Back to Archived Journals » Robotic Surgery: Research and Reviews » Volume 4
The effect of obesity on clinical and economic outcomes in robotic endometrial cancer surgery
Authors Ind TEJ, Marshall C, Hacking M, Chiu S, Harris M, Nobbenhuis M
Received 24 September 2016
Accepted for publication 25 December 2016
Published 27 March 2017 Volume 2017:4 Pages 33—37
DOI https://doi.org/10.2147/RSRR.S123108
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Masoud Azodi
Thomas E J Ind,1,2 Chris Marshall,3 Matthew Hacking,4 Selina Chiu,1 Michelle Harris,1 Marielle Nobbenhuis1
1Department of Gynaecological Oncology, Royal Marsden Hospital, 2Department of Obstetrics and Gynaecology, St. George’s University of London, 3Department of Finance, Royal Marsden Hospital, 4Department of Anaesthesia, Royal Marsden Hospital, London, UK
Abstract: The aim of this study was to compare the financial and clinical outcomes in robotic-assisted laparoscopic surgery for primary endometrial cancer between obese and nonobese women. The hospital finance department assessed the total admission costs for robotic surgery for endometrial cancer in 54 women. This included a subanalysis for costs over nine areas (ward and clinics, drugs and pharmacy, medical staff, theaters, blood products, imaging, pathology, rehabilitation therapy, and high dependency costs). Furthermore, a prospective collection of morbidity and surgical outcome data was performed. The study group included 21 nonobese and 33 obese women (body mass index >30). Obese women were more likely to stay for more than one night in hospital (20/33 [60.6%] compared to 4/21 [19.0%], P=0.032) and to have high dependency care (25/33 [75.8%] compared to 10/21 [47.6%], P=0.032). Theater time was on average 35 min longer (95% confidence interval [CI] 5–65 min, P=0.0252). Both the groups were comparable for comorbidities except for the presence of diabetes being present in the obese group (13/33 [39.4%] compared to 0/21 [0.0%], P=0.007). There were six Clavien-Dindo grade II complications in the obese group and two in the nonobese group. The average overall costs were £1,852 greater (95% CI £431–£3,277, P=0.012) in the obese group. Diabetes and hypertension were associated with increased costs, but obesity was the only independent variable. In conclusion, greater resource should be allocated to obese women undergoing primary surgery for endometrial cancer.
Keywords: obesity, cost, endometrial cancer, uterine cancer, metabolic syndrome, diabetes
Introduction
From 1993 to 2011, the age-standardized incidence rate for endometrial cancer in the UK rose from 13.5 to 20.4 in 100,000.1 This is probably due to an increase in obesity which has increased in women from 14% to 25% in the same time interval. Obesity is associated with the peripheral conversion of androstenedione to estrone which is an etiological factor.2 The increase in numbers is likely to be associated with a differing morbidity profile. Minimally invasive surgery in these women has already resulted in shorter length of stay and less complications.3 Recent studies have shown the benefit of introducing a robotic service in primary surgery for endometrial cancer, showing less conversions to laparotomy and a reduction in the number of laparotomies performed.4,5 Obesity is one of the comorbidities related to an increase in operating time, complications, and length of stay. This study investigated the different outcomes and costs in relation to body mass index (BMI) in a group of endometrial cancer patients who underwent a robotic-assisted laparoscopic hysterectomy.
Methods
The project had ethical approval as a service evaluation project from the Royal Marsden Committee on Clinical Research (SE314). All patients went through an informed consent process and signed consent forms. All women with endometrial cancer having robotic surgery from September 2012 to December 2014 were included in the analysis. Clinical data were collected from a prospectively entered database and cross-reference against the hospital’s electronic patient record (EPR) that included clinical and operative notes. The EPR system also contained a preoperative anesthetic assessment that included a thorough systematic clinical history, microbiological records, blood transfusion records, histopathology, cytopathology, hematology, and biochemistry results. All clinical documentation of the patients was reviewed for Clavien-Dindo6 grade II complications and above for 30 days following surgery.
Costs were assessed by the hospital’s finance department. These were allocated into one of nine categories, including costs for ward, high dependence care, medical staffing, theaters, drugs and pharmacy, blood products, imaging, pathology, and rehabilitation therapy. The exact allocation of different costs into each of these categories is described previously.4 These were allocated into one of nine categories, including costs for wards, high-dependence care, medical staffing, theaters, drugs and pharmacy, blood products, imaging, pathology, and rehabilitation therapy. Outcomes from 24 of the patients unstratified by BMI have been reported in another paper on a different subject.4
All operations included a hysterectomy and removal of the Fallopian tubes and ovaries. It is policy to perform a limited pelvic lymphadenectomy in patients with more than grade 1 or stage 1a disease although it is often not performed on an individual basis in patients who are elderly or who have excess comorbidity. It is not common practice in the institution nor in the United Kingdom to perform para-aortic lymphadenectomy routinely for women with endometrial cancer. Robotic cases were performed using the da Vinci-S® system (Intuitive Surgery, Sunnyvale, USA) with two rather than three 8 mm operating arms, a 12 mm umbilical port for the camera, and a 5 mm portside assistant port. Lymph nodes and other specimens were retrieved through the vagina. Lymph nodes were normally placed in a bag prior to retrieval.
The Shapiro–Wilks test for normality was applied to the total inpatient costs, and no significant difference from a normal distribution was demonstrated. Therefore, descriptive series was presented as mean values with standard deviations and the student’s t-test was used to test for differences in continuous data. Dichotomous data were compared by using Fisher’s exact test. Simple linear regression was used to compare individual comorbidity factors such as diabetes and hypertension after applying the numbers 1 or 0 for their presence or absence, respectively. Obesity was defined as a woman having a BMI ≥30 kg/m2. Factors that significantly correlated with total costs were assessed in a backward stepwise multiple linear regression to account for cofounding factors. The project had ethical approval as a service evaluation project from the Royal Marsden Committee on Clinical Research (SE314).
Results
A total of 54 women were included in the evaluation (33 obese and 21 nonobese). The differences between the two groups in stage and histology are shown in Table 1. There were no demonstrable differences in the proportion of cases with high stage, poor prognostic pathology, high grade, or the presence of lymph-vascular space invasion. The mean age was 66 years (standard deviation [SD] 11 years). No differences in age were seen between the two groups (Table 2).
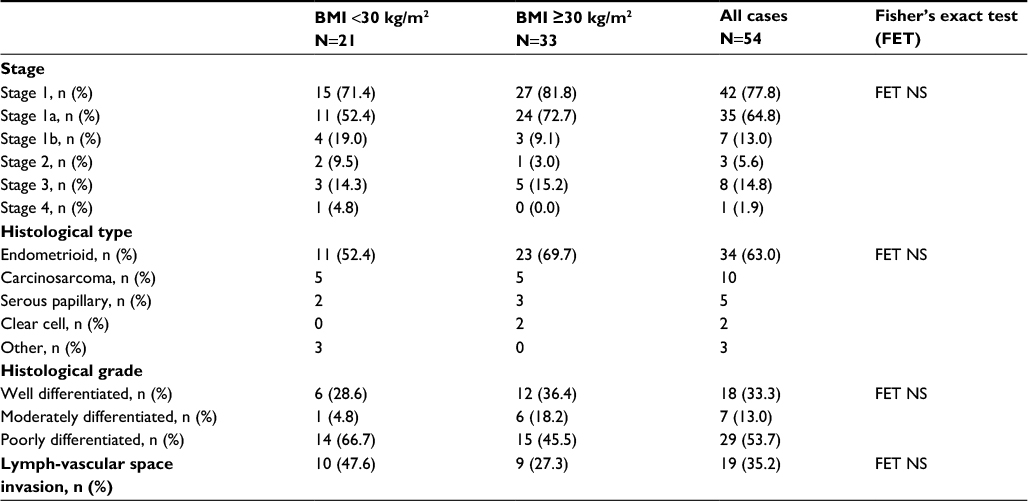 | Table 1 Stage and histology of endometrial cancer in women with body mass index (BMI) ≥30 kg/m2 compared to women with BMI <30 kg/m2 Abbreviation: NS, not significant. |
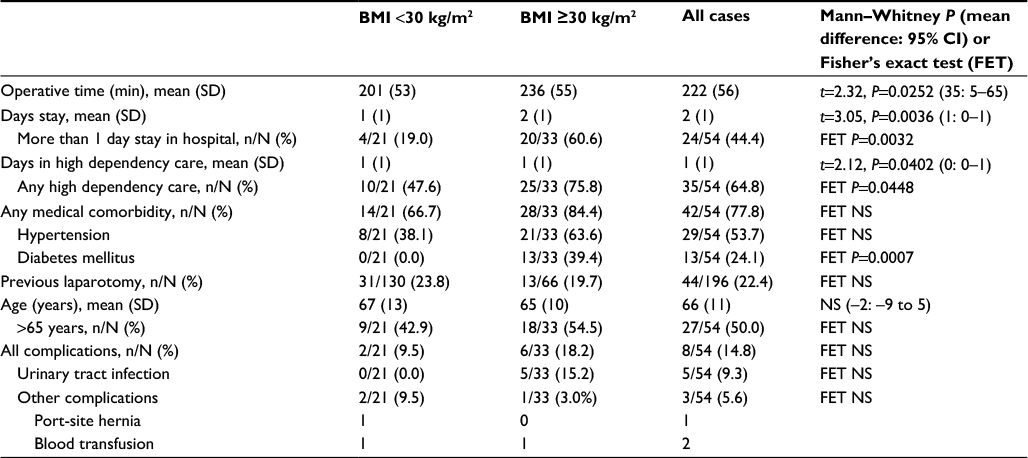 | Table 2 Clinical outcomes and comorbidities for robotic primary surgery in endometrial cancer in women with BMI ≥30 kg/m2 compared to women with BMI <30 kg/m2 Abbreviations: BMI, body mass index; CI, confidence interval; NS, not significant; SD, standard deviation. |
The mean operating time was 35 min longer in the obese group (95% CI 5–65 min, t=2.32, P=0.0252) (Table 2). Furthermore, obese patients spent an average of 1 day extra in hospital (95% CI 0–1, t=3.05, P=0.0036) (Table 2). More obese patients required postoperative stay in a high dependency unit compared to women who were not obese (P=0.0448) (Table 2). There were no differences between the two groups in the proportion of women who were hypertensive or had other comorbidities (cardiac, neurological, respiratory, or endocrinological) with the exception of diabetes which was more common in the obese group (Table 2). There were six Clavien-Dindo grade II complications in the obese group (five urinary infections and one blood transfusion) compared to two in the nonobese group (one blood transfusion and one port-site hernia). This difference was not significant (Table 2).
The cost of surgery was on average £1,854 more (95% CI £431–£3,277, t=2.61, P=0.012) in the obese group (Table 3). There were significantly higher costs for wards and clinics (£480 more, 95% CI 68–893, t=2.34, P=0.0234) and for drugs and pharmacy costs (£34 more, 95% CI 1–67, t=2.08, P=0.0426) in the obese group (Table 3). There were no demonstrable differences between the two groups in costs for medical staffing, theaters, blood products, imaging, pathology, rehabilitation, and high dependency care.
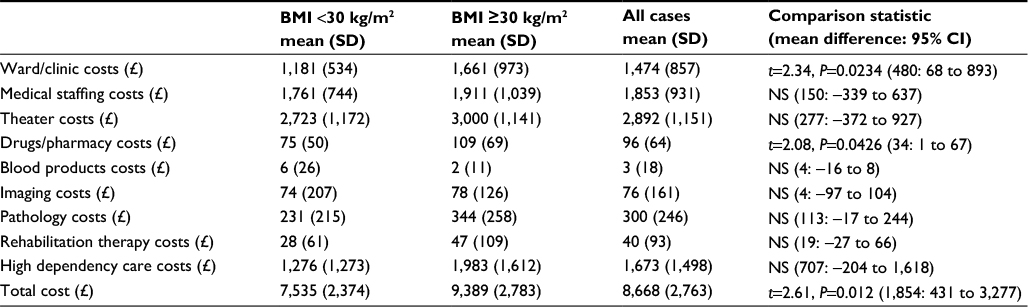 | Table 3 Cost of robotic primary surgery for endometrial cancer in women with BMI ≥30 kg/m2 compared to women with BMI <30 kg/m2 Abbreviations: BMI, body mass index; CI, confidence interval; NS, not significant; SD, standard deviation. |
Simple linear regression demonstrated a significant relationship between the total inpatient cost and obesity (r=0.33, t=2.52, P=0.0148), hypertension (r=0.32, t=2.41, P=0.0196), and diabetes (r=0.36, t=2.80, P=0.00071). There was no significant correlation between total inpatient cost and age of over 65 years or a previous laparotomy. Backward stepwise multiple regression revealed obesity alone as an independent variable associated with total cost (Table 4).
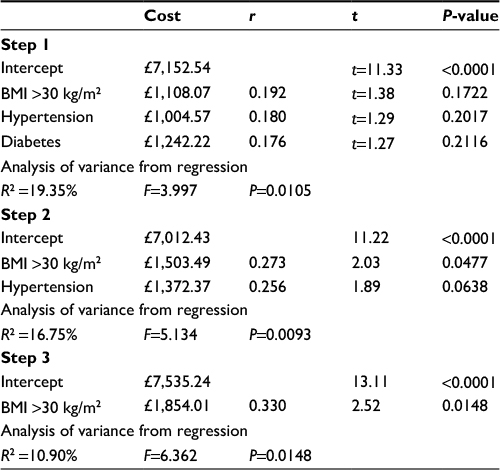 | Table 4 Backward stepwise multiple linear regression to assess correlation between hypertension, obesity, and diabetes with the total cost of inpatient stay Abbreviation: BMI, body mass index. |
Discussion
These data demonstrate that women with endometrial cancer who have a BMI >30kg/m2 incur significantly more costs for their inpatient surgical treatment compared to women with a lower BMI. Differences were demonstrated in ward, clinic, and drug costs. Although no savings were shown in theater costs and high dependency care expenses, patients were shown to spend longer in hospital and high dependency care if they had a BMI >30 kg/m2. As there was no comparable data to use for a power analysis, it may be that more significant differences in the subanalyses would have been found if higher numbers were recruited. If larger numbers were included, we might have differences in other outcomes. In addition, this study demonstrated that obesity was the only independent variable, but it would have been interesting to see if diabetes and hypertension showed additional effect in a multi-variant analysis if there was a larger series. The findings are significant in terms of overall inpatient costs for obese women and demonstrate the need for an increased resources for this group of women.
This study chose robotically assisted laparoscopic endometrial cancer surgery for the analysis over straight stick laparoscopic surgery or open laparotomy. There is clear evidence from both individual randomized controlled studies and a respected meta-analysis3 that some form of laparoscopic approach is associated with less complications and a similar survival. Therefore, laparotomy is no longer the preferred route for endometrial cancer in women who are not contraindicated to have some form of laparoscopic approach. We have looked at robotically assisted surgery as our own data have shown that it has comparable outcomes to straight stick surgery with some financial benefits to the institution by minimizing the proportion of cases having open surgery.4 Other authors have also reported clinical benefits for robotic-assisted laparoscopic surgery for primary endometrial cancer.7–10 Some authors have reported equal or improved costs for robotic-assisted laparoscopy,5,11 whereas other studies have shown increased costs when compared to straight stick laparoscopy not taking into account the proportion of cases performed open.12–15
These data assessed the specific costs of the surgical episode alone and did not look at societal costs such as time off work nor quality of life. These have been reported in other studies16,17 and as a separate comparison. Furthermore, there are additional costs for adjuvant therapy such as radiotherapy and chemotherapy. It is possible that there would be further differences if the other additional treatment costs were assessed. The type of surgery in endometrial cancer is also controversial with some institutions electing to perform full pelvic and para-aortic lymphadenectomies and others believing in hysterectomy alone.18 It is possible that differences between obese and nonobese women would be different and probably greater in an institution with an ethos for more radical surgery than ours and less in an institution that believes in hysterectomy alone.
Conclusion
This study demonstrates that the cost of robotic surgery for endometrial cancer is significantly higher if a patient has a BMI ≥30 kg/m2. This is probably related to increased hospital stay, longer time in theater, and more high dependency care usage. Greater resource should be allocated to obese women with endometrial cancer compared to nonobese women.
Disclosure
In 2007, TI received 2 days of practical training in robotic surgery. This included premium economy class travel to the USA and accommodation costs paid for, and organized by, Intuitive Surgical Inc. (CA, USA). Intuitive Surgical also sponsored a day’s preceptorship for MN and TI at the Royal Marsden Hospital in 2013. In May 2014, both MN and TI received a day of training in Essen, Germany (including travel and accommodation) sponsored by Intuitive Surgical. In February 2016, both MN and TI received a day of training in Lund, Sweden (including travel and accommodation) sponsored by Intuitive Surgical. MN is a proctor for Intuitive Surgical. The authors report no other conflicts of interest in this work.
References
UK CR. Uterine cancer incidence statistics 2014. Available from: http://www.cancerresearchuk.org/cancer-info/cancerstats/types/uterus/incidence/uk-uterus-cancer-incidence-statistics. Accessed January 12, 2017. | ||
Benedetto C, Salvagno F, Canuto EM, Gennarelli G. Obesity and female malignancies. Best Pract Res Clin Obstet Gynaecol. 2015;29:528–540. | ||
Galaal K, Bryant A, Fisher AD, Al-Khaduri M, Kew F, Lopes AD. Laparoscopy versus laparotomy for the management of early stage endometrial cancer. Cochrane Database Syst Rev. 2012;(9):CD006655. | ||
Ind TE, Marshal C, Hacking M, et al. Introducing robotic surgery into an endometrial cancer service – a prospective evaluation of clinical and economic outcomes in a UK institution. Int J Med Robot. 2016;12:137–144. | ||
Lau S, Vaknin Z, Ramana-Kumar AV, Halliday D, Franco EL, Gotlieb WH. Outcomes and cost comparisons after introducing a robotics program for endometrial cancer surgery. Obstet Gynecol. 2012;119:717–724. | ||
Dindo C, Clavien PA. What is a surgical complication? World J Surg. 2008;32:939–941. | ||
Boggess JFG, Gehring PA, Cantrell L, et al. A comparative study of 3 surgical methods for hysterectomy with staging for endometrial cancer: robotic assistance, laparoscopy, laparotomy. Am J Obstet Gynecol. 2008;199:360. | ||
Coronado PJ, Herraiz MA, Magrina JF, Fasero M, Vidart JA. Comparison of perioperative outcomes and cost of robotic-assisted laparoscopy, laparoscopy and laparotomy for endometrial cancer. Eur J Obstet Gynecol Reprod Biol. 2012;165:289–294. | ||
Gaia G, Holloway RW, Santoro L, Ahmad S, Di Silverio E, Spinillo A. Robotic-assisted hysterectomy for endometrial cancer compared with traditional laparoscopic and laparotomy approaches: a systematic review. Obstet Gynecol. 2010;116:1422–1431. | ||
Seamon LG, Cohn DE, Henretta MS, et al. Minimally invasive comprehensive surgical staging for endometrial cancer: robotics or laparoscopy? Gynecol Oncol. 2009;113:36–41. | ||
Leitao MM Jr, Bartashnik A, Wagner I, et al. Cost-effectiveness analysis of robotically assisted laparoscopy for newly diagnosed uterine cancers. Obstet Gynecol. 2014;123:1031–1037. | ||
Lonnerfors C, Reynisson P, Persson J. A randomized trial comparing vaginal and laparoscopic hysterectomy vs robot-assisted hysterectomy. J Minim Invasive Gynecol. 2015;22:78–86. | ||
Wright JD, Ananth CV, Tergas AI, et al. An economic analysis of robotically assisted hysterectomy. Obstet Gynecol. 2014;123:1038–1048. | ||
Wright JD, Burke WM, Wilde ET, et al. Comparative effectiveness of robotic versus laparoscopic hysterectomy for endometrial cancer. J Clin Oncol. 2012;30:783–791. | ||
Yu X, Lum D, Kiet TK, et al. Utilization of and charges for robotic versus laparoscopic versus open surgery for endometrial cancer. J Surg Oncol. 2013;107(6):653–658. | ||
Bell MC, Torgerson J, Seshadri-Kreaden U, Suttle AW, Hunt S. Comparison of outcomes and cost for endometrial cancer staging via traditional laparotomy, standard laparoscopy and robotic techniques. Gynecol Oncol. 2008;111:407–411. | ||
Barnett JC, Judd JP, Wu JM, Scales CD Jr, Myers ER, Havrilesky LJ. Cost comparison among robotic, laparoscopic, and open hysterectomy for endometrial cancer. Obstet Gynecol. 2010;116:685–693. | ||
Hernandez E. ACOG Practice Bulletin number 65: management of endometrial cancer. Obstet Gynecol. 2006;107:952. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.