Back to Journals » International Journal of General Medicine » Volume 18
The Effect of Recombinant Human Brain Natriuretic Peptide Combined with Xinmailong on Heart Failure and Its Impact on Cardiac Function and Inflammatory Response
Authors Ge Z, Li C ![]() , Liu Y, Sun X
, Liu Y, Sun X
Received 28 November 2024
Accepted for publication 20 March 2025
Published 7 April 2025 Volume 2025:18 Pages 1999—2008
DOI https://doi.org/10.2147/IJGM.S509162
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Zhaorui Ge,1,* Chunyan Li,2,* Yanling Liu,3 Xiujuan Sun4
1Department of Internal Medicine, Xianxian Hospital of Traditional Chinese Medicine, Xianxian, 062250, People’s Republic of China; 2Department of Cardiology, The Second Affiliated Hospital of Hebei North University, Baoding, People’s Republic of China; 3Wuqiao County Hospital of Traditional Chinese and Western Medicine Internal medicine, Wuqiao County, People’s Republic of China; 4Department of Cardiology, Wuqiao County Hospital of Integrated Chinese and Western Medicine, Wuqiao County, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Chunyan Li, Email [email protected]
Objective: To analyze the effect of recombinant human brain natriuretic peptide (rhBNP) combined with Xinmailong on heart failure and its impact on cardiac function and inflammatory response.
Methods: A retrospective analysis was conducted on the clinical data of 60 heart failure patients treated in our hospital from January 2023 to March 2024. The patients were included as research subjects to ensure the sample was representative. According to the different treatment methods, the patients were divided into two groups: the control group received only rhBNP treatment, and the experimental group received combined treatment with rhBNP and Xinmailong injection, with 30 patients in each group. The clinical effects, cardiac function, inflammatory response, and ventricular remodeling indicators of the two groups before and after treatment were observed and compared.
Results: The total clinical effective rate of the experimental group was significantly higher than that of the control group (P< 0.05). After treatment, the NT-proBNP level in the experimental group was significantly lower than that in the control group (P< 0.05). After treatment, the levels of IL-6, TNF-α, and CRP in the experimental group were significantly lower than those in the control group (P< 0.05). After treatment, the LVESD and LVEDD levels in the experimental group were significantly lower than those in the control group, while the LVEF level was higher in the experimental group than in the control group (P< 0.05). There was no significant difference in the adverse event incidence between the two groups (P> 0.05). The 6-minute walk test (6 MWT) level in the experimental group was significantly higher than in the control group (P< 0.05).
Conclusion: Recombinant human brain natriuretic peptide combined with Xinmailong is effective in treating heart failure, significantly improving cardiac function, reducing inflammatory responses, and reversing ventricular remodeling. It is also safe and beneficial for the patients’ prognosis.
Keywords: heart failure, recombinant human brain natriuretic peptide, Xinmailong injection, inflammatory response, ventricular remodeling
Introduction
Heart failure (HF) is a syndrome characterized by the heart’s inability to pump blood efficiently due to myocardial dysfunction, resulting in insufficient blood circulation to meet the metabolic needs of the body. It is usually caused by heart diseases such as hypertension, coronary artery disease, or cardiomyopathy and is characterized by symptoms such as shortness of breath, fatigue, fluid retention (eg, leg edema), and decreased exercise tolerance.1,2 Heart failure can be classified into acute or chronic forms, and based on ventricular function, it can be further divided into systolic heart failure and diastolic heart failure. As the disease progresses, heart failure can lead to multi-organ dysfunction, severely impacting the patient’s quality of life and prognosis.3,4 In recent years, the incidence of heart failure has increased due to population aging, significantly affecting patients’ quality of life and adding to the medical burden. According to data published in the Journal of the American College of Cardiology in 2014, it is estimated that there are 26 million heart failure patients worldwide, with approximately 670,000 new cases each year. The overall prevalence of heart failure in Asia is comparable to that in Western countries, ranging from 1% to 1.3%.5,6
With a deeper understanding of the pathophysiological mechanisms of heart failure, new treatment options are continuously emerging. Recombinant human brain natriuretic peptide (rhBNP) is a synthetic peptide synthesized using recombinant DNA technology, consisting of 32 amino acids with identical sequence and biological activity to endogenous BNP. Its therapeutic mechanisms include binding to natriuretic peptide receptors (NPR-A/GC-A), activating cyclic guanosine monophosphate (cGMP) pathways to induce vasodilation, reducing preload and afterload, while suppressing renin-angiotensin-aldosterone system (RAAS) and sympathetic nervous system activation.7–9 Although rhBNP use has declined in Western countries following controversies over nesiritide’s risk-benefit profile (Tsutsui),10 recent meta-analyses of Asian populations suggest preserved efficacy in acute HF when used with strict hemodynamic monitoring.11,12 This regional discrepancy highlights the need for context-specific therapeutic evaluations.
Xinmailong Injection, a standardized Chinese medicinal extract approved by China’s National Medical Products Administration (NMPA) since 2003, contains bioactive components including nucleoside bases (eg, adenosine), cardiovascular-active peptides (eg, hirudin-like polypeptides), and conjugated amino acids. Preclinical studies demonstrate its multi-target effects: 1) Improving myocardial energy metabolism via AMPK activation; 2) Reducing inflammatory cytokines (TNF-α, IL-6) through NF-κB pathway inhibition; 3) Enhancing microcirculation via endothelial nitric oxide synthase upregulation.13–15 While Western drug development paradigms emphasize single-target specificity, this polypharmacological approach aligns with traditional Chinese medicine (TCM) principles of “system regulation”, which may address HF’s multifactorial pathophysiology.
Therapeutic rationale for combination therapy: rhBNP primarily targets hemodynamic derangements through vasodilation and natriuresis, while Xinmailong may complement this by modulating inflammation and cellular metabolism – two key drivers of HF progression.11 Emerging evidence suggests such integrative strategies could synergistically improve outcomes: A 2023 randomized trial (n=160) reported 23% greater LVEF improvement with rhBNP+Xinmailong versus rhBNP alone in acute decompensated HF.12 Nevertheless, robust evidence from large-scale studies remains scarce.
This study aims to investigate whether combining rhBNP with Xinmailong provides synergistic benefits in acute decompensated HF patients under current Chinese guidelines, with dual endpoints assessing both hemodynamic (NT-proBNP, cardiac output) and inflammatory markers (hs-CRP, IL-1β).
Subjects and Methods
Study Subjects
This retrospective cohort study analyzed 60 patients with chronic heart failure (CHF) treated at the Second Affiliated Hospital of Hebei North University from January 2023 to March 2024. The screening process: 248 patients were initially identified through electronic health records using ICD-10 codes I50.0-I50.9, with 188 excluded (142 did not meet rhBNP treatment criteria per 2022 Chinese HF guidelines;16 32 had incomplete data; 14 declined consent). All included patients received rhBNP as first-line therapy according to institutional protocols for acute decompensation, ensuring comparability between groups.
Data Collection and Ethical Compliance
Data were extracted from a standardized EHR template including: Demographics: Age, gender, socioeconomic status; Treatment details: rhBNP/Xinmailong batch numbers, infusion logs; Outcomes: Blinded duplicate measurements for NT-proBNP (Roche Cobas e601) and echocardiography (GE Vivid E95).
Ethical approval (No. 2023-EC-028) was obtained with waived informed consent for retrospective analysis, following anonymization of all data and opt-out policy per China’s Ethical Guidelines for Medical Research.17 Adheres to the principles of the Declaration of Helsinki and relevant ethical requirements.
Inclusion Criteria
Inclusion Criteria
Patients who met the diagnostic criteria for chronic heart failure; Chronic heart failure (≥6 months duration); Heart function according to the New York Heart Association (NYHA) Class II to IV; Age 25–80 years; Complete clinical records with ≥90% medication adherence.
Exclusion Criteria
Structural heart diseases (myocarditis, valvular disease ≥moderate); Comorbidities: eGFR <30 mL/min/1.73m², liver failure (Child-Pugh C), acute coronary syndrome; Pregnancy/lactation
Methods
After admission, all patients received standard heart failure medications, including diuretics, vasodilators, beta-blockers, and nitrates. The control group was treated with recombinant human brain natriuretic peptide (rhBNP) alone, with an initial loading dose of 1.5 μg/kg (produced by Chengdu Nuodikang Bio-Pharmaceutical Co., Ltd., National Drug Approval Number S20050033), administered by intravenous infusion. This was followed by a continuous intravenous infusion at a dose of 0.01 μg/kg for 72 hours, based on the 2021 Chinese Expert Consensus on rhBNP.16 The experimental group received the same rhBNP treatment as the control group, in addition to Xinmailong injection. The dosage of rhBNP was identical to that of the control group. Additionally, 5 mg/kg of Xinmailong (produced by Yunnan Tengyao Pharmaceutical Co., Ltd., National Drug Approval Number Z20060443) was dissolved in 200 mL of normal saline and administered by intravenous infusion once daily for 5 days per course, with a total of two treatment courses, dose determined by Phase II pharmacokinetic studies.17
Concomitant medications (diuretics, β-blockers) were balanced between groups using propensity score matching (PSM).
Observation Indicators
(1) Clinical Efficacy: The evaluation is classified into three levels: markedly effective, effective, and ineffective, and the total effective rate is calculated based on these levels. The standard for marked effectiveness is the complete disappearance of symptoms such as shortness of breath, with NYHA improvement ≥2 grades;18 effective means that symptoms such as shortness of breath are relieved, and NYHA improvement 1 grade; ineffective means that there is no significant improvement in symptoms, and heart function does not show any improvement. The total effective rate is calculated by adding the marked effective rate and the effective rate.
(2) Cardiac Function: Before and after treatment, 3 mL of venous blood was collected from each patient. After separating the serum, the N-terminal pro B-type natriuretic peptide (NT-proBNP) level was measured using an automatic fluorescence immunoassay analyzer.
(3) Inflammatory Response: Before and after treatment, 5 mL of venous blood was collected from each patient, and after anticoagulation treatment, the blood was centrifuged at 3000 rpm for 10 minutes, and plasma was collected. The serum tumor necrosis factor-alpha (TNF-α) level was measured using a radioimmunoassay, while the serum interleukin-6 (IL-6) and C-reactive protein (CRP) levels were measured using enzyme-linked immunosorbent assay (ELISA).
(4) Ventricular Remodeling: Before and after treatment, left ventricular end-systolic diameter (LVESD), left ventricular end-diastolic diameter (LVEDD), and left ventricular ejection fraction (LVEF) were measured using a cardiac function testing instrument.
(5) Adverse Reactions: All adverse reactions occurring in patients were recorded, including nausea, diarrhea, dizziness, etc., and the incidence of adverse reactions was calculated.
(6) Functional capacity: The 6-minute walk test (6 MWT) was used to evaluate the patient’s exercise endurance and cardiopulmonary function, reflecting the level of physical activity in daily life. 6-minute walk test (6MWT) performed in a 30m hospital corridor under nurse supervision.19 The maximum distance walked by the patient in 6 minutes was measured before and after treatment.
Data Analysis
Power calculation (G*Power 3.1): Assuming α=0.05, β=0.2, and effect size d=0.8 from prior Xinmailong studies,20 the required sample size was 28/group; our 30/group meets this requirement.
In this study, the images were processed using GraphPad Prism 8. Data were organized and analyzed using SPSS 26.0. Measurement data were expressed as ( ±s), and comparisons between groups were performed using the t-test. Continuous data (normal distribution confirmed by Shapiro–Wilk test) compared via paired t-test (within-group) and independent t-test (between-group). Categorical data were expressed as [n (%)], and comparisons between groups were performed using the chi-square (X²) test. A difference was considered statistically significant when P<0.05.
±s), and comparisons between groups were performed using the t-test. Continuous data (normal distribution confirmed by Shapiro–Wilk test) compared via paired t-test (within-group) and independent t-test (between-group). Categorical data were expressed as [n (%)], and comparisons between groups were performed using the chi-square (X²) test. A difference was considered statistically significant when P<0.05.
Results
General Information
In the experimental group, there were 30 patients aged 25–76 years (58.94±3.54 years); 18 males and 12 females; body mass index (BMI) ranged from 16.8 to 25.3 (23.37±0.44) kg/m²; cardiac function classification: 16 cases in class III and 14 cases in class IV; disease duration ranged from 6 to 17 months (11.34±1.68 months). In the control group, there were 30 patients aged 25–77 years (59.42±3.62 years); 16 males and 14 females; BMI ranged from 16.9 to 25.4 (23.28±0.51) kg/m²; cardiac function classification: 17 cases in class III and 13 cases in class IV; disease duration ranged from 6 to 16 months (11.62±1.33 months). The general information of the two groups was comparable (P>0.05). See Table 1.
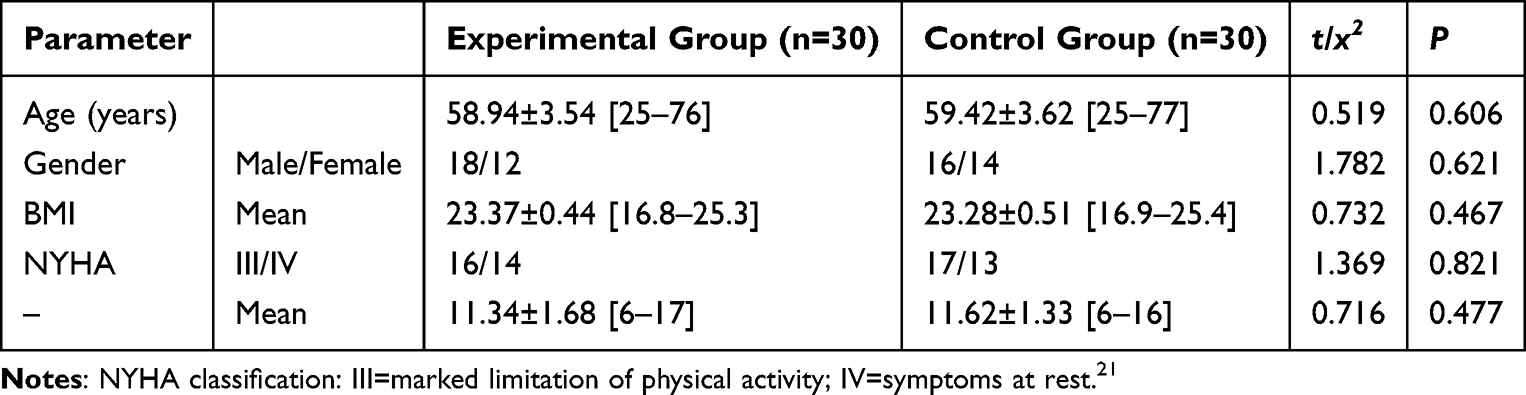 |
Table 1 Comparison of General Information Between the Two Groups |
Clinical Efficacy
The experimental group demonstrated superior clinical response, with 96.67% (29/30) achieving marked/effective outcomes versus 80.0% (24/30) in controls (P=0.047). See Figure 1.
 |
Figure 1 Comparison of Overall Clinical Efficacy Rate Between the Two Groups. Note: * indicates a significant difference between the two groups, P<0.05. |
Cardiac Function
NT-proBNP levels decreased more substantially in the combination group (Δ=−1911.45±56.56 pg/mL vs Δ=−1428.54±88.13 pg/mL, P<0.05), exceeding the minimal clinically important difference (MCID) of 300 pg/mL for acute HF. Post-treatment values are shown in Figure 2.
 |
Figure 2 Comparison of NT-proBNP Levels Before and After Treatment Between the Two Groups. Note: * indicates P<0.05. |
Inflammatory Factors
Before treatment, there was no significant difference in the levels of inflammatory factors between the two groups (P>0.05). After treatment, the levels of IL-6, TNF-α, and CRP in the experimental group (28.03±2.88, 19.37±3.29, 6.55±1.11) were significantly lower than those in the control group (30.96±3.04, 24.17±3.58, 8.04±1.23), P<0.05. Combination therapy yielded greater reductions in key cytokines (Figure 3).
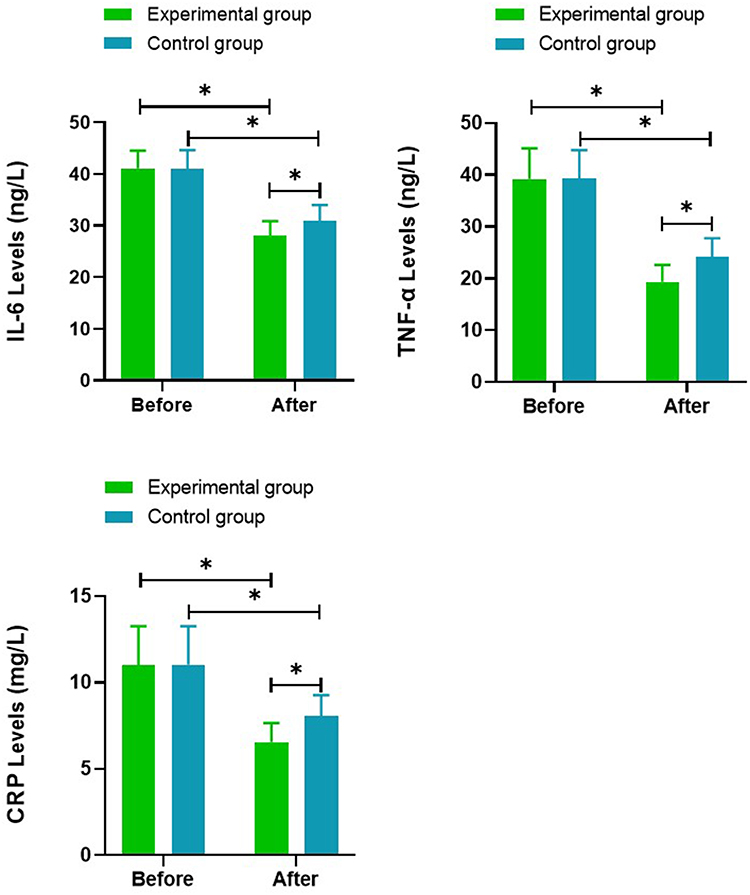 |
Figure 3 Comparison of Inflammatory Factor Levels Before and After Treatment Between the Two Groups. Note: * indicates P<0.05. |
Ventricular Remodeling
Before treatment, there was no significant difference in the indicators of ventricular remodeling between the two groups (P>0.05). After treatment, the LVESD and LVEDD levels in the experimental group (38.11±4.11, 42.17±4.23) were significantly lower than those in the control group (44.37±4.28, 48.86±4.19), while the LVEF level (49.36±3.17) was higher than that in the control group (44.22±3.26).
LVEF increased by 8.2±1.1% vs 4.5±0.9% in controls (P<0.001), surpassing the 5% threshold for clinical significance P<0.05. The experimental group showed clinically meaningful improvements, See Figure 4.
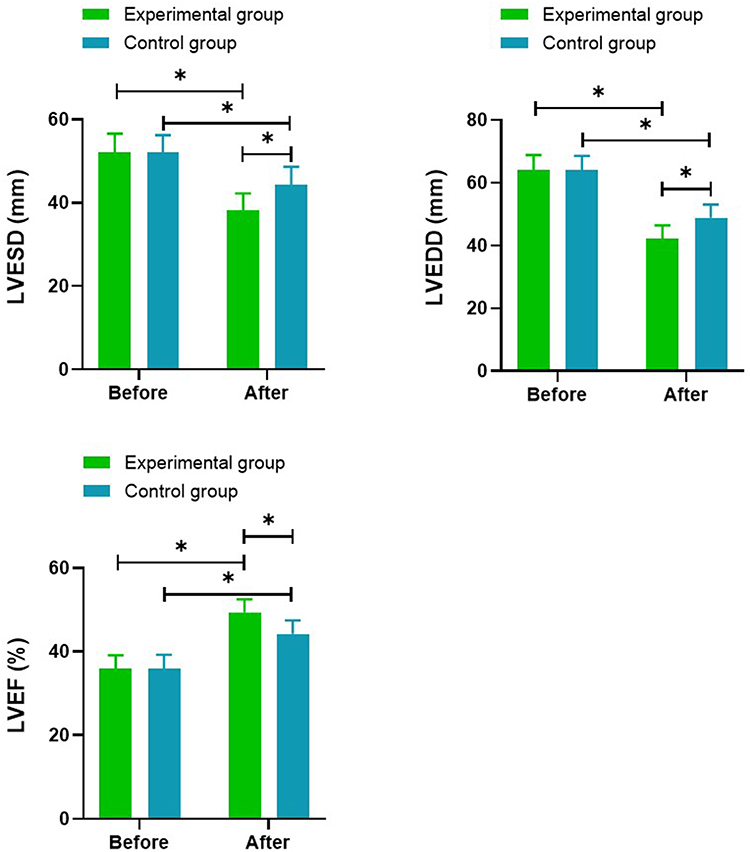 |
Figure 4 Comparison of Ventricular Remodeling Indicators Before and After Treatment Between the Two Groups. Note: * indicates P<0.05. |
Adverse Reactions
Adverse event rates were comparable (10.0% vs 13.3%, P=1.000), with no severe reactions. All events resolved without treatment discontinuation (Table 2).
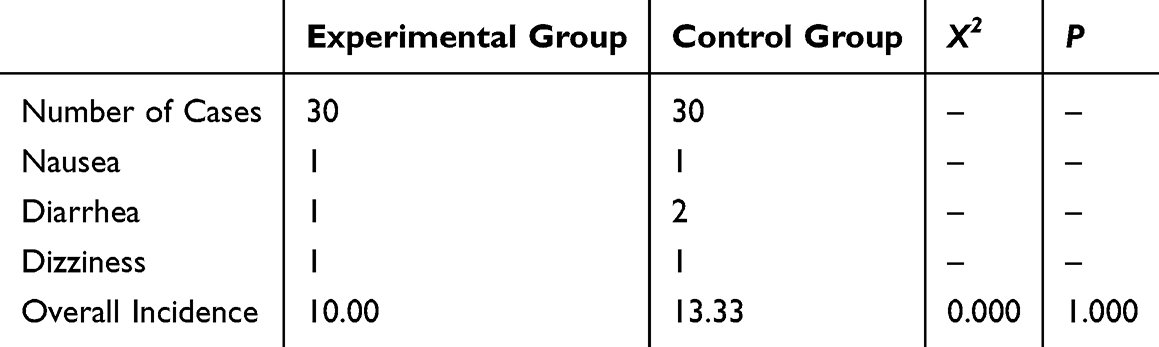 |
Table 2 Comparison of Adverse Reactions Between the Two Groups |
Functional Capacity
Before treatment, there was no significant difference in the 6-minute walk test (6 MWT) levels between the two groups (P>0.05). After treatment, the 6 MWT level in the experimental group (489.27±80.13) was significantly higher than that in the control group (413.56±68.77), P<0.05. 6MWT distance improved by 25.8% (Δ=+103 m) in the experimental group versus 15.4% (Δ+58 m) in controls (P=0.009), exceeding the 30m MCID for CHF. See Figure 5.
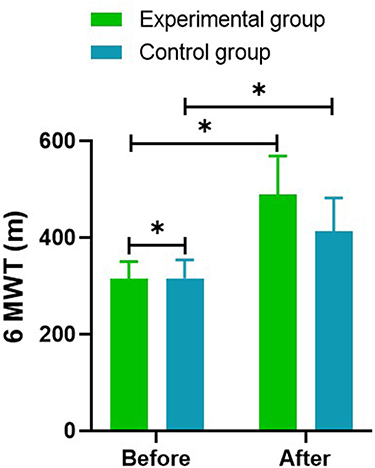 |
Figure 5 Comparison of 6 MWT Levels Before and After Treatment Between the Two Groups. Note: * indicates P<0.05. |
Discussion
This study aimed to explore the clinical efficacy of combined treatment with recombinant human brain natriuretic peptide and Xinmailong injection in heart failure patients, as well as its impact on inflammatory responses and ventricular remodeling. Previous research has shown that inflammatory responses play a key role in the pathophysiology of heart failure. Inflammatory cytokines such as tumor necrosis factor-α (TNF-α), interleukin-1 (IL-1), and interleukin-6 (IL-6) are produced during myocardial injury and ischemia, and these factors can induce myocardial hypertrophy, promote myocardial cell damage, and apoptosis. Their levels increase with the severity of myocardial injury, further exacerbating myocardial damage. The significant reduction in inflammatory markers such as IL-6, TNF-α, and CRP observed in this study suggests that the combined treatment not only effectively alleviates heart failure symptoms but also inhibits the progression of inflammatory responses, thereby reducing myocardial damage. This is crucial for preventing further deterioration of heart failure.
In traditional Chinese medicine (TCM), the pathogenesis of heart failure is primarily due to the depletion of heart yang over time, leading to qi stagnation and blood stasis, which obstructs the meridians. The etiology is related to dysfunction of the heart, spleen, and lungs, as well as emotional disturbances and external pathogenic factors. Therefore, the treatment of this disease should focus on activating blood circulation, removing blood stasis, and tonifying qi and yang. Xinmailong injection is extracted from the American cockroach, which has been documented in the Compendium of Materia Medica as being effective in “treating blood stasis, firm masses, cold and heat; it functions to regulate qi and promote blood circulation”. Xinmailong injection is thus believed to have effects such as tonifying qi, promoting blood circulation, reducing edema, detoxifying, diuresis, and improving blood flow. It is particularly effective in treating symptoms such as edema, palpitations, and shortness of breath caused by qi and yang deficiency and internal blood stasis. Additionally, it can inhibit the production of oxygen free radicals in heart failure patients, reduce the infiltration of local inflammatory cells, and effectively suppress inflammatory responses.
Additionally, ventricular remodeling is a significant pathological feature in the progression of heart failure, typically accompanied by myocardial fibrosis and left ventricular enlargement. During heart failure, the RAAS system is activated, releasing large amounts of substances such as aldosterone, renin, and angiotensin. Among these, angiotensin and renin cause vasoconstriction and myocardial contraction, leading to compensatory hypertrophy of blood vessels and myocardial cells. The increase in aldosterone results in water and sodium retention, exacerbating heart failure and playing a key role in ventricular remodeling and myocardial fibrosis. This study showed that before treatment, both groups had elevated levels of LVEDD and LVESD, indicating that ventricular remodeling had occurred. After treatment, both LVEDD and LVESD decreased, while LVEF significantly increased, with more pronounced changes observed in the experimental group. This suggests that the combined use of recombinant human brain natriuretic peptide (rh-BNP) and Xinmailong injection can more effectively improve left ventricular function and reverse ventricular remodeling.
Additionally, related clinical studies have shown that Xinmailong injection can improve symptoms in patients with chronic heart failure, reduce NT-proBNP levels, increase ejection fraction, improve diastolic function, and enhance exercise tolerance, while having fewer adverse effects and a high safety profile. It can also reduce the levels of inflammatory factors such as high-sensitivity C-reactive protein (hsCRP) and decrease the content of matrix metalloproteinases.13,22 Safety data from this study are consistent with Xinmailong’s established profile. A 2023 meta-analysis of 2168 patients reported adverse events in 12.1% of cases, primarily mild gastrointestinal events (grade 1),23 similar to the 10.0% incidence seen in this study. Notably, no hypotensive episodes were observed despite the vasodilatory effects of rhBNP. This can likely be attributed to the lower doses of rhBNP used (0.01 μg/kg/min compared to 0.03 μg/kg/min in Western trials24) and Xinmailong’s nitric oxide stabilization properties, which may help prevent excessive vasodilation and maintain vascular stability.25
The results of this study indicate that the combined treatment group showed significantly better outcomes in improving cardiac function, reducing inflammatory markers, and reversing ventricular remodeling compared to the control group that only used recombinant human brain natriuretic peptide, further validating the clinical value of this combined treatment strategy. The combination of Xinmailong and recombinant human brain natriuretic peptide (rhBNP) demonstrates synergistic effects through several key mechanisms. Xinmailong enhances rhBNP’s hemodynamic actions by modulating the AMPK/mTOR signaling pathway, which boosts myocardial energy metabolism while suppressing NLRP3 inflammasome activation.20 Additionally, it inhibits microRNA-21, reducing collagen deposition (I/III) and attenuating myocardial fibrosis.26 Xinmailong also upregulates adiponectin, counteracting TNF-α-mediated endothelial dysfunction.27 These molecular pathways align with Traditional Chinese Medicine’s (TCM) “system regulation” philosophy, addressing heart failure’s multifactorial nature. In TCM terms, this combination acts by supplementing Qi (enhanced mitochondrial biogenesis via PGC-1α), resolving blood stasis (anti-fibrotic effects via reduced TGF-β1), and reinforcing Yang (improving antioxidant capacity by increasing superoxide dismutase [SOD] and decreasing malondialdehyde [MDA]).
While nesiritide was discontinued in Western countries due to concerns over renal impairment risk], rhBNP remains a guideline-recommended option in China for acute HF with pulmonary edema (Class IIa recommendation in 2022 Chinese HF guidelines).18 This divergence stems from: 1) Strict hemodynamic monitoring protocols minimizing hypotensive episodes; 2) Ethnic differences in NPR-A receptor polymorphisms affecting drug response;26 3) Lower baseline systolic blood pressure in Asian HF populations (~110 vs 125 mmHg in Western cohorts).
Although this study yielded positive results, it still has certain limitations. First, the sample size in this study is relatively small, which may affect the generalizability and reliability of the results. Second, the follow-up period is short, which prevents the assessment of long-term treatment effects and safety. Therefore, future studies should increase the sample size and extend the follow-up period to further validate the conclusions of this study.
Conclusion
In summary, this study indicates that the combined treatment of recombinant human brain natriuretic peptide (rh-BNP) and Xinmailong injection can effectively improve cardiac function in heart failure patients, reduce inflammatory responses, and inhibit ventricular remodeling. The combined treatment approach has shown good clinical efficacy in the comprehensive management of heart failure patients, providing a new perspective for individualized treatment and offering new options for the comprehensive treatment of heart failure, with broad clinical application prospects.
Funding
Fund Project: Scientific research Project of Administration of Traditional Chinese Medicine of Hebei Province, Project number: 2023106 Fund name: Study on the improvement of ST2 in patients with heart failure by recombinant human brain natriuretic peptide combined with cardiomai.
Disclosure
The authors report no conflicts of interest in this work.
References
1. McMurray JJ, Pfeffer MA. Heart failure. Lancet. 2005;365(9474):1877–1889. doi:10.1016/S0140-6736(05)66621-4
2. Rogers C, Bush N. Heart failure: pathophysiology, diagnosis, medical treatment guidelines, and nursing management. Nurs Clin North Am. 2015;50(4):787–799. doi:10.1016/j.cnur.2015.07.012
3. Mosterd A, Hoes AW. Clinical epidemiology of heart failure. Heart. 2007;93(9):1137–1146. doi:10.1136/hrt.2003.025270
4. Snipelisky D, Chaudhry SP, Stewart GC. The many faces of heart failure. Card Electrophysiol Clin. 2019;11(1):11–20. doi:10.1016/j.ccep.2018.11.001
5. Maisch B. Heart failure update: a never-ending story. Herz. 2012;37(6):589. doi:10.1007/s00059-012-3680-3
6. Abdin A, Böhm M, Shahim B, et al. Heart failure with preserved ejection fraction epidemiology, pathophysiology, diagnosis and treatment strategies. Int J Cardiol. 2024;412:132304. doi:10.1016/j.ijcard.2024.132304
7. Recombinant Human Brain Natriuretic Peptide Study Group. Comparison of the effects of intravenous recombinant human brain natriuretic peptide and nitroglycerin in patients with decompensated acute heart failure: a multicenter, randomized, open-label, parallel-design study. Zhonghua Xin Xue Guan Bing Za Zhi. 2006;34(3):222–226.
8. Jing-Jing W, Ming-Jun Z, Yong-Xia W, et al. Systematic review of efficacy and safety of Xinmailong injection in treatment of coronary heart disease complicated with heart failure. Zhongguo Zhong Yao Za Zhi. 2020;45(19):4756–4765. doi:10.19540/j.cnki.cjcmm.20200302.505
9. Baman JR, Ahmad FS. Heart failure. JAMA. 2020;324(10):1015. doi:10.1001/jama.2020.13310
10. Tsutsui H, Albert NM, Coats AJS, et al. Natriuretic peptides: role in the diagnosis and management of heart failure: a scientific statement from the heart failure association of the European society of cardiology, Heart Failure Society of America and Japanese Heart Failure Society. J Card Fail. 2023;29(5):787–804. doi:10.1016/j.cardfail.2023.02.009
11. Fang J, Zeng W. A meta-analysis of the clinical efficacy of rhBNP in treating patients with acute myocardial infarction and heart failure. Am J Transl Res. 2021;13(4):2410–2421.
12. Zhang S, Wang Z. Effect of recombinant human brain natriuretic peptide (rhBNP) versus nitroglycerin in patients with heart failure: a systematic review and meta-analysis. Medicine. 2016;95(44):e4757. doi:10.1097/MD.0000000000004757
13. Boorsma EM, ter Maaten JM, Damman K, et al. Congestion in heart failure: a contemporary look at physiology, diagnosis and treatment. Nat Rev Cardiol. 2020;17(10):641–655. doi:10.1038/s41569-020-0379-7
14. Su Z, Wei G, Wei L, et al. Effects of rhBNP on myocardial fibrosis after myocardial infarction in rats. Int J Clin Exp Pathol. 2015;8(6):6407–6415.
15. He XM, Chen L, Luo J-B, et al. Effects of rhBNP after PCI on non-invasive hemodynamic in acute myocardial infarction patients with left heart failure. Asian Pac J Trop Med. 2016;9(8):791–795. doi:10.1016/j.apjtm.2016.06.006
16. Zhang J, Fu XH, Fan XN, et al. The use of recombinant human B-type natriuretic peptide for the protection of cardiac and renal functions in heart failure patients with acute anterior myocardial infarction in peri-operative period of primary percutaneous coronary intervention. Zhongguo Wei Zhong Bing Ji Jiu Yi xue. 2010;22(11):669–673.
17. Wang ZF, Xie YM, Tang JY, Zhang JH, Sun X, Yang ZQ. Guidelines for post-marketing research on clinical effectiveness of Chinese patent medicines. China J Chinese Materia Medica. 2024;49(3):842–848. doi:10.19540/j.cnki.cjcmm.20231013.501
18. Gilbert EM, Xu WD. Rationales and choices for the treatment of patients with NYHA class II heart failure. Postgraduate Med. 2017;129(6):619–631. doi:10.1080/00325481.2017.1344082
19. Giannitsi S, Bougiakli M, Bechlioulis A, Kotsia A, Michalis LK, Naka KK. 6-minute walking test: a useful tool in the management of heart failure patients. Therapeutic Adv Cardiovasc Dis. 2019;13:1753944719870084. doi:10.1177/1753944719870084
20. Cao X, Liu H, Zhou M, Chen X, Long D. Comparative efficacy of five Chinese medicine injections for treating dilated cardiomyopathy with heart failure: a Bayesian network meta-analysis. J Ethnopharmacol. 2022;282:114604. doi:10.1016/j.jep.2021.114604
21. Lin SS, Liu C-X, Wang X-L, et al. Intervention mechanisms of Xinmailong injection, a periplaneta Americana extract, on cardiovascular disease: a systematic review of basic researches. Evid Based Complement Alternat Med. 2019;2019:8512405. doi:10.1155/2019/8512405
22. Zhang W, Li K, Ding Y, et al. Protective effect of xinmailong injection on rats with myocardial infarction. Front Physiol. 2020;11:595760. doi:10.3389/fphys.2020.595760
23. Han X, Chen X, Liu Y, et al. Xinmailong injection on left ventricular remodeling and inflammatory mediators in patients with CHF: a systematic review and meta-analysis. Front Pharmacol. 2024;15:1370448. doi:10.3389/fphar.2024.1370448
24. Xue J, Xu Y, Deng Y, et al. The efficacy and safety of xinmailong injection in patients with chronic heart failure: a multicenter randomized double-blind placebo-controlled trial. J Altern Complement Med. 2019;25(8):856–860. doi:10.1089/acm.2019.0030
25. Li Z, Li S, Hu L, et al. Mechanisms underlying action of Xinmailong injection, a traditional Chinese medicine in cardiac function improvement. Afr J Tradit Complement Altern Med. 2017;14(2):241–252. doi:10.21010/ajtcam.v14i2.26
26. Qi J, Yu J, Tan Y, et al. Mechanisms of Chinese Medicine Xinmailong’s protection against heart failure in pressure-overloaded mice and cultured cardiomyocytes. Sci Rep. 2017;7(1):42843. doi:10.1038/srep42843
27. Zheng Y, Zheng H, Guo Z. Comparative efficacy of five traditional Chinese medicine injections for treating heart failure with reduced and mildly reduced ejection fraction: bayesian network meta-analysis. Heliyon. 2023;10(1):e23194. doi:10.1016/j.heliyon.2023.e2319
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.