Back to Journals » International Journal of Women's Health » Volume 18
The Effect of Sleep Deprivation on Cognitive Function in Postmenopausal Women: A Systematic Review
Authors Benýšková E, Beníčková M, Gimunová M ![]()
Received 16 September 2025
Accepted for publication 14 January 2026
Published 29 January 2026 Volume 2026:18 562840
DOI https://doi.org/10.2147/IJWH.S562840
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Emma Benýšková, Michaela Beníčková, Marta Gimunová
Department of Physical Activities and Health Sciences, Faculty of Sports Studies, Masaryk University, Brno, Czech Republic
Correspondence: Emma Benýšková, Department of Physical Activities and Health Sciences, Faculty of Sports Studies, Masaryk University, Kamenice 753/5, Brno 625 00, Czech Republic, Email [email protected]
Purpose: Poor sleep quality, insufficient sleep quantity, and other sleep disorders frequently emerge during the menopausal transition, with their prevalence increasing in postmenopause, and subsequently affecting cognitive function. This systematic review aims to examine the impact of sleep deprivation on cognitive function (ie, memory, attention, information processing, executive function, and overall cognitive performance) in postmenopausal women.
Patients and Methods: The systematic review was conducted in accordance with the guidelines set by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA). Out of a total of 795 studies identified in databases PubMed, Web of Science, and PsycInfo, 19 studies meeting the specified PECO criteria were included. The search was restricted to articles published from 2014 to 2024. The quality assessment of the included studies was performed using the Adjusted Downs and Black Quality Assessment Checklist.
Results: The results of this systematic review show that sleep deprivation negatively affects the overall cognitive health of postmenopausal women. Short (< 6 hours) or excessively long (> 8 hours) sleep was associated with problems in maintaining attention or slower information processing. Women with insufficient sleep were more susceptible to cognitive impairments compared to those with optimal sleep duration (~7 hours), which also worsened their quality of life. These results highlight the importance of early diagnosis and prevention of sleep disorders in women in postmenopause and during the menopausal transition. However, the review has several limitations including different ages of participants, and a wide diversity of assessment tools used to measure both cognitive function and sleep quality in included studies.
Conclusion: Sleep deprivation has a negative impact on cognitive health in postmenopausal women. Early identification and management of sleep problems may support cognitive function and improve quality of life after the menopausal transition.
Keywords: menopausal transition, sleep disorders, perception, information processing, actigraphy, older adults
Introduction
Ovarian hormones changes related to menopause were reported to affect sleep physiology and cognitive performance. Additionally, an interplay between sleep quality and cognitive function was observed in previous studies. Poor sleep quality is a strong predictor of cognitive impairments, including attention problems and executive function deficits, particularly in older women.1–3
Sleep has a positive impact on learning, memory, logical reasoning, immune responses, repair processes, microbiome, blood glucose levels, blood pressure, and more.4 In contrast, insufficient sleep (six to seven hours or less) negatively affects the immune and cardiovascular systems, increases the likelihood of developing Alzheimer’s disease (AD), and contributes to other mental disorders. Complete repetitive absence of sleep might lead to the death of the organism.5–7
The quality and duration of sleep naturally change due to the aging of the organism. With increasing age, sleep shortens, falling asleep shifts to earlier evening hours and the organism wakes up in the early morning hours.8 Sleep disorders are up to twice as common in women as in men.9,10 Several studies have shown that these problems are mainly associated with menopause. Sleep problems begin to appear already during the menopausal transition and their occurrence increases in postmenopause.11 During the postmenopause period, 40 to 56% of women suffer from sleep disorders compared to 31% of women in premenopause.11 Women in postmenopause often suffer from poor sleep quality, insufficient sleep quantity, or other sleep disorders. An eight-year longitudinal analysis by Baker et al,12 involving over 3000 women from the SWAN (Study of Women’s Health Across the Nation) cohort, showed that frequent nighttime awakenings are the most common sleep disturbance among postmenopausal women. Sex hormones, especially estradiol (E2) play an important role in women’s sleep quality.13
During perimenopause, levels of follicle-stimulating hormone (FSH) significantly increase, while E2 levels are normal or decreased.14 The rise in FSH is probably due to a decline in ovarian inhibin production, which under normal physiological conditions reduces FSH secretion in the pituitary gland.14 Postmenopause is characterized by amenorrhea lasting longer than one year, when amenorrhea becomes permanent. This period is characterized by minimal hormone production in the ovaries, reduced E2 levels, and a permanently elevated level of FSH and luteinizing hormone (LH).15 Kravitz et al11 found that sleep disturbances are linked to changes in reproductive hormone levels. A decrease in E2 was associated with difficulty falling asleep and maintaining sleep, while an increase in FSH was linked to problems with sleep maintenance.11
E2 and its neuroprotective effects have been shown to enhance cholinergic and serotonergic neurotransmission and to support synaptic plasticity in the hippocampus and prefrontal cortex.16 The decline in this ovarian hormone, during the menopausal transition appears to affect neural systems involved in learning and memory. During menopausal transition many women experience changes in cognitive performance,17 particularly in domains such as verbal memory, attention, working memory and executive function.18–20 Previous epidemiological and clinical studies suggest an association between postmenopausal hormone levels and cognitive performance indicating that lower E2 levels and/or disrupted E2 signaling correlates with a greater risk of cognitive decline.
Sleep plays a crucial role in cognitive processes. It is important to diagnose and treat insomnia in older adults properly as poor sleep can have serious consequences, including decreased health-related quality of life,21 impaired cognitive performance22 and even an increased risk of dementia, including AD.11 Therefore, the aim of this study was systematically review and summarize the results of available literature on with the impact of sleep deprivation on cognitive function in postmenopausal women.
Materials and Methods
Eligibility Criteria for Selecting Studies
The systematic review was developed in accordance with the guidelines set by the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA).23 The PECO criteria were used to evaluate the eligibility of the studies for this systematic review (Table 1).
 |
Table 1 The PECO Criteria |
Search Strategy and Selection Process
The search was performed using three databases, Web of Science, PubMed, and PsycInfo in October 2024 by one researcher (EB). The following terms with Boolean operators were used for the databases search: (“postmenopausal women” OR “postmenopause” OR “post-menopause” OR “postmenopausal” OR “elderly women” OR “older women” OR “menopausal transition”) AND (“sleep” OR “insomnia” OR “sleep initiation” OR “sleep deprivation” OR “sleep disorders” OR “sleep loss” OR “insufficient sleep” OR “sleep insufficiency” OR “sleep restriction”) AND (“cognitive function” OR “cognition” OR “memory” OR “executive function” OR “cognitive impairment” OR “attention” OR “mental health” OR “cognitive” OR “comprehension” OR “perception”).
The search was restricted to articles published within the last 10 years, ie, from 2014 to 2024. Exclusion criteria consisted of animal studies, mixed or male participants, non-English, review articles, conference papers, books, and book chapters, and no full text available.
A total of 795 studies from the Web of Science, PubMed, and PsycInfo databases were uploaded into the Rayyan system24 for title and abstract screening. Duplicate articles (n = 280), studies written in other language than English (n = 9), review articles, meta-analyses, and book chapters (n = 78) were excluded by one researcher (EB). The title and abstract of the remaining studies (n = 428) were screened independently by two researchers (EB, MG). Any disagreement between the researchers was resolved by discussion with a third researcher (MB). The full texts of the included studies (n = 66) were screened to confirm their relevance to the current systematic review. If the study’s aim, hypotheses, or content did not align with the PECO criteria, the study was excluded (n = 46). A common reason for exclusion at this stage was that the studies focused on general mental health rather than specifically on cognitive function. After the screening process, 19 studies were included into this systematic review. The study selection process is summarized in the PRISMA flow diagram (Figure 1).
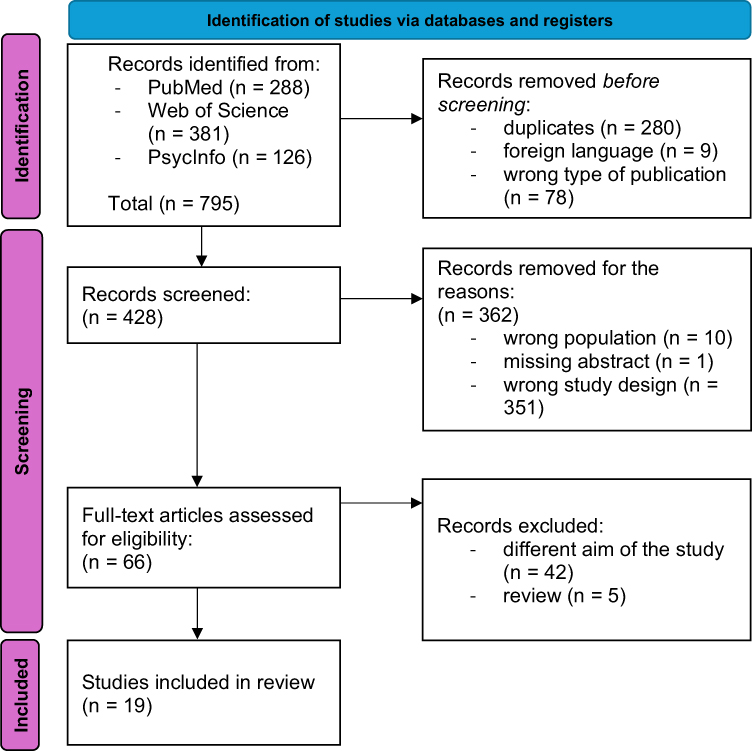 |
Figure 1 PRISMA flow diagram illustrating the identification, screening, eligibility assessment, and inclusion of studies in the systematic review. |
Data Extraction
The following information was extracted from included studies using Microsoft Excel by one researcher (EB): authors, year of publication, country of origin, number of female participants, participants’ age and BMI, method of sleep and cognitive function assessment, and the measured outcomes.
Quality Assessment of Included Studies
The quality assessment of the studies was conducted using the Adjusted Downs and Black Quality Assessment Checklist (1998) by one researcher (EB). The original checklist consists of 27 items divided into four sections: Reporting, External Validity, Internal Validity, and Power. Each item could be answered in one of the following ways: yes, no, or unable to determine (UTD). The scoring system was as follows: yes = 1 point, no and UTD = 0 points. From the 27 items, 8 were irrelevant for included studies. After adjusting the scoring system for 19 relevant items, the final score was converted into a percentage. A similar approach was used in previous systematic reviews.25–27To calculate the percentage score, Kennelly’s method was used, which states:
Kennelly’s score= ((number of criteria met)/(total number of criteria))×100
Based on these percentages, the methodological quality of the individual studies was classified as follows:
- Less than 45.4% indicates poor methodological quality.
- A range of 45.4–61.0% indicates fair methodological quality.
- More than 61.0% indicates good methodological quality.28
This systematic review is based on author’s (EB) master’s thesis at Masaryk University.29
Results
During the database search, a total of 795 studies were identified (Web of Science: 381 articles, PubMed: 288 articles, and PsycInfo: 126 articles). After the screening process, 19 studies met the predefined PECO criteria and were included in the systematic review.
Analysis of Studies and Assessment of Their Methodological Quality
The methodological quality of included studies ranged from 52.9% to 84.6% indicating a fair30–32 to good methodological quality. The most common methodological limitation was a lack of representativeness of the source population. The methodological quality assessment of the included studies is shown in Supplementary material 1.
Study Characteristics
In Table 2, the sample characteristics of the included studies are presented. The studies are listed in alphabetical order according to the first author’s surname. Of the included studies, only one was conducted in Europe (Poland), ten in North America (USA, Canada), two in South America (Brazil), five in Asia (Japan, China, Indonesia, India) and one in Australia. The number of participants varied considerably, ranging from 22 in the smallest sample to15263participants in the largest. Participant age also varied widely as no upper age limit was defined. The lower age threshold was determined by the onset of menopause, which had to have lasted for at least 12 months for women to be identified as postmenopausal.
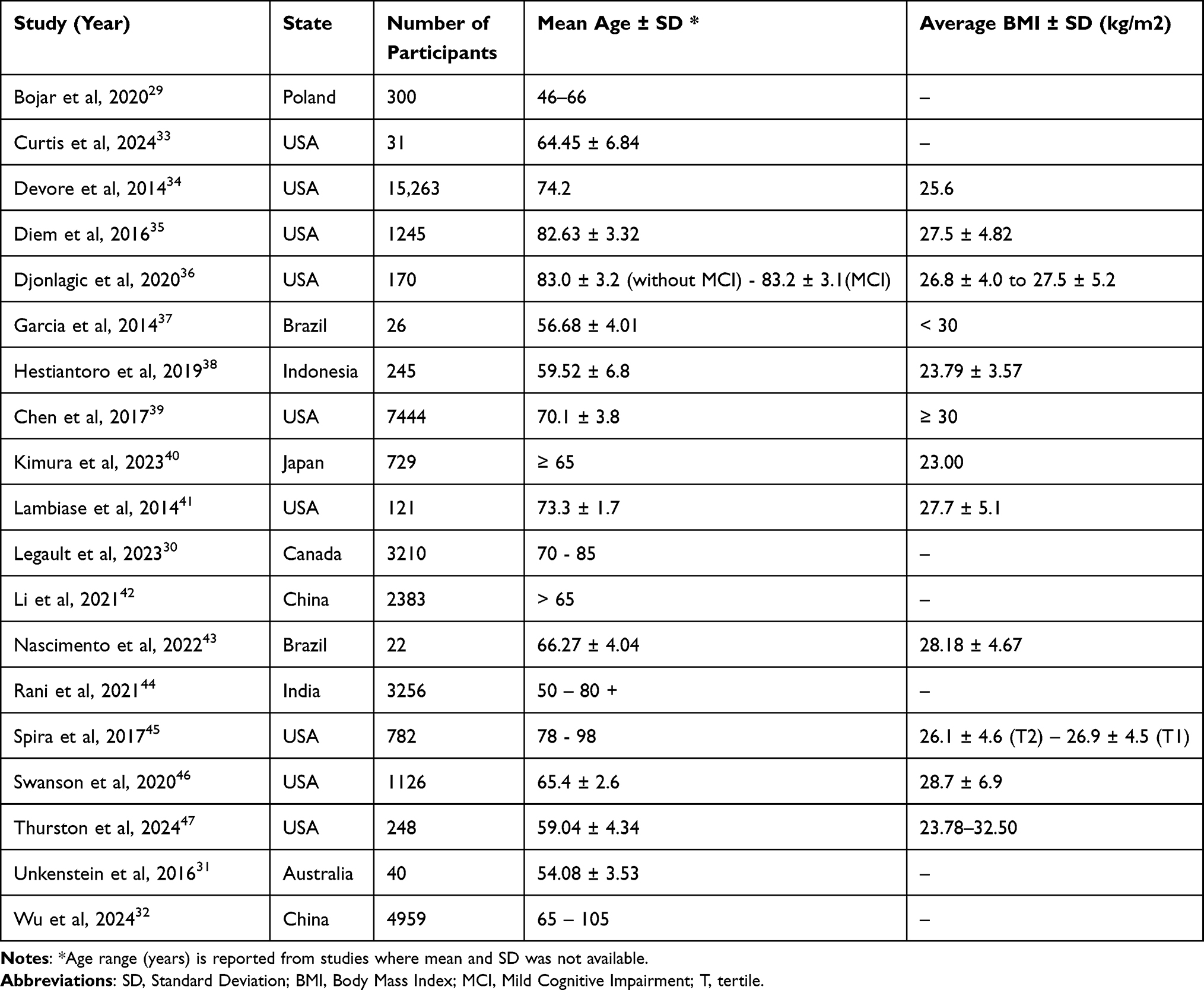 |
Table 2 Sample Characteristics |
Several tests were used to measure cognitive function. In most of the studies Mini-Mental State Examination (MMSE) and Modified Mini-Mental State Examination (3MS) were used.30,32,35,36,40,41,46 Additionally, delayed recall35,43 and verbal fluency30,46 were often assessed. Rani et al45 employed a self-assessment approach in their study. Specifically, they investigated the presence of “difficulty in concentrating or remembering things in the past 30 days”. This method was classified as self-report.
To assess sleep, actigraphy,30,31,36,41,46,47 polysomnographs37 sleep diaries,30,35,36 and questionnaires4,33,34,38 were used. The Pittsburgh Sleep Quality Index (PSQI) was used for sleep quality assessment by five studies.32,34,37,38,44 Study by Wu et al4 used information about the sleep from CESD-10 short form, originally developed to assess depressive symptoms as their study focused on correlations between sleep, cognitive function and depression. Some studies measured sleep through self-reports, in which participants indicated how many hours they slept per day or whether their sleep was disrupted (“sleep disruption”). Based on these responses, participants were categorized into groups (women experiencing sleep deprivation and women without sleep deprivation). Table 3 presents the methods used to assess sleep and cognitive function in included studies.
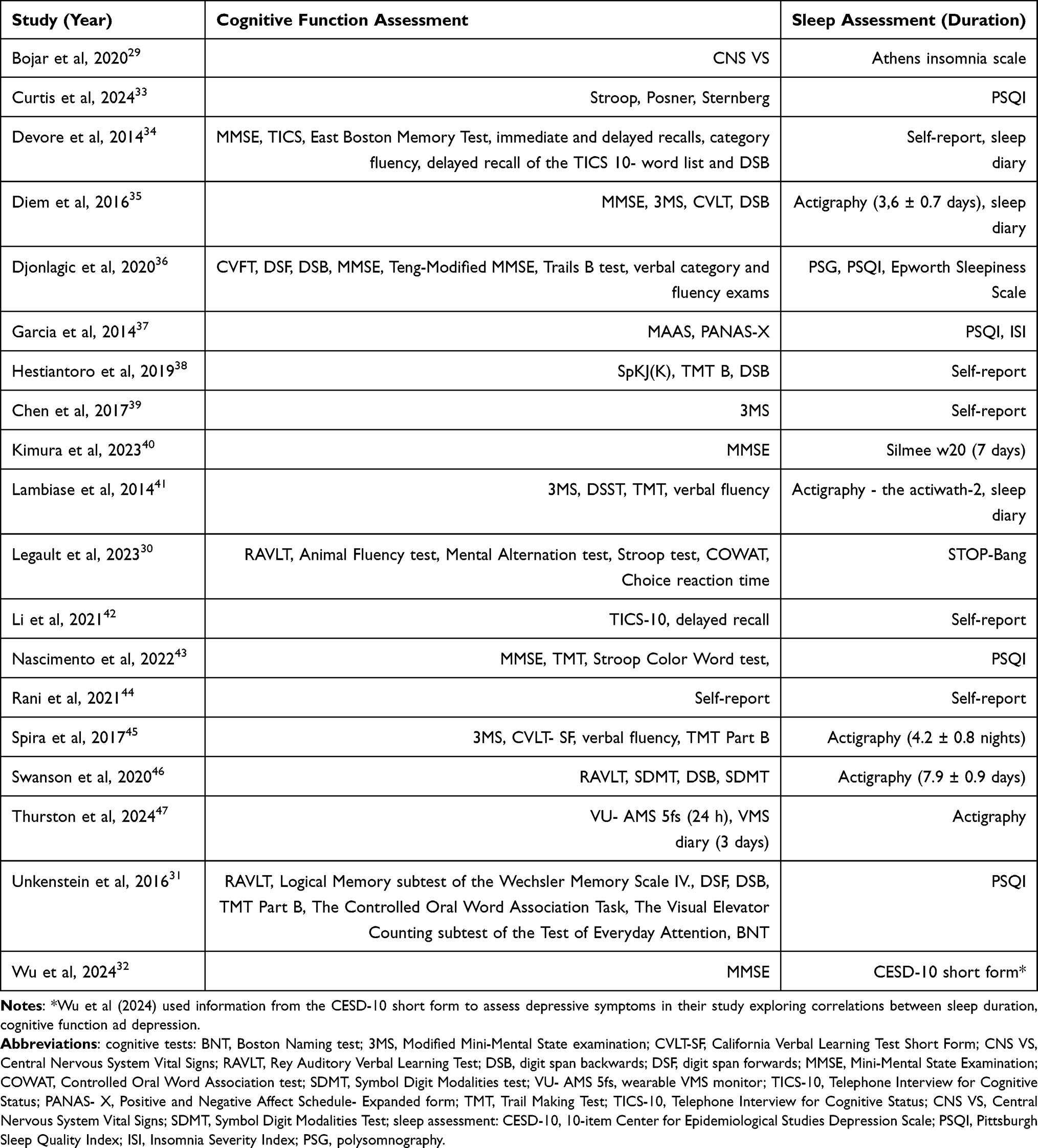 |
Table 3 Cognitive Function and Sleep Assessment Methods |
Table 4 describes the measured variables related to sleep quality. The most studied parameters were total sleep time (TST), sleep efficiency (SE), sleep fragmentation (SF), wake after sleep onset (WASO) and sleep onset latency (SOL). For studies using questionnaires or self-reports for sleep assessment, the exact numerical values are not available.
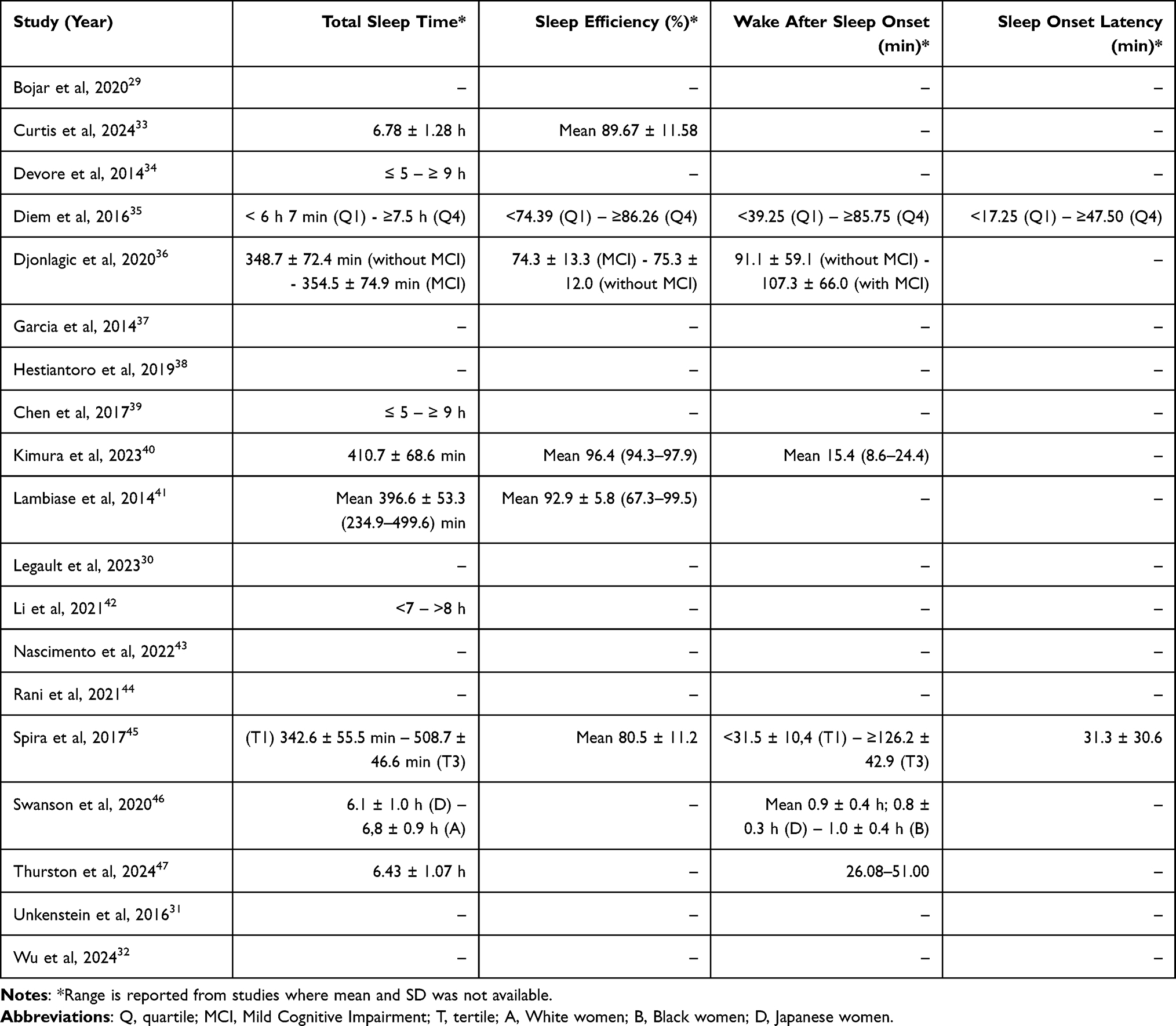 |
Table 4 Sleep Quality Characteristics |
Diem et al36 divided the study participants into four quartiles (Q1–Q4) based on SE and SOL, which were measured using actigraphy. SE values ranged from less than 74.39% in the lowest quartile (Q1) to 86.26% or higher in the highest quartile (Q4). For SOL, the lowest quartile (Q1) was defined as a sleep onset latency shorter than 17.25 minutes, while the highest quartile (Q4) included women with a latency longer than 47.5 minutes. Spira et al46 on the other hand, divided participants into three tertiles (T1–T3) based on total sleep time (TST) and wake after sleep onset (WASO). The TST tertiles ranged from a minimum value of 342.6 minutes in T1 to more than 508.7 minutes in T3, while WASO ranged from 31.5 minutes in T1 to more than 126.2 minutes in T3. In contrast to the previous studies, Swanson et al47 did not categorize participants based on sleep parameters but according to ethnicity. Participants were divided into four groups: A (White women), B (Black women), C (Chinese women), and D (Japanese women).
Impact of Sleep Characteristics on Cognition
Studies by Bojar et al,33 Curtis et al,34 Garcia et al,38 Hestiantoro et al,39 Kimura et al,41 Rani et al,45 Thurston et al31 and Wu et al4 report that poor sleep quality negatively affects the cognitive function of postmenopausal women, which may lead to the development of cognitive impairments and even dementia. Curtis et al34 and Garcia et al38 agree that poor sleep quality results in reduced attention. In contrast, Djonlagic et al,37 Nascimento et al44 and Unkenstein et al32 concluded that sleep quality has no effect on cognitive performance.
The influence of sleep duration on cognitive function in women was addressed in studies by Devore et al,35 Chen et al,40 Li et al,43 Spira et al44, and Swanson et al47 Devore et al35 claim that women with short sleep duration (< 5 hours) show lower cognitive performance compared to women with medium sleep duration (~7 hours). At the same time, the study notes that lower cognitive performance also affects women with long sleep duration (≥ 9 hours). Similar conclusions were drawn by Chen et al40 Women with a sleep duration of ≤ 6 hours have a 1.35–1.36x higher risk of mild cognitive impairment (MCI) compared to women with medium sleep duration. Women with long sleep duration (≥ 8 hours) have a 1.22–1.27x higher risk of developing MCI compared to those who sleep an average of 7 hours. Spira et al46 state that long sleep is associated with up to a 2.5x higher risk of developing MCI than medium sleep.
In contrast, the study by Swanson et al47 suggests that longer sleep duration is associated with better cognitive performance. However, in this study, long sleep duration was defined as 6.8 ± 0.9 hours, which previous two studies identified as medium sleep duration.
Sleep parameter WASO was examined in only two studies: Spira et al46 and Swanson et al47 Both studies agree that higher WASO values are associated with poorer cognitive performance. Spira et al46 even reports up to a 2x higher risk of MCI in postmenopausal women with increased WASO values.
SE was analyzed by Curtis et al,34 Diem et al,36 and Lambiase et al30 All studies reached the same conclusion: lower SE values lead to poorer cognitive status. Diem et al36 states that women with low SE have up to a 1.55x higher risk of MCI. MCI is also associated with high SE variability. Lambiase et al30 specifically notes impaired performance in attention, executive functions, and information processing. Diem et al36 also describes the impact of SOL on cognitive function. Higher sleep latency is associated with up to a 1.40x higher risk of developing MCI. Swanson et al47 uses another sleep parameter—sleep fragmentation (SF). The study describes that women with increased SF values show poorer cognitive performance and slower cognitive processing. Table 5 shows the results from included studies.
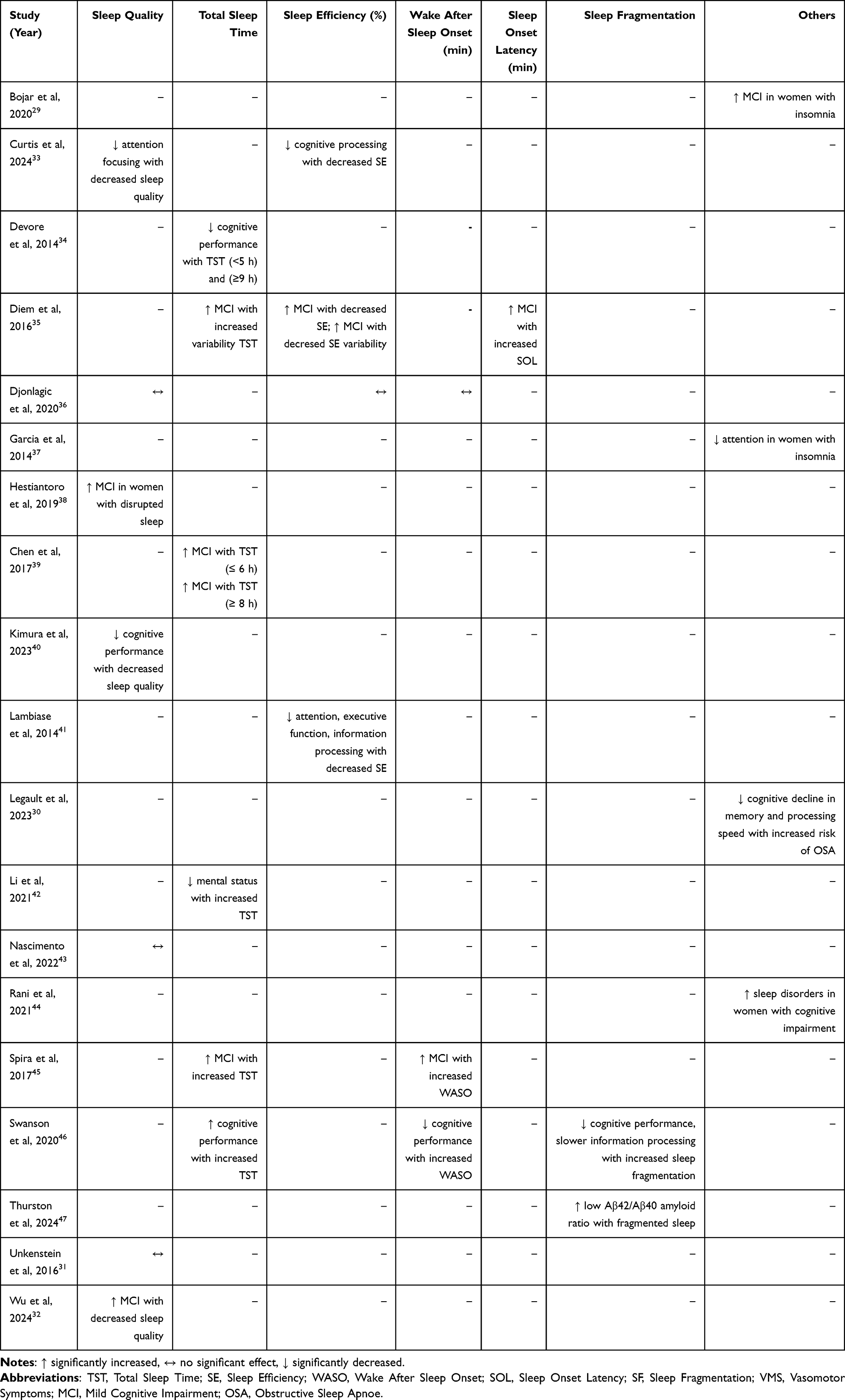 |
Table 5 The Effect of Sleep Characteristics on Cognitive Function |
Discussion
The aim of this systematic review was to summarize the available literature on the effect of sleep deprivation on cognitive function in postmenopausal women. The results consistently showed that sleep deprivation negatively affects the overall cognitive health of women in the postmenopausal period.
Impact of Sleep Characteristics on Cognition
The review identified a strong and specific relationship between sleep quantity and cognitive health. Interestingly, a U-shaped relationship emerges between sleep duration and cognition, where both insufficient (< 6 hours) and excessive (> 8 hours) sleep were associated with attention disorders, slower information processing, and a higher risk of cognitive impairment compared to women with a moderate sleep duration (~7 hours).35,40,43,46 On the other hand, three studies32,37,44 found no significant effect between sleep quality and cognitive function. These studies assessed sleep quality using questionnaires on a lower number of participants which could affect their results.
Beyond duration, other sleep quality metrics also showed a negative impact. Reduced SE and increased SF were linked to poorer performance in memory and attention tests.30,34,36,47 Similarly, longer WASO was associated with greater fatigue and lower cognitive performance, while prolonged SOL was often accompanied by impairments in executive functions and the ability to concentrate.36,46,47
The cognitive deficits associated with SF and sleep disruption may involve the impaired clearance of neurotoxic waste products. During sleep, the brain becomes more active, enabling the removal of biomolecules like amyloid-β, with this clearance being up to two times more efficient compared to wakefulness. Poor sleep quality, low SE, and higher SF are specifically associated with amyloid accumulation, which supports findings that fragmented sleep increases the risk of clinical AD. When sleep is insufficient or fragmented, amyloid-β accumulates in the brain, contributing to cognitive decline and reduced attentional capacity.48,49
Furthermore, insufficient or excessive sleep can lead to the accumulation of inflammatory markers such as C-reactive protein (CRP), interleukin-6 (IL-6), and tumor necrosis factor alpha (TNF-α).50 This chronic inflammation can lead to neurodegenerative changes and cognitive decline, thereby increasing the risk of mild cognitive impairment, dementia, or AD.51 Metabolic disorders also play a key role, as short or excessively long sleep negatively affects glucose metabolism and insulin sensitivity, potentially leading to insulin resistance and type 2 diabetes mellitus. Insulin resistance in the brain is associated with poorer cognitive abilities and an increased risk of AD.52
The hormonal context of postmenopause is also relevant, as a decline in E2 and progesterone levels has been associated with a decrease in gray matter in the prefrontal cortex. E2 is important for maintaining the balance between pro-inflammatory and anti-inflammatory factors and enhances neurochemical factors in several neurotransmitter systems (cholinergic, monoaminergic, serotonergic, and glutaminergic systems) that are severely injured in AD.53 Moreover, vasomotor symptoms during sleep may contribute to brain changes associated with AD; more frequent vasomotor symptoms were linked to an unfavorable Aβ42/Aβ40 amyloid ratio, suggesting a possible influence of sleep disorders on neurodegenerative processes.47 Additionally, poor sleep quality in the older population is also generally associated with reduced activity in the cerebral cortex.54
The Effect of an Acute and Chronic Sleep Deprivation on Cognition
The effects of sleep deprivation on cognition are multifaceted and differ substantially between acute and chronic forms. Acute sleep deprivation, such as a single night without sufficient sleep, can produce immediate perceptual and cognitive disturbances, most notably impairments in vigilance and sustained attention.55 These deficits are particularly consequential in fields that rely on optimal moment-to-moment performance, such as aviation or medicine.56 In contrast, longitudinal (chronic) sleep deprivation involves long-term, accumulated sleep loss that may undermines neuropsychological functioning.57 Long-term insufficient sleep correlates with neurodegenerative processes, especially the accumulation of Aβ, a pathological hallmark linked to cognitive deterioration.57 Together, these findings highlight that while acute sleep loss impairs cognitive performance immediately, chronic sleep deprivation poses a cumulative threat to long-term cognitive health and increases vulnerability to neurodegenerative diseases.
Ethnic Differences
The findings are complicated by several ethnic differences reported in previous studies. Swanson et al47 reported worse sleep parameters among Black women compared to White women. Specifically, increased SF was observed among Black women, who subsequently showed worse verbal memory and slower processing. While the exact mechanisms are unknown, possible reasons for these disparities include higher stress, health complications, and socioeconomic differences affecting both sleep quality and cognitive health.58 Previous studies also found that worse sleep (shorter duration, lower efficiency, higher WASO) was linked to elevated inflammatory markers in Black women, but not in White women. Black women also had lighter sleep as measured by actigraphy, which may affect cognitive function, though the exact mechanisms remain unknown.59,60
Limitations
The assessment of the methodological quality of the included studies showed that all studies met good or fair research standards, which strengthens the validity of the findings.
However, several limiting factors were identified across the reviewed studies, including varying sample sizes, inconsistent participant age ranges and a wide diversity of assessment tools used to measure both cognitive function and sleep quality. In many studies, data were assessed through self-report or standardized questionnaires, which may be subject to bias or limited accuracy compared to objective measures such as polysomnography, actigraphy or neuropsychological testing. Additionally, the geographical diversity of the study populations introduces potential cultural and environmental variations that could influence both sleep patterns and cognitive performance. It is also important to note that some degree of cognitive decline after the age of 80 is considered as a normal aspect of aging,61,62 making it essential to distinguish between age-related and pathological changes when interpreting study outcomes. These limitations highlight the importance of conducting future longitudinal and cross-cultural research using standardized, objective tools to better understand the complex relationship between sleep quality and cognitive function in postmenopausal women. Such studies could help clarify how age, hormonal status, and lifestyle factors influence cognitive aging.
Conclusion
The aim of this systematic review was to analyze the impact of sleep deprivation on cognitive function in postmenopausal women. The results showed that sleep deprivation negatively affects the overall cognitive health of women in the postmenopausal period. The results highlight the importance of early diagnosis and prevention of sleep disorders in women during and after the menopausal transition. Improving sleep hygiene, targeted education, and potential intervention measures can significantly contribute to better cognitive health and overall quality of life for women in the postmenopausal period. Future research should focus on longitudinal studies to better clarify the causal link between specific sleep parameters and cognitive decline.
Funding
Specific University Research Grant provided by the Ministry of Education, Youth and Sports of the Czech Republic (number MUNI/A/1475/2024).
Disclosure
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
1. Gervais NJ, Mong JA, Lacreuse A. Ovarian hormones, sleep and cognition across the adult female lifespan: an integrated perspective. Front Neuroendocrinol. 2017;47:134–13. doi:10.1016/j.yfrne.2017.08.002
2. Brewster GS, Varrasse M, Rowe M. Sleep and cognition in community-dwelling older adults: a review of literature. Healthcare. 2015;3(4):1243–1270. doi:10.3390/healthcare3041243
3. Miyata S, Noda A, Iwamoto K, Kawano N, Okuda M, Ozaki N. Poor sleep quality impairs cognitive performance in older adults. J Sleep Res. 2013;22(5):535–541. doi:10.1111/jsr.12054
4. Wu X, Zhang N, Chao J, Liu Y, Zhang B. Sex-specific in the association between depressive symptoms and risk of cognitive impairment in Chinese older adults. Arch Psychiatr Nurs. 2024;52:69–75. doi:10.1016/j.apnu.2024.07.012
5. Lim AS, Kowgier M, Yu L, Buchman AS, Bennett DA. Sleep fragmentation and the risk of incident alzheimer’s disease and cognitive decline in older persons. Sleep. 2013;36(7):1027–1032. doi:10.5665/sleep.2802
6. Osorio RS, Pirraglia E, Agüera-Ortiz LF, et al. Greater risk of Alzheimer’s disease in older adults with insomnia. J Am Geriatr Soc. 2011;59(3):559–562. doi:10.1111/j.1532-5415.2010.03288.x
7. Yaffe K, Laffan AM, Harrison SL, et al. Sleep-disordered breathing, hypoxia, and risk of mild cognitive impairment and dementia in older women. JAMA. 2011;306(6):613–619. doi:10.1001/jama.2011.1115
8. Borzová C, Jirák R, Holíková M, Kozelek P. Nespavost a jiné poruchy spánku pro nelékařské zdravotnické obory. Praha: Grada Publishing; 2009.
9. Bruyneel M. Sleep disturbances in menopausal women: aetiology and practical aspects. Maturitas. 2015;81(3):406–409. doi:10.1016/j.maturitas.2015.04.017
10. Otte JL, Rand KL, Landis CA, et al. Confirmatory factor analysis of the pittsburgh sleep quality index in women with hot flashes. Menopause. 2015;22(11):1190–1196. doi:10.1097/GME.0000000000000459
11. Kravitz HM, Ganz PA, Bromberger J, Powell LH, Sutton-Tyrrell K, Meyer PM. Sleep difficulty in women at midlife: a community survey of sleep and the menopausal transition. Menopause. 2003;10(1):19–28. doi:10.1097/00042192-200310010-00005
12. Baker FC, de Zambotti M, Colrain IM, Bei B. Sleep problems during the menopausal transition: prevalence, impact, and management challenges. Nat Sci Sleep. 2018;10:73–95. doi:10.2147/NSS.S125807
13. Smith RL, Flaws JA, Mahoney MM. Factors associated with poor sleep during menopause: results from the midlife women’s health study. Sleep Med. 2018;45:98–105. doi:10.1016/j.sleep.2018.01.012
14. Citterbart K, Čech E, Donát J, et al. Gynekologie. Praha: Galén; 2001.
15. Šuška P. Vybrané Kapitoly z Gynekológie. Bratislava: Univerzita Komenského v Bratislave; 2013.
16. Sherwin BB. Estrogen and cognitive functioning in women. Proc Soc Exp Biol Med. 1998;217(1):17–22. doi:10.3181/00379727-217-4420
17. Bagger YZ, Tanko LB, Alexandersen P, Qin G, Christiansen C. Early postmenopausal hormone therapy may prevent cognitive impairment later in life. Menopause. 2005;12(1):12–17.
18. Weber MT, Maki PM, McDermott MP. Cognition and mood in perimenopause: a systematic review and meta-analysis. J Steroid Biochem Mol Biol. 2014;142:90–98. doi:10.1016/j.jsbmb.2013.06.001
19. Vega JN, Zurkovsky L, Albert K, et al. Altered brain connectivity in early postmenopausal women with subjective cognitive impairment. Front Neurosci. 2016;10:433. doi:10.3389/fnins.2016.00433
20. Albert K, Hiscox J, Boyd B, Dumas J, Taylor W, Newhouse P. Estrogen enhances hippocampal gray-matter volume in young and older postmenopausal women: a prospective dose-response study. Neurobiol Aging. 2017;56:1–6. doi:10.1016/j.neurobiolaging.2017.03.033
21. LeBlanc M, Beaulieu-Bonneau S, Mérette C, Savard J, Ivers H, Morin CM. Psychological and health-related quality of life factors associated with insomnia in a population-based sample. J Psychosom Res. 2007;63(2):157–166. doi:10.1016/j.jpsychores.2007.03.004
22. Tworoger SS, Lee S, Schernhammer ES, Grodstein F. The association of self-reported sleep duration, difficulty sleeping, and snoring with cognitive function in older women. Alzheimer Dis Assoc Disord. 2006;20(1):41–48. doi:10.1097/01.wad.0000201850.52707.80
23. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
24. Ouzzani M, Hammady H, Fedorowicz Z, Elmagarmid A. Rayyan: a web and mobile app for systematic reviews. Syst Rev. 2016;5:210.
25. Paludo AC, Paravlic A, Dvořáková K, Gimunová M. The effect of menstrual cycle on perceptual responses in athletes: a systematic review with meta-analysis. Front Psychol. 2022;13:926854. doi:10.3389/fpsyg.2022.926854
26. Beníčková M, Gimunová M, Paludo AC. Effect of circadian rhythm and menstrual cycle on physical performance in women: a systematic review. Front Physiol. 2024;15:1347036. doi:10.3389/fphys.2024.1347036
27. Gombarčíková T, Svobodová L, Svobodová A, Gimunová M. The effect of physical activity intervention and detraining on postmenopausal osteopenia and osteoporosis: a systematic review. Front Sports Act Living. 2025;7:1655404. doi:10.3389/fspor.2025.1655404
28. Meignié A, Duclos M, Carling C, et al. The effects of menstrual cycle phase on elite athlete performance: a critical and systematic review. Front Physiol. 2021;12:654585. doi:10.3389/fphys.2021.654585
29. Benýšková E, Gimunová M. The Effect of Sleep Deprivation on Cognitive Function in Postmenopausal Women [Master’s Thesis]. 2025.
30. Lambiase MJ, Gabriel KP, Kuller LH, Matthews KA. Sleep and executive function in older women: the moderating effect of physical activity. J Gerontol a Biol Sci Med Sci. 2014;69(9):1170–1176. doi:10.1093/gerona/glu038
31. Thurston RC, Maki P, Chang Y, et al. Menopausal vasomotor symptoms and plasma Alzheimer disease biomarkers. Am J Obstet Gynecol. 2024;230(3):
32. Unkenstein AE, Bryant CA, Judd FK, Ong B, Kinsella GJ. Understanding women’s experience of memory over the menopausal transition: subjective and objective memory in pre-, peri-, and postmenopausal women. Menopause. 2016;23(12):1319–1329. doi:10.1097/GME.0000000000000705
33. Bojar I, Raczkiewicz D, Gujski M, et al. Oestrogen receptor α gene polymorphisms, insomnia, and cognitive functions in perimenopausal and postmenopausal women in non-manual employment. Arch Med Sci. 2020;18(5):1318–1328. doi:10.5114/aoms.2020.94977
34. Curtis AF, Costa AN, Musich M, et al. Sex as a moderator of the sleep and cognition relationship in middle-aged and older adults: a preliminary investigation. Behav Sleep Med. 2024;22(1):14–27. doi:10.1080/15402002.2023.2177293
35. Devore EE, Grodstein F, Duffy JF, Stampfer MJ, Czeisler CA, Schernhammer ES. Sleep duration in midlife and later life in relation to cognition. J Am Geriatr Soc. 2014;62(6):1073–1081. doi:10.1111/jgs.12790
36. Diem SJ, Blackwell TL, Stone KL, et al. Measures of sleep-wake patterns and risk of mild cognitive impairment or dementia in older women. Am J Geriatr Psychiatry. 2016;24(3):248–258. doi:10.1016/j.jagp.2015.12.002
37. Djonlagic I, Aeschbach D, Harrison SL, et al. Associations between quantitative sleep EEG and subsequent cognitive decline in older women. J Sleep Res. 2019;28(3):e12666. doi:10.1111/jsr.12666
38. Garcia MC, Pompéia S, Hachul H, et al. Is mindfulness associated with insomnia after menopause? Menopause. 2014;21(3):301–305. doi:10.1097/GME.0b013e31829996fc
39. Hestiantoro A, Jasirwan OS, Wiwie M, Shadrina A, Ibrahim N, Astuti BPK. Low estradiol levels escalate menopausal symptoms leading to mild cognitive impairment in postmenopausal women. Med J Indones. 2019;28(1):40–46. doi:10.13181/mji.v28i1.2447
40. Chen JC, Espeland MA, Brunner RL, et al. Sleep duration, cognitive decline, and dementia risk in older women. Alzheimers Dement. 2016;12(1):21–33. doi:10.1016/j.jalz.2015.03.004
41. Kimura N, Sasaki Y, Masuda T, et al. Lifestyle factors that affect cognitive function-a longitudinal objective analysis. Front Public Health. 2023;11:1215419. doi:10.3389/fpubh.2023.1215419
42. Legault J, Thompson C, Moullec G, et al. Age- and sex-specific associations between obstructive sleep apnea risk and cognitive decline in middle-aged and older adults: a 3-year longitudinal analysis of the Canadian longitudinal study on aging. Sleep Med. 2023;112:77–87. doi:10.1016/j.sleep.2023.09.029
43. Li W, Sun N, Kondracki A, Sun W. Sex, sleep duration, and the association of cognition: findings from the China health and retirement longitudinal study. Int J Environ Res Public Health. 2021;18(19):10140. doi:10.3390/ijerph181910140
44. Nascimento M, Maduro PAM, Rios PMB, et al. Effects of 12 weeks of physical-cognitive dual-task training on executive functions, depression, sleep quality, and quality of life in older adult women: a randomized pilot study. Sustainability. 2023;15(1):97. doi:10.3390/su15010097
45. Rani R, Arokiasamy P, Selvamani Y, Sikarwar A. Gender differences in self-reported sleep problems among older adults in six middle-income countries: a cross-sectional study. J Women Aging. 2022;34(5):605–620. doi:10.1080/08952841.2021.1965425
46. Spira AP, Stone KL, Redline S, et al. Actigraphic sleep duration and fragmentation in older women: associations with performance across cognitive domains. Sleep. 2017;40(8):zsx073. doi:10.1093/sleep/zsx073
47. Swanson LM, Hood MM, Hall MH, et al. Associations between sleep and cognitive performance in a racially/ethnically diverse cohort: the study of women’s health across the nation. Sleep. 2021;44(2):zsaa182. doi:10.1093/sleep/zsaa182
48. Kang JE, Lim MM, Bateman RJ, et al. Amyloid-beta dynamics are regulated by orexin and the sleep-wake cycle. Science. 2009;326(5955):1005–1007. doi:10.1126/science.1180962
49. Xie L, Kang H, Xu Q, et al. Sleep drives metabolite clearance from the adult brain. Science. 2013;342(6156):373–377. doi:10.1126/science.1241224
50. Park H, Tsai KM, Dahl RE, et al. Sleep and inflammation during adolescence. Psychosom Med. 2016;78(6):677–685. doi:10.1097/PSY.0000000000000340
51. Irwin MR. Sleep and inflammation: partners in sickness and in health. Nat Rev Immunol. 2019;19(11):702–715. doi:10.1038/s41577-019-0190-z
52. Tan X, van Egmond L, Chapman CD, Cedernaes J, Benedict C. Aiding sleep in type 2 diabetes: therapeutic considerations. Lancet Diabetes Endocrinol. 2018;6(1):60–68. doi:10.1016/S2213-8587(17)30233-4
53. Henderson VW. Three midlife strategies to prevent cognitive impairment due to Alzheimer’s disease. Climacteric. 2014;17:38–46.
54. Alhola P, Polo-Kantola P. Sleep deprivation: impact on cognitive performance. Neuropsychiatr Dis Treat. 2007;3(5):553–567.
55. Lo JC, Groeger JA, Santhi N, et al. Effects of partial and acute total sleep deprivation on performance across cognitive domains, individuals and circadian phase. PLoS One. 2012;7(9):e45987. doi:10.1371/journal.pone.0045987
56. Dolev T, Maoz I, Zubedat S, et al. Attention regulation among sleep-deprived air-force pilots. J Neurosci Res. 2025;103(6):e70052. doi:10.1002/jnr.70052
57. Sabia S, Fayosse A, Dumurgier J, et al. Association of sleep duration in middle and old age with incidence of dementia. Nat Commun. 2021;12(1):2289. doi:10.1038/s41467-021-22354-2
58. Chen C, Zissimopoulos JM. Racial and ethnic differences in trends in dementia prevalence and risk factors in the United States. Alzheimers Dement. 2018;4:510–520. doi:10.1016/j.trci.2018.08.009
59. Hall MH, Matthews KA, Kravitz HM, et al. Race and financial strain are independent correlates of sleep in midlife women: the SWAN sleep study. Sleep. 2009;32(1):73–82.
60. Matthews KA, Zheng H, Kravitz HM, et al. Are inflammatory and coagulation biomarkers related to sleep characteristics in mid-life women?: study of Women’s Health across the Nation sleep study. Sleep. 2010;33(12):1649–1655. doi:10.1093/sleep/33.12.1649
61. Salthouse TA. When does age-related cognitive decline begin? Neurobiol Aging. 2009;30(4):507–514. doi:10.1016/j.neurobiolaging.2008.09.023
62. Ophey A, Brijoux T, Conrad A, Folkerts AK, Zank S, Kalbe E. Cognition in people aged 80 years and older: determinants and predictors of change from a population-based representative study in Germany. J Frailty Aging. 2023;12(3):182–188. doi:10.14283/jfa.2023.20
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.