Back to Journals » Drug Design, Development and Therapy » Volume 20
The Effect of Esketamine on Peripheral Vascular Resistance in Elderly Patients During Anesthesia Induction: A Single-Center, Double-Blind, Prospective, Randomized Controlled Study
Authors Li J, Gao Y, Jing K, Lu H, Cao Y, Chen X, Wang H, Song X, Gan G, Tan S
Received 8 March 2026
Accepted for publication 24 June 2026
Published 16 July 2026 Volume 2026:20 607757
DOI https://doi.org/10.2147/DDDT.S607757
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Jingjing Li,1,* Yu Gao,2,* Kailun Jing,1,* Hanjie Lu,2 Yunlong Cao,1 Xiaolong Chen,2 Hong Wang,2 Xiaoyang Song,2 Guosheng Gan,1,2 Shigang Tan2
1Department of Anesthesiology, Graduate Joint Training Base of General Hospital of Central Theater Command of the People’s Liberation Army, School of Medicine, Wuhan University of Science and Technology, Wuhan, Hubei, People’s Republic of China; 2Department of Anesthesiology,General Hospital of Central Theater Command of the People’s Liberation Army, Wuhan, Hubei, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Guosheng Gan, Department of Anesthesiology, General Hospital of the Central Theater Command of the Chinese People’s Liberation Army, Wuchang District, Wuhan, Hubei, People’s Republic of China, Email [email protected]; [email protected] Shigang Tan, Email [email protected]
Purpose: To investigate the effect of esketamine on peripheral vascular resistance in elderly patients during anesthesia induction.
Patients and Methods: Eighty elderly patients undergoing elective surgery were randomly assigned to two groups (n=40 each): the esketamine group (Group A) received esketamine 0.3 mg/kg, while the control group (Group B) received an equal volume of normal saline. Both groups received the same standard anesthesia induction (etomidate, sufentanil, rocuronium). Hemodynamic parameters (SBP, DBP, MAP, HR) and peripheral vascular resistance assessed by the snuffbox radial artery resistance index (SBRI) were recorded at seven time points: before induction (T1), 1 min (T2) and 5 min (T3) after induction, during intubation (T4), and 1 min (T5), 5 min (T6), and 10 min (T7) after intubation. Adverse events during induction and postoperative recovery were also documented. This double-blind study masked drug administration and outcome assessment.
Results: No significant baseline differences existed between groups (P> 0.05). MAP in Group A was significantly higher than in Group B at T2–T7 (P< 0.05). SBRI in Group A was significantly higher than in Group B at T2 and T3 (P< 0.05), but not at T4–T7. Group A had lower incidences of hypotension (14.3% vs 56.4%), muscle tremor (8.6% vs 33.3%), and vasoactive drug use (5.7% vs 38.5%) (all P< 0.05). No significant differences were observed in other adverse events or postoperative recovery scores. Postoperative VAS pain score was slightly lower in Group A (P< 0.05).
Conclusion: Esketamine used during anesthesia induction shows promise in mitigating early-phase blood pressure decline, increasing peripheral vascular resistance (T2–T3), maintaining hemodynamic stability, and reducing hypotension, muscle tremor, and vasoactive drug use in elderly patients, without compromising recovery.
Keywords: esketamine, elderly patients, anesthesia induction, peripheral vascular resistance, snuffbox radial artery resistance index
Introduction
With the intensification of social aging, the number of elderly patients undergoing surgery and anesthesia is increasing. Circulatory fluctuations are prone to occur during the anesthesia induction period, which affects the safety and prognosis of patients during the peri-operative period.1 Elderly patients often exhibit preserved systolic function but reduced diastolic compliance, along with age-related decreases in baroreflex sensitivity and autonomic regulation. These changes make them more susceptible to abrupt decreases in peripheral vascular resistance during anesthesia induction compared to younger patients. Therefore, it is particularly important to maintain stable peripheral circulatory resistance.2,3
Currently, research on preventing blood pressure fluctuations during the induction period of general anesthesia mainly focuses on drug intervention.4 Selecting anesthetic drugs that have less impact on the cardiovascular system, such as etomidate,5 sufentanil, remifentanil, etc, can effectively inhibit the stress response to tracheal intubation. However, studies have found that the current measures also have some drawbacks, such as severe hemodynamic fluctuations, increased risk of arrhythmia, abnormal tissue perfusion, drug accumulation and adverse reactions.
Esketamine, a novel anesthetic agent, is the dextrorotatory enantiomer of ketamine. It retains many of ketamine’s pharmacological properties, such as potent analgesic and sedative effects.6–8 Additionally, it possesses sympathomimetic activity, which can stimulate the sympathetic nervous system9 and promote the release of catecholamines in the body.This characteristic distinguishes its impact on the cardiovascular system from other anesthetics and is closely related to changes in peripheral vascular resistance.10
With the development of ultrasound technology,11 the monitoring of hemodynamic indicators related to large and small blood vessels has become more non-invasive. The resistance index is a quantitative indicator commonly used clinically to reflect the magnitude of vascular resistance, indirectly indicating peripheral vascular status and microcirculatory state.12,13 In recent years, the snuffbox radial artery resistance index (SBRI) has gained increasing attention from clinicians. A study on the relationship between Doppler SBRI and tissue perfusion showed a high correlation between SBRI and tissue perfusion, suggesting its utility for assessing peripheral vascular disorders and reflecting peripheral tissue perfusion more accurately than overall hemodynamic status. SBRI has been proven to be a feasible and accurate parameter for evaluating vascular resistance and compliance.14
Currently, esketamine is used for induction of general anesthesia, and its clinical application is receiving widespread attention.15,16 This study primarily utilizes ultrasound technology to observe changes in the snuffbox radial artery resistance index, exploring its application in anesthesia induction for elderly patients and its effect on peripheral vascular resistance, to better guide clinical practice and ensure anesthesia safety for elderly patients.
Although studies on the hemodynamic effects of esketamine in different populations have been reported, there are still limited studies specifically focusing on the impact on peripheral vascular resistance during anesthesia induction in elderly patients. In addition, previous studies have not used the snuff - box brachial resistance index (SBRI) as a direct and non - invasive indicator to evaluate peripheral vascular resistance. Therefore, this study aims to fill this gap by using SBRI and systematically evaluate the effects of esketamine on peripheral vascular resistance and hemodynamic stability in elderly patients.
Materials and Methods
General Information
This study was reported in accordance with the CONSORT guidelines, and a complete checklist is provided. Eighty elderly patients scheduled for tracheal intubation general anesthesia at the CHCT between December 2024 and December 2025 were selected as study subjects. Inclusion criteria: (1) Age ≥ 60 years; (2) Planned elective surgery under general anesthesia; (3) ASA physical status classification17 I–III; (4) NYHA functional class I; (5) Negative Allen’s test; (6) No contraindications to the study drugs; (7) Signed informed consent. Exclusion criteria: (1) Severe cardiovascular diseases (eg:acute heart failure, myocardial infarction); (2) Patients at high risk for increased blood pressure, intraocular pressure, pulmonary artery pressure, or intracranial pressure; (3) Neurological diseases (eg: preeclampsia, eclampsia) or history of severe mental disorders; (4) Peripheral vascular disease due to underlying conditions (eg: hyperlipidemia); (5) History of hepatic or renal dysfunction; (6) Allergy to the study drugs; (7) Participation in other clinical trials within the last 3 months This study was approved by the Medical Ethics Committee of the CHCT All patients and their families voluntarily signed informed consent forms In addition to ethical approval, all methods in the study were performed in accordance with the relevant guidelines and regulations, including the Declaration of Helsinki.
Specific Process
The selected research subjects were randomly divided into the observation group (Group A) received esketamine and the control group (Group B) received non-esketamine, with 40 cases in each group, according to the random number table method. Preoperatively, patients fasted for solid food and withheld fluids for 2–4 hours. Upon entering the operating room and after three-party verification, they were placed in the supine position, and a peripheral intravenous line was established. Sodium acetate Ringer’s injection was infused at a rate of 500 mL/h. Vital signs monitoring was established, including ECG, NIBP, and SpO2. Under ultrasound guidance, the pulse Doppler function of the ultrasound device was used to obtain the radial artery lumen blood flow spectrum, and the SBRI was calculated [(PSV - EDV)/PSV].
Anesthesia Induction
An anesthesiologist who is unaware of the grouping of this trial is responsible for administering the drugs. Set the ventilator parameters, adjust the induction position with the head higher than the feet, administer oxygen through a mask at a flow rate of 4–5 L/min. After pre - oxygenation, in the Group A, slowly intravenously inject 0.3 mg/kg of esketamine (administered within 1 min after the start of induction), 0.3 mg/kg of etomidate, 0.5 μg/kg of sufentanil, and 0.9 mg/kg of rocuronium bromide (administered within 5 min after the start of induction) for anesthesia induction. Group B followed the same procedure, replacing esketamine with an equivalent volume of normal saline. After successful induction in both groups, tracheal intubation was performed under video laryngoscopy. After confirming clear and equal bilateral breath sounds and good ventilation without air leak, the patient was connected to the anesthesia machine for mechanical ventilation. Settings included: FiO2 60%, oxygen flow 2 L/min, tidal volume 6–8 mL/kg, respiratory rate 10–14 breaths/min, I:E ratio 1:2, maintaining end-tidal CO2 between 35–45 mmHg. No surgical maneuvers were performed within 10 minutes of induction. Changes in peripheral vascular resistance and hemodynamic parameters were monitored in both groups at the following time points: before induction (T1), 1 min after induction (T2), 5 min after induction (T3), during tracheal intubation (T4), 1 min after intubation (T5), 5 min after intubation (T6), and 10 min after intubation (T7).
Anesthesia Maintenance
Patients in both groups received intravenous infusion of propofol 3–5 mg/(kg·h) and remifentanil 0.3 μg/(kg·min) to maintain blood pressure fluctuations within ±20% of baseline. Management of blood pressure changes during induction: When blood pressure decreased by 20% - 30% from baseline, methoxamine 0.5–1 mg/dose or ephedrine 5–10 mg/dose was administered intravenously. Drug choice and dose adjustments were based on blood pressure recovery and heart rate changes. When blood pressure increased by 20% - 30% above baseline, urapidil was typically used, with an initial dose of 12.5–25 mg intravenously, and subsequent doses decided based on the degree of blood pressure reduction.
Observation Indicators
- Record patient basic information, including gender, age, ASA classification, NYHA functional class, baseline MAP, HR, and SBRI upon entering the operating room (T1).
- Compare hemodynamic indicators between groups at T2, T3, T4, T5, T6, T7: SBP, DBP, MAP, HR and SpO2 were measured using a patient monitor.
- Compare peripheral vascular resistance indicators between groups at T2, T3, T4, T5, T6, T7: SBRI was primarily measured via ultrasound examination. During examination, an appropriate amount of ultrasound gel was applied to the snuffbox area of the wrist. The ultrasound probe was placed at this location with the marker point facing the medial side of the thenar eminence. In color Doppler mode, the blue blood flow indicated the snuffbox radial artery. The pulse Doppler mode of the ultrasound device was activated, with the sample gate positioned at a depth of 1 cm in the sagittal plane of the radial artery, to obtain PSV and EDV. SBRI was calculated using the formula: SBRI = (PSV - EDV) / PSV, yielding the SBRI.
- Compare the effects of different drugs and maneuvers on peripheral vascular resistance and hemodynamics at different time points.
- Compare the incidence of adverse reactions between the two groups: Record occurrences of hypertension, hypotension, tachycardia, bradycardia, etc., during anesthesia induction. Incidence = (number of adverse reaction cases / total number of cases) × 100%.
- Record the occurrence of postoperative adverse reactions, postoperative recovery scores, and VAS pain scores.
Statistical Processing
Data analysis was performed using SPSS and PASS statistical software. Intention-to-treat analysis was adopted. All patients were randomly included in the analysis. Measurement data were expressed as mean ± standard deviation. Independent sample t-test was used for comparison between groups, paired t-test was used for comparison within groups, and repeated measures analysis of variance was used for comparison of indicators at multiple time points. Count data were expressed as rates (%), and chi-square test was used for comparison. A difference was considered statistically significant when P < 0.05.
Based on the standard deviation (SD=0.113) of hemodynamic and resistance index parameters reported in relevant literature,18 with a two-sided significance level (α) of 0.05 and power (1-β) of 0.8, 32 patients were required per group. Considering a possible dropout rate (eg, 20%), 40 patients per group were needed. This study selected 80 patients. Six patients were excluded due to intervention interruption (ultrasound measurement position deviation). Therefore, the final statistical analysis included 35 patients in the Group A and 39 in the Group B (Figure 1). Furthermore, recalculated based on the actual SD = 0.075 of SBRI at T1 in this study, 28 cases are required for each group.The actual effective sample size in this study meets the statistical power requirements.
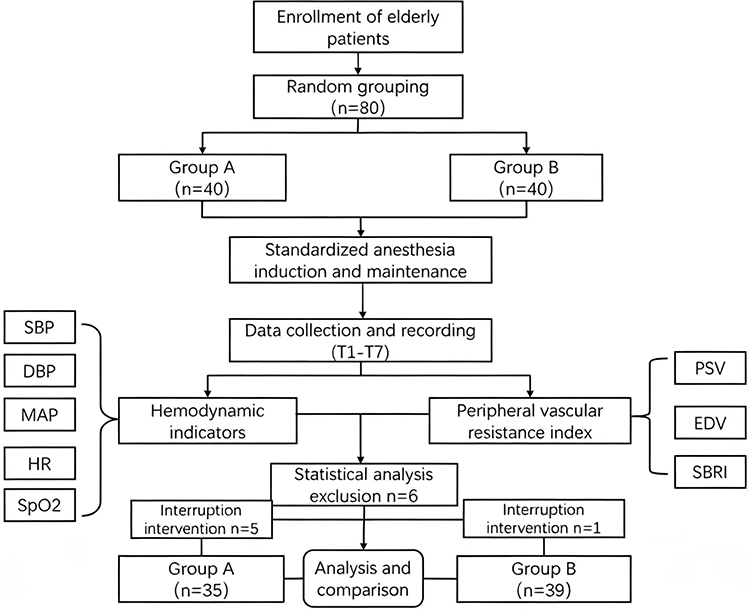 |
Figure 1 Technical roadmap. |
Results
Comparison of General Information Between Groups
There were no statistically significant differences (P > 0.05) in general information such as age, gender, height, and weight between the two groups, indicating comparability (Table 1).
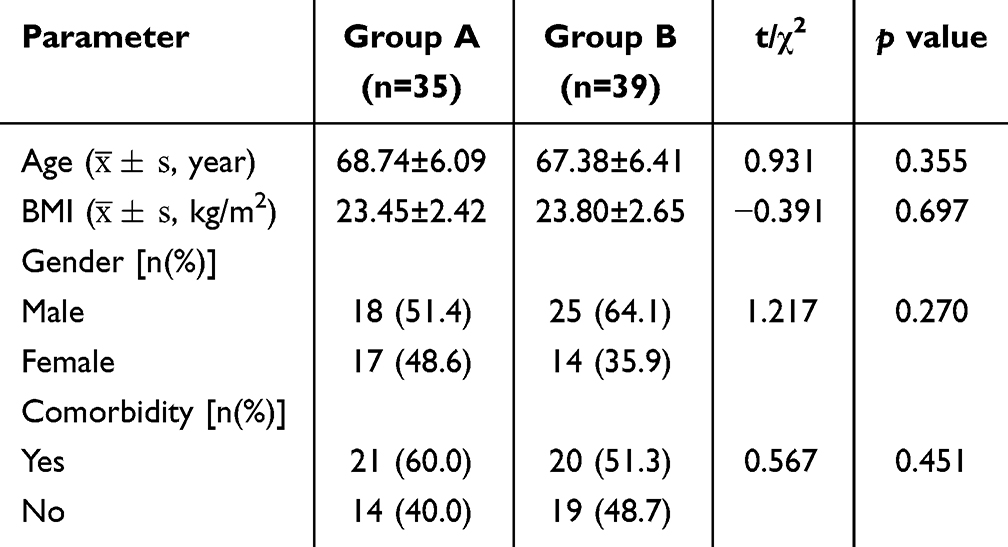 |
Table 1 Comparison of General Information Between Groups |
Comparison of Hemodynamic Indicators
Inter-group comparisons showed no statistically significant differences in MAP and HR at the T1 time point (P > 0.05). Comparison of MAP between the two groups at time points T2 - T7 showed that all P - values were < 0.05, indicating statistically significant differences. Among them, the overall MAP of the Group A was higher than that of the Group B (Figure 2A). Comparisons of HR between groups showed statistically significant differences at time points T4, T5, and T7 (P < 0.05), and the mean value of the Group A was higher than that of the Group B. Blood pressure decreased at T3 in both groups and increased at T4 due to tracheal intubation stimulus in both groups (Table 2).
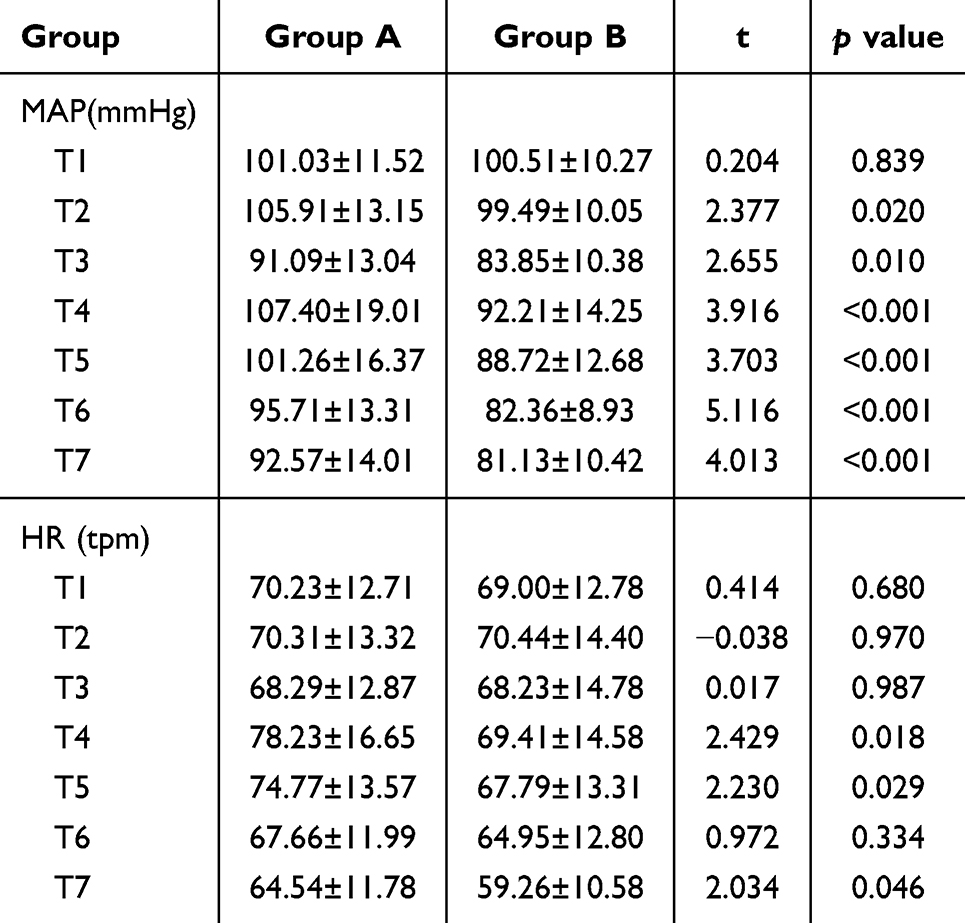 |
Table 2 Comparison of Hemodynamics Between Groups |
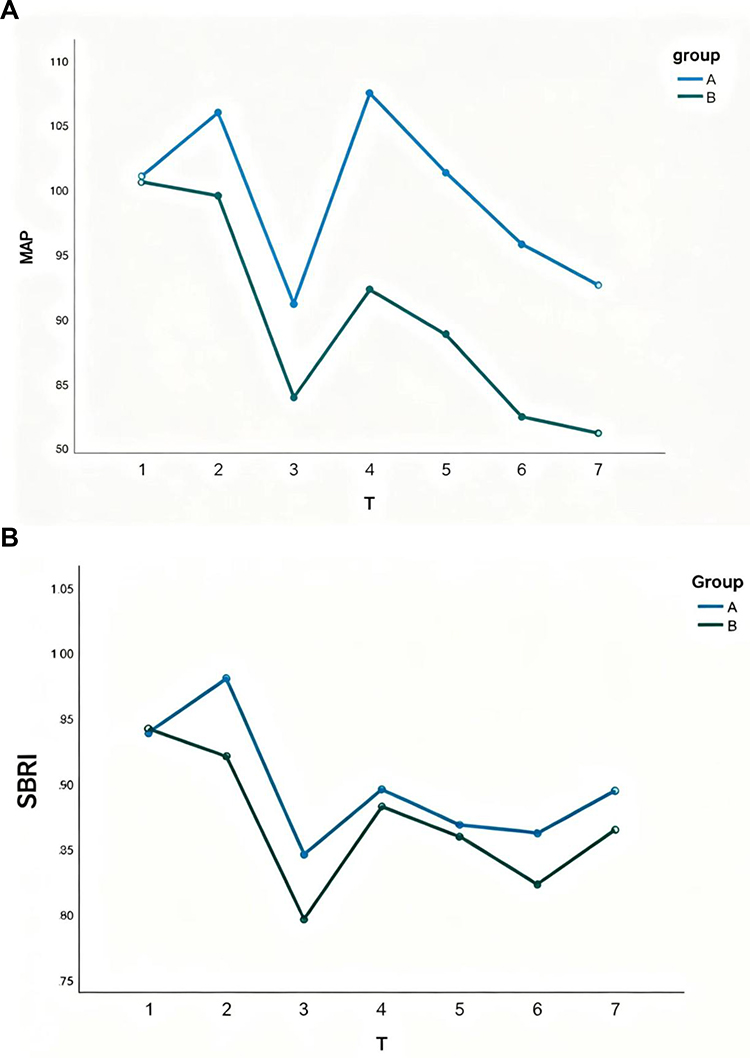 |
Figure 2 Trends of MAP and SBRI changes in two groups ((A) Changes in MAP Between Groups at Different Times; (B) Changes in SBRI Between Groups at Different Times). |
Comparison of Peripheral Vascular Resistance Index
Linear regression model analysis showed that the main effect of group was not statistically significant (F=2.167, P=0.145), indicating that group assignment did not significantly affect SBRI. However, SBRI at different time points (T1~T7) was highly statistically significant (F=17.533, P < 0.001). The interaction effect between group and time point was not statistically significant (F=1.022, P=0.382). SBRI in the Group A at 1 minute post-induction (T2) was higher than the preoperative baseline (P < 0.05) (Figure 2B) and higher than SBRI in the Group B at T2 (Figure 3).The Group B showed no significant change in SBRI between T2 and T1 (Figure 4). SBRI in both groups decreased significantly at 5 minutes post-induction (T3) compared to T2 (P < 0.05), with SBRI in the Group A still higher than the Group B at T3. At time points T4-T7, there were no statistically significant differences in SBRI between the two groups (P > 0.05) (Table 3).
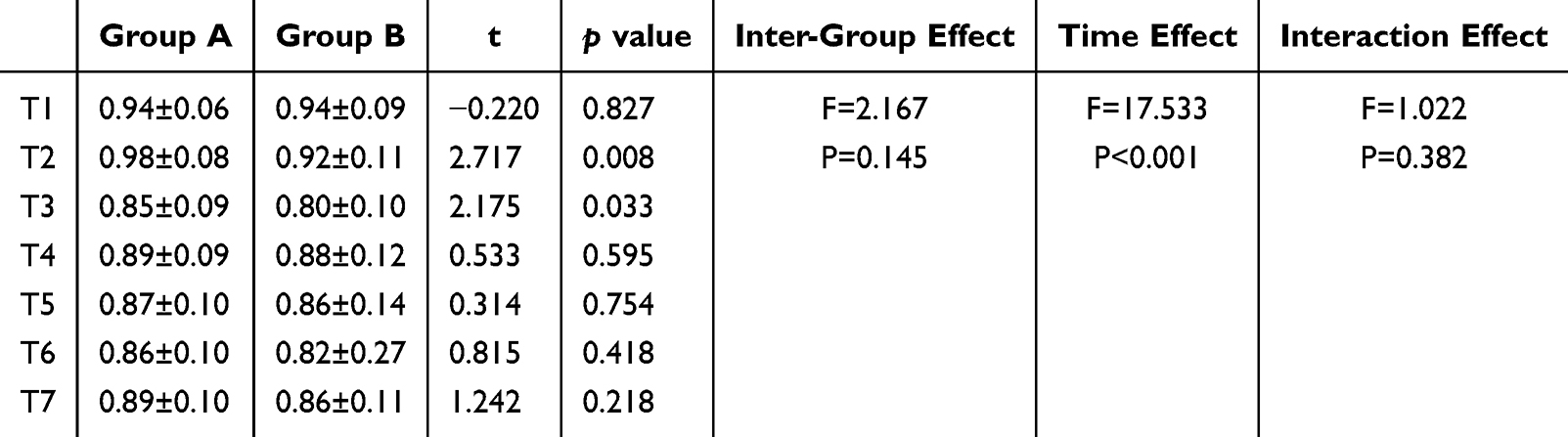 |
Table 3 Comparison of Resistance Index SBRI Between Groups at Different Times |
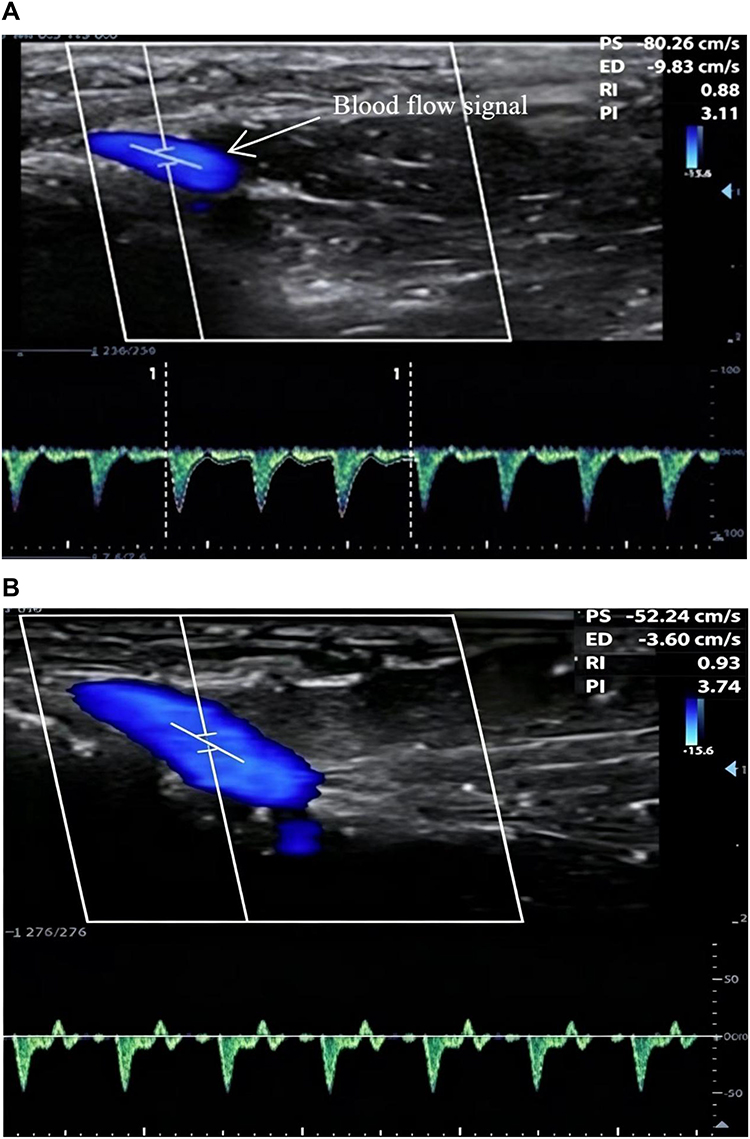 |
Figure 3 Group A Snuffbox Radial Artery Blood Flow ((A) Group A T1 Snuffbox Radial Artery Blood Flow; (B) Group A T2 Snuffbox Radial Artery Blood Flow). |
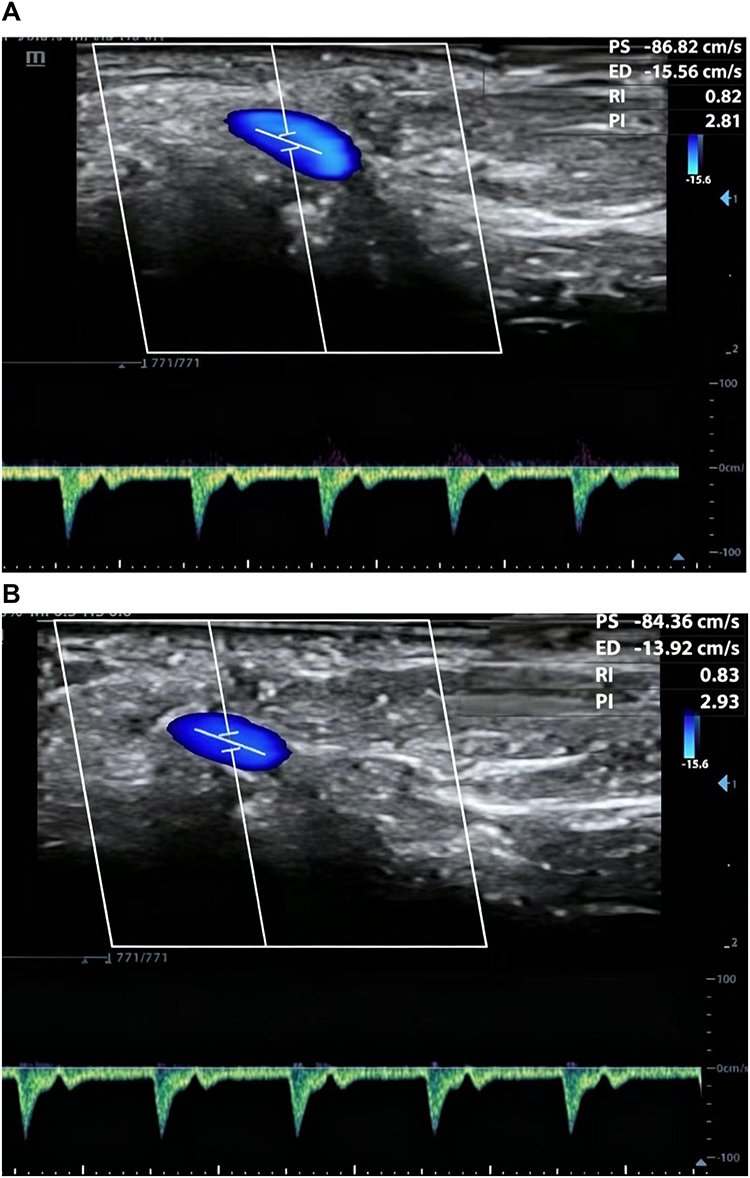 |
Figure 4 Group B Snuffbox Radial Artery Blood Flow ((A) Group B T1 Snuffbox Radial Artery Blood Flow; (B) Group B T2 Snuffbox Radial Artery Blood Flow) Group (A) group receiving esketamine; Group B group receiving non-esketamine. |
After excluding the influence of age, gender, BMI, comorbidities, and baseline blood pressure, the snuffbox radial artery resistance index in the Group A was on average 0.972 units higher than in the Group B(95% confidence interval 0.747~1.197). The pseudo R2 of the model was 0.256, and residual analysis suggested good model fit (Table 4).
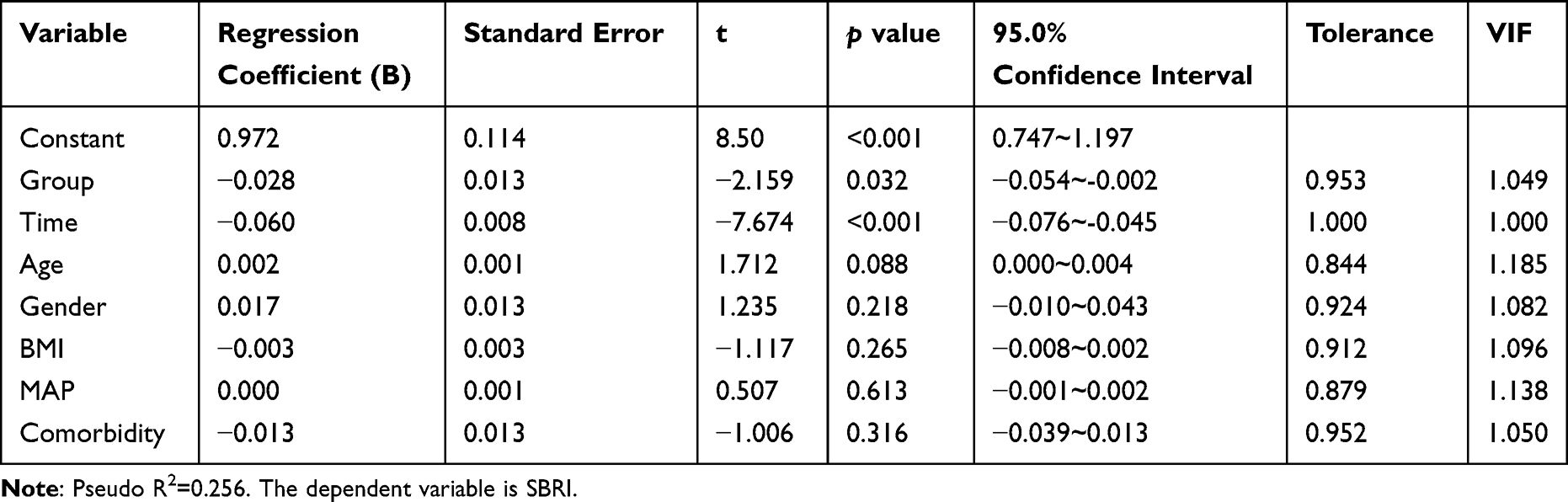 |
Table 4 Beta Regression Model Analysis Results for Factors Influencing SBRI |
Comparison of Adverse Reaction Incidence During Induction Between Groups
During anesthesia induction, there were statistically significant differences between the two groups in the incidence of hypotension, muscle tremor, and vasoactive drug use (P < 0.05). There were no statistically significant differences in the incidence of hypertension, tachycardia, bradycardia, or coughing (P > 0.05). The Group A had lower incidence rates of hypotension (14.3% vs 56.4%), muscle tremor (8.6% vs 33.3%), and vasoactive drug use (5.7% vs 38.5%) compared to the Group B (Table 5).
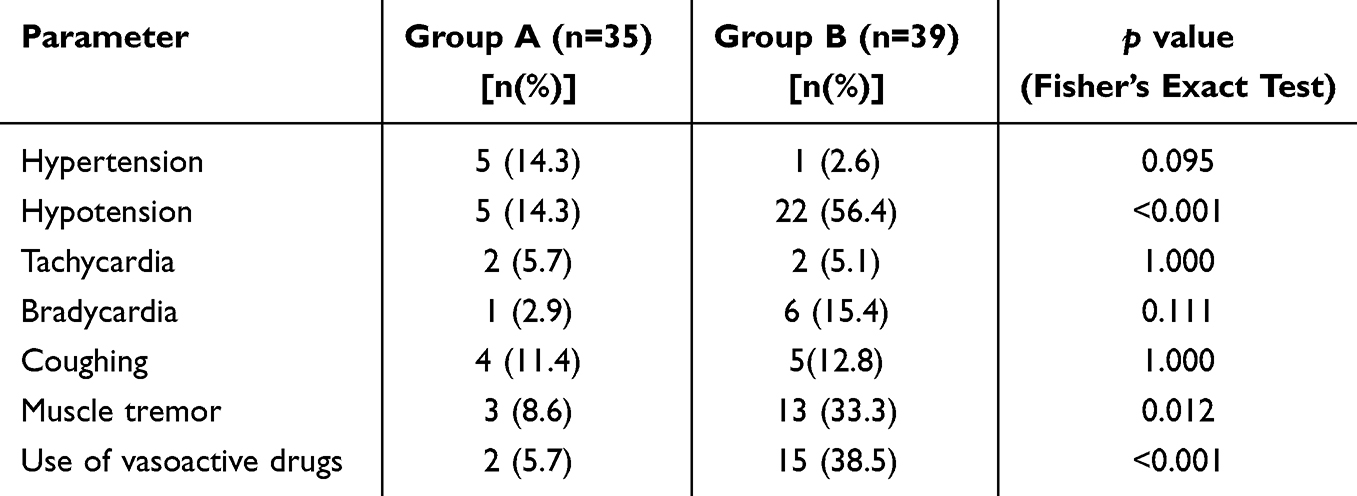 |
Table 5 Comparison of Adverse Reactions During Anesthesia Induction [n(%)] |
Comparison of Recovery Time, Postoperative Recovery Score, and Visual Analogue Scale Between Groups
There were no statistically significant differences between the two groups in postoperative recovery time, Steward recovery score upon awakening, or incidence of postoperative adverse reactions (P > 0.05). The postoperative Visual Analogue Scale (VAS) in the Group A was slightly lower than that in the Group B, a difference that was statistically significant (P < 0.05), with VAS in both groups being below 3 points (Table 6).
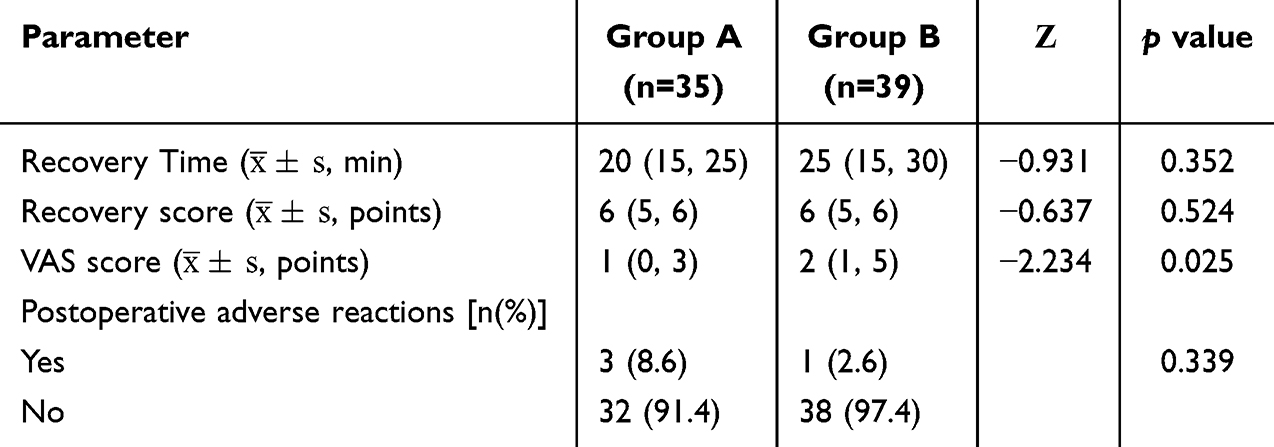 |
Table 6 Comparison of Postoperative Scores Between Groups |
Discussion
The anesthesia induction period is the phase of general anesthesia with the most significant hemodynamic fluctuations.19 Elderly patients, even without severe cardiovascular comorbidities, often exhibit age-related changes in baroreflex sensitivity and autonomic regulation, which increase their sensitivity to anesthetic agents.20 In our study, patients with severe cardiovascular diseases (eg, acute heart failure, myocardial infarction) were excluded, so our findings primarily apply to relatively healthy elderly patients.Studies indicate a high incidence of hypotension during anesthesia induction in elderly patients, and sustained hypotension may lead to inadequate perfusion of vital organs, increasing the risk of adverse cardiovascular and cerebrovascular events.21 Therefore, exploring anesthesia strategies to maintain circulatory stability during induction in elderly patients is a research focus in clinical anesthesia.
Some studies using esketamine for general anesthesia induction in elderly patients found more stable hemodynamics compared to other anesthetics.22,23 Furthermore, assessing peripheral vascular resistance is key to verifying drug efficacy. Traditional vascular resistance measurement requires invasive arterial monitoring, which carries risks of bleeding, infection, and vascular damage in elderly patients. The snuffbox radial artery resistance index, however, can be obtained via ultrasound Doppler technology. It is simple, non-invasive, intuitive (as shown in Figures 3–4), directly reflects peripheral vascular resistance, and is a feasible indicator for evaluating peripheral tissue perfusion.24 Based on this, this study employed a double-blind, prospective, randomized controlled design to systematically evaluate the effect of esketamine used during anesthesia induction on peripheral vascular resistance and hemodynamics in elderly patients.
The results of this study showed no statistically significant differences (P > 0.05) in general data such as age, gender, BMI, comorbidities, and baseline indicators like MAP, HR, and SBRI before induction (T1) between the two groups, eliminating interference from baseline differences and establishing comparability. Hemodynamic results showed that MAP in the Group A was overall higher than in the Group B at time points T2~T7. MAP in the Group A showed a mild increase at T2 after esketamine injection and remained higher than the Group B at T3 after administration of other anesthetics, consistent with the aforementioned mechanism where esketamine’s sympathomimetic effect counteracts the vasodilatory and myocardial depressive effects of etomidate and sufentanil. This aligns with findings from Eberl et al.25 Blood pressure in the Group B significantly decreased at T3 post-induction, while fluctuations in the Group A were smaller, suggesting a certain circulatory protective effect in elderly patients. HR comparison showed blood pressure increased at T4 due to tracheal intubation stimulus in both groups, with mean values higher in the Group A but maintained within clinically safe ranges and without severe tachycardia, indicating that esketamine has a controllable effect on heart rate without increasing cardiac load.
In this study, peripheral vascular resistance results showed that SBRI in the Group A was significantly higher than in the Group B at time points T2-T3. No statistically significant differences in SBRI were found between groups at T4-T7 (P > 0.05). Esketamine may provide beneficial effects on peripheral vascular resistance primarily during the early induction phase (T2–T3), but this effect was not sustained at later time points.The Beta regression model, after excluding confounding factors, showed that SBRI in the Group A was on average 0.972 units higher than in the Group B. As an indicator reflecting peripheral vascular resistance, an increase in SBRI suggests vasoconstriction. Although the differences between MAP and SBRI are statistically significant, the effect size of this single-center study should be interpreted with caution, and larger-scale multicenter studies are needed to verify its universality.
Esketamine’s sympathomimetic effect is likely the primary mechanism for its hemodynamic stabilizing effect. Esketamine can stimulate the sympathetic nervous system center, promoting the release of catecholamines like norepinephrine from sympathetic nerve endings, which bind to α-adrenergic receptors on vascular smooth muscle, causing vasoconstriction, increased peripheral vascular resistance, accelerated heart rate, enhanced myocardial contractility, increased cardiac output, and elevated blood pressure.26,27 The decrease in SBRI at T3, but still higher in the Group A than the Group B, indicates that esketamine can delay the decline in peripheral vascular resistance. The increase in both groups at T4-T7 due to intubation stress suggests that esketamine’s impact on peripheral vascular resistance is concentrated in the early induction phase,19 which is also the period most prone to circulatory fluctuations in elderly patients, highlighting the value of its intervention.
From a clinical application perspective, the advantages of esketamine are also reflected in the following aspects. First, its potent analgesic and sedative effects can reduce intraoperative and postoperative opioid consumption, aligning with the current concept of opioid-sparing anesthesia.28 The lower postoperative VAS in the Group A in this study also confirms the persistence of its analgesic effect. Second, esketamine can also act on bronchial smooth muscle, causing bronchodilation, relieving airway spasm, maintaining airway patency, and reducing airway resistance, which helps maintain good ventilation.29 In this study, the incidence of coughing was slightly lower in the Group A(though not statistically significant), possibly related to this effect. Third, the lack of significant difference in postoperative recovery time and scores between groups suggests that while providing circulatory protection, esketamine did not negatively impact the quality of patient recovery.
Although the incidence of hypertension and tachycardia was slightly higher in the Group A, the differences were not statistically significant, both were within controllable limits, and did not lead to serious clinical consequences. This also indicates the need for individualized dose adjustment and close hemodynamic monitoring in clinical application. This study is a single-center design with a limited sample size, potentially subject to selection bias. Future multi-center, large-sample studies are needed to further validate the conclusions. As a commonly used anesthetic agent, the application of esketamine in general anesthesia induction for elderly patients and its impact on peripheral vascular resistance warrant further in-depth research.
Conclusion
In summary, the use of esketamine during anesthesia induction shows promise in mitigating blood pressure decline and increasing peripheral vascular resistance during the early induction phase (T2-T3) in the elderly patients, maintain hemodynamic stability, and simultaneously reduce the incidence of hypotension, muscle tremor, and the use of vasoactive drugs, demonstrating good clinical application value. The results suggest a potential beneficial effect of esketamine on peripheral vascular resistance during the early induction phase, but these findings should be interpreted with caution due to the single-center design and limited sample size.
Clinical Trial Registry
A single-center, double-blind, prospective, randomized controlled study to evaluate the effect of esketamine on peripheral vascular resistance in elderly patients during anesthesia induction. Registry identifier:ChiCTR2500102259.This study was registered at the Chinese Clinical Trial Registry with the registration number ChiCTR2500102259 on 12/05/2025.
Abbreviations
SBP, Non-invasive arterial systolic pressure; DBP,diastolic pressure; MAP, mean arterial pressure; HR, heart rate; SBRI, the snuffbox radial artery resistance index; PSV, peak systolic velocity; EDV, end-diastolic velocity; CHCT, General Hospital of Central Theater Command of the People’s Liberation Army of China; ASA, American Society of Anesthesiologists; NYHA, New York Heart Association; ECG, electrocardiogram; NIBP, non-invasive blood pressure; SpO2, pulse oxygen saturation; VAS, visual analogue scale.
Ethical Approval
Ethical approval for this study ([2025]118-01) was provided by the Medical Ethics Committee of General Hospital of Central Theater Command of the People’s Liberation Army of China,Wuhan, China on 28 April 2025.
Consent
Written informed consent was obtained from the subjects. All patients and their families voluntarily signed informed consent forms.
Author Contributions
Jingjing Li, Yu Gao and Kailun Jing contributed equally and shared the first authorship. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the construction funds of the key medical specialty-Anesthesiology Department of the Joint Logistic Support Force of the General Hospital of the Central Theater Command (ID:1727), and Guosheng Gan’s project funded by the Open Fund of Hubei Provincial Key Laboratory(Grant No. ZZYKF202301); the Scientific research project of Hubei Provincial Health Commission (Grant No. WJ2025ZH010); the Scientific research project of Hubei Provincial Health Commission (Grant No. WJ202SM129).
Disclosure
The authors did not report any potential conflict of interests.
References
1. Aissaoui Y, Jozwiak M, Bahi M, et al. Prediction of post-induction hypotension by point-of-care echocardiography: a prospective observational study. Anaesth Crit Care Pain Med. 2022;41(4):101090. doi:10.1016/j.accpm.2022.101090
2. Jeong H. Ahn HJ.Optimal remimazolam infusion rate for general anesthesia induction in elderly patients: a dose determination study by the k-in-a-row method. Korean J Anesthesiol. 2025;2005–13.
3. Peng X, Liu C, Zhu Y, et al. Hemodynamic influences of remimazolam versus propofol during the induction period of general anesthesia: a systematic review and meta-analysis of randomized controlled trials. Pain Physician. 2023;26E761–E773.
4. Ren J, Wang L, Sun X. The effect of propofol combined with sufentanil on anesthetic effect, cognitive function, and hemodynamics in patients undergoing intertrochanteric fracture surgery evaluated by propensity score matching. Am J Transl Res. 2023;15(5):3607–3615.
5. Xia Z, Kamra K, Dong J, et al. Comparison of efficacy and safety of etomidate with other anesthesia induction drugs for patients undergoing cardiac surgery: a systematic review and meta-analysis of randomized controlled trials. Heliyon. 2024;10(22):e38274. doi:10.1016/j.heliyon.2024.e38274
6. Shoib S, Kotra M, Javed S, Nguyen VS, Malathesh BC. Esketamine-A quick-acting novel antidepressant without the disadvantages of ketamine. Horm Mol Biol Clin Investig. 2022;43(4):505–511. doi:10.1515/hmbci-2021-0099
7. Zhang S, Bai C, Xu M, et al. Clinical benefits and challenges of esketamine in elderly patients during the perioperative period. Drug Des Devel Ther. 2025;19:8251–8263. doi:10.2147/DDDT.S536813
8. Huang X, Lin F, Chen Q, Hu X. Safety and efficacy of the combination of esketamine and propofol in procedural sedation/analgesia: a systematic review and meta-analysis. Minerva Anestesiol. 2023;89(7–8):680–689. doi:10.23736/S0375-9393.23.17100-8
9. Luo LL, Xiao R, Zhang JP, Xi WF, Xu GH, Yuan H. Opioid-free anesthesia with esketamine combined with iliac fascia block in elderly patients undergoing hip surgery. Drug Des Devel Ther. 2025;19:3337–3349. doi:10.2147/DDDT.S508805
10. Mihaljević S, Pavlović M, Reiner K, Ćaćić M. Therapeutic mechanisms of ketamine. Psychiatry Danub. 2020;32(3–4):325–333. doi:10.24869/psyd.2020.325
11. Liu M, Song D, Hong S, et al. Characteristics and correlations of wall shear stress and flow turbulence in the carotid bifurcation evaluated using an ultrasound vector flow imaging. J Vasc Res. 2024;61(1):38–49. doi:10.1159/000534738
12. Rodríguez Aparicio EE, Almanza Hernández DF, Rubio Ramos C, Moreno Knudsen MP, Rodriguez Lima DR. Correlation between the radial artery resistance index and the systemic vascular resistance index: a cross-sectional study. Ultrasound J. 2024;16(1):29. doi:10.1186/s13089-024-00379-0
13. Du Y, Zhao J. Feasibility study of arterial pressure measurement by snuff pot artery puncture. Zhonghua Wei Zhong Bing Ji Jiu Yi Xue. 2023;35(10):1070–1073. doi:10.3760/cma.j.cn121430-20220124-00088
14. Lee EP, Hsia SH, Huang CC, et al. Strong correlation between Doppler snuffbox resistive index and systemic vascular resistance in septic patients. J Crit Care. 2019;49:45–49. doi:10.1016/j.jcrc.2018.10.010
15. Wang Y, Xu J, Zhou X, et al. Esketamine/Ketamine: dual-action mechanisms and clinical prospects beyond anesthesia in psychiatry, immunology, and oncology. Adv Sci. 2025. Published online.
16. Wang Y, Chang S, Chen D. Research trends and hotspots of ketamine from 2014 to 2023: a bibliometric analysis. Front Neurosci. 2024;18:1407301. doi:10.3389/fnins.2024.1407301
17. Daabiss M. American society of anaesthesiologists physical status classification. Indian J Anaesth. 2011;55(2):111–115. doi:10.4103/0019-5049.79879
18. Ban K, Kochi K, Imai K, Okada K, Orihashi K, Sueda T. Novel Doppler technique to assess systemic vascular resistance: the snuffbox technique. Circ J. 2005;69(6):688–694. doi:10.1253/circj.69.688
19. Ren G, Li C, Wei X, Wang J. Effect of heptaflourane inhalation and anesthesia induction on hemodynamics of elderly patients undergoing elective gastrointestinal tumor surgery. J Oncol. 2022;2022:9022614. doi:10.1155/2022/9022614
20. Wang J, Li Y, Su H, Zhao J, Tu F. Carotid artery corrected flow time and respiratory variations of peak blood flow velocity for prediction of hypotension after induction of general anesthesia in elderly patients. BMC Geriatr. 2022;22(1):882. doi:10.1186/s12877-022-03619-x
21. Zhang L, Yang J, Zhou L, Yu H, Liu B, Zhou L. The use of remimazolam versus propofol for anesthesia induction in video-assisted thoracoscopic surgery: study protocol for a multicenter randomized controlled trial. Trials. 2025;26(1):173. doi:10.1186/s13063-025-08833-7
22. Zhang Y, Zhou Q, Chen R, et al. Effect of esketamine on postinduction hypotension in elderly patients undergoing elective noncardiac surgery: a secondary analysis of a randomized clinical trial. Sci Rep. 2025;15(1):18843. doi:10.1038/s41598-025-03297-w
23. Li Y, Li H, Zhang F, Chen Y, Zhang D. Effects of esketamine versus remifentanil on hemodynamics and prognosis in patients with septic shock receiving invasive mechanical ventilation: a randomized controlled trial. Drug Des Devel Ther. 2025;19:4139–4149. doi:10.2147/DDDT.S520252
24. Wang C, Wang X, Zhang H, Su L, Huang W, Liu D. Association between doppler snuffbox resistive index and tissue perfusion in septic patients. Shock. 2020;54(6):723–730. doi:10.1097/SHK.0000000000001547
25. Eberl S, Koers L, van Hooft JE, et al. Sedation with propofol during ERCP: is the combination with esketamine more effective and safer than with alfentanil? Study protocol for a randomized controlled trial. Trials. 2017;18(1):472. doi:10.1186/s13063-017-2197-8
26. Schnoebel R, Wolff M, Peters SC, et al. Ketamine impairs excitability in superficial dorsal horn neurones by blocking sodium and voltage-gated potassium currents. Br J Pharmacol. 2005;146(6):826–833. doi:10.1038/sj.bjp.0706385
27. Yamakage M, Hirshman CA, Croxton TL. Inhibitory effects of thiopental, ketamine, and propofol on voltage-dependent Ca2+ channels in porcine tracheal smooth muscle cells. Anesthesiology. 1995;83(6):1274–1282. doi:10.1097/00000542-199512000-00018
28. Kleeman-Forsthuber L, Pollet A, Johnson RM, Boyle J, Jennings JM, Dennis DA. Evaluation of low-dose versus high-dose opioid pathway in opioid-naïve patients after total knee arthroplasty. Arthroplast Today. 2022;14:81–85. doi:10.1016/j.artd.2021.11.019
29. Shi DJ, Bao Y, Pei CM, Liang X, Xi CH, Wang GY. Effect of low-dose s-ketamine on cough response during extubation period in patients undergoing suspension laryngoscopic surgery. Zhonghua Yi Xue Za Zhi. 2025;105(8):611–616. doi:10.3760/cma.j.cn112137-20240828-01987
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Analysis of Hemodynamic Effects of Remimazolam and Propofol Combined with Esketamine in Colonoscopic Procedures in the Elderly
Deng BR, Zhang Y, Xie ZF, Wang DD, Zeng T, Zhang DB, Huang L, Wang QY, Shen T, Wu QL
Drug Design, Development and Therapy 2024, 18:5269-5280
Published Date: 19 November 2024
Effects of Esketamine on Postoperative Delirium and Postoperative Cognitive Function in Elderly Gastrointestinal Tumor Patients with Preoperative Anxiety
Zha J, Chen H, Sun Z, Shi R, Yan R, Guo L, Chen X, Lan X, Huang H, Wang L
Drug Design, Development and Therapy 2025, 19:9425-9437
Published Date: 17 October 2025
Effects of Fentanyl-Reduced Regimen with Esketamine and Remimazolam on Bronchoscopy in Elderly Patients
Xie A, Zhang X, Han J, Wu D, Ju F, Zhou Y, Zhou R
Drug Design, Development and Therapy 2025, 19:10485-10493
Published Date: 25 November 2025
Effect of Intraoperative Low-Dose Esketamine on Postoperative High-Sensitivity Troponin T in Elderly Patients Undergoing Ivor Lewis Esophagectomy
Zhou H, Pan Y, Feng X, Zhou M, Yang Z, Zhou F, Chen J, Xu W, Qi Y, Cai L, Wang L
Drug Design, Development and Therapy 2026, 20:588535
Published Date: 25 March 2026
The Effect of Intraoperative Infusion of Different Doses of Esketamine on the Quality of Recovery in Elderly Patients Undergoing Knee Arthroplasty
Fang C, Hu Z, Lv G, Fan X, Zhang X, Li W, Tian T, Yuan Y, Wang J, Chen X
Drug Design, Development and Therapy 2026, 20:590805
Published Date: 6 May 2026