Back to Journals » International Journal of Women's Health » Volume 17
The Effect of Maternal Attitudes and Depression on Bonding During the Postpartum Period
Authors Şenyaşar Meterelliyoz K ![]() , Çağlar Mengi K, Yazar MS, Akbay Kısa AS
, Çağlar Mengi K, Yazar MS, Akbay Kısa AS ![]()
Received 5 November 2024
Accepted for publication 8 March 2025
Published 15 March 2025 Volume 2025:17 Pages 773—784
DOI https://doi.org/10.2147/IJWH.S504763
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Kumru Şenyaşar Meterelliyoz,1 Kıymet Çağlar Mengi,2 Menekşe Sıla Yazar,3 Ayşe Sevim Akbay Kısa4
1Department of Psychiatry, Bakirköy Prof. Dr. Mazhar Osman Research and Training Hospital for Neurology, Neurosurgery and Psychiatry, Istanbul, Turkey; 2Department of Psychiatry, Edirne Sultan 1st Murat State Hospital, Edirne, Turkey; 3Department of Psychiatry, Altınbaş University, School of Medicine, Istanbul, Turkey; 4Department of Nursing, Obstetrics and Gynecology Nursing, Süleyman Demirel University, Faculty of Health Sciences, Isparta, Turkey
Correspondence: Kumru Şenyaşar Meterelliyoz, Department of Psychiatry, Bakirkoy Prof. Dr. Mazhar Osman Training and Research Hospital for Psychiatry, Neurology, and Neurosurgery, Zuhuratbaba Mah. Akıl Hastanesi Cd. 25/2 Bakırköy, Istanbul, 34147, Turkey, Tel +90 (212) 409 15 15, Email [email protected]
Purpose: Bonding refers to the development of an emotional relationship between a mother and her baby, which forms a strong and continuous bond that provides the baby with a sense of security and plays an important role in its mental well-being throughout life. The objective of this study was to assess the relationship between cognitive distortions, attitudes towards motherhood and postpartum depression, which have not been studied before, as well as to elucidate their impact on the mother-infant bonding process.
Patients and Methods: The sample of the study was created between November 2018- June 2019 using the non-discriminatory multiplicity snowball sampling technique through social media. Women with infants aged 0– 1 year residing in Turkey were asked to participate in the online survey. A sociodemographic data form, the Edinburgh Postpartum Depression Scale, Attitudes Towards Motherhood Scale (AToM), Postpartum Bonding Questionnaire (PBQ), and Cognitive Distortions Scale (CDS) were applied to the sample via social media.
Results: The study sample consisted of 387 women with infants aged 0– 1 years, and the rate of impairment bonding was found to be 11.4%. CDS, ATOM and depression scores were significantly higher in the impaired attached group (p < 0.05). The findings indicated that an individual with a psychiatric diagnosis was 2.653 times more likely to exhibit impaired bonding (OR: 2.653, 95% CI: [1.08– 6.517]; p = 0.033), and those with a higher AToM score were 1.044 times more likely to display impaired bonding (OR: 1.044, 95% CI: [1.013– 1.075]; p = 0.004).
Conclusion: The cognitive structure of the mother is associated with impaired mother-baby bonding. Eliminating the mentioned cognitive elements with psychotherapy interventions will be protective in terms of impaired bonding related to psychopathologies and/or interpersonal relationship problems.
Keywords: postpartum, bonding, attitudes towards motherhood, depression, cognitive distortions
Introduction
Bonding is a two-way interactional process that develops between the infant and the primary caregiver, shaped by the behaviors of both the mother and the infant.1 The development of the emotional relationship between the mother and the baby provides the formation of a strong and continuous bond that provides the baby with a sense of security and plays an important role in its mental well-being throughout its life.2 It is thought that this first relationship structure established between the mother and the baby does not change in the relationship cycles established by the later in life and forms the basis for a recurring basic pattern structure in relationships with others.3–5 Bonding has been shown to be an important predictive indicator of infant social−affective development. Bonding is associated with the cognitive, language, and motor development of the baby.6
To understand mother-infant bonding, it is important to evaluate the mother’s feelings, thoughts, and behaviors, mental health and the interactions between mother and infant as a whole.7 According to cognitive theory, thoughts and beliefs influence and determine emotions and behaviors.8 Understanding and working with the mother’s behaviors and emotions is important because it is a pathway to the mother’s cognition. Although there are studies on women’s mental health and bonding, the relationship between cognitive styles and motherhood cognition and bonding has not been examined.
When examining postpartum depression, which is the most studied subject in bonding in mothers,9 it has been observed that they tend to exhibit a reduced sensitivity to their infants’ needs, a greater tendency towards punitive behaviors, and an increased indifference and rejection in their interactions with the infant.10 When postpartum depression is prolonged and untreated, the adverse effects on the mother–infant relationship are exacerbated, and the risk of developing a impairment bonding is increased.11–13
According to Beck’s cognitive theory, it has long been known that cognitive distortions play an important role in the development and maintenance of depressive symptoms.14 When this model is applied to stressful events, it has been shown that stressor-specific cognitive distortions come to the fore rather than general cognitive distortions and play a role as a vulnerability factor with the diathesis-stress model.15–17 Another factor that affects maternal cognitions is the culture in which they live. In Turkish culture, where the concept of family and motherhood are given considerable importance, the transition to motherhood is an important process in a woman’s life.18 It has been shown in various cultures and in our country that specific dysfunctional attitudes to motherhood are significantly associated with depression symptoms in the period that includes the transition to the role of motherhood of women, such as pregnancy and the postpartum period.17,19–21
In recent years, research has shifted its focus from exploring the personal factors associated with postnatal depression that are challenging to change to a greater emphasis on examining cognitive processes that can be modified through psychological interventions. Identifying and intervening cognitive distortions, which are risk factors that can be changed with psychotherapy interventions, and revealing their effects on mother-infant bonding, will provide an opportunity to eliminate factors that negatively affect mental well-being. Cognitive distortion and dysfunctional attitudes towards motherhood have the potential to act as a modifiable determinant of maternal bonding.
To our knowledge, although the relationship between bonding – postpartum depression, postpartum depression – cognitive distortions has been shown in the literature, there is no study examining the relationship between bonding and the cognitive structure of the woman. Our study is the first to evaluate the effects of maternal cognition and dysfunctional attitudes on mother-infant bonding. Our study aimed to evaluate postpartum depressive symptoms, general and maternal cognitive distortions, and reveal their relationship with the mother-infant bonding process.
Materials and Methods
Methods
The study was approved by Bakirköy Prof. Dr. Mazhar Osman Research and Training Hospital for Neurology, Neurosurgery and Psychiatry Ethic Committee (Decision number: 30.10.2018/36,132).
The study was conducted in accordance with the Declaration of Helsinki. The study was planned by following the STROBE guideline.22 The sample of the study was created between November 2018- June 2019. Because mothers with babies between the ages of 0–1 have limited time for outdoor activities, the sample of our study was created using the non-discriminatory multiple snowball sampling technique to reach more people. The questions and answer options of the scales, all of which were self-report, were created via Google Forms and shared via general social media platforms (eg Facebook, Instagram). Women between the ages of 18–45 years who had children between the ages of 0–1, residing in Turkey, could read and speak Turkish, had internet access, and consented to participate in the study were included in the study.
The sample size was calculated using power analysis with the G*Power 3.1.9.4 program and priority analysis method. A minimum sample size of 172 participants was determined based on a power of 95%, margin of error 0.05, and 0.15 effect size value. Due to the fact that people were reached through certain social networks, the homogeneity of the sample may increase, which may create a disadvantage in terms of generalization of the research.23 The number of participants in our study was kept high considering the disadvantages of the snowball technique.
Participants declared their consent to participate in the study by completing the consent form at the beginning of the online response process, in which the purpose of the study and the procedure to be applied were explained in detail. Participants who agreed to participate in the study were asked to complete a sociodemographic data form, the Edinburgh Postnatal Depression Scale (EPDS), Attitudes Toward Motherhood Scale (AToM), Postpartum Bonding Questionnaire (PBQ), and Cognitive Distortions Scale (CDS), which were arranged for online use. The scales were filled in the form of self-report via Google Forms. Due to the nature of self-report scales, there may be biases in the perception of questions and the accuracy of the results, which may limit generalizability.
Although a total of 450 women started to complete the scale battery, 34 women were not included in the study because their infants were not within the specified age range, and 30 women did not fully complete the scale battery. Accordingly, the sample consisted of 386 women. All women who participated in the survey were informed about the aims of the study and given contact information for mental health support if needed.
Scales
Sociodemographic Data Form
This detailed form was prepared by the researchers for the study, evaluating the demographic information of the participants such as age, sex, education, marital status, income, and medical history. All women participating in the study were informed about the study’s aims. Contact information was given to provide mental health support if needed.
Edinburgh Postnatal Depression Scale (EPDS)
The EPDS was developed by Cox et al.24 This scale was prepared for screening purposes to determine the risk of depression in women in the postpartum period. The first validity and reliability study of EPDS in our country was conducted by Engindeniz et al. A score of 13 and above was accepted as risky for postpartum depression.25
Attitudes Toward Motherhood Scale (AToM)
AToM is a 12-item scale developed by L. Sockol. It consists of three subgroups. Beliefs about the idealization of the maternal role, beliefs about maternal responsibility, and beliefs about the judgments of others are subgroups of this scale. The scale is a 6-point Likert scale and its scoring is between 0 and 5. The total score of the subgroups shows the test total score. High subgroup scores and high-test total scores indicate high dysfunctional attitudes about motherhood.19
Postpartum Bonding Questionnaire (PBQ)
The PBQ was developed by Brockington et al to provide early diagnosis of problems in the mother–infant relationship.26 The scale is completed by the mother. It consists of 25 items with a 6-point Likert scale. The reliability study was conducted by Yalçın et al in 2014. The Turkish version was not found suitable for evaluation with subgroups and the cut-off score was calculated as 26.27
Cognitive Distortions Scale (CDS)
The CDS was developed by Covin et al in 2011, as a 7-point Likert-type scale. The scale consists of 20 items in total and has 10 cognitive distortions (mind reading, catastrophizing or all-or-nothing thinking, reaching conclusions from emotion, labeling, mental filtering, overgeneralization, personalization, imperative statements [should.], underestimating the positive and or ignoring).28 Each cognitive distortion includes two domains, interpersonal and personal. The validity and reliability study of the scale in a Turkish sample was performed by Özdel et al.29
Statistical Analysis
Data were analyzed using the IBM SPSS V23 software package. Conformity to normal distribution was evaluated using Kolmogorov–Smirnov and Shapiro–Wilk tests. Analysis results are presented as mean ± standard deviation and median (minimum-maximum) for quantitative data and as frequency and percentage for categorical data. Spearman correlation analysis was used to compare the PBQ total scores of continuous sociodemographic characteristics. To compare the PBQ total scores of categorical sociodemographic characteristics, the Mann–Whitney U-test was used in groups of two to compare the variables that were not normally distributed. The Kruskal–Wallis H-test was used to compare variables that were not normally distributed according to groups of three or more, and multiple comparisons were examined using the Dunn test.
The sample was divided into two according to the PBQ cut-off score of 26.27 Twenty-six points and above were defined as impaired bonding, and 26 points and below were defined as secure bonding. The independent two-sample t-test was used to evaluate whether the mean scores of the EPDS, AToM, and CDC subgroups and their total scores were different from each other in terms of the secure bonding and impaired bonding groups.
Data that did not show normal distribution were evaluated using the Mann–Whitney U-test. Spearman’s rho correlation coefficient was used to examine the relationship between PBQ, EPDS, ATOM, and CDC points. A binary logistic regression analysis was employed to assess the factors influencing postpartum impaired bonding and examine both univariate and multivariate models. The significance level was accepted as p < 0.05.
Results
The mean age of the women was 27.15 (range, 18–53) years. Of the women, 28.2% were working. Three-quarters (74.6%) of the women had one child. The mean age of infants was 5.94 months. Of the women, 79.3% stated that they had planned pregnancies. It was observed that 43.8% of the women gave birth by normal vaginal delivery. The majority (86.3%) of the women stated that their babies were given to them after birth. The test results according to the sociodemographic characteristics of the sample and PBQ are shown in Table 1.
 |
Table 1 Comparison of PBQ Total Score According to Sociodemographic Characteristics |
When the sample was evaluated according to the EPDS and PBQ cut-off scores, it was seen that 88.6% had secure bonds and 32.4% had depressive symptoms shown in Table 2
 |
Table 2 Descriptive Statistics for the Sample’s PBQ Score and EPDS Score by Cut-off Point |
The total score and subgroup scores of AToM and CDS were evaluated according to the PBQ cut-off score (Table 3).
 |
Table 3 Evaluation of Cognitive Distortions and Depressive Symptoms in Secure and Impairment Bonding |
The interrelationships of the scales used in our study were evaluated using Spearman correlation analysis, significant correlations with AToM, EPDS, and CDS scores are shown in Table 4 (p < 0.001).
 |
Table 4 Spearman Correlation Analysis for Scales |
When the sample was evaluated according to the postpartum bonding questionnaire, the factors affecting impaired bonding were examined as univariate and multivariate models using binary logistic regression analysis. In the univariate model, those with a psychiatric diagnosis were 3.575 times more likely to have impaired bonding risk (OR: 3.575, 95% CI: [1.589–8.04]; p = 0.002). As the dysfunctional attitudes towards motherhood increased, the risk of impaired bonding increased 1.051 times (OR:1.051, 95% CI: [1.025–1.077]; p < 0.001). As the depressive symptoms increased by 1 point, the risk of impaired bonding increased 1.092 times (OR:1.092, 95% CI: [1.041–1.145]; p < 0.001). As the cognitive distortions increased, the risk of impaired bonding increased 1.015 times (OR: 1.015, 95% CI: [1.002–1.028]; p = 0.023). Although cognitive distortions and depressive symptoms significantly predict impaired bonding in univariate analyses, their significance was reduced when other variables were included. Beliefs according to the judgments of others score increased, and the risk of impaired bonding increased 1.119 times (OR: 1.119 95% CI: [1.073–1.168]; p < 0.001). As the maternal role idealization score increased, the risk of impaired bonding increased 1.063 times (OR: 1.063, 95% CI: [1–1.13]; p = 0.049). No other variables were statistically significant (p > 0.05).
When the multivariate model was examined, it was determined that the presence of psychiatric diagnosis and dysfunctional attitudes towards motherhood predicted impaired bonding. It was observed that the presence of a psychiatric disease increased the risk of impaired bonding by 2.653 times (OR: 2.653, 95% CI: [1.08–6.517]; p = 0.033) and when the dysfunctional attitudes towards motherhood increased by 1 point, the risk of impaired bonding increased by 1.044 times (OR: 1.044, 95% CI: [1.013–1.075]; p = 0.004) (Table 5).
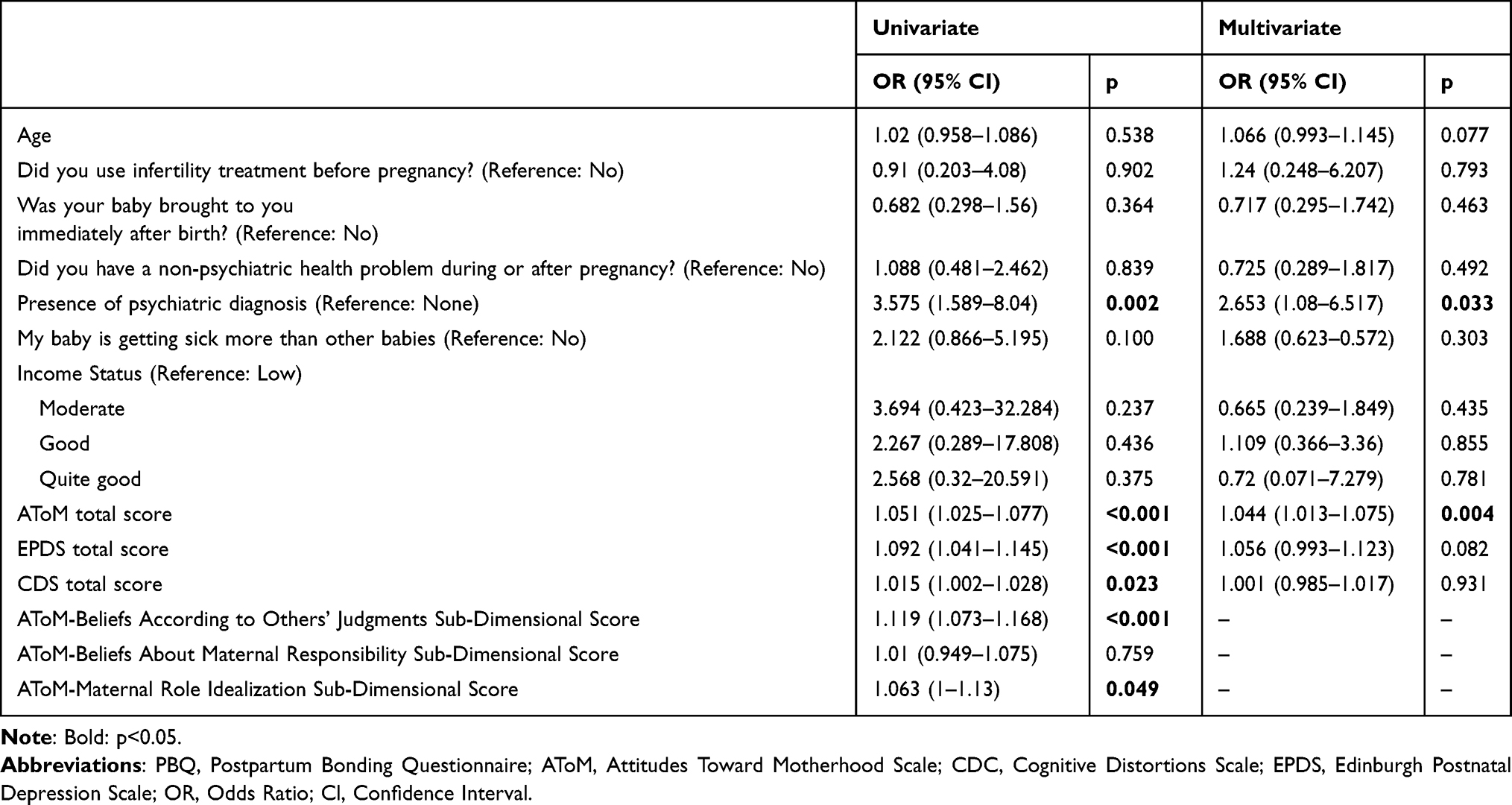 |
Table 5 Examination of Factors Affecting Impairment Bonding With a Binary Logistic Regression Model |
Discussion
In our study, it was found that the rate of impaired bonding was 11.4%, and 32.4% of the participants had depressive symptomatology (Table 2). In the group with impaired bonding, beliefs according to the judgments of others, catastrophizing and minimizing the positive, and CDS total scores were found to be significantly higher than the securely bonded group (Table 3). When the factors affecting impaired bonding were examined, it was shown that the presence of a psychiatric diagnosis and the total score of AToM predicted impaired bonding. The risk of impaired bonding increased 2.653 times in those with a psychiatric diagnosis. It was determined that as the AToM total score increased, the risk of impaired bonding increased 1.044 times (Table 5).
When the sociodemographic characteristics of the study sample were evaluated, the level of impaired bonding was found to be statistically significantly higher in participants who were not given their baby immediately after birth and in participants with a psychiatric diagnosis in the pregnancy and postpartum period (Table 1). It is stated that close contact immediately after birth contributes physically to the health of the newborn and the mother, and bonding. For a newborn, the mother’s body is defined as a natural playground.30 It has been stated that sensual contact in the postnatal period causes an increase in the mother’s interest and communication with the baby in the short and long term. In studies, it was found that mothers who had physical contact for 16 hours or longer postpartum were associated with being more attentive during the examination of the baby, not wanting to leave the baby, having more eye contact with the baby, and being more calming and caressing the baby31 In line with the existing literature, our findings suggest that mothers who are separated from their infants after birth due to medical or social reasons have higher levels of impaired bonding.
In our study, when the sample was examined according to the PBQ cut-off score, 11.4% were found to have impaired bonding characteristics (Table 2). When the bond between parents and infants is evaluated in studies conducted in community samples, it is seen that impaired bonding rates approach 10%.32 The results of our study are consistent with the rates of impaired bonding in the literature.
When our sample was analyzed according to the EPDS cut-off score, 32.4% of the women had depressive symptoms (Table 2). In meta-analysis, the rate of postpartum depression varies between 8% and 28%.33–35 It is stated that the rates are higher in developing countries.36 In a meta-analysis assessing depressive symptoms in the postnatal period within our country, the prevalence of postpartum depression (PPD) was found to range from 9.1% to 51.3%, with an aggregate prevalence rate of 25.2%.37 Our study revealed a higher prevalence of depressive symptoms than that reported in previous research. This finding may be attributed to the characteristics of the sample.
In our study, women with impaired bonding exhibited a higher level of depressive symptoms (Table 3). Studies have shown that mothers with depression symptoms are more likely to experience bonding problems in the first few months postpartum, regardless of the severity of the depression.38–40 Cornish et al found that women with chronic depression experienced greater impairment in bonding with their babies and reported higher levels of hostility and anger towards their offspring compared to women with short-term depression and healthy controls.41 As in our study, Warfa et al reported in their meta-analysis that postpartum depression is associated with impaired bonding.42 The development of a more comprehensive understanding of the shared risk factors between impaired bonding and depression, which frequently co-occur, could significantly contribute to the optimization of treatment approaches for both conditions.
In our study examining the factors influencing maternal bonding among women with infants aged 0–1 years, we found that the presence of a psychiatric diagnosis increased the risk of impaired bonding by a factor of 2.653, while dysfunctional attitudes toward motherhood were associated with a 1.044-fold increase in the risk of impaired bonding (Table 5). The presence of a psychiatric diagnosis has been closely associated with impaired bonding, although it does not always occur. Impaired bonding is detected in the general population at a rate of 3–9%; however, it is reported that the rate of mother–infant relationship problems in the psychiatric population increases to 10–25%.43–45 There is evidence showing that the presence of psychiatric diagnoses such as depression, anxiety disorders, and PTSD is associated with impaired bonding.40,46,47 Ozcan et al evaluated women with postpartum mental disorders and found that women with mental disorders were more impaired bonding than healthy controls, they took care of the babies less, and the duration of breastfeeding was shorter than in healthy controls.48 Parfitt et al examined the transition to parenthood in men and women who became parents for the first time in their study and found that people with mental disorders started to have positive feelings towards the baby later than the healthy population.49
The presence of psychiatric disorders in the mother may cause impaired bonding patterns by affecting the bonding and this may increase the risk of children having problems in cognitive, emotional, and interpersonal relationships in their future lives.50
Our study is consistent with studies in the literature reporting that bonding is impaired in the presence of mental disorders and that the presence of mental disorders is an important risk factor for impaired bonding.51–53 It may be crucial for women with mental disorders to receive psychiatric follow-up and clinical support during their decision to become mothers and during their motherhood experience in terms of bonding.51–53
In our study, it was determined that impaired bonded women had higher general cognitive distortions, catastrophizing, ignoring the positive and dysfunctional attitudes towards motherhood compared with securely bonded women (Table 3). According to cognitive theory, cognitive styles in which a person evaluates the world take shape at an early age by the by the family and culture. Cognitive style has been shown to influence how individuals evaluate the world around them, their self-concept, and their parenting.54,55 In studies conducted in our country, it has been stated that Turkey is a more collectivist country compared with the Czech Republic and Spain.56 In our country, a traditional mother is expected to have high standards in childcare.57 This is thought to affect women’s cognition related to motherhood. In a study conducted in our country, it was shown that dysfunctional attitudes associated with motherhood were associated with postpartum depression and anxiety symptoms.21 Ingram et al examined the relationship between bonding and dysfunctional thoughts and showed that individuals reporting positive maternal bonding had less negative and more positive thoughts than those reporting impaired bonding.55 This finding suggests that the increased risk of impaired bonding may be explained by more negative automatic thoughts. Our study supports and extends previous research indicating that women with impaired bonding have more negative automatic thoughts55,58 and extends this understanding by identifying specific types of automatic thoughts such as catastrophizing and ignoring the positive.
It was determined in previous studies that women with postpartum depression were overly critical of the maternal role and associated high-performance standards with extreme self-sacrifice. In this case, it has been stated that in line with the high-performance standards that the individuals expect from themselves, they evaluate events related to their own parenting experiences negatively, so that negative events are perceived as more catastrophic, which makes it difficult to adapt to the mothering role.59–61 The fact that women who ignore the positive about themselves and their motherhood and catastrophized the problems, focus on negative thoughts such as inadequacy about themselves and motherhood in the new role change process may lead to the inability to read the baby’s needs correctly and negatively affect mother-infant bonding.58
According to the findings of our study, it was revealed that dysfunctional attitudes towards motherhood increased impaired bonding 1.044 times (Table 5). Dysfunctional attitudes specific to motherhood are an important component of women’s psychological experiences during the transition to motherhood.62 In particular, the idea of inadequacy and beliefs about negative judgments of others are among the dysfunctional attitudes that emerge in the postpartum period. Dysfunctional motherhood beliefs have been associated with postpartum depressive symptoms,20,63 eating disorders64,65 and emotional distress.62
Our study examines the impact of dysfunctional maternal attitudes, which have been shown to be the main component of psychological stress in the postpartum period62 on bonding.
There are few studies in the literature examining the relationship cognitive distortions, cognitive structure on bonding. Gamble et al examined the relationship between parenting styles and dysfuncitonally attitudes and impaired bonding. Their findings suggest that adolescents who perceive their parents as critical and perfectionistic may develop dysfunctional attitudes through impaired bonding. Additionally, they found that these adolescents tend to perceive negative events as more global, stable, and internal in nature.66 Although there are studies showing that adolescents and adults with an impaired bonding have more frequent dysfunctional attitudes and less positive automatic cognitions,67,68 there is no study examining the cognitive style of the mother/woman on bonding in the literature.
Our study highlights the strong relationship between dysfunctional maternal attitudes and impaired bonding, emphasizing the importance of screening for these attitudes during early pregnancy and the postnatal period. Screening that can be performed during pregnancy and postpartum follow-up will provide an opportunity for the detection of risky groups and early preventive interventions in terms of public health. In addition, the training to be provided during this process will make a significant contribution to raising public awareness and implementing early intervention strategies more effectively. Furthermore, it provides a basis for cognitive psychotherapy interventions targeting these attitudes, and underlines that this method can strengthen the mother-infant bond.
Conclusion
Bonding style, which develops from early childhood and continues consistently throughout life, has been shown to cause depressive symptoms and mental problems in relation to cognitive distortions in adulthood.69 In our study, depression symptoms, dysfunctional attitudes toward motherhood and general cognitive distortions were more common in women with impaired bonding than in those with secure bonding. Furthermore, we demonstrated that dysfunctional attitudes toward motherhood and the presence of psychiatric diagnoses increase the risk of impaired bonding among women with infants aged 0–1 years. It can be thought that early detection of factors that may adversely affect bonding and the removal of these cognitive factors with psychotherapy interventions will be protective in terms of impaired bonding associated with psychopathologies and/or interpersonal relationship problems in adulthood. Cognitive distortions and psychoeducation that can be screened with short and self-applicable scales in routine checkups during pregnancy and the postpartum period form the basis for early preventive interventions in terms of identification of risk groups and public health.
The present study is strengthened by several factors. Primarily, the relationship between bonding and attitudes toward motherhood has not been previously examined in the literature. Secondly, in addition to the effects of mother-infant bonding on children, the fact that it was handled with an approach from a women’s mental health perspective and that the cognitive structure of women was evaluated are among the strengths of our study. Our results may also prove useful for physicians and researchers interested in developing interventions cognitive behavior therapy in women’s mental health.
The limitations of our study are that our scales are self-reported and sample was totally online, so it may not be representative of the Turkish population. Therefore, future studies should include different recruitment methods (eg, online and face-to-face). Secondly, the study was cross-sectional in design. Although the relationship between dysfunctional attitudes and impaired bonding has been shown, it cannot be concluded that it fully explains the nature of the relationship due to the cross-sectional nature of the study. It is necessary to clarify the relationship between dysfunctional attitudes towards motherhood and bonding with longitudinal studies. Another limitation of the current study was the homogeneity of our subjects. The lack of sociodemographic diversity is a demonstrated problem in healthcare research.70 It is further recommended that future research explores the role of maternal attitudes in bonding by increasing participant diversity. Specifically, our findings suggest that postpartum women’s motherhood dysfunctional attitudes play an important role in bonding. Additionally, future research can explore whether there is a mediating effect of (ie, depression, anxiety, anxiety, sensitivity, relationship, social support) on the relationship between dysfunctional attitudes or beliefs toward motherhood and important and relevant outcomes such as impaired bonding.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Feldman R, Weller A, Leckman JF, Kuint J, Eidelman AI. The nature of the mother’s tie to her infant: maternal bonding under conditions of proximity, separation, and potential loss. J Child Psychol Psychiatry Allied Disciplines. 1999;40(6):929–939. doi:10.1111/1469-7610.00510
2. Winston R, Chicot R. The importance of early bonding on the long-term mental health and resilience of children. London J Prim Care. 2016;8(1):12–14. doi:10.1080/17571472.2015.1133012
3. Opie JE, McIntosh JE, Esler TB, et al. Early childhood attachment stability and change: a meta-analysis. Attach Hum Dev. 2021;23(6):897–930. doi:10.1080/14616734.2020.1800769
4. Chris Fraley R. Attachment stability from infancy to adulthood: meta-analysis and dynamic modeling of developmental mechanisms. Personality Social Psychol Rev. 2002;6(2):123–151. doi:10.1207/S15327957PSPR0602_03
5. Hamilton CE. Continuity and discontinuity of attachment from infancy through adolescence. Child Dev. 2000;71(3):690–694. doi:10.1111/1467-8624.00177
6. Le Bas G, Youssef G, Macdonald JA, et al. The role of antenatal and postnatal maternal bonding in infant development. J Am Acad Child Adolesc Psychiatry. 2022;61(6):820–829. doi:10.1016/j.jaac.2021.08.024
7. Murray L, Cooper PJ, Wilson A, Romaniuk H. Controlled trial of the short-and long-term effect of psychological treatment of post-partum depression: 2. Impact on the mother-child relationship and child outcome. Br J Psychiatry. 2003;182(5):420–427. doi:10.1192/bjp.182.5.420
8. Beck AT, Weishaar M. Cognitive therapy. In: Comprehensive Handbook of Cognitive Therapy. Springer; 1989:21–36.
9. Olivine AM. Predictive Factor or Factors That Most Influence Maternal-Infant Attachment during Postpartum: A Meta-Analysis. Doctoral dissertation. Northcentral University; 2021.
10. Wittkowski A, Garrett C, Cooper A, Wieck A. The relationship between postpartum depression and beliefs about motherhood and perfectionism during pregnancy. J Woman’s Reprod Health. 2017;1(4):9. doi:10.14302/issn.2381-862X.jwrh-15-848
11. Pawlby S, Sharp D, Hay D, O’Keane V. Postnatal depression and child outcome at 11 years: the importance of accurate diagnosis. J Affect Disord. 2008;107(1–3):241–245. doi:10.1016/j.jad.2007.08.002
12. Milgrom J, Westley D, Gemmill AW. The mediating role of maternal responsiveness in some longer-term effects of postnatal depression on infant development. Infant Behav Dev. 2004;27. doi:10.1016/j.infbeh.2004.03.003
13. Righetti-Veltema M, Bousquet A, Manzano J. Impact of postpartum depressive symptoms on mother and her 18-month-old infant. Eur Child Adolesc Psychiatry. 2003;12(2):75–83. doi:10.1007/s00787-003-0311-9
14. Beck AT. Cognitive Therapy of Depression. Guilford press; 1979.
15. Clak DA, Beck AT. Scientific Foundations of Cognitive Theory and Therapy of Depression. John Wiley & Sons; 1999.
16. Beck AT, Haigh EAP. Advances in cognitive theory and therapy: the generic cognitive model. Annu Rev Clin Psychol. 2014;10(1):1–24. doi:10.1146/annurev-clinpsy-032813-153734
17. Sockol LE. A systematic review of the efficacy of cognitive behavioral therapy for treating and preventing perinatal depression. J Affect Disord. 2015;177:7–21. doi:10.1016/j.jad.2015.01.052
18. Bornstein MH. Cultural Approaches to Parenting. Psychology Press; 2013.
19. Sockol LE, Epperson CN, Barber JP. The relationship between maternal attitudes and symptoms of depression and anxiety among pregnant and postpartum first-time mothers. Arch Womens Ment Health. 2014;17(3):199–212. doi:10.1007/s00737-014-0424-9
20. Fonseca A, Canavarro MC. Exploring the paths between dysfunctional attitudes towards motherhood and postpartum depressive symptoms: the moderating role of self‐compassion. Clin Psychol Psychother. 2018;25(1):e96–e106. doi:10.1002/cpp.2145
21. Şenyaşar Meterelliyoz K, Yazar MS. Dysfunctional attitudes toward motherhood that predict anxiety and depressive symptoms during pregnancy. J Cognit-Behav Psychotherapy Res. 2024;34–44. doi:10.5455/jcbpr.153396
22. Babaoğlu AB, Tekindal M, Büyükuysal MÇ, et al. Epidemiyolojide gözlemsel çalışmaların raporlanması: STROBE kriterlerinin Türkçe uyarlaması. Bati Karadeniz Tip Dergisi. 2021;5(1):86–93. Turkish. doi:10.29058/mjwbs.869832
23. Leighton K, Kardong-Edgren S, Schneidereith T, Foisy-Doll C. Using social media and snowball sampling as an alternative recruitment strategy for research. Clin Simul Nurs. 2021;55:37–42. doi:10.1016/j.ecns.2021.03.006
24. Cox J, Holden J, Sagovsky R. Detection of postnatal depression: development of a 10 item postnatal depression scale. Br J Psychiatry. 1987;150. doi:10.1192/bjp.150.6.782
25. Engindeniz AN, Küey L, Kültür S. Edinburgh doğum sonrası depresyon ölçeği Türkçe formu geçerlilik ve güvenilirlik çalışması. Bahar Sempozyumlari. Turkish. 1996;1:51–52.
26. Brockington I. Maternal rejection of the young child: present status of the clinical syndrome. Psychopathology. 2011;44(5):329–336. doi:10.1159/000325058
27. Yalçın SS, Örün E, Özdemir P, Mutlu B, Dursun A. Türk annelerde doğum sonrası bağlanma ölçeklerinin güvenilirliği. Çocuk Sagligi ve Hastaliklari Dergisi. Turkish. 2014;57(4):246–251.
28. Covin R, Dozois DJA, Ogniewicz A, Seeds PM. Measuring cognitive errors: initial development of the cognitive distortions scale (CDS). Int J Cogn Ther. 2011;4(3):297–322. doi:10.1521/ijct.2011.4.3.297
29. Özdel K, Taymur İ, Guriz SO, Tulaci RG, Kuru E, Turkcapar MH. Measuring cognitive errors using the cognitive distortions scale (CDS): psychometric properties in clinical and non-clinical samples. PLoS One. 2014;9(8):e105956. doi:10.1371/journal.pone.0105956
30. Winberg JAN. Mother and newborn baby: mutual regulation of physiology and behavior—a selective review. Develop Psychobiol. 2005;47(3):217–229. doi:10.1002/dev.20094
31. Joas J, Möhler E. Maternal bonding in early infancy predicts childrens’ social competences in preschool age. Front Psychiatry. 2021;12:687535. doi:10.3389/fpsyt.2021.687535
32. Skovgaard AM, Houmann T, Christiansen E, et al. The prevalence of mental health problems in children 1½ years of age–the Copenhagen child cohort 2000. J Child Psychol Psychiatry. 2007;48(1):62–70. doi:10.1111/j.1469-7610.2006.01659.x
33. Gavin NI, Gaynes BN, Lohr KN, Meltzer-Brody S, Gartlehner G, Swinson T. Perinatal depression: a systematic review of prevalence and incidence. Obstetrics Gynecol. 2005;106(5 Part 1):1071–1083. doi:10.1097/01.AOG.0000183597.31630.db
34. Milgrom J, Gemmill AW, Bilszta JL, et al. Antenatal risk factors for postnatal depression: a large prospective study. J Affect Disord. 2008;108(1–2):147–157. doi:10.1016/j.jad.2007.10.014
35. O’hara MW, Swain AM. Rates and risk of postpartum depression—a meta-analysis. Int Rev Psychiatry. 1996;8(1):37–54. doi:10.3109/09540269609037816
36. Xiong R, Deng A. Prevalence and associated factors of postpartum depression among immigrant women in Guangzhou, China. BMC Pregnancy Childbirth. 2020;20(1):1–7. doi:10.1186/s12884-020-02946-4
37. Karaçam Z, Çoban A, Akbaş B, Karabulut E. Status of postpartum depression in Turkey: a meta-analysis. Health Care Women Int. 2018;39(7):821–841. doi:10.1080/07399332.2018.1466144
38. Ayers S, Wright DB, Wells N. Symptoms of post‐traumatic stress disorder in couples after birth: association with the couple’s relationship and parent–baby bond. J Reprod Infant Psychol. 2007;25(1):40–50. doi:10.1080/02646830601117175
39. Moehler E, Brunner R, Wiebel A, Reck C, Resch F. Maternal depressive symptoms in the postnatal period are associated with long-term impairment of mother–child bonding. Arch Womens Ment Health. 2006;9:273–278. doi:10.1007/s00737-006-0149-5
40. Parfitt YM, Ayers S. The effect of post‐natal symptoms of post‐traumatic stress and depression on the couple’s relationship and parent–baby bond. J Reprod Infant Psychol. 2009;27(2):127–142. doi:10.1080/02646830802350831
41. Cornish AM, McMahon CA, Ungerer JA, Barnett B, Kowalenko N, Tennant C. Maternal depression and the experience of parenting in the second postnatal year. J Reprod Infant Psychol. 2006;24(02):121–132. doi:10.1080/02646830600644021
42. Warfa N, Harper M, Nicolais G, Bhui K. Adult attachment style as a risk factor for maternal postnatal depression: a systematic review. BMC Psychol. 2014;2(1):1–11. doi:10.1186/s40359-014-0056-x
43. O’Dea GA, Youssef GJ, Hagg LJ, et al. Associations between maternal psychological distress and mother-infant bonding: a systematic review and meta-analysis. Arch Womens Ment Health. 2023;26(4):441–452. doi:10.1007/s00737-023-01332-1
44. Brockington IF, Fraser C, Wilson D. The postpartum bonding questionnaire: a validation. Arch Womens Ment Health. 2006;9:233–242. doi:10.1007/s00737-006-0132-1
45. Brockington I. Postpartum psychiatric disorders. Lancet. 2004;363(9405):303–310. doi:10.1016/S0140-6736(03)15390-1
46. Field T, Diego M, Hernandez-Reif M, et al. Comorbid depression and anxiety effects on pregnancy and neonatal outcome. Infant Behav Dev. 2010;33(1):23–29. doi:10.1016/j.infbeh.2009.10.004
47. Glasheen C, Richardson GA, Fabio A. A systematic review of the effects of postnatal maternal anxiety on children. Arch Womens Ment Health. 2010;13:61–74. doi:10.1007/s00737-009-0109-y
48. Özcan NK, Boyacıoğlu NE, Dikeç G, Dinç H, Enginkaya S, Tomruk N. Prenatal and postnatal attachment among Turkish mothers diagnosed with a mental health disorder. Issues Ment Health Nurs. 2018;39(9):795–801. doi:10.1080/01612840.2018.1455773
49. Parfitt Y, Ayers S. Transition to parenthood and mental health in first‐time parents. Infant Ment Health J. 2014;35(3):263–273. doi:10.1002/imhj.21443
50. Ramchandani P, Psychogiou L. Paternal psychiatric disorders and children’s psychosocial development. Lancet. 2009;374(9690):646–653. doi:10.1016/S0140-6736(09)60238-5
51. Brand SR, Brennan PA. Impact of antenatal and postpartum maternal mental illness: how are the children? Clin Obstet Gynecol. 2009;52(3):441–455. doi:10.1097/GRF.0b013e3181b52930
52. Gumley AI, Taylor HEF, Schwannauer M, MacBeth A. A systematic review of attachment and psychosis: measurement, construct validity and outcomes. Acta Psychiatr Scand. 2014;129(4):257–274. doi:10.1111/acps.12172
53. Wan MW, Green J. The impact of maternal psychopathology on child–mother attachment. Arch Womens Ment Health. 2009;12:123–134. doi:10.1007/s00737-009-0066-5
54. Beck AT. Depression: Clinical, Experimental, and Theoretical Aspects. University of Pennsylvania Press; 1967. Vol 32.
55. Ingram RE, Overbey T, Fortier M. Individual differences in dysfunctional automatic thinking and parental bonding: specificity of maternal care. Pers Individ Dif. 2001;30(3):401–412. doi:10.1016/S0191-8869(00)00032-5
56. Hofstede G. Dimensionalizing cultures: the Hofstede model in context. Online Readings Psychol Culture. 2011;2(1):8. doi:10.9707/2307-0919.1014
57. Aytac FK. Is it love? The mediating role of traditional motherhood between maternal warmth and maternal gatekeeping. Curr Psychol. 2023;42(8):1–15.
58. Rodrigues S, Canavarro MC, Fonseca A. Attachment representations and maternal confidence: the mediating role of postnatal depressive symptoms and negative thoughts. J Child Fam Stud. 2018;27:3585–3597. doi:10.1007/s10826-018-1182-5
59. Delmore-Ko P, Pancer SM, Hunsberger B, Pratt M. Becoming a parent: the relation between prenatal expectations and postnatal experience. J Family Psychol. 2000;14(4):625. doi:10.1037/0893-3200.14.4.625
60. Gelabert E, Subirà S, García-Esteve L, et al. Perfectionism dimensions in major postpartum depression. J Affect Disord. 2012;136(1–2):17–25. doi:10.1016/j.jad.2011.08.030
61. O’Mahen HA, Flynn HA, Nolen-Hoeksema S. Rumination and interpersonal functioning in perinatal depression. J Soc Clin Psychol. 2010;29(6):646–667. doi:10.1521/jscp.2010.29.6.646
62. Sockol LE, Battle CL. Maternal attitudes, depression, and anxiety in pregnant and postpartum multiparous women. Arch Womens Ment Health. 2015;18(4):585–593. doi:10.1007/s00737-015-0511-6
63. Thompson KD, Bendell D. Depressive cognitions, maternal attitudes and postnatal depression. J Reprod Infant Psychol. 2014;32(1):70–82. doi:10.1080/02646838.2013.858312
64. Lai BP, Tang CS, Tse WK. A longitudinal study investigating disordered eating during the transition to motherhood among Chinese women in Hong Kong. Int J Eating Disorders. 2006;39(4):303–311. doi:10.1002/eat.20266
65. O’Loghlen E, Galligan R. Disordered eating in the postpartum period: role of psychological distress, body dissatisfaction, dysfunctional maternal beliefs and self-compassion. J Health Psychol. 2022;27(5):1084–1098. doi:10.1177/1359105321995940
66. Gamble SA, Roberts JE. Adolescents’ perceptions of primary caregivers and cognitive style: the roles of attachment security and gender. Cognit Ther Res. 2005;29(2):123. doi:10.1007/s10608-005-3160-7
67. Reinecke MA, Rogers GM. Dysfunctional attitudes and attachment style among clinically depressed adults. Behav Cognitive Psychother. 2001;29(2):129–141. doi:10.1017/S1352465801002016
68. Roberts JE, Gotlib IH, Kassel JD. Adult attachment security and symptoms of depression: the mediating roles of dysfunctional attitudes and low self-esteem. J Pers Soc Psychol. 1996;70(2):310. doi:10.1037/0022-3514.70.2.310
69. Bowlby J. Attachment and loss. Volume II. Separation, anxiety and anger. In: Attachment and Loss. Volume II. Separation, Anxiety and Anger. 1973:429–p.
70. Woodall A, Morgan C, Sloan C, Howard L. Barriers to participation in mental health research: are there specific gender, ethnicity and age related barriers? BMC Psychiatry. 2010;10:1–10. doi:10.1186/1471-244X-10-103
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.