Back to Journals » Drug Design, Development and Therapy » Volume 20
Effect of Intraoperative Low-Dose Esketamine on Postoperative High-Sensitivity Troponin T in Elderly Patients Undergoing Ivor Lewis Esophagectomy
Authors Zhou H, Pan Y, Feng X, Zhou M, Yang Z, Zhou F, Chen J ![]() , Xu W, Qi Y
, Xu W, Qi Y ![]() , Cai L
, Cai L ![]() , Wang L
, Wang L
Received 12 December 2025
Accepted for publication 20 March 2026
Published 25 March 2026 Volume 2026:20 588535
DOI https://doi.org/10.2147/DDDT.S588535
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Anastasios Lymperopoulos
Hai Zhou,1,2,* Yifei Pan,1,2,* Xinran Feng,1,2,* Meiyan Zhou,2,3 Zixuan Yang,1,2 Fan Zhou,1,2 Jiao Chen,1,3 Wenjing Xu,1,2 Yu Qi,1,3 Liangyu Cai,4 Liwei Wang1– 3
1The Xuzhou Clinical College of Xuzhou Medical University, Xuzhou, Jiangsu, People’s Republic of China; 2Department of Anesthesiology, Xuzhou Central Hospital, Xuzhou, Jiangsu, People’s Republic of China; 3Anesthesiology Department, Xuzhou Central Hospital, Southeast University, Xuzhou, Jiangsu, People’s Republic of China; 4Wuxi Affiliated Hospital of Nanjing University of Chinese Medicine, Wuxi, Jiangsu, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Liwei Wang, The Xuzhou Clinical College of Xuzhou Medical University, Anesthesiology Department, Xuzhou Central Hospital, Southeast University, Xuzhou, Jiangsu, People’s Republic of China, Email [email protected] Liangyu Cai, Wuxi Affiliated Hospital of Nanjing University of Chinese Medicine, Wuxi, Jiangsu, People’s Republic of China, Email [email protected]
Purpose: Ivor Lewis esophagectomy impacts circulatory and cardiac function significantly, often leading to elevated postoperative troponin levels. This study aimed to investigate the effect of low-dose esketamine on postoperative levels of the myocardial injury marker high-sensitivity cardiac troponin T in elderly patients undergoing this procedure.
Patients and Methods: 70 elderly patients scheduled for elective Ivor Lewis esophagectomy were randomly assigned using a random number table to the Control group (Group C, n=35) or the Esketamine group (Group K, n=35). In Group K, in addition to conventional anesthetic drugs, intravenous esketamine 0.25 mg/kg was administered during anesthesia induction, followed by continuous intraoperative infusion at 0.125 mg/kg/h as an adjunct to balanced anesthesia. The Control group received conventional anesthesia induction and maintenance. The primary outcome was hs-cTnT concentration at 24 h postoperatively.
Results: In Group K, hs-cTnT concentrations were significantly lower than in the control group at 24h (12.1 ± 3.5 vs 18.7 ± 4.7, P < 0.0001) postoperatively, as well as at 6– 12h and 48h postoperatively. Although the incidence of myocardial injury within 2 days postoperatively (11.4% vs 22.9%, P = 0.205) and perioperative severe arrhythmias (2.9% vs 11.4%, P = 0.164) was lower in Group K than in Group C, the differences were not statistically significant. Compared to the control group, Group K indicated more stable hemodynamics. Among postoperative complications, the incidence of dreaming was higher in Group K, with no significant differences in other complications. For postoperative pain, Group K had lower Numerical Rating Scale (NRS) scores at PACU discharge and on postoperative day 1 to day 3. The PACU stay was shorter in Group K.
Conclusion: Intraoperative low-dose esketamine effectively reduced hs-cTnT concentrations within 2 days postoperatively in elderly patients undergoing Ivor Lewis esophagectomy, demonstrating a potential beneficial effect in preventing myocardial injury and cardiovascular adverse events.
Keywords: high-sensitivity cardiac troponin T, myocardial injury, esketamine, Ivor-Lewis esophagectomy, elderly patients
A Letter to the Editor has been published for this article.
Introduction
The Ivor Lewis esophagectomy is associated with prolonged duration of anesthesia, complex surgical maneuvers, and significant tissue trauma, which frequently induce pronounced perioperative hemodynamic fluctuations and a substantial stress response.1 These pathophysiological disturbances predispose patients to various postoperative complications, including myocardial injury after non-cardiac surgery (MINS) and cardiac arrhythmias.2,3
MINS carries a prognostic significance comparable to that of perioperative myocardial infarction.4,5 Substantial evidence from numerous studies establishes a strong association between MINS and an increased risk of mortality and major adverse cardiovascular events within 30 days to 2 years postoperatively, with 30-day mortality rates reported as high as 8.9%.4,6–9 Among patients who experience MINS, only a minority (approximately 15.8%) present with overt ischemic symptoms, while the vast majority (up to 84.2%) remain clinically asymptomatic.10 This high rate of silent presentation is primarily attributed to the masking effects of postoperative analgesic medications and the overriding surgical stress response, which can obscure typical symptoms such as chest pain.5 High-sensitivity cardiac troponin T (hs-cTnT) demonstrates high specificity for diagnosing clinically silent myocardial injury11 and is recognized as the most sensitive and effective biomarker for detecting MINS.6,12 A large, multicenter study further demonstrated that the peak postoperative hs-cTnT level within the first three days, even in the absence of ischemic features, is significantly associated with 30-day mortality.8 The diagnostic criteria for MINS are defined as an elevated hs-cTnT level (≥ 65 ng/L) or a dynamic change (absolute increase of ≥ 5 ng/L when the postoperative level is between 20 and 65 ng/L) occurring within the first 48 hours after surgery.10
The risk factors for MINS are multifactorial, encompassing advanced patient age, history of vascular disease, prior coronary stenting, acute trauma, significant hemorrhage, tachycardia, hypotension, systemic inflammation, hypoxemia, and pain.10,13 Optimizing anesthetic management strategies to address these modifiable risk factors intraoperatively may potentially reduce the incidence of MINS.
Esketamine, an N-methyl-D-aspartate (NMDA) receptor antagonist, exerts its pharmacological effects through interactions with multiple receptor systems. This multifaceted action confers a range of clinical effects, including sedation, analgesia, anesthesia, sympathomimetic activity, anti-hyperalgesia, anti-inflammation, and anxiolytic/antidepressant properties.14 Recent preclinical investigations by Zhang et al have suggested that esketamine may confer cardioprotective benefits. Their findings indicate that esketamine can enhance cellular antioxidant enzyme activity, reduce levels of oxidative enzymes, and inhibit apoptosis, thereby alleviating cardiomyocyte injury.15 Furthermore, in earlier studies focusing on its racemic parent compound ketamine, Luo et al demonstrated that ketamine attenuates calcium overload in isolated rabbit ventricular myocytes, suggesting another potential mechanism for myocardial protection.16
Despite these promising preclinical findings, whether esketamine translates to clinically meaningful myocardial protection in surgical patients remains uncertain. Therefore, this study was designed to investigate the effect of low-dose esketamine on postoperative hs-cTnT concentrations in elderly patients undergoing Ivor Lewis esophagectomy and to explore its potential cardioprotective role.
Materials and Methods
Study Design and Participants
This was a single-center, prospective, randomized controlled trial. The study protocol was approved by the Ethics Committee of Xuzhou Central Hospital (Approval No.: XZXY-LK-20240906-0142) and was registered in the Chinese Clinical Trial Registry (ChiCTR, http://www.chictr.org.cn; Registration No: ChiCTR2500098877) prior to patient enrollment. The study was conducted in accordance with the ethical principles of the Declaration of Helsinki (1964) and its subsequent amendments. Written informed consent was obtained from all individual participants.
The inclusion criteria were as follows: 1) Aged ≥ 60 years; 2) American Society of Anesthesiologists (ASA) physical status II or III; 3) Body mass index (BMI) between 18.5 and 28.0 kg/m2; 4) Scheduled for elective Ivor Lewis esophagectomy; 5) Intact cognitive function and ability to comprehend and communicate effectively; 6) Provision of written informed consent. Patients were excluded based on the following criteria: 1) Known contraindication or hypersensitivity to esketamine or any other medications used in the study’s anesthetic protocol; 2) History of psychiatric disorders or significant central nervous system injury; 3) History of chronic use of opioids or sedatives, or suspected substance abuse; 4) Major cardiovascular event (eg, myocardial infarction, heart failure) within the past 6 months; 5) Presence of active systemic infection, such as sepsis; 6) Severe hepatic or renal dysfunction; 7) Unwillingness to provide informed consent. The withdrawal criteria included: 1) Occurrence of an allergic reaction to esketamine or other study medications during the trial period; 2) Patient’s decision to withdraw from the study at any point; 3) Administration of any non-protocol interventions that could potentially confound the study outcomes (eg, unplanned reoperation).
Participants were randomly assigned in a 1:1 ratio to either the esketamine group or the control group using a computer-generated randomization sequence. The allocation information was concealed in sequentially numbered, opaque, sealed envelopes, which were opened only after the patient arrived in the operating room. This was a double-blind study, where the participating patients, the research personnel responsible for patient recruitment and enrollment and the personnel responsible for all postoperative assessments were blinded to group assignment. The responsible anesthesiologists were informed about the study medications but received no information identifying individual patients’ group assignments. All study drugs (esketamine or placebo) were prepared by dedicated anesthesia nurses who were not involved in any other aspect of the study or patient care. Outcome data were collected by dedicated trial staff, who were blinded to group allocation, during postoperative follow-up. All other aspects of perioperative care were managed according to standard protocols at the discretion of the clinical surgical and anesthesia teams.
Anesthesia and Monitoring
All patients followed standard preoperative fasting guidelines and did not receive any premedication. Upon arrival in the operating room, standard monitoring was established, incorporating five-lead electrocardiogram (ECG), pulse oximetry (SpO2), non-invasive blood pressure, bispectral index (BIS), and temperature monitoring. Peripheral intravenous access was secured, and an invasive radial arterial catheter was placed under local anesthesia for continuous blood pressure monitoring. All patients received 50 mg of intravenous flurbiprofen axetil as preemptive analgesia before the induction of anesthesia. Anesthesia was induced with intravenous remimazolam (0.1 mg/kg), etomidate (0.2 mg/kg), sufentanil (0.1–5.0 μg/kg), and cisatracurium (0.15 mg/kg). Patients in the esketamine group (Group K) additionally received a bolus of 0.25 mg/kg esketamine at induction, while the control group received an equal dose of normal saline. All patients were preoxygenated and ventilated by facemask for a minimum of 3 minutes until deemed ready for intubation. Following the administration of muscle relaxants, a double-lumen endotracheal tube was placed. Mechanical ventilation was then initiated using a lung-protective strategy, with a tidal volume of 6–8 mL/kg predicted body weight, a respiratory rate of 12–15 breaths/minute, and a fractional inspired oxygen concentration (FiO2) of 60%. The FiO2 was increased to 80% during one-lung ventilation. The end-tidal carbon dioxide (EtCO2) was maintained between 35 and 45 mmHg. Anesthesia was maintained in the control group (Group C) with continuous intravenous infusions of ciprofol (0.4–2.4 mg/kg/h), remifentanil (0.1–1.0 ug/kg/min) and an equal dose of normal saline. Supplemental boluses of cisatracurium were administered as required to maintain muscle relaxation. In Group K, anesthesia was maintained with a balanced technique that included an additional continuous infusion of esketamine at 0.125 mg/kg/h, alongside the infusions of ciprofol and remifentanil. Hemodynamic management aimed to maintain heart rate and mean arterial pressure (MAP) within 20% of pre-induction baseline values. Hypertension, defined as a MAP increase exceeding 20% from baseline, was managed by deepening anesthesia with a bolus of ciprofol or an increase in the remifentanil infusion rate. Hypotension, defined as a MAP decrease greater than 20% from baseline, was treated with intravenous boluses of norepinephrine. Goal-directed fluid therapy was implemented throughout the perioperative period. Fluid administration was guided by pulse pressure variation (PPV) and stroke volume variation (SVV), with the objective of maintaining PPV below 10% and SVV below 15%. Active warming strategies and continuous core temperature monitoring via a nasopharyngeal probe were employed for all patients to maintain normothermia. All surgical procedures were performed by a consistent team of three experienced thoracic surgeons. At the conclusion of surgery, patients were transferred to the postanesthesia care unit (PACU). Upon meeting standardized discharge criteria, they were transferred back to the thoracic surgery ward.
Postoperative Pain Management
All patients were equipped with a patient-controlled intravenous analgesia (PCIA) pump postoperatively. Both groups received the same standardized PCIA regimen. Upon arrival in the PACU or the surgical ward, rescue analgesia was administered if the Numerical Rating Scale (NRS) pain score exceeded 5. The PCIA infusion was temporarily suspended if the NRS score remained below 1 and was accompanied by adverse effects such as respiratory depression, excessive sedation, or hemodynamic instability. The PCIA was recommenced following the resolution of these symptoms.
Outcome Measurements
Data on patient demographics and preoperative laboratory results were collected. Hemodynamic parameters, including systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), and heart rate (HR), were recorded at predefined time points: upon operating room arrival (T0), before tracheal intubation (T1), before surgical incision (T2), after repositioning (T3), after initiation of one-lung ventilation (OLV) (T4), after cessation of OLV (T5), and at the end of surgery (T6). Intraoperative data collection included the duration of surgery, anesthesia, and OLV; the cumulative duration of significant hemodynamic deviations (HR <40 bpm or >100 bpm; MAP <80% or <70% of baseline; MAP >120% or >130% of baseline); total fluid intake, urine output, and estimated blood loss; the consumption of all anesthetic and vasoactive agents; the duration of postanesthesia care unit (PACU) stay; and the length of hospital stay. Arterial blood gas analyses were performed at four time points: baseline in the operating room, after OLV establishment, at the end of surgery, and upon PACU discharge. Postoperative pain assessment included Numerical Rating Scale (NRS) scores at PACU discharge and on postoperative days (POD) 1, 2, and 3. The total number of PCIA demands over the first 48 postoperative hours was recorded. The requirement for rescue analgesia was documented during the PACU stay, on POD 1, POD 2, from POD 3–7, and from POD 7 until hospital discharge. Blood samples were drawn to measure serum hs-cTnT concentrations preoperatively, at the end of surgery, and at 6–12h, 24h, and 48h postoperatively. White blood cell count, neutrophil count, and high-sensitivity C-reactive protein (hs-CRP) levels were measured on POD 1. The incidence of predefined perioperative arrhythmias (atrial fibrillation, ventricular premature contractions [≥5 per minute], and supraventricular tachycardia) was monitored and recorded. The occurrence of perioperative adverse events was documented.
The primary outcome measure was the serum concentration of hs-cTnT at 24h postoperatively.
Secondary outcomes included: the serum concentration of hs-cTnT at the end of surgery, at 6–12h and 48h postoperatively; the incidence of myocardial injury within 2 days postoperatively; the incidence of perioperative arrhythmias; perioperative hemodynamic profiles (as defined in the data collection section); perioperative arterial blood gas parameters; the incidence of perioperative adverse events (definitions and diagnoses are provided in the Appendix); the concentrations of white blood cells, neutrophils, and hs-CRP on POD 1; NRS pain scores upon PACU discharge and on POD 1, 2, and 3; the duration of PACU stay; and the length of hospital stay.
The diagnostic criteria for MINS are defined as an elevated hs-cTnT level (≥ 65 ng/L) or a dynamic change (absolute increase of ≥ 5 ng/L when the postoperative level is between 20 and 65 ng/L) occurring within the first 48 hours after surgery.
Statistical Analysis
Based on previous literature and our pilot study data, which indicated that postoperative hs-cTnT levels typically peak within 24 hours, the sample size was determined using the 24-hour postoperative hs-cTnT concentration. The calculation was based on mean (± standard deviation) 24-hour hs-cTnT values of 10.6 ± 4.5 ng/L in the esketamine group and 15.8 ± 7.5 ng/L in the control group, derived from our pilot study. A two-tailed analysis with a power (1-β) of 0.9 and an alpha (α) level of 0.05 was applied. Using PASS software (Version 20.0.6, NCSS, LLC, Kaysville, USA), a minimum of 31 patients per group (total n=62) was calculated. To account for an anticipated dropout rate of approximately 10%, 35 patients were enrolled per group, resulting in a total sample size of 70.
Statistical analyses were performed using SPSS Statistics (Version 19.0, IBM Corp., Armonk, NY, USA) and GraphPad Prism (Version 10.1.2, GraphPad Software, Boston, MA, USA). The normality of continuous variables was assessed using the Shapiro–Wilk test. Normally distributed continuous data are presented as mean ± standard deviation (SD) and were compared between groups using the Student’s t-test. Non-normally distributed data are presented as median and interquartile range and were compared using the Mann–Whitney U-test. Comparisons of longitudinal measurements within groups across different time points were analyzed using repeated-measures analysis of variance. Categorical variables are summarized as numbers and percentages (%). Differences in categorical variables between groups were assessed using the Pearson chi-square (χ2) test. For the analysis of hs-cTnT trajectory over time, a linear mixed-effects model was employed. The model included group, time and their interaction as fixed effects. Subject was included as a random intercept to account for individual variability and correlation among repeated measurements. An unstructured covariance structure was specified. Significant main effects and interactions were further explored using marginal means comparisons with appropriate adjustment for multiple comparisons. Additionally, a post hoc sensitivity analysis was performed for the outcome of hospital length of stay. During data review, we observed that a subset of patients in both groups developed postoperative pulmonary infections requiring antibiotic treatment, which substantially prolonged their hospitalization. These prolonged stays were attributed to infectious complications rather than factors directly related to the study intervention or the surgical procedure itself, and we were concerned that these outliers might obscure a potential true difference in recovery time between groups. Therefore, we conducted an exploratory analysis excluding patients with documented postoperative pneumonia to assess whether the observed trend toward shorter hospital stay in the esketamine group would become more apparent after removing this confounding factor. The results of this sensitivity analysis are presented in the Results section and should be interpreted with caution given its exploratory nature. A two-sided P-value < 0.05 was considered statistically significant.
Results
Patients
Between September 2024 and June 2025, 74 patients were assessed for eligibility. Three patients were excluded prior to randomization due to surgery cancellation (n=1), withdrawal of consent (n=1), or a history of opioid abuse (n=1). The remaining 71 patients were randomized to the esketamine group (n=35) or the control group (n=36). One patient in the control group was excluded after randomization due to reoperation, resulting in a final analysis cohort of 70 patients (Figure 1).
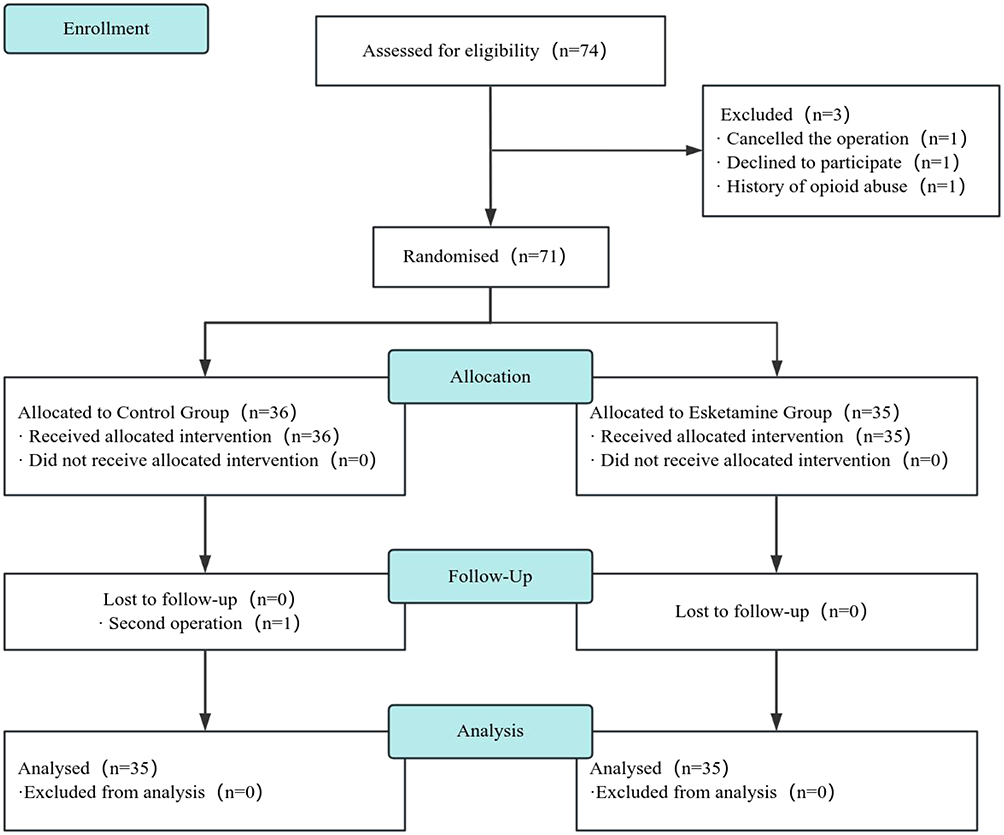 |
Figure 1 Flow diagram. |
Patient demographics, including age, sex, body mass index (BMI), American Society of Anesthesiologists (ASA) physical status, and comorbidities, were comparable between the two groups (all P > 0.05; Table 1). Preoperative laboratory findings also showed no significant differences (Supplementary Table 1). Intraoperative characteristics, including the duration of surgery and anesthesia, one-lung ventilation time, estimated blood loss, urine output, and total fluid intake, were similar between groups (P > 0.05 for all). However, the duration of postanesthesia care unit (PACU) stay was significantly shorter in the esketamine group (82.9 ± 25.9 min) compared to the control group (122.4 ± 41.5 min; P < 0.001). No significant differences were found in the length of hospital stay between the two groups, regardless of whether patients who developed pulmonary infections were included (P = 0.128) or excluded (P = 0.053) from the analysis, although a trend towards shorter stay was noted in the esketamine group (Table 2).
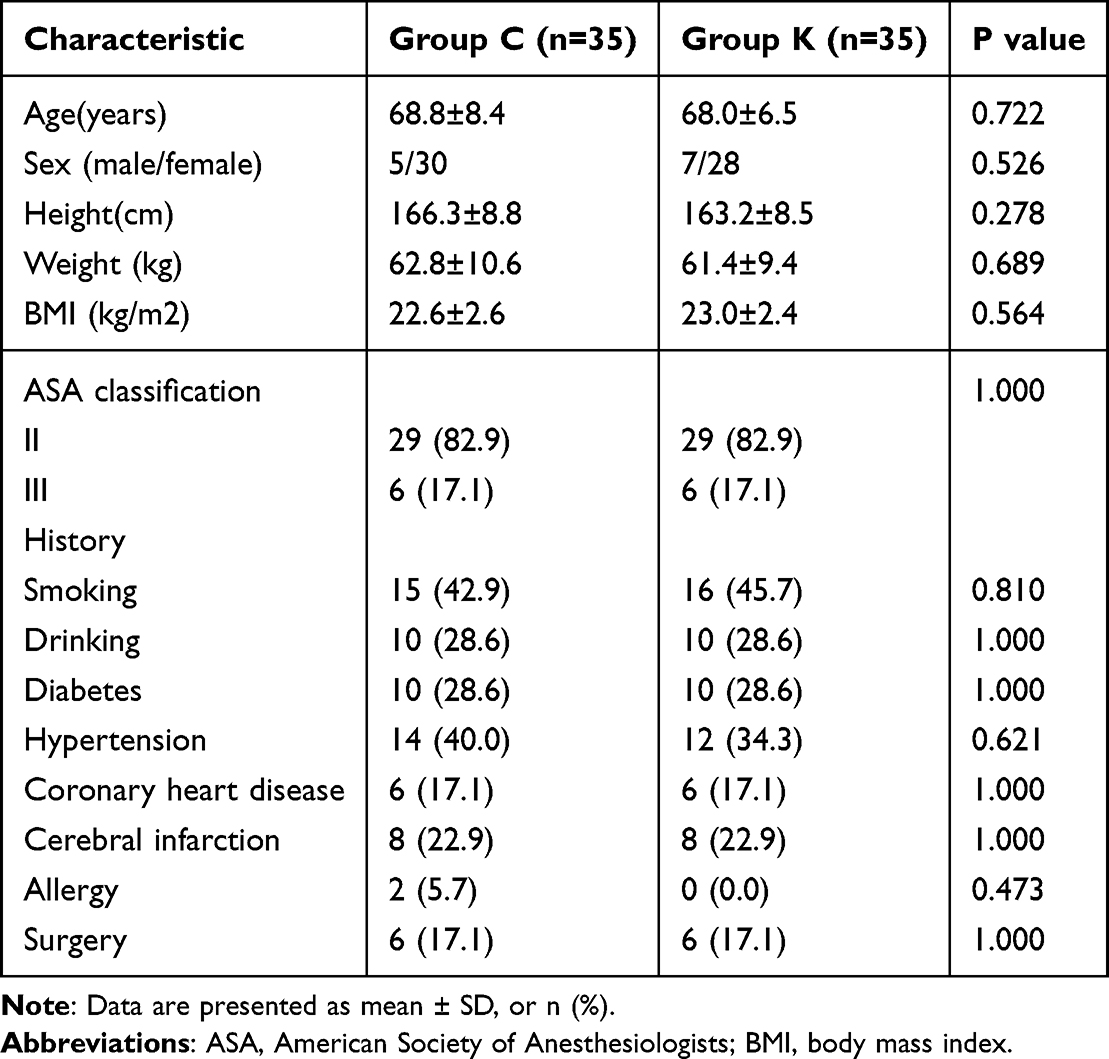 |
Table 1 Comparison of Demographic Data |
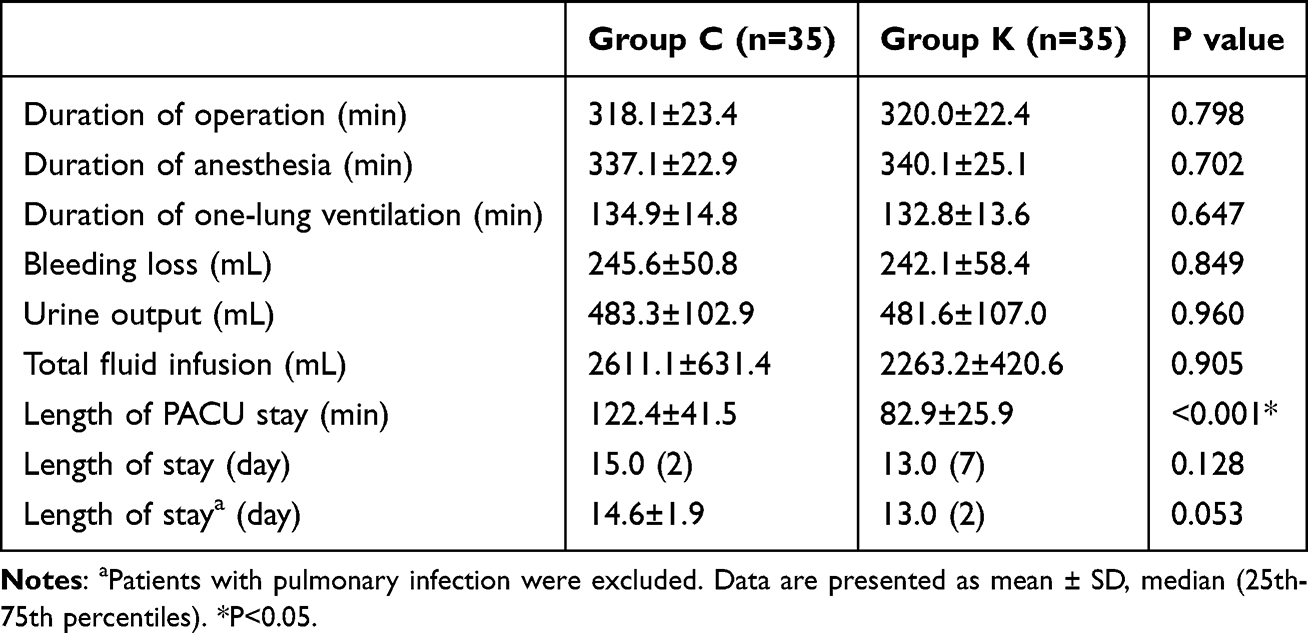 |
Table 2 Comparison of General Perioperative Data |
Outcome Measures
The trajectory of postoperative hs-cTnT concentrations was analyzed using a linear mixed-effects model (Figure 2). The analysis revealed significant main effects of group (F = 22.570, P < 0.001) and time (F = 47.937, P < 0.001), as well as a significant group×time interaction (F = 8.653, P < 0.001). This significant interaction indicates that the temporal pattern of hs-cTnT elevation differed between the two groups. Marginal means comparisons, adjusted for preoperative baseline values, demonstrated that overall hs-cTnT concentrations were significantly lower in the esketamine group compared to the control group (11.90 vs 15.86, mean difference 3.96, P < 0.001). Time point-specific comparisons revealed that while concentrations were similar at the end of surgery, significant between-group differences emerged at 6–12h (15.9 ± 4.1 vs 19.3 ± 4.8, P = 0.021), 24h (12.1 ± 3.5 vs 18.7 ± 4.7, P < 0.0001), and 48h (9.3 ± 2.4 vs 14.7 ± 2.7, P < 0.0001) postoperatively. The esketamine group demonstrated a smaller initial rise, lower peak concentration, more rapid decline by 24h, and faster return toward baseline by 48h, confirming that the intervention modified the temporal trajectory of postoperative hs-cTnT elevation.
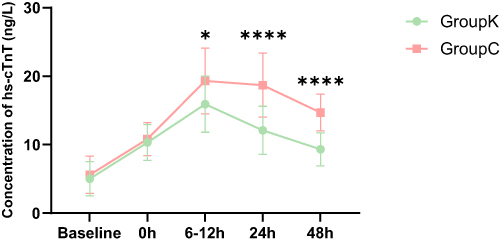 |
Figure 2 Comparison of concentration of hs-cTnT. *P<0.05, ****P<0.0001. |
The absolute change in hs-cTnT from baseline was significantly smaller in the esketamine group at 24 hours (7.0 ± 4.0 vs 13.2 ± 5.5 ng/L, P < 0.001) and 48 hours (4.3 ± 3.1 vs 9.2 ± 4.3 ng/L, P < 0.001), but not immediately post-surgery or at 6–12 hours. Similarly, the change in hs-cTnT from the end-of-surgery value was significantly smaller in the esketamine group at 6–12 hours (5.5 ± 4.2 vs 8.5 ± 3.2 ng/L, P = 0.021), 24 hours (1.7 ± 3.9 vs 7.9 ± 5.0 ng/L, P < 0.001), and 48 hours (−1.0 ± 3.0 vs 3.9 ± 3.0 ng/L, P < 0.0001) (Figure 3). Subsequent intra-group analyses of changes between later postoperative time points (eg, 24h vs 6–12h; 48h vs 24h) revealed no significant differences between the two groups.
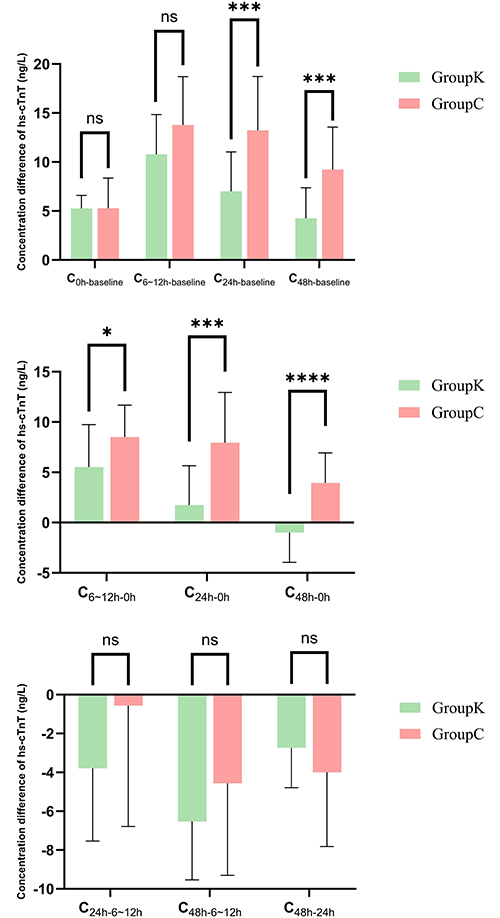 |
Figure 3 Comparison of the concentration differences of hs-cTnT at different times. Abbreviation: ns, no statistical difference. Notes: C0h-baseline represents the difference in hs-cTnT concentration between 0 hours post-operation (at the end of the surgery) and the baseline value. The remaining differences are described in the same way. *P<0.05, ***P<0.001, ****P<0.0001. |
The incidence of myocardial injury within the first 2 postoperative days was lower in the esketamine group (11.4%) compared to the control group (22.9%), but this difference did not reach statistical significance (P = 0.205). One patient in the esketamine group experienced ventricular premature contractions. In the control group, two patients developed atrial fibrillation and two had ventricular premature contractions. The overall incidence of perioperative arrhythmias was 2.9% in the esketamine group and 11.4% in the control group (P = 0.164), with no significant differences in the incidence of specific arrhythmia types (Table 3).
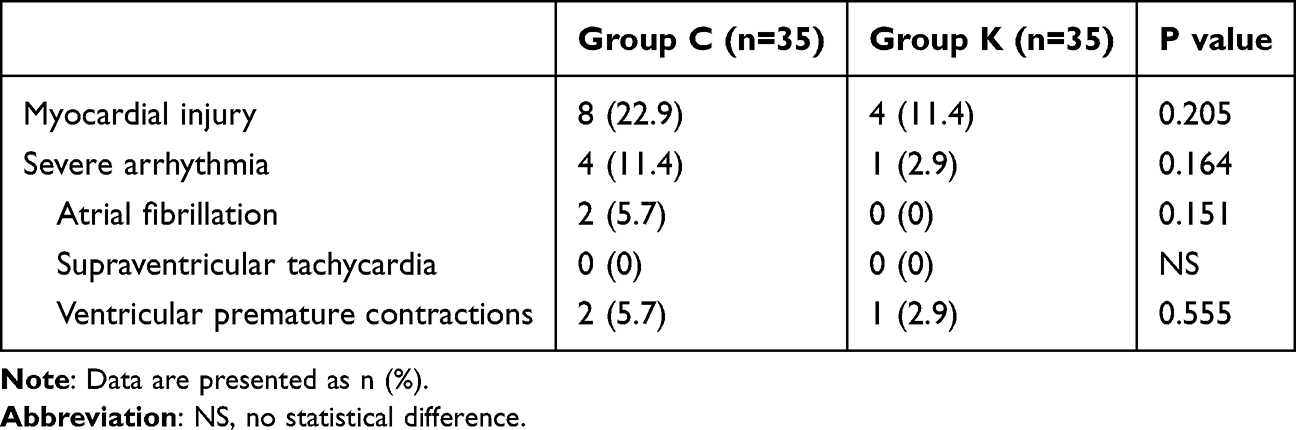 |
Table 3 Comparison of Postoperative Cardiovascular Adverse Events |
Mean systolic, diastolic, and mean arterial pressures (MAP), as well as heart rate, at discrete intraoperative time points were not significantly different between groups (Figure 4, Supplementary Tables 2A and B). To better assess hemodynamic stability, we analyzed the cumulative duration of hypotension. The total time during which MAP fell below 80% of baseline was significantly shorter in the esketamine group (36.1 ± 27.9 min vs 66.4 ± 26.0 min, P = 0.002). Similarly, the time with MAP below 70% of baseline was shorter in the esketamine group (20.8 ± 23.6 min vs 7.0 ± 9.0 min, P = 0.029). No between-group differences were observed in the duration of hypertension (MAP >120% or >130% of baseline). Concordant with these findings, the total intraoperative dose of norepinephrine was lower in the esketamine group (322.8 ± 186.8 µg vs 447.5 ± 176.9 µg, P = 0.045) (Table 4).
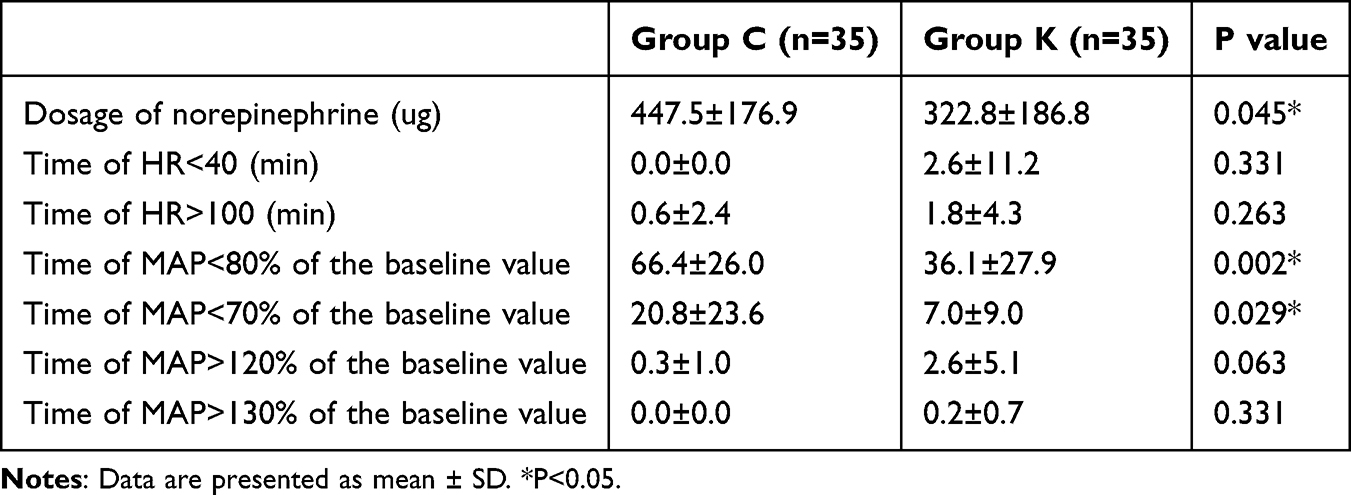 |
Table 4 Comparison of Hemodynamic Data |
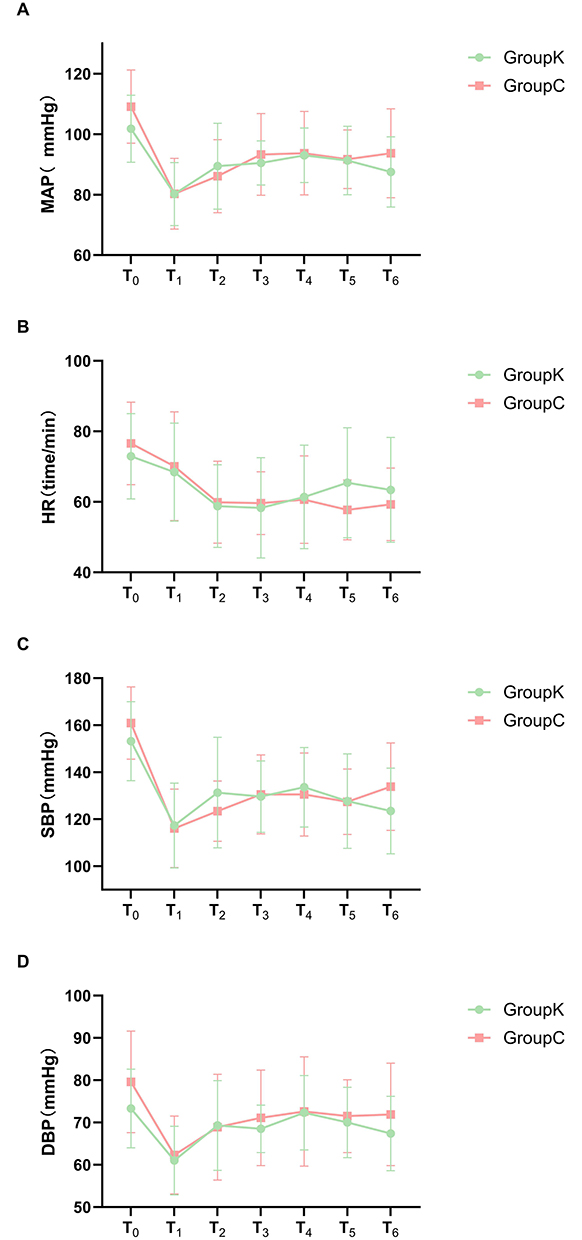 |
Figure 4 Comparison of hemodynamic data, including mean arterial pressure (A), heart rate (B), systolic blood pressure (C) and diastolic blood pressure (D). |
The consumption of perioperative anesthetic agents is detailed in Supplementary Table 3. Total dosages of ciprofol (233.1 ± 64.9 vs 298.6 ± 62.4 mg, P = 0.004), remifentanil (3.95 ± 1.23 vs 5.04 ± 1.39 mg, P = 0.016), and sufentanil (25.0 ± 7.8 vs 43.9 ± 6.8 µg, P < 0.001) were significantly lower in the esketamine group compared to the control group. Postoperative pain scores, assessed using the Numerical Rating Scale (NRS), were significantly lower in the esketamine group upon PACU discharge (3.2 ± 1.4 vs 4.9 ± 2.0, P = 0.005) and on postoperative days 1 (4.2 ± 2.0 vs 5.4 ± 1.3, P = 0.030), 2 (3.4 ± 1.7 vs 4.8 ± 0.9, P = 0.004), and 3 (3.7 ± 1.6 vs 5.3 ± 1.7, P = 0.004). However, the number of patients requiring rescue analgesia and the total number of PCIA demands did not differ significantly between the groups (Table 5). The incidence of adverse events is summarized in Table 6. Patients in the esketamine group experienced a higher rate of dreaming (28.6% vs 8.6%, P = 0.031). No other significant differences in adverse events were observed between the groups.
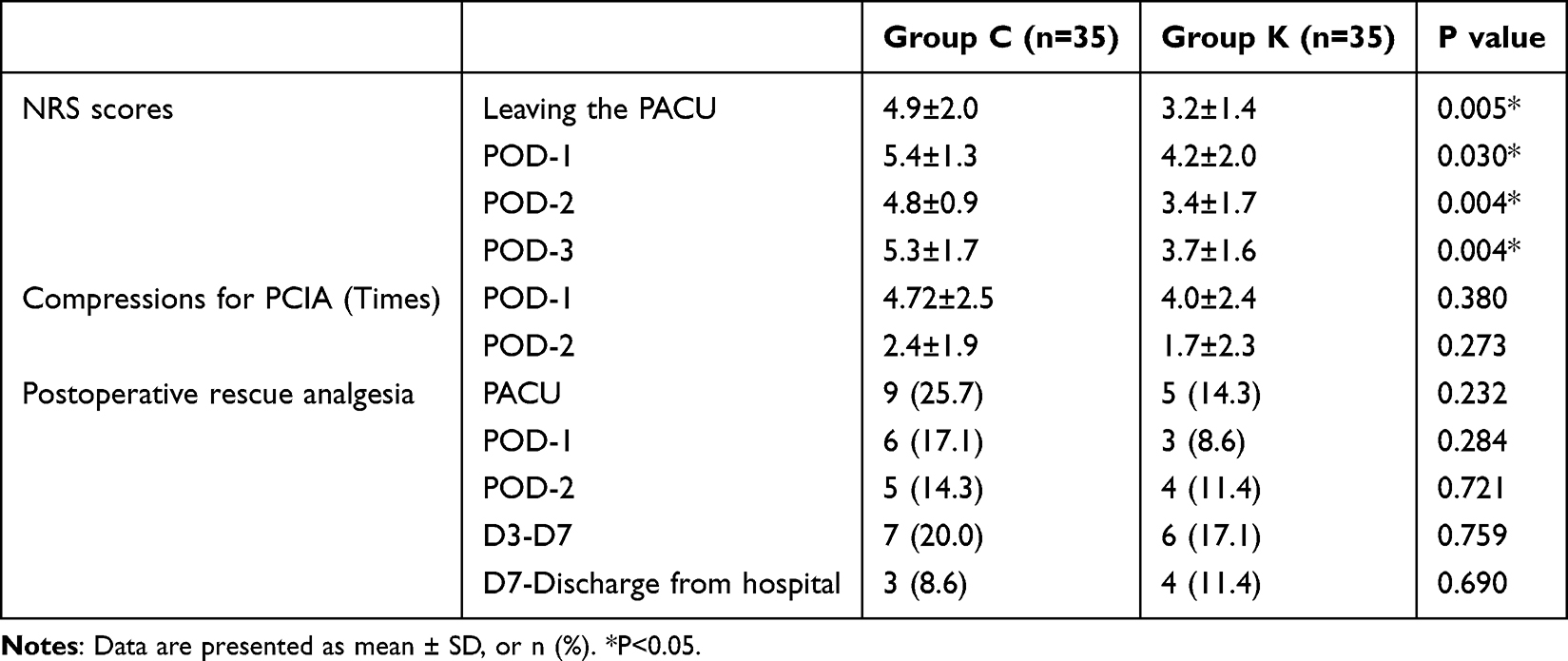 |
Table 5 Comparison of Pain-Related Data |
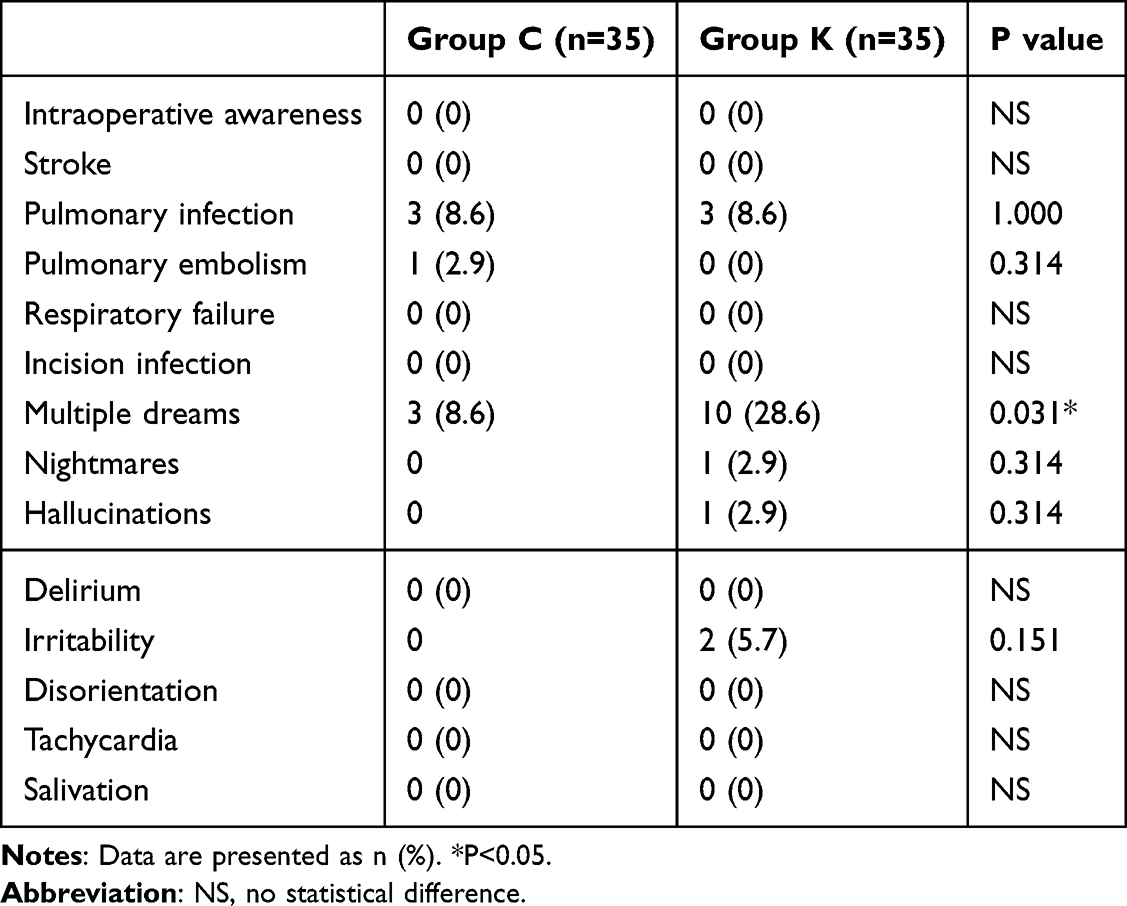 |
Table 6 Comparison of Postoperative Complications |
Furthermore, on postoperative day 1, white blood cell count (8.44 ± 2.44 vs 11.67 ± 2.86 x109/L, P < 0.001), neutrophil count (7.74 ± 2.43 vs 10.18 ± 2.64 x109/L, P = 0.006), and high-sensitivity C-reactive protein (hs-CRP) levels (70.57 ± 27.10 vs 93.10 ± 32.52 mg/L, P = 0.029) were significantly lower in the esketamine group compared to the control group (Supplementary Table 4 and Supplementary Figure 1). Perioperative arterial blood gas parameters were comparable between the two groups (Supplementary Table 5).
Discussion
The present study found that intraoperative use of low-dose esketamine in elderly patients undergoing Ivor Lewis esophagectomy has potential benefits. Specifically, it significantly reduced serum high-sensitivity cardiac troponin T (hs-cTnT) concentrations within the first 48 hours postoperatively compared to a standard anesthetic regimen. The reduction in hs-cTnT was more pronounced in the esketamine group at 24 and 48 hours, both in terms of the absolute change from baseline and the change from the immediate postoperative value. This temporal pattern, where the most significant cardioprotective effect appears within the first 1–2 days, aligns with the typical window for the diagnosis of myocardial injury after non-cardiac surgery (MINS),10 suggesting a potential role for esketamine in mitigating early postoperative myocardial injury. Our findings are consistent with previous work by Bi et a.l17 The observed reduction in hs-cTnT may be attributed to the multifaceted pharmacological profile of esketamine. Proposed mechanisms include its anti-inflammatory properties, which can attenuate the release of inflammatory mediators,18–21 its ability to promote hemodynamic stability, and its potential for direct organ protection. Furthermore, modulation of myocardial calcium handling via L-type voltage-gated calcium channels has been suggested as another potential mechanism.22 The relative contribution of these pathways warrants further investigation. Although we observed no statistically significant differences in the incidence of MINS or perioperative arrhythmias, a trend favoring the esketamine group was noted. The relatively small sample size of this trial, calculated based on a continuous primary outcome (hs-cTnT concentration), likely limited its power to detect significant differences in these less frequent categorical secondary outcomes. Future studies with larger sample sizes are required to definitively assess the impact of esketamine on these clinical endpoints, especially whether this biomarker reduction could translate into improved clinical outcomes.
The Ivor Lewis esophagectomy remains a cornerstone procedure for resectable esophageal cancer.23 While totally minimally invasive approaches exist, comparative studies have not consistently demonstrated their superiority over the open technique in terms of major outcomes, including the incidence of perioperative atrial fibrillation.2,24 Therefore, the Ivor Lewis procedure remains a prevalent and relevant surgical model for investigating perioperative interventions. The transthoracic approach is inherently associated with significant hemodynamic stress and is a recognized independent risk factor for new-onset atrial fibrillation post-esophagectomy.2 Consequently, strategies to enhance hemodynamic stability and minimize myocardial oxygen supply-demand imbalance are critically important in this surgical population. Esketamine is known for its sympathomimetic effects, which are expected to improve hemodynamics. Interestingly, despite a visual trend towards greater stability, mean blood pressure and heart rate at the six predefined intraoperative time points did not differ significantly from the control group, a finding that contrasts with some previous reports.17,25 This discrepancy may be attributable to the limited temporal resolution of discrete time-point measurements, which can fail to capture the full extent of hemodynamic variability. Our subsequent analysis of the duration of hypotension provides a more nuanced insight: the esketamine group spent significantly less time with MAP below 80% and 70% of baseline and required less norepinephrine. This indicates that esketamine supplementation contributed to improved overall hemodynamic stability by reducing the burden of intraoperative hypotension, even if instantaneous values were similar.
Inadequate pain control after thoracotomy leads to severe postoperative pain, which is itself an established risk factor for MINS.13 Our study demonstrated significantly lower NRS pain scores in the esketamine group upon PACU discharge and on the first three postoperative days. This enhanced analgesia is likely mediated by the inhibition of central sensitization by esketamine,26 which extends the duration of effective postoperative pain relief. By mitigating the stress and catecholamine surge associated with severe pain, superior analgesia may represent an additional mechanism through which esketamine contributes to a lower risk of myocardial injury. Furthermore, the consumption of primary anesthetic agents was significantly reduced in the esketamine group, with decreases of 22% for ciprofol, 43% for sufentanil, and 22% for remifentanil. This opioid-sparing effect is clinically relevant, as it may attenuate the known cardiovascular depressive effects of high-dose opioids, thereby further supporting hemodynamic stability.
The duration of PACU stay was approximately 32% shorter in the esketamine group. This finding is supported by preliminary data from our group and is consistent with results from an animal study.27 Esketamine’s ability to promote arousal and maintain hemodynamic stability during emergence28 likely facilitates a faster recovery of consciousness, respiration, and motor function, potentially reducing the period of heightened vulnerability to myocardial ischemia in the immediate postoperative phase.
On postoperative day 1, patients receiving esketamine exhibited significantly lower levels of white blood cells, neutrophils, and high-sensitivity C-reactive protein (hs-CRP). This observation is consistent with the known anti-inflammatory properties of esketamine reported in the literature and aligns with findings from Shen et al in thoracic surgery29 as well as our previous work.25 While these results are suggestive of an attenuated postoperative systemic inflammatory response, it is important to acknowledge that single time-point measurements of non-specific inflammatory markers provide limited evidence for definitive mechanistic conclusions. Future studies incorporating serial measurements of specific cytokines (eg, IL-6, TNF-α) would be valuable to more definitively characterize the anti-inflammatory effects of esketamine. Nevertheless, given that systemic inflammation is a recognized risk factor for MINS, and that elevated hs-CRP is independently associated with an increased risk of early cardiac events,30 the observed reduction in inflammatory markers may represent one of several potential pathways contributing to the cardioprotective effects observed in this study.
An important consideration is the higher incidence of dreaming reported in the esketamine group (28.6% vs 8.6%). Notably, these episodes were predominantly confined to the first 24 hours and were largely described as pleasant by the patients, with only a single instance of a nightmare that caused no significant distress. While this side effect did not lead to major sequelae in our cohort, the nature and impact of perioperative esketamine on dreaming and other psychiatric symptoms warrant careful evaluation in future trials.
Finally, no significant difference was found in the overall length of hospital stay. However, a post hoc analysis excluding patients with prolonged stays due to pulmonary infection revealed a trend towards a shorter hospitalization in the esketamine group (P=0.053). This suggests that our study may have been underpowered to detect a significant difference in this outcome, and a potential benefit on recovery and hospital stay cannot be ruled out.
Several important limitations should be considered when interpreting the secondary outcomes of this study. First and foremost, the sample size calculation was performed based on the primary outcome—postoperative hs-cTnT concentration, a continuous biomarker—rather than on binary clinical events such as MINS incidence, perioperative arrhythmias, or length of hospital stay. Continuous outcomes typically require smaller sample sizes to detect statistically significant differences compared to binary outcomes, particularly those with low expected event rates. Consequently, our study was likely underpowered to detect clinically meaningful differences in these secondary endpoints. This may explain why, despite observing consistent trends favoring the esketamine group across multiple secondary outcomes, these differences did not reach statistical significance. Therefore, these secondary findings should be interpreted as exploratory and hypothesis-generating rather than definitive. They provide preliminary evidence that warrants confirmation in future larger-scale studies specifically powered to detect differences in these clinically relevant outcomes.
Limitations
This study has several limitations. First, the modest sample size may have resulted in insufficient statistical power to detect significant differences in several secondary and exploratory outcomes. These findings therefore require confirmation in larger studies. Furthermore, the observation period was limited to the immediate postoperative hospital stay, and long-term clinical outcomes, including major adverse cardiac events, were not assessed, so the long-term effects of biomarker reductions in patients require further study. Additionally, the scope of biomarkers and mechanistic studies was limited; thus, the precise mechanisms underlying the observed cardioprotective effects of esketamine remain to be fully elucidated. Finally, as a single-center trial, the generalizability of our findings needs to be verified by future rigorously designed, multi-center, large-scale randomized controlled trials to confirm the long-term benefits of low-dose esketamine in elderly patients undergoing Ivor Lewis esophagectomy.
Conclusions
In conclusion, intraoperative low-dose esketamine effectively reduced hs-cTnT concentrations within 2 days postoperatively in elderly patients undergoing Ivor Lewis esophagectomy, suggesting a potential beneficial role in preventing myocardial injury. This cardioprotective signal was accompanied by improvements in some secondary outcomes, including enhanced intraoperative hemodynamic stability, underlying attenuation of the systemic inflammatory response, superior postoperative analgesia, and a shorter PACU stay, without a significant increase in major adverse events.
Data Sharing Statement
All data generated or analyzed during this study were included in the published article. Further inquiries about the datasets can be directed to the corresponding author on reasonable request. Any information we share will be deidentified.
Acknowledgment
The authors thank all patients, surgeons, and nursing staff involved in this trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by New Round of Xuzhou “PengchengTalent Program”- High-level Healthcare Talent Recruitment and Development Project (Project Number: XWRCHT20220017 and XWRCHT20210033), Jiangsu Province’s Key Discipline / Laboratory of Medicine (Project Number: JSDW202231).
Disclosure
The authors declare no competing interests.
References
1. Li B, Xiang J, Zhang Y, et al. Comparison of Ivor-Lewis vs Sweet esophagectomy for esophageal squamous cell carcinoma: a randomized clinical trial. JAMA Surg. 2015;150(4):292–14. doi:10.1001/jamasurg.2014.2877
2. Lohani KR, Nandipati KC, Rollins SE, et al. Transthoracic approach is associated with increased incidence of atrial fibrillation after esophageal resection. Surg Endosc. 2015;29(7):2039–2045. doi:10.1007/s00464-014-3908-9
3. D’Journo XB, Boulate D, Fourdrain A, et al. Risk Prediction model of 90-day mortality after esophagectomy for cancer. JAMA Surg. 2021;156(9):836–845. doi:10.1001/jamasurg.2021.2376
4. Puelacher C, Lurati Buse G, Seeberger D, et al. Perioperative myocardial injury after noncardiac surgery: incidence, mortality, and characterization. Circulation. 2018;137(12):1221–1232. doi:10.1161/circulationaha.117.030114
5. Devereaux PJ, Xavier D, Pogue J, et al. Characteristics and short-term prognosis of perioperative myocardial infarction in patients undergoing noncardiac surgery: a cohort study. Ann Internal Med. 2011;154(8):523–528. doi:10.7326/0003-4819-154-8-201104190-00003
6. Botto F, Alonso-Coello P, Chan MT, et al. Myocardial injury after noncardiac surgery: a large, international, prospective cohort study establishing diagnostic criteria, characteristics, predictors, and 30-day outcomes. Anesthesiology. 2014;120(3):564–578. doi:10.1097/aln.0000000000000113
7. Puelacher C, Gualandro DM, Glarner N, et al. Long-term outcomes of perioperative myocardial infarction/injury after non-cardiac surgery. Eur Heart J. 2023;44(19):1690–1701. doi:10.1093/eurheartj/ehac798
8. Devereaux PJ, Chan MT, Alonso-Coello P, et al. Association between postoperative troponin levels and 30-day mortality among patients undergoing noncardiac surgery. JAMA. 2012;307(21):2295–2304. doi:10.1001/jama.2012.5502
9. Ekeloef S, Alamili M, Devereaux PJ, Gögenur I. Troponin elevations after non-cardiac, non-vascular surgery are predictive of major adverse cardiac events and mortality: a systematic review and meta-analysis. Br J Anaesth. 2016;117(5):559–568. doi:10.1093/bja/aew321
10. Devereaux PJ, Szczeklik W. Myocardial injury after non-cardiac surgery: diagnosis and management. Eur Heart J. 2020;41(32):3083–3091. doi:10.1093/eurheartj/ehz301
11. Ndrepepa G, Braun S, Mehilli J, et al. Prognostic value of sensitive troponin T in patients with stable and unstable angina and undetectable conventional troponin. Am Heart J. 2011;161(1):68–75. doi:10.1016/j.ahj.2010.09.018
12. Iddagoda MT. The role of high-sensitive troponin measurement as a biomarker during the postoperative period for the detection of myocardial injury after non-cardiac surgery. J Perioperat Pract. 2021;31(7–8):300–305. doi:10.1177/1750458920930993
13. Devereaux PJ, Sessler DI, Longo DL. Cardiac complications in patients undergoing major noncardiac surgery. New Engl J Med. 2015;373(23):2258–2269. doi:10.1056/NEJMra1502824
14. Li X, Xiang P, Liang J, Deng Y, Du J. Global trends and hotspots in esketamine research: a bibliometric analysis of past and estimation of future trends. Drug Des Devel Ther. 2022;16:1131–1142. doi:10.2147/dddt.S356284
15. Zhang Y, Lu Q, Hu H, Yang C, Zhao Q. Esketamine alleviates hypoxia/reoxygenation injury of cardiomyocytes by regulating TRPV1 expression and inhibiting intracellular Ca(2+) concentration. Clinics. 2024;79:100363. doi:10.1016/j.clinsp.2024.100363
16. Luo AT, Cao ZZ, Xiang Y, et al. Ketamine attenuates the Na+-dependent Ca2+ overload in rabbit ventricular myocytes in vitro by inhibiting late Na+ and L-type Ca2+ currents. Acta Pharmacol Sin. 2015;36(11):1327–1336. doi:10.1038/aps.2015.75
17. Bi Z, Kong L, Zhao J, Song D, Duan F. Positive effects of low-dose S-ketamine on preventing myocardial injury after thoracoscopic lobectomy in patients aged 70 to 85. BMC Anesthesiol. 2024;24(1):103. doi:10.1186/s12871-024-02491-z
18. Lin Z, Li S, Zhou Y, et al. A comparative study of esketamine-dexmedetomidine and sufentanil-dexmedetomidine for sedation and analgesia in lung tumor percutaneous radiofrequency ablation (PRFA): a randomized double-blind clinical trial. BMC Anesthesiol. 2023;23(1):304. doi:10.1186/s12871-023-02266-y
19. Zeng X, Zhang X, Jiang W, Zhou X. Efficacy of intravenous administration of esketamine in preventing and treating rebound pain after thoracic paravertebral nerve block: a prospective randomized, double-blind, placebo-controlled trial. Drug Des Devel Ther. 2024;18:463–473. doi:10.2147/dddt.S448336
20. Wang CM, Zhang Y, Yang YS, Lin S, He HF. Effect of esketamine pretreatment on acute sepsis-associated encephalopathy. Exp Neurol. 2024;372:114646. doi:10.1016/j.expneurol.2023.114646
21. Godoy DA, Badenes R, Pelosi P, Robba C. Ketamine in acute phase of severe traumatic brain injury “an old drug for new uses?”. Crit Care. 2021;25(1):19. doi:10.1186/s13054-020-03452-x
22. Robinson B, Gu Q, Kanungo J. Antidepressant actions of ketamine: potential role of L-type calcium channels. Chem Res Toxicol. 2021;34(5):1198–1207. doi:10.1021/acs.chemrestox.0c00411
23. Mariette C, Piessen G, Triboulet JP. Therapeutic strategies in oesophageal carcinoma: role of surgery and other modalities. Lancet Oncol. 2007;8(6):545–553. doi:10.1016/s1470-2045(07)70172-9
24. van der Wilk BJ, Hagens ERC, Eyck BM, et al. Outcomes after totally minimally invasive versus hybrid and open Ivor Lewis oesophagectomy: results from the International Esodata Study Group. Br J Surg. 2022;109(3):283–290. doi:10.1093/bjs/znab432
25. Qi Y, Zhou M, Zheng W, et al. Effect of S-ketamine on postoperative nausea and vomiting in patients undergoing video-assisted thoracic surgery: a randomized controlled trial. Drug Des Devel Ther. 2024;18:1189–1198. doi:10.2147/dddt.S449705
26. Wang X, Lin C, Lan L, Liu J. Perioperative intravenous S-ketamine for acute postoperative pain in adults: a systematic review and meta-analysis. J Clin Anesth. 2021;68:110071. doi:10.1016/j.jclinane.2020.110071
27. Duan WY, Peng K, Qin HM, et al. Esketamine accelerates emergence from isoflurane general anaesthesia by activating the paraventricular thalamus glutamatergic neurones in mice. Br J Anaesth. 2024;132(2):334–342. doi:10.1016/j.bja.2023.10.038
28. Song N, Yang Y, Zheng Z, et al. Effect of esketamine added to propofol sedation on desaturation and hypotension in bidirectional endoscopy: a randomized clinical trial. JAMA Network Open. 2023;6(12):e2347886. doi:10.1001/jamanetworkopen.2023.47886
29. Shen W, Yan Y, Zhang W, Xu J, Li Z, Yang L. Esketamine mitigates systemic inflammation via modulating phenotypic transformation of monocytes in patients undergoing thoracic surgery. Life Sci. 2025;371:123594. doi:10.1016/j.lfs.2025.123594
30. Scrutinio D, Passantino A, Di Serio F, Angiletta D, Santoro D, Regina G. High-sensitivity C-reactive protein predicts cardiovascular events and myocardial damage after vascular surgery. J Vascular Surg. 2011;54(2):474–479. doi:10.1016/j.jvs.2011.01.041
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Comparative Analysis of Hemodynamic Effects of Remimazolam and Propofol Combined with Esketamine in Colonoscopic Procedures in the Elderly
Deng BR, Zhang Y, Xie ZF, Wang DD, Zeng T, Zhang DB, Huang L, Wang QY, Shen T, Wu QL
Drug Design, Development and Therapy 2024, 18:5269-5280
Published Date: 19 November 2024
Effects of Esketamine on Postoperative Delirium and Postoperative Cognitive Function in Elderly Gastrointestinal Tumor Patients with Preoperative Anxiety
Zha J, Chen H, Sun Z, Shi R, Yan R, Guo L, Chen X, Lan X, Huang H, Wang L
Drug Design, Development and Therapy 2025, 19:9425-9437
Published Date: 17 October 2025
Effects of Fentanyl-Reduced Regimen with Esketamine and Remimazolam on Bronchoscopy in Elderly Patients
Xie A, Zhang X, Han J, Wu D, Ju F, Zhou Y, Zhou R
Drug Design, Development and Therapy 2025, 19:10485-10493
Published Date: 25 November 2025
The Effect of Intraoperative Infusion of Different Doses of Esketamine on the Quality of Recovery in Elderly Patients Undergoing Knee Arthroplasty
Fang C, Hu Z, Lv G, Fan X, Zhang X, Li W, Tian T, Yuan Y, Wang J, Chen X
Drug Design, Development and Therapy 2026, 20:590805
Published Date: 6 May 2026
The Median Effective Infusion Rate of Ciprofol with Different Doses of Esketamine During Gastrointestinal Endoscopy: A Randomized Controlled Trial
Tang SH, Bao SY, He YY, Ding T, Zhang H, Song JC
Drug Design, Development and Therapy 2026, 20:557205
Published Date: 3 July 2026