")
Back to Journals » Patient Preference and Adherence » Volume 17
The Effect of Health Literacy on Preoperative Anxiety Levels in Patients Undergoing Elective Surgery
Authors Demirel A , Balkaya AN, Onur T, Karaca Ü, Onur A
Received 19 May 2023
Accepted for publication 22 July 2023
Published 11 August 2023 Volume 2023:17 Pages 1949—1961
DOI https://doi.org/10.2147/PPA.S419866
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Asiye Demirel, Ayşe Neslihan Balkaya, Tuğba Onur, Ümran Karaca, Anıl Onur
University of Health Sciences, Bursa Yuksek Ihtisas Training and Research Hospital, Department of Anaesthesiology and Reanimation, Bursa, Turkey
Correspondence: Asiye Demirel, University of Health Sciences, Bursa Yuksek Ihtisas Training and Research Hospital, Department of Anaesthesiology and Reanimation, Mimar Sinan District, Emniyet Street, Yıldırım, Bursa, Turkey, Tel +90 224 2955000, Fax +90 224 295 54 97, Email [email protected]
Objective: This study aimed to determine preoperative anxiety levels, their associated factors, and the relationship between health literacy and preoperative anxiety in adult patients undergoing elective surgery.
Materials and Methods: This descriptive cross-sectional study was conducted in a tertiary hospital between December 21, 2021, and June 20, 2022, and included 466 adult patients. Participants were administered the demographic data and basic health status form, Health Literacy Scale (HLS), and Beck Anxiety Inventory (BAI). Statistical significance was set at p < 0.05.
Results: The participants’ mean BAI score was low to moderate (9.28± 10.85). The total HLS score was 105.89± 24.42. For the BAI, a negative correlation was found between the access to information sub-dimensions of the HLS and BAI (p=0.043, r=− 0.094). In addition, a negative correlation was detected between patients’ age and HLS and its sub-dimensions (p< 0.001, respectively [r=− 0.188, r=− 0.193, r=− 0.205, r=− 0.161]), and a positive correlation was observed among the HLS sub-dimensions (p< 0.001, respectively [r=0.873, r=0.057, r=0.966, r=0.915]). Higher HLS and sub-dimension averages were observed in single, high school, university graduates, and civil servant participants. In addition, higher BAI averages were detected in females, homemakers, urban residents, participants living only with their children, and those with additional diseases (respectively, p< 0.001, p< 0.001, p=0.007, p=0.0034, p< 0.01).
Conclusion: As the level of health literacy increased, preoperative anxiety levels decreased. Preoperative assessment and education are fundamental to perioperative patient care, particularly in the surgical setting.
Keywords: preoperative anxiety, health literacy, Beck Anxiety Inventory, anesthesia, surgery
Introduction
The surgical process is stressful and triggers emotional, cognitive, and physiological responses. Anxiety can be explained as feelings of uncertainty, uneasiness, apprehension, or tension that a person experiences in response to an unknown object or situation.1 Preoperative anxiety (PA), generally considered a type of state anxiety related to impending surgery, is likely linked to individual personality traits and coping processes. A growing number of studies have indicated that PA is associated with increased and worse perioperative outcomes, including impaired wound healing, nausea, vomiting, and postoperative pain.2 Although PA varies by country and region, according to the type of surgery, patients’ sex and age; the prevalence of anxiety in the preoperative period ranges from 11% to 80% due to reasons such as separation from family, expectations of postoperative pain, type of surgery or procedures, first surgical intervention, fear of not waking up from surgery, inability to work after surgery, fear of anesthesia, and death.3–8 Surgical anxiety can lead to cardiac problems, rehospitalizations, decreased quality of life, postoperative pain, increased analgesic use, prolonged hospital stays, adverse effects, experiences during patient recovery, and reduced patient satisfaction.3,9,10
In the information age, individuals are expected to be knowledgeable about their illnesses, detect symptoms, and make appropriate decisions. These decisions are often based on health-related knowledge, skills, and capacities. This is called health literacy (HL).11 The World Health Organization (WHO) defines HL as cognitive and social skills related to individuals’ abilities and desires to access, understand, and use health information to maintain and improve well-being.12
Most patients may not express anxiety during the preoperative period unless asked. Therefore, patients should be carefully assessed and their PA levels should be determined. In addition, patients must understand the nature, risks, and benefits of surgical procedures; comply with instructions related to surgery; and make complex care decisions about interventions; thus, HL is essential.13
Clinicians and researchers have recently begun to evaluate PA.14 Various tests, such as the State-Trait Anxiety Inventory (STAI), Amsterdam Preoperative Anxiety and Information Scale (APAIS), Hospital Anxiety and Depression Scale, Taylor Anxiety Scale, Hamilton Anxiety Scale, and Depression Anxiety and Stress Scale, were used to assess anxiety. These tests have proven useful for evaluating PA and general anxiety.14 The Beck Anxiety Inventory (BAI) is another scale used to assess general anxiety in patients and has been incorporated into studies also in our country.15,16 Although the literature on PA levels measured by the BAI in patients undergoing surgery is limited, we did not find any publications evaluating the relationship between PA levels measured by the BAI and HL levels.
This study was conducted at a training and research hospital in the western region of Turkey to determine the levels of HL and associated risk factors in patients undergoing planned surgery. The primary objective of this study was to investigate the relationship between HL status and PA levels. Second, we explored the interaction between PA and HL using demographic and basic health status-related data.
Materials and Methods
Study Design and Patient Selection
This prospective observational study was conducted between December 21, 2021, and June 20, 2022, after obtaining approval from the Health Sciences University Bursa Yuksek Ihtisas Training and Research Hospital Ethics Committee on December 15, 2021, with decision number 2011-KAEK-25 2021/12-17. The study was conducted in the anesthesiology and reanimation outpatient clinics of our hospital. Patients included in the study were those who were scheduled for any planned surgery, aged 18 and above, had at least primary school education, were Turkish-speaking, conscious, and communicative, classified as American Society of Anesthesiology (ASA) Groups I and II, cooperative, and voluntarily participated in the study. Illiterate patients, classified as ASA III–IV, who did not consent to participate, were pregnant, had dementia or psychiatric disorders, were excluded from the study.
Questionnaire Forms
Written informed consent was obtained from all the patients who agreed to participate in the study. A three-part questionnaire was administered at the anesthesiology outpatient clinic one week before the operation. All patients were adequately informed about the research and anesthesia methods to be applied. The first part of the form is prepared by the researchers and questions included patients’ demographic and basic health status-related data; the second part is self-filling questionnaire consisted of the HLS to determine health literacy; and the third part is self-filling questionnaire contained the BAI to evaluate PA levels. The total time to complete all the questions was 20–25 minutes.17,18
Part 1: Demographic Data and Basic Health Status Form
This form consisted of questions about individuals’ age, sex, occupation, education, marital status, income status, where they live and with whom, other diseases, medications they regularly use, previous surgery and anesthesia experiences, and information about the surgery they would undergo.
Part 2: Health Literacy Scale
This scale was developed by Sorensen et al (Health Literacy Survey in Europe-HLS-EU)19 was simplified to 25 items by Toçi and Burazeri.17 The validity and reliability of this scale were assessed by Aras and Bayık Temel.18 The scale consists of 25 questions and four sub-dimensions: 1) access to information, with a score range of 5–25 (min.-max.); 2) understanding information, with a score range of 7–35 (min.-max.); 3) appraisal/evaluation, with a score range of 8–40 (min.-max.); and 4) application/use, with a score range of 5–25 (min.-max.). The total score obtained ranged from 25 to 125. Scale items are answered by participants in a Likert format, as follows: “5: No difficulty, 4: A little difficulty, 3: Some difficulty, 2: A lot of difficulty, 1: Unable to do it at all/ have no ability/ impossible”. All items on the scale were positively worded with no reverse-coded items. Low scores indicate inadequate, problematic, and weak HL, while high scores indicate sufficient and excellent HL. As the score increases, an individual’s HL level increases.17
Part 3: Beck Anxiety Inventory (BAI)
This self-assessment scale measures the frequency of anxiety symptoms experienced by an individual. It consists of 21 items scored on a Likert-type scale, ranging from 0 to 3. The higher the total score, the higher the anxiety experienced by the individual. It was developed by Beck et al, and its validity and reliability in Turkey were evaluated by Ulusoy et al20,21 Anxiety levels were assessed as follows: 0–7 points = normal anxiety, 8–15 points = mild anxiety, 16–25 points = moderate anxiety, and 26–63 points = severe anxiety.
All patients were scheduled for elective surgeries classified as minor, medium, or major, based on blood loss, pain intensity, invasiveness, required monitoring level, and length of hospital stay due to the surgical procedure. The types and sizes of the surgeries performed were grouped according to the list regulated in Article 22 of the Health Implementation Notification published by the Social Security Institution in the Official Gazette of Turkey.22 Patients were informed of the size of their surgeries.22 In the study, the answers given by the patients to the monthly income levels were determined according to the monthly minimum wage they received at the time of the study. Low income is the amount below the minimum wage.
Surgical Groups
Group A surgeries (intracranial mass, intracranial aneurysm, total gastrectomy, rectal and colon surgery, Whipple operation, total nephrectomy, percutaneous nephrolithotomy, long segment vertebral stabilization surgery, etc.); Group B surgeries (thyroidectomy, parathyroidectomy, retinal detachment, vitrectomy, partial nephrectomy, lumbar and cervical vertebra stabilization, tympanoplasty, rhinoplasty, total hip-knee surgery, meniscus arthroscopy, ureteroscopy, etc.) Groups C, D, and E surgeries are inguinal hernia, laparoscopic cholecystectomy, septoplasty, refractory surgery, D-J catheter insertion and removal, pilonidal sinus, anal fistulectomy, and hemorrhoidectomy, etc).22
Statistical Analysis
The power analysis was conducted after the study, as it was performed in patients who had surgery planned in the first 6 months. Accordingly, with 466 patients, a power of 99% and a significance level of 0.05 were determined using a two-tailed hypothesis test, and the effect size was set at 0.2.
Data were analyzed using the SPSS 21.0 (version 21.0, SPSS, Chicago, IL, USA) software package. Descriptive statistics (number, percentage, mean ± standard deviation, maximum, and minimum) were used for data analysis. The independent samples t-test was applied for pairwise comparisons within groups, the ANOVA test was used for multiple comparisons of variables with normal distribution, and the Kruskal–Wallis Test was used for variables without normal distribution. The Scheffe post hoc test was applied to determine the source of significant differences in the mean scores. Pearson’s correlation analysis was used to assess the relationships between the scales. Finally, the Shapiro–Wilk test was used to evaluate the normality of the data distribution. Statistical significance was set at p<0.05.
Results
In our study, 535 patients were evaluated over 6 months. Owing to incomplete data from 35 patients and 34 patients undergoing day surgery, 466 patients were included in the study. The mean age of the patients in the survey was 45.78±15.18 years, with 55.6% male and 71.8% married. It was determined that 37.3% of patients were primary school graduates, 71.9% were married, 19% were university graduates, and 51.7% were employed as workers. In addition, 51.7% of the patients had a low-income level, 83% resided in the city, and 87.1% lived with their families (Table 1).
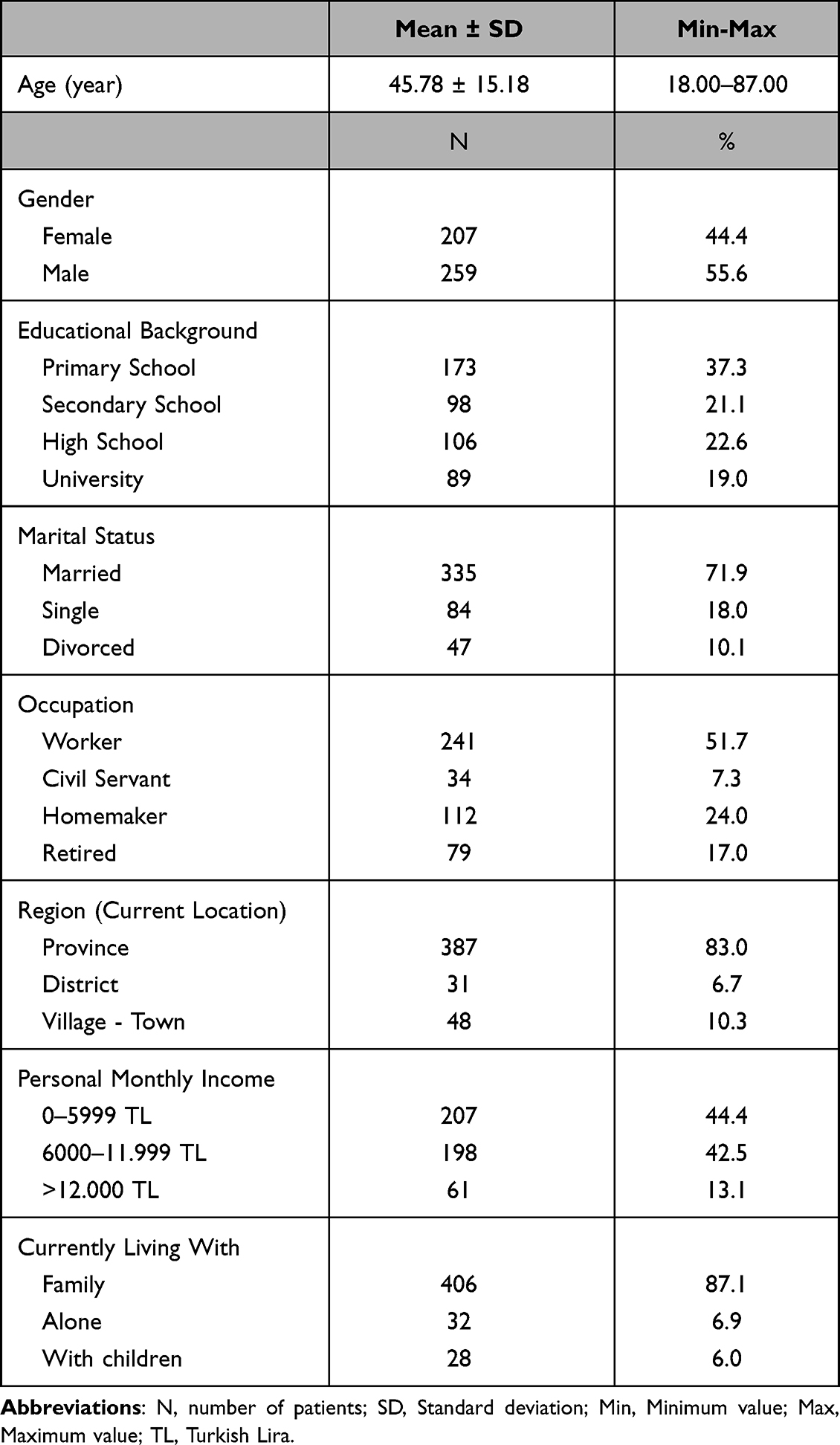 |
Table 1 Patient Distribution Based on Social-Demographic Characteristics |
It was found that 42.1% of the study group smoked, the mean body mass index (BMI) was 27.19±4.54 kg/m2, 75.5% of the patients had additional diseases, and 39.1% used medication regularly. Medications used included antihypertensive, antidiabetic, and antidepressant drugs. The study group comprised 16.1% of patients with hypertension, 45.3% with diabetes, and 6.5% with chronic diseases, such as coronary artery disease, heart failure, thyroid disorders, and Chronic Obstructive Pulmonary Disease. The proportion of patients who had previously undergone surgery was 70.2%, and 98.5% reported no problems related to anaesthesia in previous surgeries. Among the participants, 64.2% had ASA II, and when examined by surgery type and size, Group B surgeries were the most common (42.5%). The highest proportion of patients visiting the clinic were scheduled for general surgery (30.5%). The proportion of patients who received general anaesthesia was 58.2% (Table 2).
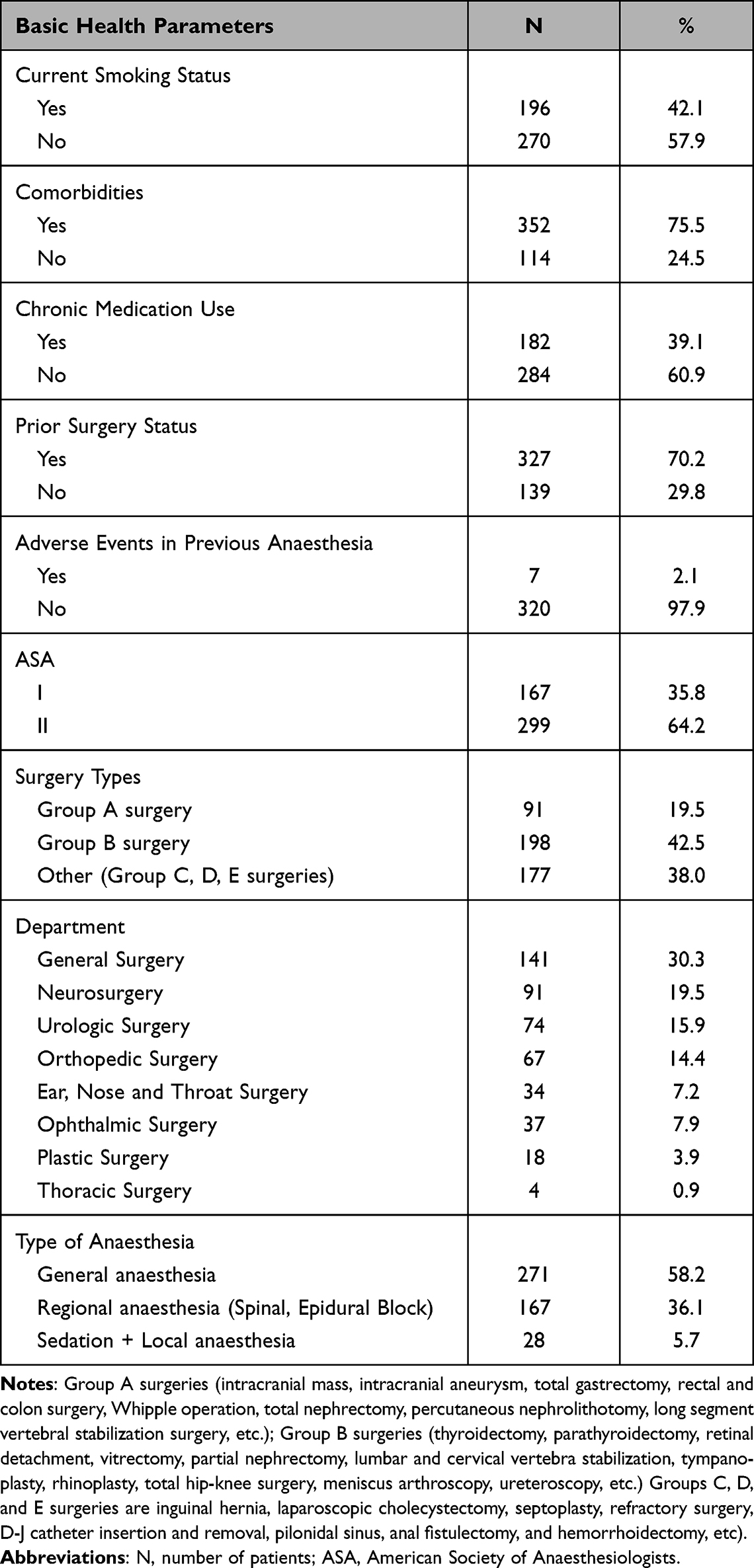 |
Table 2 Patient Distribution Based on Basic Health Parameters |
The mean HLS for the study group was determined as 105.89±24.42. The mean scores for the sub-dimensions were as follows: access to information:20.85±5.27; understanding information:29.24±7.34; evaluation:34.24±8.17; and application:21.55±5.39. The highest score was obtained from the evaluation sub-dimension, whereas the lowest was from the access to information sub-dimension. Participants’ HL levels were high (Table 3).
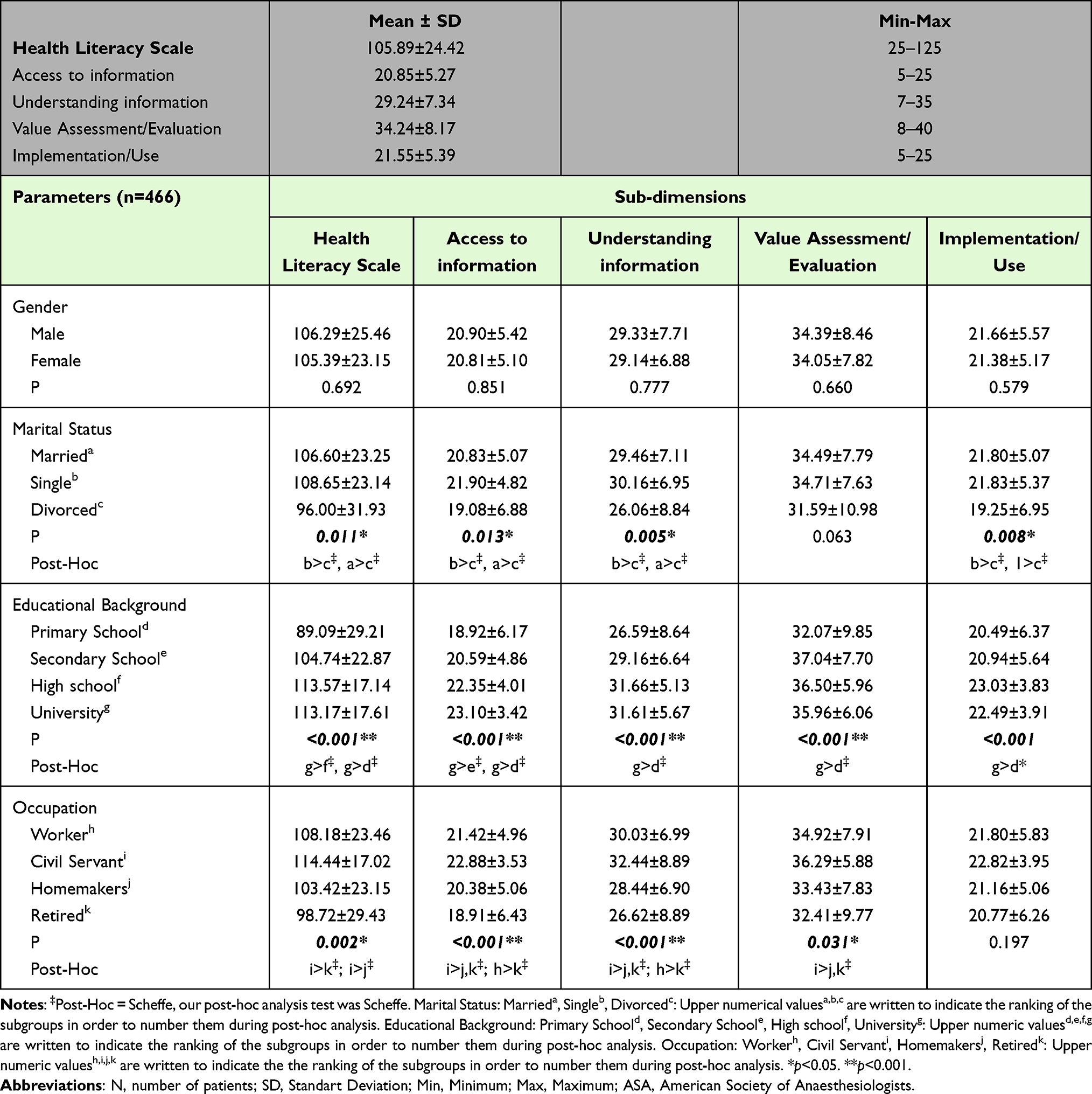 |
Table 3 A Comparative Analysis of Demographic Data, Basic Health Parameters, and the Health Literacy Scale |
When examining the distribution of the mean scores for the HLS and its sub-dimensions according to the demographic variables of the participants, no significant difference was found in the mean scores of the HLS and its sub-dimensions based on the participants’ gender (p>0.05) (Table 3).
When examining the HLS and its sub-dimensions of access to information, understanding information, and application based on the marital status of the participants, a statistically significant difference was found (p=0.013 and p<0.01, respectively), but no significant difference was observed in the evaluation sub-dimension (p>0.05). Single participants had higher mean scores than married and divorced participants (Table 3).
A highly statistically significant difference was found in the HLS and its sub-dimensions of access to information, understanding of information, evaluation, and application based on the participants’ education levels (p<0.001). Accordingly, the difference in the mean scores of the HLS and all sub-dimensions was higher for participants with a university education than those with a primary school education (Table 3). In addition, a statistically significant difference was found in the mean scores of the HLS evaluation sub-dimension based on participants’ occupations. A highly statistically significant difference was found in the mean scores of understanding information and access to information sub-dimensions. However, no significant difference was found in the application sub-dimension (p=0.031, p<0.001, and p>0.05, respectively) (Table 3).
No significant difference was found in the mean scores of the HLS and its sub-dimensions based on participants’ smoking status, ASA group, and the type and size of surgery they would undergo (p>0.05) (Table 3).
Our study’s mean BAI score was 9.28±10.85. The mean BAI score for the female participants was statistically significant (p<0.001). A statistically significant difference was found in the mean BAI scores among the different occupations (p<0.001), with homemakers having the highest mean BAI scores. A high level of statistical significance was found in BAI scores among those living in the city (p<0.01). Patient who live only with their children have low to moderate BAI levels (p=0.034). Patients who have comorbid disease also have low to moderate BAI levels (p=0.008). Finally, a statistically significant difference was found in BAI score averages among income levels (p=0.029), with lower-income individuals having higher BAI scores (Table 4).
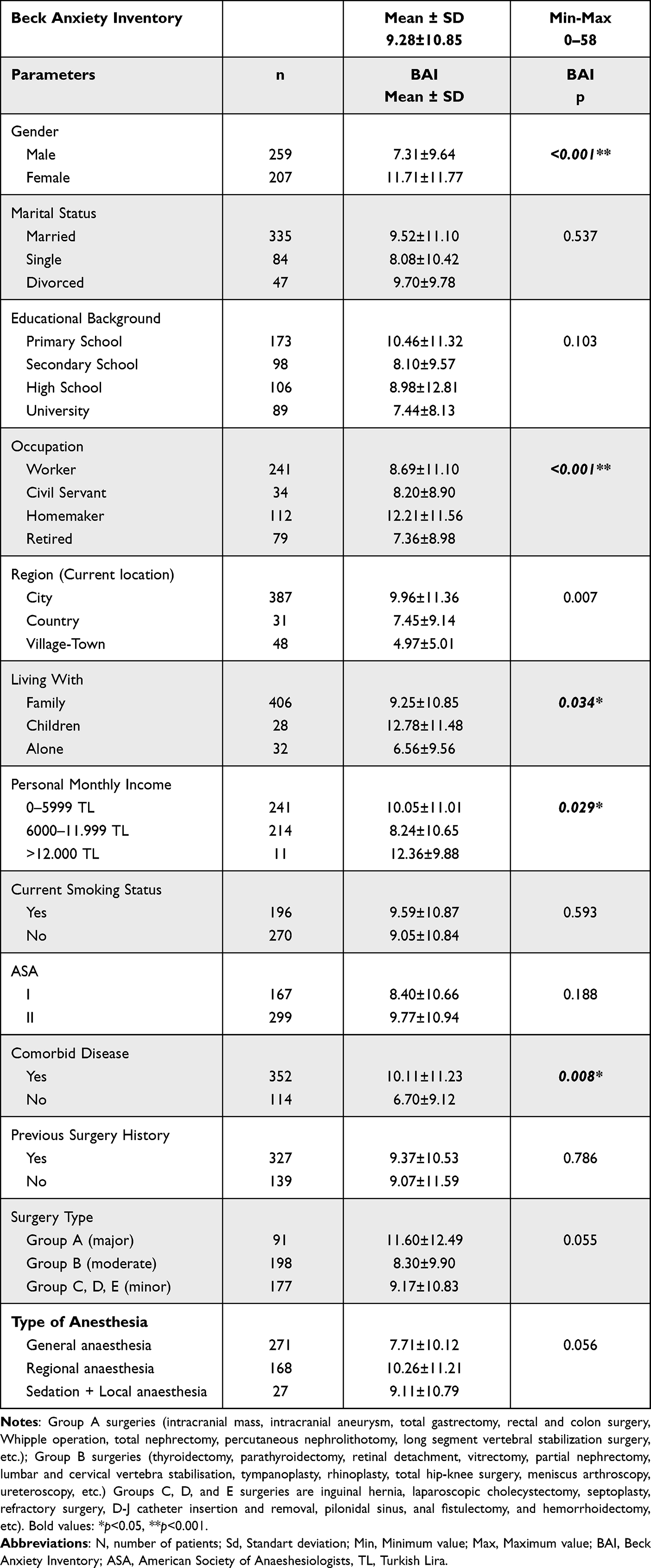 |
Table 4 Distribution of Beck Anxiety Inventory Scale Total Mean Scores According to Socio-Demographic Characteristics and Basic Health Variables (n=466) |
No significant differences were found between marital status, education level, ASA classification, history of previous surgery, type and size of the surgery to be performed, anaesthesia method used, and BAI scores (p>0.05) (Table 4).
The findings of the correlation analysis investigating the relationship between participants’ age, BMI, and mean scores obtained from the scales are presented in Table 5. Accordingly, a moderate positive relationship was found between participants’ age and BMI values (p<0.001, r=0.328); a low-level negative relationship was detected between age and HLS, access to information, understanding of information, and evaluation (n [p<0.001 (r=−0.188, r =−0.193, r =−0.205, r=−0.161]). A high-level negative relationship was found between the application levels (p=0.003, r=−1.133) (Table 5).
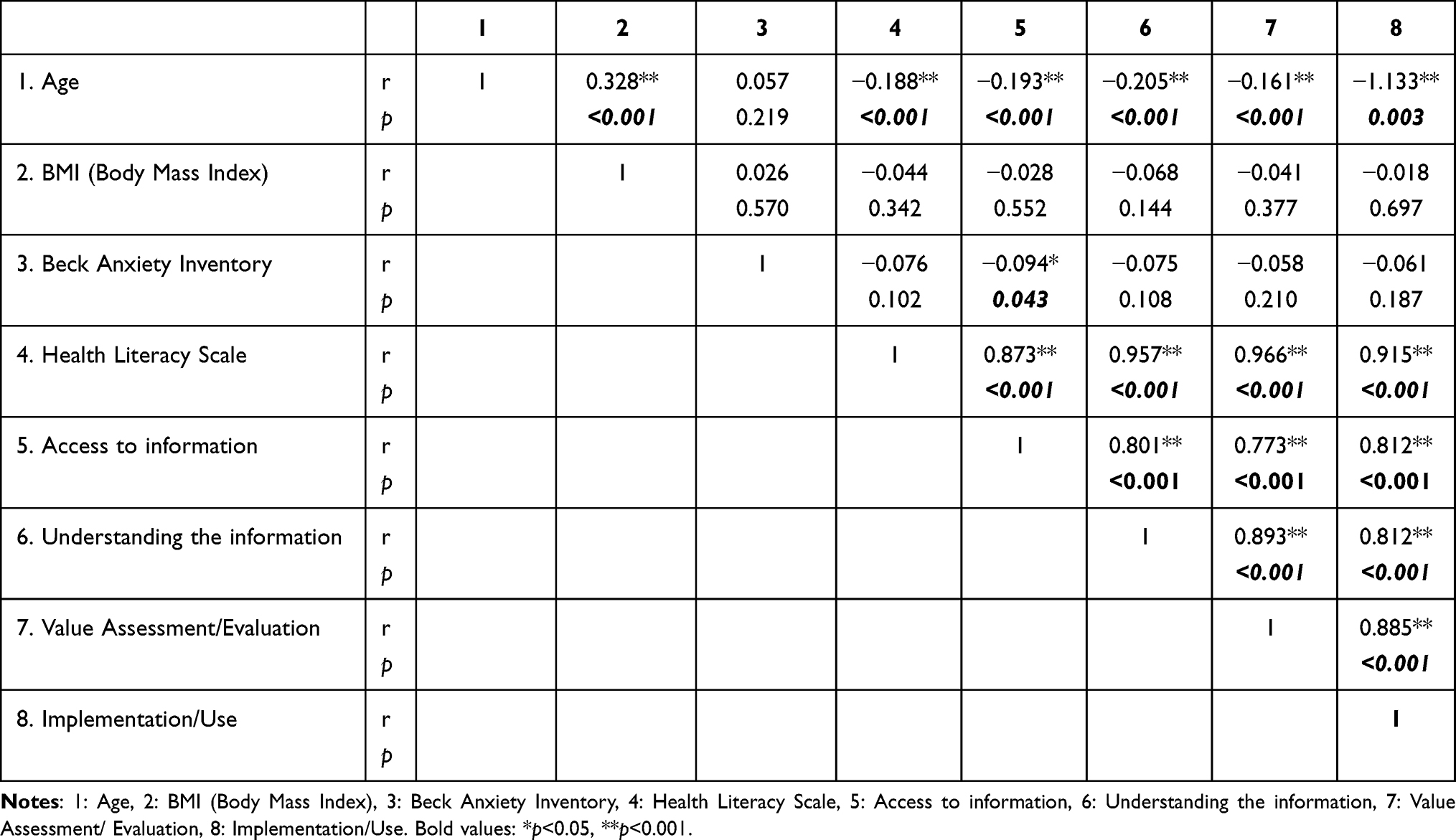 |
Table 5 Analysis of the Correlation Between Health Literacy Scale and Other Parameters |
A weak negative relationship was found between BAI score and the mean scores of the access to information sub-dimension (r=−0.094, p=0.043). In contrast, no significant association was found between the BAI score and the mean scores of the HLS and the understanding of information, evaluation, and application sub-dimensions (p>0.05) (Table 5). A statistically significant positive correlation was found among the HLS subdimensions (p<0.001) (Table 5).
Discussion
This study evaluated the relationship between HL and PA levels in patients undergoing surgery at a training hospital. We found high HL levels among the patients who participated in our study. Average anxiety levels, considered low-to-moderate, were observed for BAI. A negative relationship was found between access to information, a sub-dimension of the HLS, and PA. A negative relationship was detected between patient age and HLS and its sub-dimensions, whereas a positive relationship was found among HLS sub-dimensions. No correlation was found between the other subdimensions and PA. High mean scores for marital status, education level, and occupational groups were observed in the HLS and its sub-dimensions. It was determined that females, homemakers, those living in the province and with children only, and those with other diseases had higher PA rates.
Generally, being well-educated is a fundamental determinant of health. The accurate perception and application of health-related messages are essential for treating and preventing diseases. Individuals with higher education levels are more likely to participate in activities related to maintaining and improving their health. In a study by Çetin et al, the patient’s mean age was 50.03±11.42 years, and the total mean score of health HLS was high (100.82±15.62).11 In a study by Çimen and Bayık Temel, the total mean score of HLS in the elderly with chronic diseases was low (87.96±13.89).23 In another study, the HL levels of patients undergoing elective surgery were evaluated, and it was found that 37.3% of the participants had limited HL.24 In our study, the mean age of the participants was 45.78±15.18 years, and the total mean score of HLS was high (105.89±24.42). The younger age of our sample group, the majority being workers and civil servants, may have elevated HL levels due to health education in the workplace and mandatory participation in these educational activities. Another reason could be the increased use of television, the internet, social media, and other communication tools when people stay home to protect their health and maintain a healthy lifestyle after the COVID-19 pandemic. As HL is a perception, individuals’ perceptions and awareness can affect this situation. Furthermore, patients today prefer to play an active role in their treatment and care, and want to be involved in decisions related to their treatment. All these factors can be achieved at higher HL levels.12
Health Literacy is generally influenced by demographic, cultural, and psychosocial factors, overall literacy levels, individual characteristics, experiences related to the disease, and factors related to the healthcare system.19 The HL demographic factors included age, sex, marital status, income, education, and employment status. In general, HL is lower among older individuals, females, singles, and those with lower levels of education.25–27 It has been found in the literature that HL becomes insufficient as age increases.28 Similarly, in our study, it was found to be highly significant that HLS decreased with increasing age. The relationship between cognitive function loss and HL results in elderly individuals not benefiting from health services.29 In our study, no significant differences were found between HLS and sex, smoking status, ASA group, or type of surgery to be performed. Contrary to the literature, when examining marital status, singles were found to have significantly higher HLS and all sub-dimensions, except for value attribution.12
The general literacy level is also related to HL; however, a high literacy level does not necessarily mean high HL. Although research has found that individuals with low literacy levels have difficulty understanding health information, those with high literacy levels may have low HL.30 Regarding education level, our study found significance in the high HLS and all sub-dimensions among those who received high school and university education.
The BAI is considered the gold standard for measuring anxiety because it assesses short, simple, and general anxiety.31 Furthermore, BAI, which has an advantage in distinguishing anxiety that often overlaps with depression, includes patients’ feelings within the last week before surgery and their current feelings; its short duration of application is also advantageous.23 In recent years, it has been used in studies evaluating anxiety during the preoperative period.32
Continuing with the information provided, we often see in many studies that the STAI-I scale is frequently used in PA evaluations.33,34 However, there are limitations to the practical application of the STAI-I and STAI-II scales in the preoperative period, such as length and difficulty in understanding questions individually while answering.35 ROC analysis was performed in a study where a significant positive relationship was found between the STAI-I-STAI and STAI-II-STAI. When the threshold value for STAI-I was taken as 40, a value of 8.5 was predicted for BAI.36 In other words, a threshold value of 8.5, equivalent to the classification of moderate anxiety (BAI; 8–15) when measuring general anxiety, has become the threshold value for PA. Consistent with the literature, in our study, average anxiety levels considered low-medium were observed for the BAI and were in line with the literature.36,37
Different results were observed for sex and anxiety. In some studies, anxiety levels were higher in women during the preoperative period,34,38 while in others, PA levels were higher in men.39,40 Preclinical studies have shown that fluctuations in estrogen and progesterone levels play a role in the etiology of mood and anxiety disorders, which may explain the higher risk of anxiety in women.41 The results of our study showed that anxiety levels were higher in women. The higher anxiety level in women can be attributed to women being more comfortable expressing their emotions than men.
Although no significant relationship was found between educational level and BAI in our study, the lowest BAI rate was observed among those who received university education. This can be explained by better-educated individuals aware of the risks associated with surgery and anaesthesia. Another explanation could be that these individuals can better express themselves in anxiety scale questions directed to them. Our study found the highest anxiety value among those with low-income status. In a survey by Bahar et al, income status significantly affected the average anxiety score.42
Our study found no significant difference between the ASA classification and BAI. A few studies have found a substantial relationship between anaesthetic complications (eg, cardiac arrest, hypotension, and aspiration) and ASA classification however, a relationship between ASA status and PA has not been reported before.43
In line with the literature; we found individuals with additional diseases have been found to have increased PA.44 This may be because any postoperative complication that developed in patients undergoing surgery could be due to other diseases.
In contrast to the literature;45 we found that the type or size of surgery did not add extra stress to patients’ baseline anxiety states. Although the average BAI in group A surgeries was low-moderate (11.60±12.49), it was not statistically significant. This may be explained by the fact that the surgical departments provided sufficient and explanatory information to the patients about the surgeries they would undergo in our hospital.
In our study, we observed that hospitalization and the prospect of surgery did not increase the anxiety levels in this population. This may be attributed to strong family relationships or high anxiety levels regarding the country’s living standards.
Study Limitations
Our study has several limitations that should be considered when interpreting the results. First of all, as the study population was derived from a single center and did not include patients with high levels of preoperative anxiety, such as those undergoing cardiovascular surgery, caesarean section, etc., it may introduce a selection bias and limit the applicability of the results to other settings or populations. Second, the study’s cross-sectional design prevented us from establishing causal relationships between variables. A longitudinal study design might provide more insight into the temporal relationships between the factors examined and the development of PA. Self-report questionnaires could also contribute to response bias, particularly when measuring sensitive topics like anxiety levels. Furthermore, we did not consider the potential influence of healthcare professionals’ communication skills and patient-centered care on patients’ anxiety levels. Lastly, we did not evaluate the impact of PA on postoperative outcomes, such as pain, recovery time, and patient satisfaction. Therefore, future studies should investigate the relationship between PA and postoperative outcomes to better understand the clinical implications of addressing anxiety in surgical settings.
Despite these limitations, our study provides valuable insights into the factors associated with PA. These findings may help healthcare professionals to identify patients at risk of increased anxiety and to develop targeted interventions to reduce anxiety levels and potentially improve surgical outcomes.
Conclusion
The aim of this study was to evaluate the relationship between PA and HL. No correlation was found between HLS and BAI except access to health-related information. We suggest that improving patients’ access to health-related information may significantly reduce PA levels. When we searched the literature, we did not find any study examining the relationship between PA (measured with BAI) and HL. The lack of a publication similar to our study can be interpreted as a limitation and strength of the study.
There are different results in the literature regarding the relationship between PA levels and educational status, and no consensus has been reached. There is also no consensus between HL and education levels. In addition, even if individuals have similar levels of education, their reading, writing, comprehension and calculation skills may be different. Therefore, it is stated that HL level, not education level, should be taken into consideration when evaluating individuals in health-related issues.46 The effect of educational level on PA may actually be due to the effect of educational status on HL. The most important reason for this idea is that the relationship between educational level and PA is found in very different ranges in the literature. Perhaps, if the HL level of the patients in these studies could have been evaluated, a clearer relationship with PA could have been shown. In the light of all this information, it was considered appropriate to assess HL rather than educational status when evaluating PA levels, but more studies examining the relationship between HL, educational level and PA are needed.
In addition, we think that in the near future, the level of HL of patients in the preoperative period can be evaluated and PA levels can be reduced by increasing HL regardless of educational level with appropriate trainings.
Understanding the risk factors associated with PA can help healthcare professionals plan targeted interventions to ensure a safer and less stressful surgical experience for patients. Future research should focus on assessing the impact of PA on postoperative outcomes such as pain, recovery time and patient satisfaction.
Ethics Approval and Consent to Participate
The study was reviewed and approved by the Health Sciences University Bursa Yuksek Ihtisas Training and Research Hospital Ethics Committee with the ethical no - (2011-KAEK-25 2021/12-17) and written informed consent was obtained from participants. This study was conducted in accordance with the Declaration of Helsinki.
Acknowledgments
We wish to thank all the patients who participated in the study.
Disclosure
The authors report no financial and nonfinancial competing interests in relation to this work.
References
1. Shives LR. Basic Concepts of Psychiatric-Mental Health Nursing. Lippincott Williams & Wilkins; 2008.
2. Kassahun WT, Mehdorn M, Wagner TC, et al. The effect of preoperative patient-reported anxiety on morbidity and mortality outcomes in patients undergoing major general surgery. Sci Rep. 2022;12:6312. doi:10.1038/s41598-022-10302-z
3. Abate SM, Chekol YA, Basu B. Global prevalence and determinants of preoperative anxiety among surgical patients: a systematic review and meta-analysis. Int J Surg Open. 2020;25:6–16. doi:10.1016/j.ijso.2020.05.010
4. Sigdel S. Perioperative anxiety: a short review. Glob Anesth Perioper Med. 2015;1(4):107–108. doi:10.15761/GAPM.1000126
5. Caumo W, Schmidt AP, Schneider CN, et al. Risk factors for postoperative anxiety in adults. Anaesthesia. 2001;56(8):720–728. doi:10.1046/j.1365-2044.2001.01842.x
6. Jlala HA, French JL, Foxall GL, et al. Effect of preoperative multimedia information on perioperative anxiety in patients undergoing procedures under regional anaesthesia. Br J Anaesth. 2010;104(3):369–374. doi:10.1093/bja/aeq002
7. Maranets I, Kain ZN. Preoperative anxiety and intraoperative anesthetic requirements. Anesth Analg. 1999;89(6):1346–1351. doi:10.1097/00000539-199912000-00003
8. Maheshwari D, Ismail S. Preoperative anxiety in patients selecting either general or regional anesthesia for elective cesarean section. J Anaesthesiol Clin Pharmacol. 2015;31:196–200. doi:10.4103/0970-9185.155148
9. Ayyadhah Alanazi A. Reducing anxiety in preoperative patients: a systematic review. Br J Nurs. 2014;23(7):387–393. doi:10.12968/bjon.2014.23.7.387
10. Chang ME, Baker SJ, Dos Santos Marques IC, et al. Health literacy in surgery. Health Lit Res Pract. 2020;4(1):e46–e65. doi:10.3928/24748307-20191121-01
11. Çetin F, Yılmaz E. The effect of Health Literacy Levels of Patients in Surgical Clinic on Health Perception and Surgical Fear. Izmır Katip Celebi University Health Sciences University Journal. 2022;7(1):61–67.
12. Balçık YP, Taşkaya S, Şahin B. Health literacy. TAF Prev Med Bull. 2014;13(4):321–326.
13. Altun Şahin Ö, Özlü Karaman Z, Olçun Z, et al. Does the fear ofsurgery prevent patients from sleeping? Anadolu Hemsirelik ve Saglik Bilimleri Dergisi. 2017;20(4):260–266.
14. Stamenkovic DM, Rancic NK, Latas MB, et al. Preoperative anxiety and implications on postoperative recovery: what can we do to change our history. Minerva Anestesiol. 2018;84:1307–1317. doi:10.23736/S0375-9393.18.12520-X
15. Lemos MF, Lemos-Neto SV, Barrucand L, et al. Preoperative education reduces preoperative anxiety in cancer patients undergoing surgery: usefulness of the self-reported Beck anxiety inventory. Rev Bras Anestesiol. 2019;69:1–6. doi:10.1016/j.bjan.2018.07.003
16. Arık E, Dolgun H. The effect of Sociodemographic Parameters on Anxiety in Patients Who are Planned Surger Under General Anesthesia. Anestezi Derg. 2019;27 (1) :22–29 doi:10.5222/jarss.2019.35229.
17. Toci E, Burazeri G, Jerliu N, et al. Health literacy, self-perceived health and self-reported chronic morbidity among older people in Kosovo. Health Promot Int. 2015;30(3):667–674. doi:10.1093/heapro/dau009
18. Aras Z, Bayık Temel A. Evaluation of Validity and Reability of the Turkish Version of Health Literacy Scale.Florence Nightingale Journal of Nursing. 2017;25(2):85–94.
19. Sorenson K, Van den Broucke S, Fullam J, et al. Health literacy and public health: a systematic review and integration of definitions and models. BMC Public Health. 2012;12:80. doi:10.1186/1471-2458-12-80
20. Beck AT, Epstein N, Brown G et al. An inventory for measuring clinical anxiety: phychometric properties. J Consult Clin Psychol. 1988;56:893–897 doi:10.1037/0022-006x.56.6.893.
21. Ulusoy, M, Şahin, N, Erkmen, H Turkish version of the Beck anxiety inventory: psychometric properties J Cogn Psychother. 1998; 12: 28–35
22. Avaible from: http://www.resmigazete.gov.tr/eskiler/2018/02/20180204-11.htm
23. Çimen Z, Bayık Temel A, et al. Investigation of Health Literacy,Perception of Health and Related Factors in Eldery Patients with Chronic Illness. Journal of Ege University Nursing Faculty. 2017;33(3):105–125.
24. Koster E, Schmidt A, Philbert D et al, et al. Health literacy of patients admitted for elective surgery. Z Gesund Wiss. 2017;25(2):181–186. doi:10.1007/s10389-016-0774-z
25. Paasche-Orlow MK, Parker RM, Gazmararian JA, et al. The prevalence of limited health literacy. J Gen Intern Med. 2005;20:175–184. doi:10.1111/j.1525-1497.2005.40245.x
26. Cho YI, Lee SYD, Arozullah AM, et al. Effects of health literacy on health status and health service utilization amongst the elderly. Soc Sci Med. 2008;66:1809–1816. doi:10.1016/j.socscimed.2008.01.003
27. Morris NS, MacLean CD, Littenberg B. Change in health literacy over 2 years in older adults with diabetes. Diabetes Educ. 2013;39(5):638–646. doi:10.1177/0145721713496871
28. Bozkurt H, Demirci H. Health literacy among older persons in Turkey. Aging Male. 2019;22(4):272–277. doi:10.1080/13685538.2018.1437901
29. Goh VH, Hart WG. Association of general and abdominal obesity with age, endocrine and metabolic factors in Asian men. Aging Male. 2016;19:27–33. doi:10.3109/13685538.2015.1088825
30. Australian Commission on Safety and Quality in Health Care. Consumers, the system and health literacy: taking action to improve safety and quality. Consultation Paper. Sydney. 2013.
31. Muntingh AD, van der Feltz-Cornelis CM, van Marwijk HW, et al. Is the beck anxiety inventory a good tool to assess the severity of anxiety? A primary care study in the Netherlands Study of Depression and Anxiety (NESDA). BMC Fam Pract. 2011;12:66. doi:10.1186/1471-2296-12-66
32. Uysal Aİ, Altıparmak B, Korkmaz Toker M, et al. The effect of preoperative anxiety level on mean platelet volume and propofol consumption. BMC Anesthesiol. 2020;20:34. doi:10.1186/s12871-020-0955-8
33. Arlı ŞK. Evaluation of teh Preoperative Anxiety with APAIS and STAI-I Scales. Hacettepe Üniversitesi Hemsirelik Fakültesi Dergisi. 2017;4 (3) :38–47.
34. Aykent R, Kocamanoğlu S, Üstün E, et al. Preoperative Causes and Assessment of Anxiety: Comparison of APAIS and STAI Scores. Türkiye Klinikleri J Anest Reanim. 2007;5:7–13.
35. Facco E, Stellini E, Bacci C, et al. Validation of visual analogue scale for anxiety (VAS-A) in preanesthesia evaluation. Minerva Anestesiol. 2013;79(12):1389–1395.
36. Peker K. Comparison of Beck and Stait Trait Anxiety Scales in the Evaluation of Preoperative Anxiety. JARSS. 2020;28(2):109–115.
37. Demirhan A, Velioglu Y, Yoldas H, et al. An easy and reliable way to prevent electrocardiographic deteriorations of patients undergoing off-pump coronary artery bypass surgery: preoperative anxiolytic treatment. Braz J Cardiovasc Surg. 2019;34(3):311–317. doi:10.21470/1678-9741-2018-0282
38. Demir A, Akyurt D, Ergün B, et al. Anxiety therapy in cardiac surgery patients. Türk Gögüs Kalp Damar Cerrahisi Dergisi. 2010;18 (3) :177–182.
39. Jafar MF, Khan FA. Frequency of preoperative anxiety in Pakistani surgical patients. J Pak Med Assoc. 2009;59(6):359–363.
40. Arslan S, Taylan S, Deniz S. Preoperative anxiety levels of neurosurgical patients. J Anatolia Nurs Health Sci. 2017;20 (1) :17–21.
41. Weinstock LS. Gender differences in the presentation and management of social anxiety disorder. J Clin Psychiatry. 1999;60:9–13.
42. Bahar A, Sertbaş G, Sönmez A. Determination of depression and anxiety levels of patients with diabetes mellitus. Anadolu Psikiyatri Derg. 2006;7:18–26.
43. Wolters U, Wolf T, Stützer H, et al. ASA classification and perioperative variables as predictors of postoperative outcome. Br J Anaesth. 1996;77(2):217–222. doi:10.1093/bja/77.2.217
44. Forlani M, Morri M, Belvederi Murri M, et al. Anxiety symptoms in 74+ community-dwelling elderly: associations with physical morbidity, depression and alcohol consumption. PLoS One. 2014;9:e89859. doi:10.1371/journal.pone.0089859
45. Erkilic E, Kesimci E, Soykut C, et al. Factors associated with preoperative anxiety levels of Turkish surgical patients: from a single center in Ankara. Patient Prefer Adherence. 2017;11:291–296. doi:10.2147/PPA.S127342
46. Berkman ND, Davis TC, McCormack L. Health literacy: what is it? J Health Commun. 2010;15(2):9–19. doi:10.1080/10810730.2010.499985
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.