framework was established by adding social norms to the TPB, based on which the questionnaire for this study was developed. Through multistage random sampling, a cross-sectional questionnaire survey was conducted among 292 physicians in Fujian and Jiangxi provinces. Due to the multicollinearity problem of the data, ridge regression was applied to determine the influencing factors of physicians’ intentions to use CEUS.
Results: Most participants (87.30%) reported that they were willing to use liver cancer screening in their clinical practice. The scores of TPB variables were generally higher than those of social norms variables. Ridge regression results indicated that the proposed model was explanatory, which has accounted for 73.5% of the total variance in physicians’ intentions. Analyses also illustrated the significant role of TPB variables (attitude and perceived behavioral control) and social norms variables (personal norms, organizational norms, and industrial norms) on physicians’ intentions to use CEUS.
Conclusion: The study extended the TPB by including the concepts of social norms, which is not only conducive to expanding the knowledge of factors associated with physicians’ intentions to use liver cancer screening, but also provides implications for developing strategies to promote the use of certain health services or products, such as playing the role of core members, holding panel meetings, and establishing information push systems.
Keywords: social norms, intention, liver cancer, screening, physicians
Introduction
With its incidence on the rise over the past few decades, liver cancer is one of the most serious malignant tumors globally, as well as the current second leading cause of cancer-related deaths.1 Worse of all, once clinical manifestations appear, most patients are already in advanced stages, where has a low 5-year survival rate, poor quality of life, and unaffordable burden of disease.2,3 The situation is particularly acute in China, which accounts for more than half of the world’s new liver cancer cases and deaths each year.4 Under the critical situation of liver cancer prevention and treatment, it is urgent to promote the use of liver cancer screening, which will facilitate early diagnosis and treatment of liver cancer, further improve patients’ survival rate and quality of life, and reduce the burden on the health system. Although a growing body of research aims at better understanding and increasing the use of cancer screening5,6 and the fact that a fairly large number of cases can avoid advanced cancer through screening is well-established,7 it remains challenging for researchers and policymakers to persuade or motivate the public (including patients and physicians) to adopt cancer screening. In order to design targeted measures that promote the use of cancer screening, it is of great theoretical and practical significance to identify the influencing factors that can be intervened. It is to this end that this study hopes to provide some clues.
Researchers have been trying to use various theories and models to explain the rational mechanisms of human behaviors, such as the Theory of planned behavior (TPB) developed by Ajzen,8 which is a representative theory in the field of technology or behavior adoption and is one of the most influential and widely used theories to predict behavioral intentions.9 It presumes that people’s particular behavior can be predicted and explained via their intentions. In turn, the intentions are functioned by three elements, namely, attitude, subjective norms, and perceived behavior control.8 Attitude reflects the perception or evaluation of performing a particular behavior. Perceived behavior control is defined as the perception of the controllable extent of performing a specific behavior. Subjective norms are perceived social pressures that whether people important to individuals think the behavior should be performed. To date, the TPB has been applied in considerable research about health professionals’ intentions,10 including the acceptance of innovative health technology,11,12 and the adherence to clinical guidelines.13 Moreover, numerous TPB studies have explained over fifty percent of the total variance of intentions.14–16
According to Ajzen, “TPB is principally open to the inclusion of additional predictors if it can be shown that they capture a significant proportion of the variance”.8 That is, the additional predictors are allowed in the TPB to improve the explanatory power in intentions. For instance, social environment, not least in the context of current concerns about the social environment factors of health issues.17,18 In addition to the direct application of TPB, several studies have shown that TPB has been extended in different areas with success.19–23 To some extent, subjective norms in the TPB are virtually a kind of social norm.24,25 Social norms shape people’s motivation and behavior based on the social environment.26 It can be understood as the perceived prevalence of others’ behavior and the perceptions of how others think about or evaluate a behavior,27 which may come from multiple resources, such as the people, organizations, or industries around us. The perceptions from those around us are personal norms, namely subjective norms, which have been addressed in the TPB. The influence of the perceptions from the organization and the industry on the individual can be called the organizational norms and the industrial norms, representing the behavioral readiness of the whole members of the hospital and the competition pressure from the peers in the industry, respectively. In general, it’s hard to make decisions that are not influenced by the persons and various environmental elements around us, and people adjust their behavior and conform to the social expectation by information learned from observing others.28
To the best of our knowledge, the research object and content were relatively single and fixed in previous studies about cancer screening intentions. On the one hand, previous studies mainly look at the patient level, as a number of studies have been conducted to investigate the intentions to use screening of different cancer groups, such as cervical cancer,29 breast cancer,30 prostate cancer,31 and colorectal cancer,32 etc., but rarely focus on the health services provider (ie, physicians). On the other hand, in a few studies of cancer screening intentions for physicians, they have focused more on individual-level internal factors (ie, physicians’ attitudes, beliefs, knowledge,33,34 and nonprofessional experiences35) than on the influence of organizational and industry settings on individuals, which can fall under the scope of social norms. It’s noteworthy that although recently the social norms have received particular attention as the determinants of the adoption of certain behaviors, including cancer screening,6,36 most studies set forth only a single level of social norms: either personal normative beliefs and mimetic pressures at the level of the personal norms,37,38 or institutional pressures and organizational culture at the level of the organizational norms,39,40 or industry competition at the level of the industrial norms.41 The comprehensive consideration of these three aspects is necessary, especially for the physicians in public hospitals,42 given the strong reliance of public hospital physicians on their hospitals and the industrial environment may lead to the internalization of organization norms and industrial norms that contribute greatly to their decision-making.43
Therefore, given the value of cancer screening intention studies for cancer prevention and control practices, coupled with on the paucity of such studies targeting physicians and lack of discussion of perceived norms other than the individual, this study aims to determine the predictors of the intentions to use liver cancer screening from the physicians’ perspective and the influence of the potential social norms from the personal, organizational and industrial level. To make the study more pertinent and focused, contrast-enhanced ultrasound (CEUS), one of the confirmed effective screening technology for liver cancer, will be taken as an example to conduct the survey. This study is promising for bridging the literature gap about the factors affecting physicians’ intentions to use liver cancer screening from the perspective of health services providers. The findings will not only provide direct guidance for giving full play to the role of social norms in promoting the use of CEUS and other liver cancer screening, but also have several implications for expanding the use of other health services/products.
Materials and Methods
Theoretical Framework
Based on the existing literature and the context of CEUS use, we developed a research framework that originated from the TPB and the concepts of social norms, as shown in Figure 1. The TPB includes some important elements such as attitude, perceived behavioral control, and subjective norms. Social norms are explained by three aspects: personal norms (namely the variable of “subjective norms” mentioned above, it is the intersection of TPB and social norms), organizational norms (“hospital culture” and “technology sharing” were seen as measurement variables because both of which reflect the overall tendency exhibited by the hospital as an organization and in accordance with the connotation of social norms), and industrial norms (“industry pressure” was chosen as the measurement variable because industry pressure is the physicians’ perception of technical tendencies projected from the industry environment, and it also conforms to the connotation of social norms). Demographic characteristics such as province, gender, age, education level, professional title, administration position and years in practice, were included as covariates.
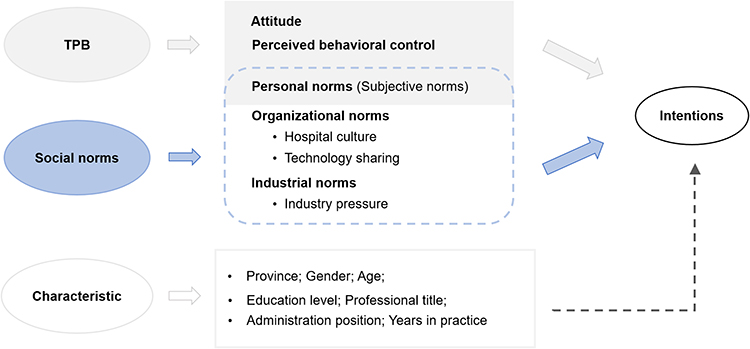 |
Figure 1 The research framework of physicians’ intentions to use liver cancer screening. |
Survey Instrument
For the data collection, a structured questionnaire with 28 items was developed on the basis of our research framework. Questions were derived from the previous literature, which are rationalized in this paper to fit the characteristics of CEUS. The questionnaire was divided into four parts: (1) demographic characteristics of participants, including six items such as sex, age, education, professional title, department, and years in practice. (2) Intentions to use CEUS.8 To measure the behavioral intentions, physicians were asked three items about the degree to which they would be willing to use, learn, and recommend CEUS in their practice. (3) The scale of TPB.8 Nine items proposed by the TPB were used to capture attitude, subjective norms, and perceived behavioral control, and the items were restated to fit the practical context of CEUS. (4) The scale of social norms.44–46 For the subjective norms that had been included in the TPB scale for measurement, this part of ten questions focused on measuring organization norms and industrial norms. Organizational norms were measured by two dimensions of hospital culture and technology sharing, while industrial norms were measured by the dimension of industry pressure. Items in part 2 to part 4 were rated on a five-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree). Table 1 provides the number of items of the dimension, sample questions, and Cronbach’s α for the dimensions and the questionnaire. The detailed questionnaire is available in Supplementary File. The results of the reliability and validity test showed that the questionnaire has satisfactory reliability and validity. Specific results are also available in Supplementary File.
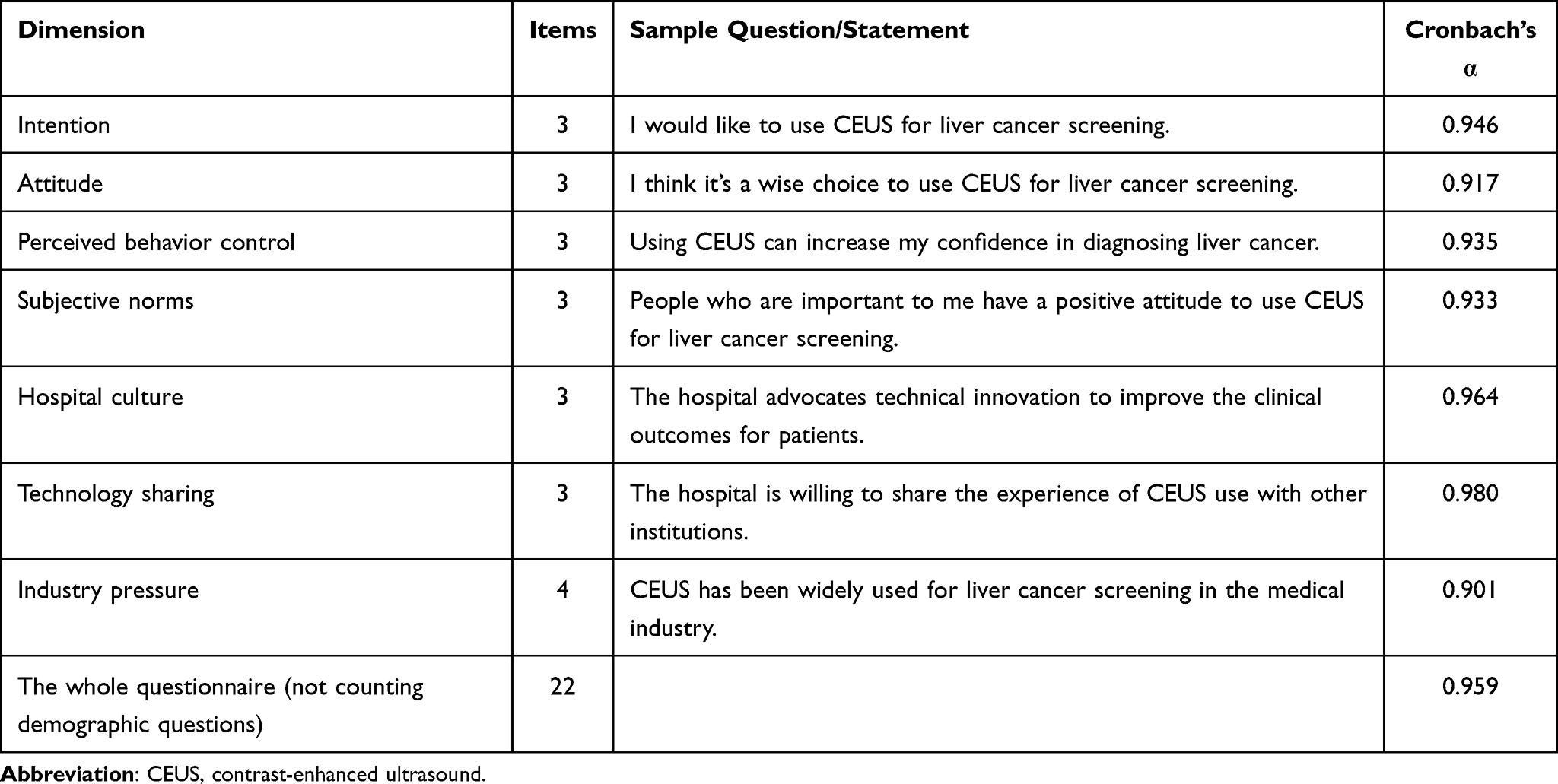 |
Table 1 Dimensions and the Sample Questions of the Questionnaire |
Sample and Data Collection
From February to August 2019, we conducted a cross-sectional survey in China using a multistage sampling method. Firstly, based on the latest average incidence of liver cancer in China (26.92/100,000),47 Fujian and Jiangxi province were randomly selected from the provinces with a high and low incidence of liver cancer, respectively (the incidence of liver cancer in Fujian and Jiangxi were 32.18/100,000 and 23.80/100,000, respectively).48,49 Secondly, since almost all health institutions are included in different medical alliances under the context of the implementation of hierarchical health system in China, we listed all medical alliances in each province as the sampling frame. Two medical alliances were randomly selected from each province. Thirdly, a sampling frame was made to list all health institutions of the four included medical alliances. Half of the health institutions within each medical alliance were randomly selected. Finally, physicians in these health institutions who meet the following criteria were included as the participants: (1) work in liver disease-related departments, such as the department of hepatology, oncology, infection, gastroenterology, interventional medicine, radiotherapy, general surgery, and traditional Chinese medicine, (2) have knowledge of CEUS, (3) agree to participate in this study. With the support of selected health institutions, the distribution of the questionnaires was accompanied by a trained coordinator to introduce the study purpose. Participation in the study was voluntary and anonymous, and informed consent was obtained from all participants.
Each medical alliance was expected to investigate 5~8 health institutions, and four medical alliances in two provinces would include 20~30 medical institutions. Each health institution would investigate 10~20 physicians on average. At least a total of 200 physicians were approached, which can meet the sample size requirement that at least five times the survey question.50
Statistical Analysis
Invalid questionnaires, including those that were incomplete or provided the same responses for all items or with many missing values, were eliminated. SPSS 21.0 software program was used as the main statistical tool to analyze the data. Firstly, the characteristics of the participants were described. Descriptive analyses were performed to represent categorical variables by frequencies and percentages, and continuous variable scores were represented by means and standard deviations (SD). Independent t-tests were used in the comparison of physicians’ intentions scores of two groups for demographic characteristics; variance analyses were performed in the comparison of three or more groups, and further post-hoc tests were performed when the results showed significant differences, with the Tukey method chosen if the number of cases between groups was equal and Scheffe method chosen if the number of cases between groups was not equal. The dimension score was calculated as the sum of the scores of each item divided by the number of items, and the percentage with a positive score of each dimension was obtained by dividing the number of participants who scored above 3 of this dimension by the total participants. Secondly, Pearson correlation was used to assess the relationship between physicians’ intentions to use CEUS and its potential determinants. Also, correlation analysis results are the basis of collinearity diagnostics. When the correlation coefficient is greater than 0.7, multicollinearity can be considered.51,52 Finally, if multicollinearity exists, ridge regression rather than traditional multiple linear regression, a proper technique enabling regression coefficients more stable in the case of multicollinearity,53 will be chosen to produce the estimates in the next analysis to determine the influencing factors of physicians’ intentions to use CEUS. Statistical significance was set at P < 0.05.
Patient and Public Involvement
Patients and the public were not involved in the design of the study, or in the recruitment to and conduct of the study.
Results
Characteristics of the Sample
A total of 329 questionnaires were distributed. After excluding invalid questionnaires, 292 were included in the analysis, with a valid response rate of 88.75%. The characteristics of the participants are presented in Table 2. Among the participants, 65.07% were males, 86.64% were under 45 years old, 93.84% reported having a bachelor’s degree or above, 76.37% had a junior or intermediate title, and 82.88% had no administration role. Participants with less than 15 years of practice accounted for 87.33%. t-tests and variance analyses showed that no statistically significant effect of characteristics other than age on physicians’ intentions to use CEUS (P > 0.05). Post-hoc analysis further revealed that physicians aged 35~44 years scored significantly higher on intentions to use CEUS than those under the age of 35.
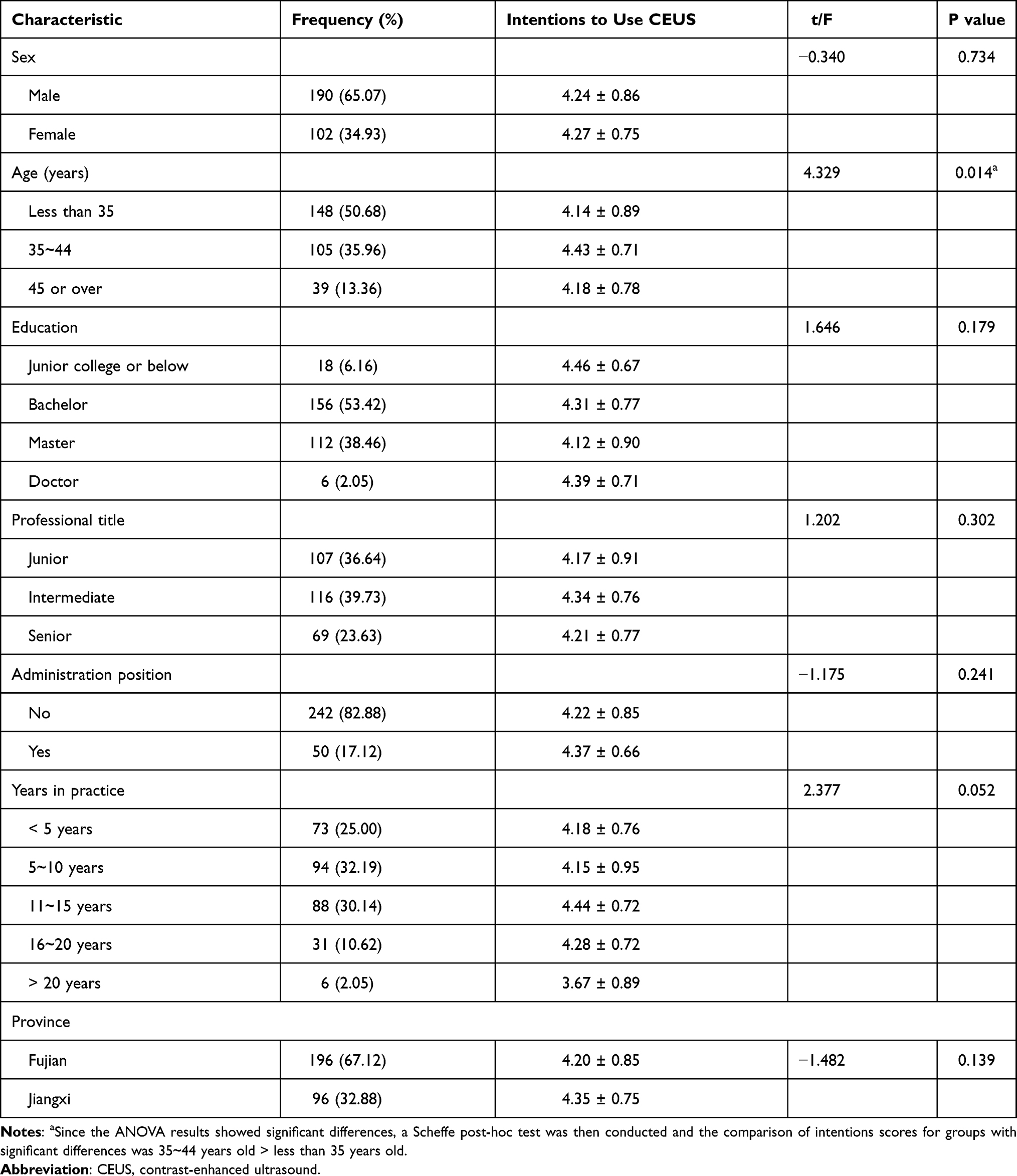 |
Table 2 Characteristics of the Sample Physicians and Variance Analysis of Physicians’ Intentions to Use CEUS (n=292) |
Of the participants, 87.30% reported that they intended to use liver cancer screening in their clinical practices, meaning 87.30% of potential adopters. The scores (mean ± SD) for each variable and the percentage of participants who had positive scores are presented in Table 3. The majority of participants had a positive score on all dimensions. Attitude and perceived behavior control scored 4.21 ± 0.83 and 4.21 ± 0.80. Subjective norms, hospital culture, technology sharing and industry pressure respectively scored 4.02 ± 0.95, 4.07 ± 1.07, 4.04 ± 1.09 and 3.78 ± 0.93. The scores of TPB variables were generally higher than those of social norms variables. Among them, the attitude has the highest proportion of positive responses, while industry pressure has the lowest proportion of positive responses.
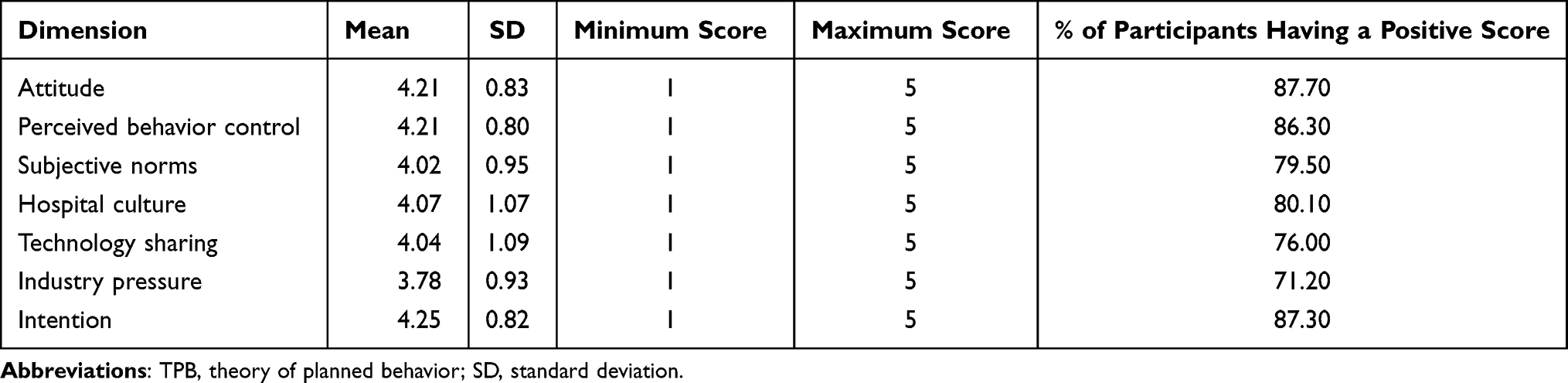 |
Table 3 Mean Scores for the Dimensions of the TPB Variables and Social Norms Variables |
Relationships Between the Intentions and Its Potential Determinants
As shown in Table 4, all potential determinants were positively correlated with physicians’ intentions to use CEUS (r = 0.462 to 0.860, P < 0.01). Some predictor variables were highly correlated (including attitude and perceived behavior control, attitude and subjective norms, perceived behavior control and subjective norms, hospital culture, and technology sharing), reaching the common threshold of multicollinearity of 0.7.46,47
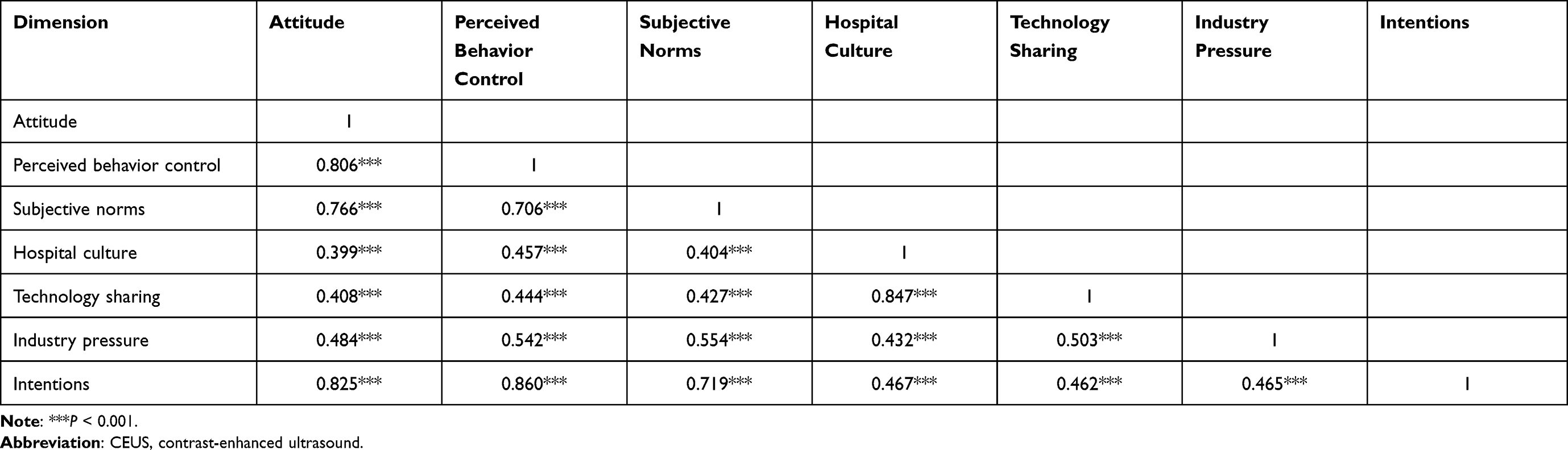 |
Table 4 Pearson Correlation Matrix of Physicians’ Intentions to Use CEUS and Its Potential Determinants (r) |
Ridge Regression
The ridge regression model supported the assumptions in the proposed framework (Table 5). The overall model accounted for 73.5% of the variance in physicians’ intentions to use CEUS. Although the effect of characteristics was not significant, physicians’ attitude (β = 0.227, P < 0.001) and perceived behavior control (β = 0.258, P < 0.001) were positively associated with their intentions to use CEUS, and all social norms variables (including subjective norms, hospital culture, technology sharing, and industry competition) were found to be significantly affect physicians’ intentions to use CEUS (P < 0.05).
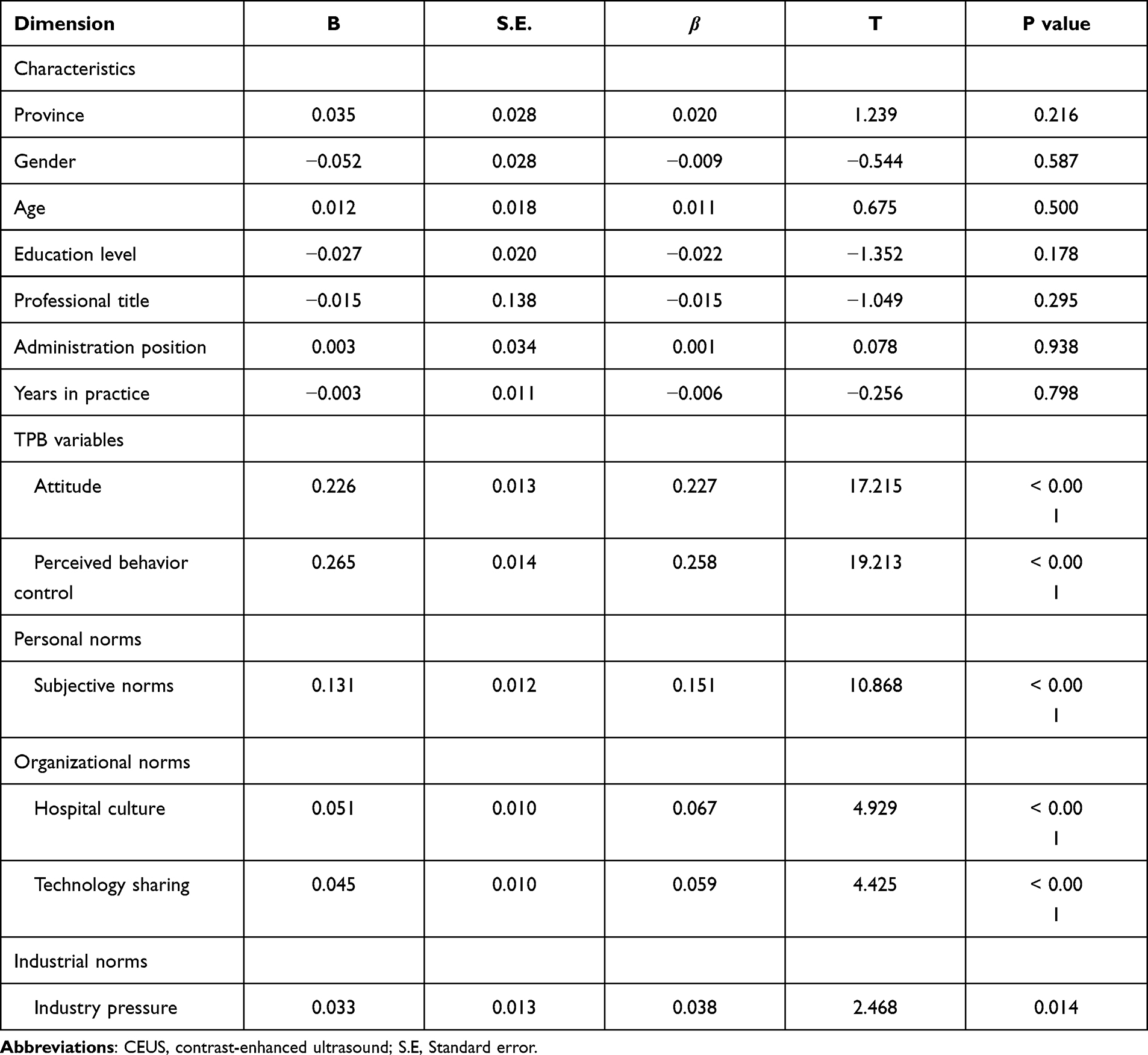 |
Table 5 Ridge Regression Model for Influencing Factors of Physicians’ Intentions to Use CEUS |
Discussion
The purpose of this study was to provide insights into the predictors associated with physicians’ intentions to use liver cancer screening. The research framework developed from the TPB plus the social norms constructs was supported in this study. Additionally, the predictability of TPB variables and social norms variables on physicians’ intentions to use CEUS was verified, including attitude, perceived behavioral control, subjective norms, hospital culture, technology sharing, and industry pressure. The findings of this study could provide a direct reference for promoting physicians’ intentions and behaviors in the use of liver cancer screening.
Contrary to expectations, there was no significant difference in physicians’ intentions to use CEUS in provinces with a high incidence of liver cancer (eg, Fujian) or low incidence (eg, Jiangxi). The reason may be that although the low incidence of liver cancer in Jiangxi compared with the national average, liver cancer is still the leading cause of death among the local residents. Thus, in the context of the great demand for medical services, physicians in Jiangxi would not use CEUS significantly less than physicians in Fujian for a technical service with specificity, sensitivity, and cost-effectiveness.
Consistent with previous research,54–56 attitude and perceived behavioral control are the important influencing factors of health professionals’ intentions to use a certain service or product. TPB suggests that an individual’s intentions and usage behaviors are the results of combined function of the internal factors. The consistency of behavior with attitude and motivation is the requirement for performing a specific behavior.57 A favorable attitude toward liver cancer screening is indispensable feedback to a behavior. In addition, the results indicated that physicians’ intention to use liver cancer screening was influenced by perceived behavioral control that could control or enhance their intention. More specifically, the perception of the obstacles, risks, or rewards associated with the use of liver cancer screening decreases or increases physicians’ willingness to try to achieve it or to avoid it.
The influence of social norms on physicians’ intention to use liver cancer screening was also confirmed in three aspects: personal norms, organizational norms, and industrial norms. Personal norms, namely subjective norms, refer to the perceived expectations or evaluations for particular behaviors by which people are important to us.8 In a work situation, these people are usually colleagues, superiors, and authorities.
An important reminder from the results was that even though those influential figures did not exert direct pressure on us to act, they play the exemplary and leading role that implicitly affects others’ intentions and behaviors, especially for new members and marginal groups. In addition to personal norms, the effects of organizational norms and industrial norms were also significant in this study. Hospital culture and technology sharing represented the organizational norms. The former is the ensemble of values and beliefs accumulated by the members within a hospital over a long time,58,59 while the latter is the extent to which knowledge and information are shared with other health care institutions.60,61 Both of them reflected the hospitals’ overall attitude and readiness for liver cancer screening at the spirit level in this study. As the invisible “public opinion environment”, it’s recognized that the organizational norms unavoidably affected physicians’ intention to use liver cancer screening. In order to give full play to its role, it is necessary to attach the importance to the cultivation of hospital spirit,62,63 reach consensus beliefs within the hospital that encourage early diagnosis and treatment for liver cancer patients or high-risk populations via screening, and develop an atmosphere of advocating technology diffusion in a wider range to promote health.
Industrial norms referred to industry pressure in this study. Such pressure may be from surrounding hospitals, business partners, and standards in this industry.64 In most cases, hospitals and physicians face competition from peers for more patients, and the pressure from the technology developers and suppliers will impact their expectations for investment returns.65 The industry pressure would enhance physicians’ intention to use liver cancer screening if they want to stay competitive.
Social norms interventions have received increased interest in “changing or promoting certain behaviors” in health professionals. Several strategies based on the compliance mechanism of social norms can be recommended to strengthen physicians’ intentions and behaviors of using liver cancer screening.66 The first strategy is core members take the lead. The wide acceptance and use of liver cancer screening by senior physicians and supervisors, who generally have a demonstration role for other physicians, are the best guides. For better expanding the use of liver cancer screening, it is recommended to mobilize the senior individuals at first. The second is panel meeting. Through collective thinking, the meeting will be capable of reshaping norms and practices from a critical perspective.67 Another strategy is information push system. By regularly and timely sending information and hot spots in the field of liver cancer diagnosis and treatment, physicians will be capable of making decisions on the basis of the knowledge of industry trends.
In addition to the implications, this study is also strengthened by some features. One of the strengths is the research framework developed by integrating the TPB with the concepts of social norms, which is conducive to identifying the influence of organizational norms and industrial norms in addition to those of individuals. The second strength is that the findings extend the corresponding knowledge of physicians’ intentions to use cancer screening, this will be useful in providing approaches for future interventions. Another strength is that the application of ridge regression analysis avoids the problems caused by multicollinearity and makes the model more realistic. Inevitably, this study also has some limitations. First, since all of the variables were measured by self-report, social desirability bias, in which some physicians may tend to make more positive responses, cannot be ruled out. Second, some potential factors may not have been considered and should be studied more comprehensively. Third, due to limited time and funding, the representativeness of research data may be a concern and the sample size needs to be expanded in future work. Finally, the cross-sectional study design does not allow for causal inferences.
Conclusion
This study enriches the knowledge in the field of technology diffusion and utilization, especially by increasing the understanding of the associated factors of physicians’ intentions to use liver cancer screening. In addition to internal factors including attitude and perceived behavioral control in TPB, this study identified that physicians’ intentions to use liver cancer screening were predicted by physicians’ perceived social norms at three levels: personal, organizational, and industrial norms. It is concluded that appropriate social norms interventions should be integrated to improve physicians’ intentions and usage behaviors. Furthermore, some specific measures, such as playing core members’ roles, holding panel meetings, and establishing information push systems, are proposed for future practice.
Abbreviations
TPB, Theory of Planned Behavior; CEUS, contrast-enhanced ultrasound.
Ethical Statement
This study did not involve patients or public. Ethical permission was granted for this study from the Ethics Committee of Fujian Medical University (No. 2017-17). The entire process of this study was conducted under the Declaration of Helsinki. A formal letter of cooperation was written to the directors of each selected medical institution, and permission was obtained. All participants were informed of the study purpose, participation was voluntary, and all responses were anonymous. Participants were considered to have given informed consent If they completed and returned the questionnaire.
Consent for Publication
All participants provided written informed consent to publish this study.
Acknowledgments
We acknowledge each hospital for their support in participating in this study and all the facilitators who contributed to the coordination efforts in the site. We would also like to thank all the physicians who agreed to participate.
Funding
This research was supported by the National Natural Science Foundation of China (Grant Number: 71704026) and the Distinguished Young Scientific Research Talents Plan in Universities of Fujian Province (Grant number: 2018B030). And the funders had no involvement in study design, data collection, statistical analysis, and manuscript writing.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Ma C, Kesarwala AH, Eggert T, et al. NAFLD causes selective CD4(+) T lymphocyte loss and promotes hepatocarcinogenesis. Nature. 2016;531:253–257. doi:10.1038/nature16969
2. Ma J, Yang F. Survey of chronic hepatitis B of community and early liver cancer screening for these specific population in follow-up. Biomed Res. 2017;28:10043–10047.
3. Qiu WQ, Shi JF, Guo LW, et al. Medical expenditure for liver cancer in urban China: a 10-year multicenter retrospective survey (2002–2011). J Cancer Res Ther. 2018;14:163–170. doi:10.4103/jcrt.JCRT_709_16
4. Chen W, Zheng R, Baade PD, et al. Cancer statistics in China, 2015. CA Cancer J Clin. 2016;66:115–132. doi:10.3322/caac.21338
5. Duffy SW, Myles JP, Maroni R, et al. Rapid review of evaluation of interventions to improve participation in cancer screening services. J Med Screen. 2017;24:127–145. doi:10.1177/0969141316664757
6. von Wagner C, Hirst Y, Waller J, et al. The impact of descriptive norms on motivation to participate in cancer screening - Evidence from online experiments. Patient Educ Couns. 2019;102:1621–1628. doi:10.1016/j.pec.2019.04.001
7. Zou XN. Epidemic trend, screening, and early detection and treatment of cancer in Chinese population. Cancer Boil Med. 2017;14:50–59. doi:10.20892/j.issn.2095-3941.2016.0047
8. Ajzen I. The theory of planned behavior. Organ Behav Hum Decis Process. 1991;50:179–211. doi:10.1016/0749-5978(91)90020-T
9. Chiu YL, Chou YC, Chang YW, et al. Using an extended theory of planned behaviour to predict smoking cessation counsellors’ intentions to offer smoking cessation support in the Taiwanese military: a cross-sectional study. BMJ Open. 2019;9:e026203. doi:10.1136/bmjopen-2018-026203
10. Godin G, Bélanger-Gravel A, Eccles M, et al. Healthcare professionals’ intentions and behaviours: a systematic review of studies based on social cognitive theories. Implement Sci. 2008;3:36. doi:10.1186/1748-5908-3-36
11. Seehusen DA, Deavers J, Mainous AG, et al. The intersection of physician wellbeing and clinical application of diabetes guidelines. Patient Educ Couns. 2018;101:894–899. doi:10.1016/j.pec.2017.12.007
12. Ly BA, Labonté R, Bourgeault IL. The beliefs of Senegal’s physicians toward the use of telemedicine. Pan Afr Med J. 2019;34:97. doi:10.11604/pamj.2019.34.97.20216
13. Deng Q, Liu W. Utilization of clinical practice guideline on antimicrobial in China: an exploratory survey on multilevel determinants. BMC Health Serv Res. 2020;20:282. doi:10.1186/s12913-020-05171-z
14. Armitage CJ, Conner M. Social cognition models and health behaviour: a structured review. Psychol Health. 2000;15:173–189. doi:10.1080/08870440008400299
15. Bamberg S, Hunecke M, Blobaum A. Social context, personal norms and the use of public transportation: two field studies. J Environ Psychol. 2007;27(3):190–203. doi:10.1016/j.jenvp.2007.04.001
16. Olsson LE, Huck J, Friman M. Intention for car use reduction: applying a stage-based model. Int J Environ Res Public Health. 2018;15:216. doi:10.3390/ijerph15020216
17. Wilkins KG, Mody B. Redeveloping development communication: developing communication and communicating development. Commun Theory. 2001;11:385–396. doi:10.1111/j.1468-2885.2001.tb00249.x
18. Frank LB. Social norms about a health issue in work group networks. Int J Environ Res Public Health. 2015;12:11621–11639. doi:10.3390/ijerph120911621
19. Cheng OY, Yam CLY, Cheung NS, Lee PLP, Ngai MC, Lin C-Y. Extended theory of planned behavior on eating and physical activity. Am J Health Behav. 2019;43(3):569–581. doi:10.5993/AJHB.43.3.11
20. Lin C-Y, Broström A, Årestedt K, Mårtensson J, Steinke EE, Pakpour AH. Using extended theory of planned behavior to determine factors associated with help-seeking behavior of sexual problems in women with heart failure: a longitudinal study. J Psychosom Obstet Gynaecol. 2020;41:54–61. doi:10.1080/0167482X.2019.1572743
21. Lin C-Y, Broström A, Nilsen P, Pakpour AH. Using extended theory of planned behavior to understand aspirin adherence in pregnant women. Pregnancy Hypertens. 2018;12:84–89.
22. Fan C-W, Chen I-H, Ko N-Y, et al. Extended theory of planned behavior in explaining the intention to COVID-19 vaccination uptake among mainland Chinese university students: an online survey study. Hum Vaccin Immunother. 2021;17(10):3413–3420. doi:10.1080/21645515.2021.1933687
23. Lin C-Y, Tseng Y-H, Lin M-L, Hou W-L. Factors related to intentions to commit dating violence among Taiwanese university students: application of the extended theory of planned behavior. Int J Environ Res Public Health. 2021;18:1956. doi:10.3390/ijerph18041956
24. Wan C, Shen GQ, Choi S. The moderating effect of subjective norm in predicting intention to use urban green spaces: a study of Hong Kong. Sust Cities Soc. 2018;37:288–297. doi:10.1016/j.scs.2017.11.022
25. Gkargkavouzi A, Halkos G, Matsiori S. Environmental behavior in a private-sphere context: integrating theories of planned behavior and value belief norm, self-identity and habit. Resour Conserv Recycl. 2019;148:145–156. doi:10.1016/j.resconrec.2019.01.039
26. Thomas JM, Liu J, Robinson EL, et al. The effects of liking norms and descriptive norms on vegetable consumption: a randomized experiment. Front Psychol. 2016;7:442. doi:10.3389/fpsyg.2016.00442
27. Cialdini RB, Kallgren CA, Reno RR. A focus theory of normative conduct: a theoretical refinement and reevaluation of the role of norms in human behavior. In: Advances in Experimental Social Psychology. Vol. 24. Academic Press; 1991:201–234.
28. Li Y, Yan X. How could peers in online health community help improve health behavior. Int J Environ Res Public Health. 2020;17:2995. doi:10.3390/ijerph17092995
29. Ebu NI, Ogah JK. Predictors of cervical cancer screening intention of HIV-positive women in the central region of Ghana. BMC Womens Health. 2018;18:43. doi:10.1186/s12905-018-0534-z
30. Lee FH. Intention to receive breast cancer screening and related factors of influence among Vietnamese women in transnational marriages. J Nurs Res. 2018;26:112–122. doi:10.1097/jnr.0000000000000210
31. Sieverding M, Matterne U, Ciccarello L. What role do social norms play in the context of men’s cancer screening intention and behavior? Application of an extended theory of planned behavior. Health Psychol. 2010;29:72–81. doi:10.1037/a0016941
32. Besharati F, Karimi-Shahanjarini A, Hazavehie SMM, et al. Predictors of colorectal cancer screening intention among Iranian adults: an application of the preventive health model. J Prev Med Hyg. 2018;59:E159–E166.
33. Henderson LM, Marsh MW, Benefield TS, et al. Opinions and practices of lung cancer screening by physician specialty. N C Med J. 2019;80:19–26. doi:10.18043/ncm.80.1.19
34. Raz DJ, Wu GX, Consunji M, et al. Perceptions and utilization of lung cancer screening among primary care physicians. J Thorac Oncol. 2016;11:1856–1862. doi:10.1016/j.jtho.2016.06.010
35. Ragland M, Trivers KF, Andrilla C, et al. Physician nonprofessional cancer experience and ovarian cancer screening practices: results from a national survey of primary care physicians. J Womens Health. 2018;27:1335–1341. doi:10.1089/jwh.2018.6947
36. Sieverding M, Decker S, Zimmermann F. Information about low participation in cancer screening demotivates other people. Psychol Sci. 2010;21:941–943. doi:10.1177/0956797610373936
37. Honda K, Gorin SS. A model of stage of change to recommend colonoscopy among urban primary care physicians. Health Psychol. 2006;25:65–73. doi:10.1037/0278-6133.25.1.65
38. Messerschmidt CM, Hinz O. Explaining the adoption of grid computing: an integrated institutional theory and organizational capability approach. J Strategic Inf Syst. 2013;22:137–156. doi:10.1016/j.jsis.2012.10.005
39. Liu H, Ke W, Wei KK, et al. The role of institutional pressures and organizational culture in the firm’s intention to adopt internet-enabled supply chain management systems. J Oper Manag. 2010;28:372–384. doi:10.1016/j.jom.2009.11.010
40. Mitchell PF, Pattison PE. Organizational culture, intersectoral collaboration and mental health care. J Health Organ Manag. 2012;26:32–59. doi:10.1108/14777261211211089
41. Kornilaki M, Font X. Normative influences: how socio-cultural and industrial norms influence the adoption of sustainability practices. A grounded theory of cretan, small tourism firms. J Environ Manage. 2019;230:183–189. doi:10.1016/j.jenvman.2018.09.064
42. Zhang Y, Li J. Influence of physician multi-pilot practice on hospital human resource management. Chinese Hospital Manage. 2019;39:79–80.
43. Gavrilets S, Richerson PJ. Collective action and the evolution of social norm internalization. P Natl Acad Sci USA. 2017;114:6068–6073. doi:10.1073/pnas.1703857114
44. Helfrich CD, Li YF, Sharp ND, et al. Organizational readiness to change assessment (ORCA): development of an instrument based on the promoting action on research in health services (PARIHS) framework. Implement Sci. 2009;4(1):1–13. doi:10.1186/1748-5908-4-38
45. Mccormack B, Mccarthy G, Wright J, et al. Development and testing of the context assessment index (CAI). Worldviews Evid Based Nurs. 2009;6(1):27–35. doi:10.1111/j.1741-6787.2008.00130.x
46. Sheu C, Chae B, Yang CL. National differences and ERP implementation: issues and challenges. Omega. 2004;32(5):361–371. doi:10.1016/j.omega.2004.02.001
47. Sun KX, Zheng RS, Zhang SW, et al. Report of cancer incidence and mortality in different areas of China, 2015. China Cancer. 2019;28:4–14.
48. Zhou Y, Ma JY, Jiang HJ, et al. Analysis of cancer incidence and mortality in Fujian cancer registries, 2014. Chin J Clin Oncol. 2018;45:898–903.
49. Liu J, Zhu LP, Yang XL, et al. Incidence, mortality and life lost of malignancies among residents living in areas covered by cancer registry in Jiangxi province, 2010–2017. Chin J Public Health. 2018;34:1692–1695.
50. Nunnally JC. Psychometric Theory.
51. Dormann CF, Elith J, Bacher S, et al. Collinearity: a review of methods to deal with it and a simulation study evaluating their performance. Ecography. 2013;36:27–46. doi:10.1111/j.1600-0587.2012.07348.x
52. Prunier JG, Colyn M, Legendre X, et al. Multicollinearity in spatial genetics: separating the wheat from the chaff using commonality analyses. Mol Ecol. 2015;24:263–283. doi:10.1111/mec.13029
53. Obenchain RL. Classical F-test and confidence regions for ridge regression. Technometrics. 1977;19:429–439. doi:10.1080/00401706.1977.10489582
54. Hassan ZM. Attitudes, social norms, perceived behavioral control, and intention toward methicillin-resistant Staphylococcus aureus screening among health care workers. Res Theory Nurs Pract. 2017;31:321–333. doi:10.1891/1541-6577.31.4.321
55. Ly BA, Kristjansson E, Labonté R, et al. Determinants of the intention of Senegal’s physicians to use telemedicine in their professional activities. Telemed E Health. 2018;24:897–898. doi:10.1089/tmj.2017.0276
56. Liu C, Liu C, Wang D, et al. Determinants of antibiotic prescribing behaviors of primary care physicians in Hubei of China: a structural equation model based on the theory of planned behavior. Antimicrob Resist Infection Control. 2019;8:23. doi:10.1186/s13756-019-0478-6
57. Abamecha F, Tena A, Kiros G. Psychographic predictors of intention to use cervical cancer screening services among women attending maternal and child health services in Southern Ethiopia: the theory of planned behavior (TPB) perspective. BMC Public Health. 2019;19:434. doi:10.1186/s12889-019-6745-x
58. Wilcock M, Harding G. What do pharmacists think of MURs and do they change prescribed medication? Pharm J. 2008;281:163–167.
59. Kummer TF, Recker J, Bick M. Technology-induced anxiety: manifestations, cultural influences, and its effect on the adoption of sensor-based technology in German and Australian hospitals. Inform Manage. 2017;54:73–89. doi:10.1016/j.im.2016.04.002
60. Kim KK, Sankar P, Wilson MD, et al. Factors affecting willingness to share electronic health data among California consumers. BMC Med Ethics. 2017;18:25. doi:10.1186/s12910-017-0185-x
61. Weitzman ER, Kelemen S, Kaci L, et al. Willingness to share personal health record data for care improvement and public health: a survey of experienced personal health record users. BMC Med Inform Decis Mak. 2012;12:39. doi:10.1186/1472-6947-12-39
62. Wraikat H, Bellamy A, Tang H. Exploring organizational readiness factors for new technology implementation within non-profit organizations. Open J Soc Sci. 2017;5:1–13.
63. Williams I. Organizational readiness for innovation in health care: some lessons from the recent literature. Health Serv Manage Res. 2011;24:213–218. doi:10.1258/hsmr.2011.011014
64. Benavides VS, Strode A, Sheeran BC. Using technology in the delivery of mental health and substance abuse treatment in rural communities: a review. J Behav Health Serv Res. 2013;40:111–120. doi:10.1007/s11414-012-9299-6
65. Wallner PE, Konski A. A changing paradigm in the study and adoption of emerging health care technologies: coverage with evidence development. J Am Coll Radiol. 2008;5:1125–1129. doi:10.1016/j.jacr.2008.06.008
66. Young HP. The evolution of social norms. Ann Rev Econ. 2015;7:359–387. doi:10.1146/annurev-economics-080614-115322
67. Cislaghi B, Heise L. Theory and practice of social norms interventions: eight common pitfalls. Global Health. 2018;14:83. doi:10.1186/s12992-018-0398-x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.