Back to Journals » Journal of Multidisciplinary Healthcare » Volume 18
The Effect of Self Identity on Increasing Iron Tablet Adherence Among High School Adolescent Girls Through Health Belief Model as Mediator Variables
Authors Salim LA, Silitonga HTH, Nurmala I, Muthmainnah M, Devi YP, Salsabila AC, Restuti DY
Received 12 March 2025
Accepted for publication 11 July 2025
Published 23 July 2025 Volume 2025:18 Pages 4173—4183
DOI https://doi.org/10.2147/JMDH.S527641
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr David C. Mohr
Lutfi Agus Salim,1 Hanna Tabita Hasianna Silitonga,2 Ira Nurmala,1 Muthmainnah Muthmainnah,1 Yuli Puspita Devi,1 Annisa Clara Salsabila,3 Dini Yulia Restuti4
1Department of Epidemiology, Biostatistics, Population Studies, and Health Promotion, Faculty of Public Health, Universitas Airlangga, Surabaya, East Java, Indonesia; 2Faculty of Medicine, Ciputra University, Surabaya, East Java, Indonesia; 3Department of Health Policy and Administration, Faculty of Public Health, Universitas Airlangga, Surabaya, East Java, Indonesia; 4Department of Health Resources, East Java Provincial Health Office, Surabaya, East Java, Indonesia
Correspondence: Lutfi Agus Salim, Department of Epidemiology, Biostatistics, Population Studies, and Health Promotion, Faculty of Public Health, Universitas Airlangga, Campus C Unair, Mulyorejo Sub-District, Surabaya, East Java, 60115, Indonesia, Tel +62 31 5920948, Email [email protected]
Introduction: Adherence to taking iron tablets is a challenge in the Fe supplementation program. Self-identity is an essential factor to consider while enhancing teenage adherence to taking Fe tablets. Health Belief Model showed that likelihood of action is affected by health belief variables and eventually affected the actual behavior which is the adherence.
Purpose: The purpose of this study is to examine the effect of high school adolescent self-identity on iron tablet consumption adherence using HBM variables such as expectation, perceived susceptibility and severity, and perceived threat, as well as iron tablet problem-solving abilities which represent the likelihood of action variable.
Material and Methods: This was an analytical observational study using a cross-sectional design. The sample size was 375 adolescent girls students from Sidoarjo Regency, Indonesia. The sample approach used was multistage random sampling. Data collection was conducted from October to December 2022. Data analysis was carried out from December 2022 to February 2023. The data for this study was analyzed using structural equation model-partial least square with Smart-Partial Least Squares (PLS) software.
Results: Self identity was found to have significant effect on expectation (p-value < 0.001), perceived susceptibility and severity (p-value < 0.001), and problem solving ability (p-value 0.005). Self-identity also influences adolescents adherence through the problem solving ability p-value 0.042) and expectation (p-value < 0.001) and both problem solving ability and expectation (p-value 0.001).
Conclusion: Adolescents’ self-identity significantly influences their expectations and problem-solving abilities, which represent key constructs of the Health Belief Model, namely perceived benefits and likelihood of action, and these factors positively affect adherence to iron tablet consumption. The findings suggest that strengthening HBM-related constructs such as expectations, perceived susceptibility, and problem-solving abilities through self-identity development may effectively improve iron tablet adherence among high school adolescents.
Keywords: adolescent health, self identity, belief, problem solving ability, iron tablet, public health
Introduction
Iron supplementation is recommended as prevention of anemia among adolescent girls. WHO recommended intermittent iron and folic acid (IFA) supplementation (once weekly) as a public health strategy for menstruating women in areas with anaemia prevalence ≥20%, aiming to improve haemoglobin levels, iron status, and reduce anaemia risk.1 In settings where anaemia prevalence is ≥40%, daily iron supplementation is advised, particularly for menstruating women and adolescent girls, to prevent anaemia and iron deficiency.1,2 Iron supplementation is recommended to prevent anemia in women of reproductive age, aligning with SDG 3: Good Health and Well-Being,3 by improving hemoglobin levels and reducing the risk of iron deficiency anemia. Research indicates that adolescent adherence to iron supplements is a key factor in reducing anemia prevalence.4 This also supports SDG 5: Gender Equality, by promoting the health and well-being of adolescent girls and young women. Research shows that an indicator of the success of this program is the adherence of adolescents in taking iron supplements which ultimately succeeded in reducing the prevalence of anemia.5 From this research, it was found that several important elements in achieving compliance in adolescent girls above 85% are the knowledge of knowing the consequences of anemia, the benefits of iron supplementation, having shared days to take iron supplements, ongoing monitoring, service packages including counseling, and support to improve motivation and interests of adolescents. In some places, the low compliance of young women in consuming iron tablets is a problem in the success of this program.6
In Indonesia, 18.4% of young women aged 15–24 years experienced anemia in 2013, and then increased to 32% in 2018.7 Based on these data, anemia in teenagers in Indonesia is a moderate public health problem. Previous studies conducted in East Java have reported that the prevalence of anaemia among adolescent girls ranges from 13.9% to 29.9%.8–10 In comparison, the prevalence in other developing countries remains considerably high, with estimates ranging from 44% to 48% in India,11,12 14% to 18% in Nepal,13,14 and 38% to 51% in Bangladesh.15,16 These findings highlight that adolescent girls continue to represent a high-risk group for anaemia, particularly in low- and middle-income settings, due to increased physiological demands and potential nutritional deficiencies during this critical developmental stage. There are many prevention strategies for anemia such as food diversification, increasing knowledge and fortification and iron supplementation. This study focuses specifically on iron supplementation due to its relevance as a government-recommended, school-based intervention targeting adolescent girls.17 Weekly iron–folic acid (IFA) supplementation offers a practical and immediate solution to prevent anaemia in settings where dietary improvements alone may be insufficient or difficult to achieve in the short term. Iron supplementation among adolescent girls has been shown to improve haemoglobin levels, enhance serum ferritin concentrations, and reduce the prevalence of anaemia.18 This approach is supported by WHO recommendations and national guidelines, particularly for areas with moderate to high anaemia prevalence. This approach has been widely recommended in regions with moderate to high anaemia prevalence, where achieving sufficient iron intake through diet alone may be challenging due to socioeconomic and cultural factors.1
The Government of Indonesia has issued guidelines for iron supplementation among school-aged adolescent girls. The program targets all girls aged 12 to 18 years, providing iron and folic acid (IFA) tablets containing 60 mg of elemental iron and 0.4 mg of folic acid. The supplementation is administered once weekly throughout the year and is carried out simultaneously within schools according to schedules set by each educational institution.17 The results of the 2018 Basic Health Research show that the proportion of adolescent girls aged 10–19 years who had received iron tablet in the last 12 months was 76.2%. These teenagers receive the most iron tablet at school compared to health facilities or on their own initiative.7,19 Adolescents who receive iron tablet are expected to consume the iron tablet as recommended (right dose, right method, right amount). In East Java Province, more teenagers receive iron tablet from school (83%), then from their own initiative (11%) and from health facilities (9.7%). The East Java provincial report shows that the proportion of teenagers who take iron tablet more or equal to 52 tablets in one year is only 2.05%.20 This is the proportion of those who received iron tablet from school. Adolescents who received iron tablet from health facilities had a proportion taking iron tablet more than 52 tablets of 3.55% and only 1.44% took iron tablet more than 52 tablets from the proportion of teenagers who obtained iron tablet on their own initiative. The most common reasons for not taking iron tablet are feeling it is not necessary, the taste is smelly or unpleasant, and forgetting.20,21
Adolescence is a critical transition phase from child to adult. In this phase, physical and hormonal changes occur which will affect the psychological and social (psychosocial). Some psychosocial changes in adolescents can include an identity crisis, mental instability, increased verbal ability to express oneself, feeling important to have friends, reduced respect and finding fault with parents, and the influence of peers.22 According to Marcia, an identity crisis is a period for teenagers to make conscious decisions. During this period, commitment is formed as a personal investment in work or a belief system (ideology). Several factors that influence identity status during adolescence are family factors and personality.23 According to Orji et al self identity has a direct and indirect relationship with health behavior where perceived benefit, barrier, susceptibility and severity mediate between these two variables.24
Self-identity is important variable to consider in increasing adolescents’ adherence with taking iron tablets, because generally adolescents are not given the opportunity to make decisions during this period, due to perceived inability both in terms of cognition, morals and psychology. Adolescents are often considered a vulnerable group. Berzonsky stated that individuals differ in the social-cognitive processes they use to form and maintain a sense of self-identity. In this study, teenagers’ self-identity was measured using Berzonsky’s identity style, where there is a relationship between teenagers’ identity styles and coping strategies.25
According to Health Belief Model, likelihood of engaging health behavior is affected by health belief variables, namely, perceived severity, perceived susceptibility, perceived benefit and perceived barriers.26 A limitation of the HBM is that it does not consider attitudes or other individual determinants related to behavior change such as self-identity. The variables likelihood of action in HBM comes before the action or behavior change, so in this research, the likelihood of action was measured by the iron tablet problem solving ability that then affect the adherence of taking Fe supplementation. Therefore, this research is aimed to find the effect of self identity to adolescent’s adherence in taking Fe supplementation through HBM variables. This study examine the effects among latent variables using Partial Least Squares Structural Equation Modeling (PLS-SEM). Unlike traditional correlation analysis, PLS-SEM allows for the estimation of direct, indirect, and total effects between constructs within a theoretical framework. Although this research employs a cross-sectional design, the use of PLS-SEM justifies the investigation of effects in terms of statistical influence, rather than strict causality.
Materials and Methods
Design
This research was an analytical observational study with a cross-sectional design. It was conducted in Sidoarjo Regency, East Java Province, Indonesia. It is directly borders Surabaya City, and is a peri-urban area that continues to experience rapid development. Data collection was conducted from October to December 2022. Data analysis was carried out from December 2022 to February 2023. Sidoarjo Regency comprises 17 subdistricts and 71 senior high schools, including 13 public and 58 private institutions. In 2022, the total number of senior high school students was 26,486, consisting of 11,486 males and 15,000 females.
Participants and Sampling Techniques
The study population consisted of 15,000 adolescent girls in high school. The sample size was 375 respondents. Sample size determination in this study was based on multiple considerations. First, to estimate the proportion of adherence to iron tablet consumption among adolescent girls, the sample size was calculated using the finite population correction (FPC) formula:

where Z=1.96 (for a 95% confidence level), p=0.5 (to reflect maximum variability), d=0.05, and the total population N=15,000. This resulted in a minimum required sample size of 375 participants. Second, to ensure adequate statistical power, based on Cohen’s (1992) guidelines for power analysis, the minimum required sample size was determined to ensure the detection of a small effect size, represented by an R² value of at least 0.10, with a statistical power of 80% and a significance level of 5%.27 Given that the most complex endogenous construct in the structural model is predicted by seven independent variables, the corresponding minimum sample size is 137. Therefore, the chosen sample size which is 375 respondents, was deemed sufficient and appropriate to support the analytical approach and hypotheses testing.
The Inclusion and Exclusion Criteria
The inclusion criteria for this study were: (a) high schools that had implemented an iron supplementation (IFA) program for at least three months prior to the study; (b) adolescent girls aged 15–18 years; and (c) respondents who had previously received information or education about the iron supplementation program. The exclusion criteria included: (a) schools that did not grant permission for data collection; (b) schools that enforced mandatory, scheduled group iron tablet consumption; and (c) students with special conditions such as chronic illness, disabilities, chronic depression, or other conditions that could hinder their ability to take iron tablets regularly on a weekly basis. Before the study was conducted, informed consent was obtained from the parents of all student respondents, in accordance with ethical research standards.
Data Collection Procedure
The sampling technique used was multistage random sampling. The sampling process was conducted in three stages. In the first stage, a study area was selected from one of the three administrative zones of Sidoarjo Regency—North, West, or South—using simple random sampling. In the second stage, a school within the selected area was randomly chosen. In the third stage, the sample units (students) were selected from each school according to inclusion criteria and exclusion criteria. A total of 37 to 38 female students were recruited from each selected school, proportionally distributed across grades 10, 11, and 12.
Instruments and Variables
The instruments used in this research are questionnaires. The self-identity variable is measured using the ISI-5 questionnaire.28 There were four indicators of self-identity which were informative style, normative style, diffuse-avoidant style and commitment. The HBM variable was measured using a modified instrument from several sources and then tested again to obtain a valid and reliable instrument.29 The HBM variables consisted of three variables which were expectation, perceived susceptibility and severity, perceived threat. Expectation contained two indicators which were perceived benefit and perceived barrier. The perceived susceptibility and severity also contained two indicators. The perceived threat contained one indicator. The iron tablet problem solving ability variable was measured using a modified instrument from various sources.30 There were four indicators in this construct which were define problem, discover alternatives, decide solution, and implementation. Iron tablet adherence was measured with questionnaire about completeness, regularity and accuracy of drinking iron tablet from high school teenage girls in three months period of supplementation. The questionnaire contains 9 questions using a Likert scale (scale 4).
Validity and Reliability Analysis
To see the validity of each construct, we use composite reliability which can be seen in Table 1 and to see the validity can use the discriminant validity from the Fornell-Larcker analysis in Table 2.
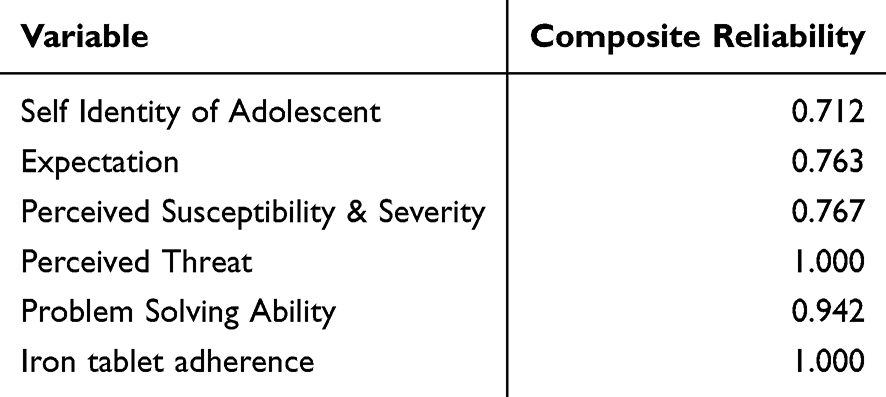 |
Table 1 Composite Reliability of the Variables |
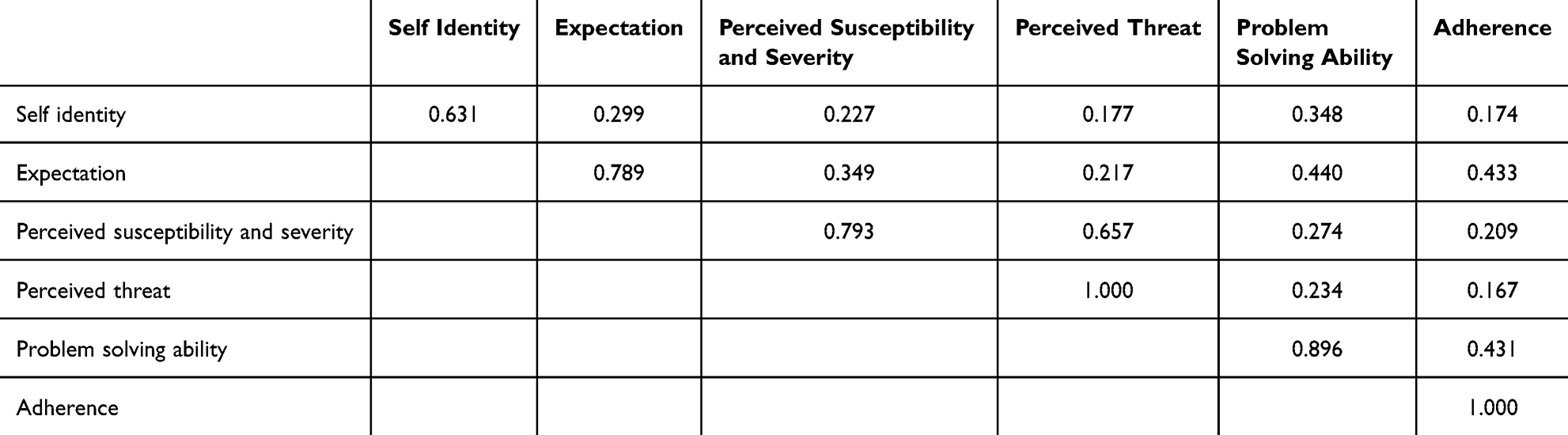 |
Table 2 Discriminant Validity of the Research |
Table 1 shows the value of composite reliability. Composite reliability is used to see the consistency of internal reliability. Cronbach alpha can also be used to see the consistency of internal reliability in social science research but is a conservative measurement in PLS-SEM.31 As a substitute, composite reliability can be used and values greater than 0.6 indicate a high level of internal reliability consistency.31,32 The results of data processing show that all variables have a composite reliability above 0.6. Table 2 shows the discriminant validity seen by assessing the square root of the AVE of each latent variable. If the value is greater than the correlation between the values of other latent variables then the result is valid. The results of discriminant validity can be seen from the Fornell-Larcker analysis. The results of the final tests showed that the composite reliability values of all variables were more than 0.7, and the Fornell-Larcker analysis showed well-established results.
Data Analysis
The descriptive analysis for ordinal and nominal data uses frequency tables and percentages using SPSS software. Analysis for ratio data uses average (mean) and standard deviation, The inferential analysis used in this study is path analysis in structural equation model partial least square using Smart-PLS software.
Analytical Framework
Analytical framework of iron tablet adherence among adolescent girls can be seen in Figure 1.
 |
Figure 1 Analytical framework of iron tablet adherence among adolescent girls. |
Results
Descriptive Analysis
Sociodemographic Characteristic
Table 3 showed the sociodemographic characteristics of respondents. The participants in this study consisted of adolescent girls aged between 15 and 18 years. The majority were 16 years old (n = 134; 35.7%), followed by 17 years old (n = 104; 27.7%), 15 years old (n = 83; 22.1%), and 18 years old (n = 54; 14.4%). This age distribution reflects the typical age range of senior high school students in Indonesia and represents a critical developmental period for identity formation and health behavior establishment. In terms of academic level, the participants were relatively evenly distributed across the three school grades. Most of the respondents were in grade X (n = 149; 39.7%), followed by grade XII (n = 118; 31.5%), and grade XI (n = 108; 28.8%). This balanced distribution allows for the comparison of behavioral and cognitive aspects, such as iron supplement adherence, across different stages of adolescence and educational experiences. These demographic characteristics provide a comprehensive representation of the adolescent population in senior high schools, ensuring the relevance of the findings for interventions targeting this age group.
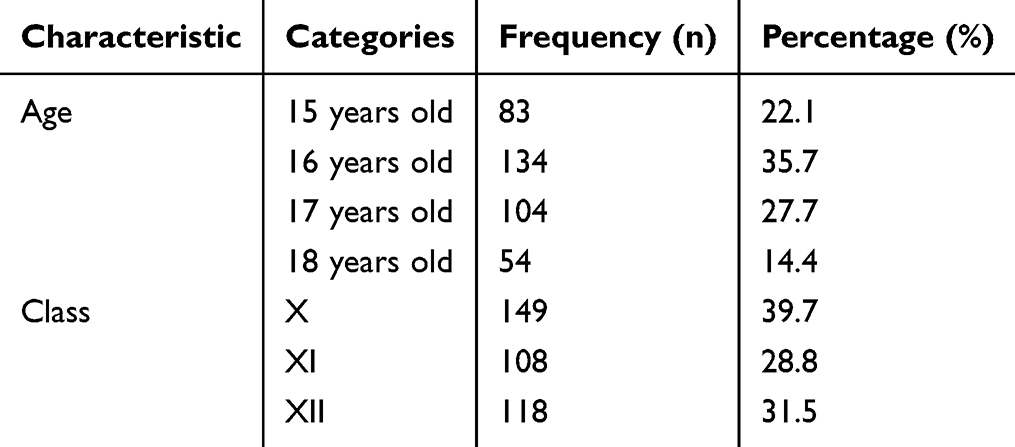 |
Table 3 Sociodemographic Characteristic of Respondents |
Univariate Analysis
Table 4 showed the descriptive statistic of variables. The average scores of self-identity indicators showed that participants had the highest mean in the informative style (M = 85.75, SD = 9.32), followed by the normative style (M = 73.07, SD = 11.51), commitment (M = 71.01, SD = 16.60), and the lowest in diffuse-avoidant style (M = 61.16, SD = 12.64).
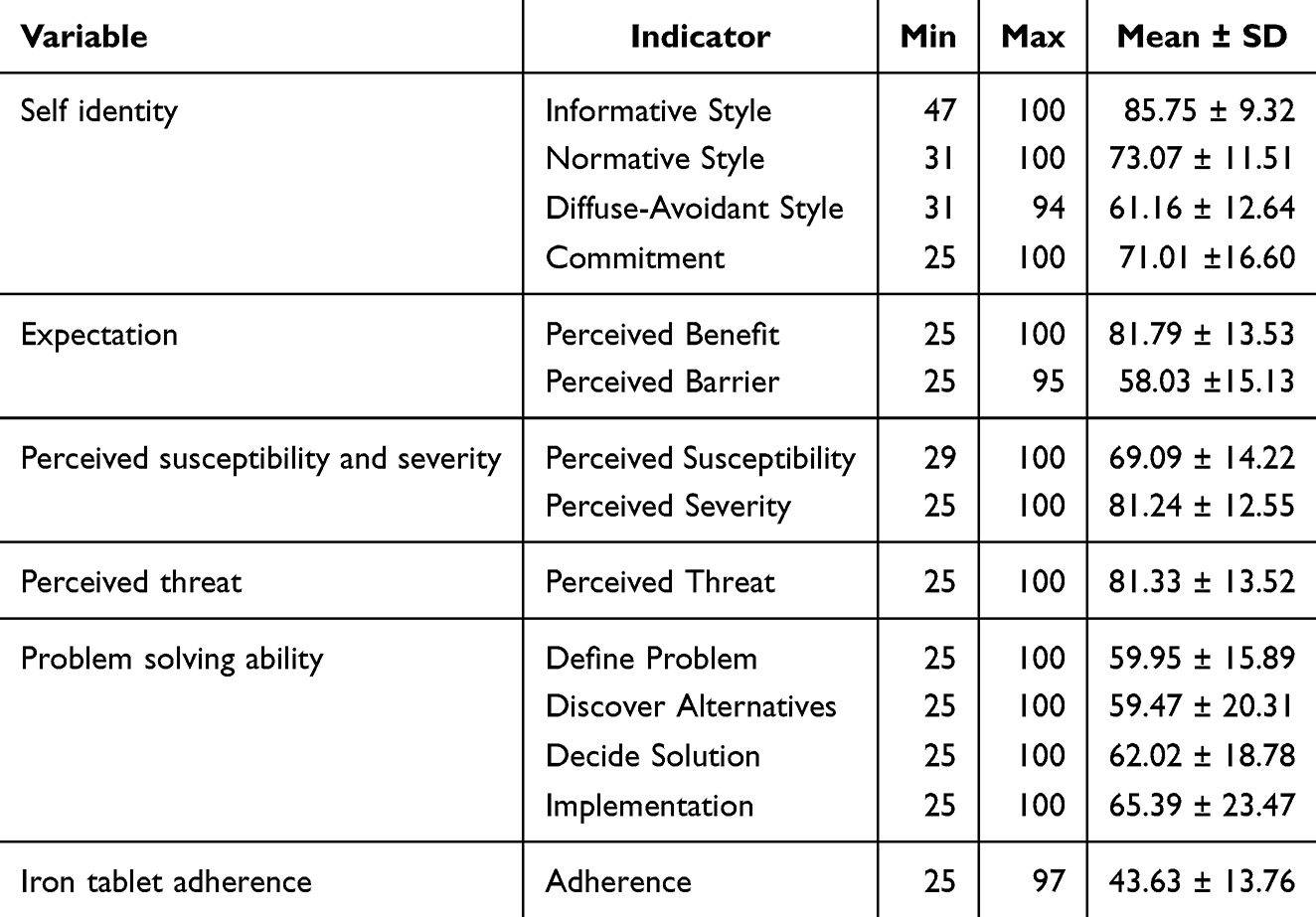 |
Table 4 Univariate Analysis of the Variables’ Indicators (n = 375) |
Regarding expectations, the mean perceived benefit was relatively high (M = 81.79, SD = 13.53), while perceived barrier was lower (M = 58.03, SD = 15.13). Perceptions of susceptibility (M = 69.09, SD = 14.22) and severity (M = 81.24, SD = 12.55) contributed to a high perceived threat score (M = 81.33, SD = 13.52).
Problem-solving ability indicators were moderate, ranging from a mean of 59.47 (discover alternatives) to 65.39 (implementation). The mean score of iron tablet adherence was relatively moderate (M = 43.63, SD = 13.76), indicating potential challenges in compliance.
Bivariate Analysis
Table 5 showed the bivariate analysis between two variables. The path analysis demonstrated that self-identity significantly influenced expectation (C = 0.299, p < 0.001) and perceived susceptibility and severity (C = 0.215, p < 0.001). However, its direct effect on perceived threat was not statistically significant (C = 0.034, p = 0.533). Self-identity also had a significant direct effect on iron tablet problem-solving ability (C = 0.158, p = 0.005).
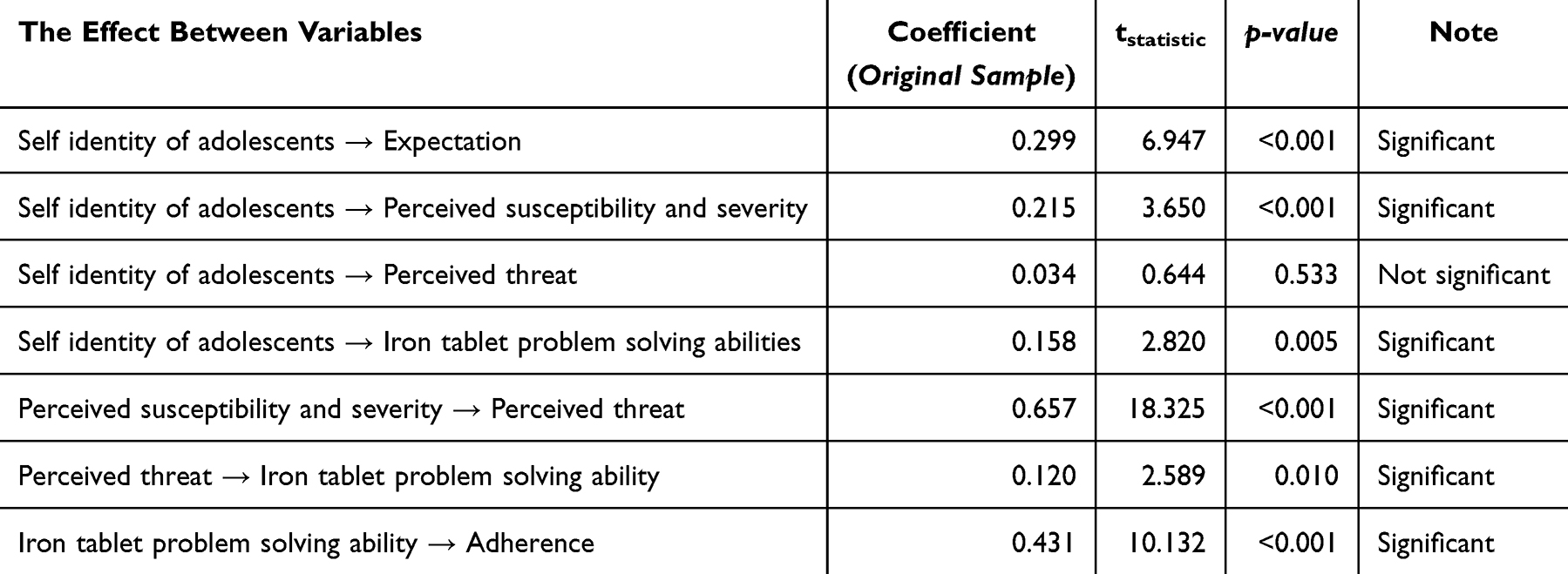 |
Table 5 The Effect Between Variables of Research |
The perceived susceptibility and severity had a strong and significant effect on perceived threat (C = 0.657, p < 0.001), which in turn significantly influenced problem-solving ability (C = 0.120, p = 0.010). Finally, problem-solving ability showed a strong, significant association with adherence to iron tablet consumption (C = 0.431, p < 0.001).
These results indicate that self-identity plays a central role in shaping adolescents’ expectations and risk perceptions, which in turn affect their cognitive ability to solve problems related to adherence. Notably, the indirect pathway through perceived threat and problem-solving appears to be a critical mechanism linking identity to behavior.
Path Analysis
Table 6 shows the path analysis from self identity to adherence. The mediation analysis revealed several significant indirect pathways between self-identity and iron tablet adherence. The pathway from self-identity through problem-solving ability to adherence was statistically significant (C = 0.035, p = 0.042), indicating that adolescents with stronger self-identity are more likely to develop better problem-solving abilities, which in turn enhances adherence. The pathway from self-identity through expectation to adherence was also significant (C = 0.092, p < 0.001), suggesting that expectations mediate the relationship between identity and adherence behavior.
 |
Table 6 Path Analysis of the Research |
A more complex mediation path, from self-identity through expectation, then problem-solving ability, to adherence, was found to be significant as well (C = 0.024, p = 0.001), reinforcing the layered influence of cognitive and motivational factors in behavior change. In contrast, the pathway from self-identity through perceived susceptibility and severity, perceived threat, and problem-solving ability to adherence did not reach statistical significance (C = 0.004, p = 0.063). This suggests that while threat perception is conceptually important, its full mediation chain in this model may be weaker or more context-dependent. These findings underscore the pivotal role of expectation and problem-solving abilities as mediators in the relationship between self-identity and adherence behavior, highlighting their potential as targets for intervention.
Discussion
The self-identity of adolescent girls has a significant effect on their belief in iron tablet consumption as a prevention of iron deficiency anemia. The majority of respondents in this study had a high informative style self-identity. Informative style is a strategy that shows individuals actively searching, analyzing, and evaluating relevant information during the identity formation process. Teens who have this style tend to be critical, skeptical of their views, open to new information, and flexible to feedback, contrary to their preferred identity. Therefore, they try to evaluate and change their chosen identity.28 The study showed that the higher the level of informative style of a teenager, the more confident they were in iron tablet. Teens with informative identity styles will then have an open attitude to new information that can influence beliefs about iron tablet as well to increase. Apart from that, self-identity might have a strong correlation with perceived self-efficacy, which is the belief and confidence in the ability of one self to do something. Perceived self-efficacy is proven to have significant influence to the intention of adolescent girls in consuming Fe tablet.33
Berzonsky et al (2007) showed that adolescent identity styles are formed from communication between adolescents and their parents. The parent-adolescent relationship perceived by adolescents was found to be related to identity styles in late adolescence. Parenting practices with authoritative styles, which include communicating explanations, being responsive, and making reasonable demands in a climate of warmth and acceptance, are associated with adolescent identity formation with informative styles, whereas permissive parenting styles correlate with adolescent identity formation with diffuse-avoidant styles. The normative style is related to strict authoritarian upbringing and family cohesion, care, and emotional closeness34 Previous research related to differences in adolescent self-identity in perceiving quality of life has also shown how different patterns of identity formation in adolescents relate to different levels of quality of life.35 The results of this study show that adolescent self-identity can also influence perceptions of health such as perceived benefit and perceived susceptibility and severity.
Self-identity has a significant effect on adolescents’ confidence in the vulnerability and seriousness of iron deficiency anemia disease. This shows that the higher the self-identity, the higher the perceived susceptibility and severity. This explains why adolescents who are given information or knowledge have different perceptions of the severity of iron deficiency anemia due to the presence of psychological factors, namely self-identity.According to Orji et al, self-identity can influence health behaviors directly or indirectly. From self-identity research, what is meant is how a person perceives himself in relation to certain behaviors so that the role of self-identity is to motivate the person to change behavior according to his identity. Perceptions of vulnerability, severity, benefits, barriers, and cues to action mediate the relationship between self-identity and healthy behavior so that designs to enhance self-identity will be able to give rise to perceptions of vulnerability and severity, benefits and action cues while reducing perceived barriers.24
This study found that self-identity does not directly affect threat perception, but self-identity influences threat perception through mediation from vulnerability and severity perception variables. This means that efforts to improve self-identity will have more influence on the perception of vulnerability and seriousness of iron deficiency anemia than the perception of the threat of iron deficiency anemia in adolescent girls. This findings aligns with a recent study, which demonstrated that threat sensitivity mediates the relationship between perceived security and anxiety responses in adolescents, emphasizing the role of cognitive appraisals like vulnerability and severity in shaping response to health threats.36
Self-identity directly affects iron tablet problem solving ability and indirectly affects iron tablet adherence through several channels, one of which is through perceived susceptibility and severity and perceived threat. This is in line with the research of Orji et al which states that the self-identity variable is a strong determinant in the development of HBM theory and is significantly correlated with a person’s tendency to behave healthily. In their growth and development, adolescents experience a phase of identity formation. A previous study stated that a healthier identity in adolescents is significantly associated with positive self-perceptions, especially in domains such as physical appearance, close friendships, and global self-worth, which vary depending on gender and motor competence level.37 Positive identity status will affect the increase in compliance behavior of adolescent girls taking iron tablet. The identity status of adolescents can be shaped through their social environment. One of them is school involvement through the role of Guidance and Counseling. There are studies that show that reality counseling for adolescents is effective in increasing understanding of self-identity.38
The findings of this study have important public health implications. By identifying key psychosocial predictors of iron supplement adherence—particularly the role of self-identity and health beliefs—this research provides evidence to inform the design of more targeted and effective interventions for adolescent girls. Given the short but critical nature of adolescence for physical and cognitive development, timely behavioral interventions can help prevent long-term health consequences associated with iron deficiency and anemia. School-based iron–folic acid supplementation programs can be strengthened by integrating behavior change strategies that enhance self-efficacy, perceived benefits, and identity as a healthy individual. This approach aligns with national and WHO recommendations and can support efforts to reduce anemia prevalence among adolescent populations in similar peri-urban settings.
Strengths and Limitations
This study has several strengths. It offers a novel perspective by developing a predictive model of adolescent girls’ adherence to iron–folic acid (IFA) supplementation based on psychosocial factors, particularly self-identity and health beliefs. By focusing on behavioral determinants, the study contributes to a better understanding of how to tailor interventions to improve compliance with iron supplementation programs. The multi-stage random sampling method and relatively large sample size also enhance the representativeness and generalizability of the findings within the study setting.
However, this study has certain limitations. As the sample was drawn from high school adolescent girls in a peri-urban district of East Java, the generalizability of the results to other regions or populations may be limited. Differences in cultural, socioeconomic, and educational contexts could influence adherence behavior and psychosocial constructs measured in this study. Additionally, the reliance on self-reported data introduces the potential for response bias, such as social desirability or recall bias, which may affect the accuracy of reported adherence. Despite these limitations, self-reported measures remain widely used and practical in behavioral research, and efforts were made to ensure anonymity and confidentiality to minimize such biases. Future studies could benefit from including objective measures of adherence and expanding the sample to include more diverse populations to enhance external validity.
Conclusion
A self-identity of adolescent girls that can increase young women’s beliefs about the benefits of iron tablet and decrease confidence in barriers gained when taking iron tablet is an informative style of self-identity in which individuals actively seek, analyze, and evaluate relevant information. The self-identity of adolescent girls can increase their confidence in the vulnerability of being exposed and the seriousness of iron deficiency anemia disease. Positive self-identity of adolescent girls can increase adolescent fear of iron deficiency anemia if they have high belief in the vulnerability and seriousness of iron deficiency anemia disease. Adolescents who have a positive self-identity are able to overcome the obstacles that arise in taking iron tablet regularly which in turn can increase adolescent compliance in taking iron tablet supplementation.
Health education and intervention programs aimed at improving iron tablet adherence among adolescent girls should incorporate components that foster the development of a positive and informative self-identity. Specifically, programs should encourage adolescents to actively seek and critically evaluate health-related information, strengthen their belief in the benefits of iron supplementation, and increase awareness of their vulnerability to and the seriousness of iron deficiency anemia. By enhancing self-identity, such interventions can help adolescents overcome perceived barriers and improve their confidence in managing health-related challenges, ultimately leading to better compliance with iron tablet intake.
Data Sharing Statement
Derived data supporting the findings of this study are available from the corresponding author on request.
Ethics Approval
This study was carried out in accordance with the principles of the Declaration of Helsinki. This research has received a certificate of feasibility for the implementation of health research by the Health Research Ethics Commission, Faculty of Nursing, Universitas Airlangga with certificate number 2648-KEPK.
Acknowledgments
The researchers would like to express the gratitude towards all of the respondents by willing to participate in this research.
Disclosure
The authors report no conflicts of interest in this work.
References
1. WHO. Weekly Iron and Folic Acid Supplementation as an Anaemia-Prevention Strategy in Women and Adolescent Girls Lessons Learnt From Implementation of Programmes Among Non-Pregnant Women of Reproductive Age. World Health Organization; 2018.
2. World Health Organization. The double burden of malnutrition. Policy Brief. 2017.
3. World Health Organization. Daily iron supplementation in adult women and adolescent girls. 2020. Available from: https://www.who.int/publications/i/item/9789240000124.
4. Peña-Rosas JP, De-Regil LM, Garcia-Casal MN, Dowswell T. Daily oral iron supplementation during pregnancy. Cochrane Database Systematic Rev. 2015;2015(7). doi:10.1002/14651858.CD004736.pub5
5. Aguayo VM, Paintal K, Singh G. The adolescent girls’ anaemia control programme: a decade of programming experience to break the inter-generational cycle of malnutrition in India. Public Health Nutr. 2013;16(9):1667–1676. doi:10.1017/S1368980012005587
6. Hasianna Silitonga HT, Salim LA, Nurmala I, Wartiningsih M. Compliance of iron supplementation and determinants among adolescent girls: a systematic review. Iran J Public Health. 2023. doi:10.18502/ijph.v52i1.11664
7. Ministry of Health RI. National Health Basic Research. 2018. Published online 2018.
8. Mahmudiono T, Setyaningtyas SW, Ridlo IA, Rachmah Q, Nindya TS. Consumption of iron supplement and anemia among Indonesian adolescent girls. Glob J Health Sci. 2019;11(2):64. doi:10.5539/gjhs.v11n2p64
9. Sodik MA, Yudhana A, Dwianggimawati MS. Nutritional status and anemia in islamic boarding school adolescent in Kediri City East Java Indonesia. Indonesian J Nutrit Epidemiol Reproduc. 2018;1(3):172–176.
10. Soekarjo D, de Pee S, Bloem M, et al. Socio-economic status and puberty are the main factors determining anaemia in adolescent girls and boys in East Java, Indonesia. Eur J Clin Nutr. 2001;55(11):932–939. doi:10.1038/sj.ejcn.1601247
11. Patil N, Jagadeesh KV, Yamini Priyanka K, Kari A, Angolkar M. Prevalence of anemia among adolescent girls in a North Karnataka school: a cross sectional study. Int J Community Med Public Health. 2018;5(12):5360. doi:10.18203/2394-6040.ijcmph20184817
12. Chandrakumari AS, Sinha P, Singaravelu S, Jaikumar S. Prevalence of anemia among adolescent girls in a rural area of Tamil Nadu, India. J Family Med Prim Care. 2019;8(4):1414–1417. doi:10.4103/jfmpc.jfmpc_140_19
13. Ghimire M, Bhandari S, Rajbanshi M. Prevalence of anemia and its associated factors among school-going adolescent girls in schools of Dhankuta municipality, Nepal. PLOS Global Public Health. 2024;4(9):1–17. doi:10.1371/journal.pgph.0003684
14. Budhathoki L, Shrestha B, Phuyal N, Shrestha L. Prevalence of anemia in adolescent girls attending specific schools of kavrepalanchok, Nepal. J Nepal Med Assoc. 2021;59(235):284–287. doi:10.31729/jnma.6330
15. Mistry SK, Jhohura FT, Khanam F, et al. An outline of anemia among adolescent girls in Bangladesh: findings from a cross-sectional study. BMC Hematol. 2017;17(1):1–8. doi:10.1186/s12878-017-0084-x
16. Ara G, Hassan R, Haque A, et al. Anaemia among adolescent girls, pregnant and lactating women in the southern rural region of Bangladesh: prevalence and risk factors. PLoS One. 2024;19(7 July):1–17. doi:10.1371/journal.pone.0306183
17. Ministry of Health Republic of Indonesia. Pedoman Pencegahan Dan Penanggulangan Anemia Pada Remaja Putri Dan Wanita Usia Subur (Guidelines for the Anaemia Pre- Vention and Control in Adolescent Girls and Women of Childbearing Age). Ministry of Health Republic of Indonesia; 2016.
18. Silitonga HTH, Salim LA, Nurmala I. A systematic review of iron supplementation’s effects on adolescent girls. Jurnal Gizi Indonesia. 2024;12(2):60–69. doi:10.14710/jgi.12.2.60-69
19. Ansari MR, Kandarina BI, Kusmayanti N, Destriani D, Masfufah M, Fikrinnisa R. The acceptability of weekly iron-folic acid supplementation and its influencing factors among adolescent school girls in Yogyakarta city: a mix-methods study. Malays J Nutr. 2021;27(1):053–066. doi:10.31246/mjn-2020-0019
20. Ministry of Health RI. Health Basic Research 2018. Badan Litbang Kesehatan (Health Research and Development Agency); 2019.
21. Bhatt RB, Mehta HK, Khatri V, Chhaya J, Rahul K, Patel P. A study of access and compliance of iron and folic acid tablets for prevention and cure of anaemia among adolescent age group females in Ahmedabad district of India surveyed under multi indicator cluster survey 2011. Glob J Med Public Health. 2013;2(4).
22. Batubara JR. Adolescent development (Perkembangan Remaja). Sari Pediatri. 2016;12(1):21. doi:10.14238/sp12.1.2010.21-9
23. Berk LE. Development Through the Life Span. Allyn and Bacon-Pearson Education; 2018.
24. Orji R, Vassileva J, Mandryk R. Towards an effective health interventions design: an extension of the health belief model. J Public Health Inform. 2012;4.
25. Berzonsky MD. Identity Style and Coping Strategies. Vol. 60.
26. Glanz K, Lewis FM, Rimer BK. Health Behavior and Health Education Theory, Research and Practice.
27. Hair JF, Hult MGT, Ringle CM, Sarstedt M. A Primer on Partial Least Squares Structural Equation Modeling (PLS-SEM).
28. Muttaqin D. Psychometric properties of identity style inventory-5 Indonesian version: FACTOR structure, reliability, and criterion validity. J Psikol. 2021;48(1):23–40.
29. Aprianti R, Sari GM, Kusumaningrum T. Factors correlated with the intention of iron tablet consumption among female adolescents. Jurnal Ners. 2018;13(1):122–127. doi:10.20473/jn.v13i1.8368
30. Chang EC, D’Zurilla TJ, Sanna LJ. Social problem solving: theory, research, and training. Ame Psycholog Assoc. 2004. doi:10.1037/10805-000
31. Wong KKK. Partial Least Squares Structural Equation Modeling (PLS-SEM) Techniques Using SmartPLS. Vol. 24. Mark Bul; 2013.
32. Hair JF Jr, Hult GTM, Ringle CM, Sarstedt M, Danks NP, Ray S. Partial Least Squares Structural Equation Modeling (PLS-SEM) Using R a Workbook. Springer; 2021.
33. Annisa FN, Nurmala I. Influence perceived benefit and perceived self efficacy with intention of adolescent girls in consuming fe tablet. Indian J Public Health Res Dev. 2018;9(4):326. doi:10.5958/0976-5506.2018.00307.8
34. Berzonsky MD, Branje SJT, Meeus W. Identity-processing style, psychosocial resources, and adolescents’ perceptions of parent-adolescent relations. J Early Adolesc. 2007;27(3):324–345. doi:10.1177/0272431607302006
35. Oleś M. Dimensions of identity and subjective quality of life in adolescents. Soc Indic Res. 2016;126(3):1401–1419. doi:10.1007/s11205-015-0942-5
36. Carpenter C, Heeter AR, Shampine MM, et al. Threat sensitivity mediates the association between perceived safety and anxiety in adolescents from urban communities. J Psychiatr Res. 2025;181:294–297. doi:10.1016/j.jpsychires.2024.11.046
37. Timler A, McIntyre F, Harris S, Hands B. Does level of motor competence affect the associations between identity health and self-perceptions in adolescents? Hum Mov Sci. 2020;74:102710. doi:10.1016/j.humov.2020.102710
38. Maslikan M. Effectiveness of reality group counseling to improve junior high school students’ understanding of self-identity. Perspektif Ilmu Pendidikan. 2018;32(2):107–115. doi:10.21009/PIP.322.3
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.