Back to Journals » Therapeutics and Clinical Risk Management » Volume 15
The Effect of Coenzyme Q10 Supplementation on Vascular Endothelial Growth Factor and Serum Levels of Interleukin 6 and 8 in Women with Breast Cancer: A Double-Blind, Placebo-Controlled, Randomized Clinical Trial
Authors Zahrooni N, Hosseini SA, Ahmadzadeh A, Ahmadi Angali K, Assarehzadegan MA
Received 16 October 2019
Accepted for publication 20 November 2019
Published 4 December 2019 Volume 2019:15 Pages 1403—1410
DOI https://doi.org/10.2147/TCRM.S234930
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Garry Walsh
Nazanin Zahrooni,1 Seyed Ahmad Hosseini,2 Ahmad Ahmadzadeh,3 Kambiz Ahmadi Angali,4 Mohammad Ali Assarehzadegan5
1Department of Nutrition, Faculty of Paramedicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 2Nutrition and Metabolic Diseases Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 3Thalassemia and Hemoglobinopathy Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 4Biostatistics Division, Health School, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran; 5Department of Immunology, Faculty of Medicine, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Correspondence: Seyed Ahmad Hosseini
Nutrition and Metabolic Diseases Research Center, Ahvaz Jundishapur University of Medical Sciences, Ahvaz, Iran
Tel +98-6133367543
Fax +98-6133720299
Email [email protected]
Background: To better evaluate the efficacy of CoQ10 on the inflammatory markers in breast cancer patients, we conducted a clinical study of patients with breast cancer undergoing tamoxifen therapy. CoQ10 serves as an antioxidant and inhibits oxidation caused by reactive oxygen species. The aim of the current study was to assess the effect of coenzyme Q10 supplementation on serum levels of interleukin 6, 8, and vascular endothelial growth factor (VEGF) in patients with breast cancer undergoing tamoxifen therapy by a double-blind, placebo-controlled, randomized clinical trial.
Methods: In the study, 30 breast cancer patients and 29 healthy subjects were randomized into four groups. Two groups of intervention received 100 mg CoQ10, and two control groups took placebo once a day for 2 months. Blood draws were obtained at baseline and at the end of the study. Serum levels of IL-6, IL-8 and VEGF were analyzed using ELISA kits.
Results: The data of the 59 participants were analyzed. Supplementation with CoQ10 demonstrated a significant decrease in IL-8 and IL-6 serum levels compared to placebo (P< 0.05). Although the downward trend was evident, CoQ10 supplementation did not reveal any significant effect on serum VEGF concentration. The group of patients who received supplements showed the most reduction in serum levels of cytokines among other groups.
Conclusion: CoQ10 supplementation could be effective in ameliorating inflammatory cytokine levels, thereby reducing the consequences of inflammation caused by breast cancer. To generalize the results, larger and longer intervention studies with higher safe doses are needed and should take account of possible costs and harms as well as benefits (registration number: IRCT2015042021874N1).
Keywords: breast cancer, CoQ10, inflammatory cytokines, quality of life, tamoxifen
Background
Coenzyme Q10 (CoQ10) is a protective lipophilic molecule, synthesized in human cells under the control of HMG CoA reductase1 and plays a vital role in the production of ATP as an electron carrier in the respiratory chain.1,2 CoQ10 has an extensive range of functions, which is dependent on sufficient levels of it.3 Other than its role in energy production, CoQ10 has also antioxidant properties. CoQ10 has the potency of conferring protection from reactive oxygen species (ROS), improves the function of protein and enzymes, and reconstructs antioxidants such as vitamin E, vitamin C, and lipoic acid after protecting DNA, lipids and other proteins from oxidative damage. In addition, CoQ10 preserves the brain and other neural tissues from damages caused by free radicals.1–3
Breast cancer (BC) is the most prevalent female cancer and the major cause of death in middle-aged women.4,5 There are different types of breast cancer mainly determined by the expression of the estrogen receptor (ER) and human epidermal growth factor receptor 2 (HER2).6 Damages caused by ROS to DNA and other cell molecules are the most important culprit in the onset and development of the disease. One of the most common drugs used to treat breast cancer is tamoxifen – a selective estrogen receptor modulator.7,8 There are promising publications that antioxidants would complete tamoxifen therapy in BC patients in different aspects.9
Cytokines have both tumor-promoting and inhibitory effects on breast cancer growth depending presumably on their relative concentrations and the presence of other moderating factors.10 Cancer is related to inflammation, which means the levels of pre-inflammatory cytokines such as interleukin-6 (IL-6), interleukin-8 (IL-8), and vascular endothelial growth factor (VEGF) could rise.6,8,10
Cytokines play a significant role in immune system management. IL-6 is a pleiotropic cytokine with noticeably tumor-promoting and tumor-inhibitory effects. Referring to patients’ serum IL-6 levels, unexpectedly unique data are indicated, that IL-6 to be a negative predictor in breast cancer patients.10
In addition, IL-8 seems to have a remarkable capability to functions as a prognostic cancer biomarker via autocrine and paracrine. IL-8 is highly expressed in ER− breast tumors, but it boosts invasiveness and metastatic potential of both ER− and ER+ breast cancer cells.6
Moreover, angiogenesis is crucial for tumor growth. VEGF is one of the most potent angiogenic cytokines. Heer et al have shown that serum VEGF has a much higher sensitivity (62.1%) in detecting BC than both the presently used tumor markers, CA15-3 (13.6%) and CEA (10.3%), with a specificity of 74%.8
The reduction of CoQ10 serum levels in BC patients is associated with less accurate prediction.2 Thus, besides medical treatment in cancer patients, physicians prescribe CoQ10 alongside other antioxidants. One of the CoQ10 anti-inflammatory properties is performed by reducing inflammatory cytokines' secretion.11,12 A study on the efficacy of Q10 supplemented with other nutrients revealed a significant decline in serum levels of IL-1β, IL-6, IL-8, TNF-α, and VEGF after 90 days.13
In our literature review, no clinical trials have been found to support the efficacy of CoQ10 alone in BC patients. Therefore, this study sought to further elucidate CoQ10 effects on serum levels of IL-6, IL-8, and VEGF in breast cancer patients undergoing tamoxifen therapy.
Methods
In this randomized double-blind placebo-controlled clinical trial, 143 women diagnosed as breast cancer patients with positive estrogen receptor were first assessed for eligibility and 30 patients met the inclusion criteria. Patients were recruited from the Medical Oncology Department of the Governmental Shaffa Hospital, Ahvaz, Iran, by their physicians.
The inclusion criteria were as follows: ages between 19 and 49, at least 6 months have passed since chemotherapy and radiation therapy, and a history of taking 20mg/day tamoxifen for at least one year, not taking Q10 supplement or other antioxidants such as vitamin E, willingness to comply with all interventions and follow-up procedures, non-pregnant and non-lactating, having no uncontrolled diseases such as diabetes and hypo/hyper-thyroid, not taking non-prescription drugs, corticosteroids, and statins. Exclusion criteria were as follows: metastasis and total or partial mastectomy. Informed consent was obtained from all subjects with a due explanation of the study.
The patients were randomly allocated into two groups of intervention and control. Subjects in the intervention group (Group 1.A) received an oral dose of 100 mg/day CoQ10,13 and the control group (Group 2.A) received placebo for 2 months. Placebo capsules were the same color and shape as the supplements. The subjects were advised to take the supplements within meals. Compliance was checked by counting the number of tablets handed out to the patients and recollected at the end of the study. The safety of the dose and duration of the study had been proved by the preceding studies.14,15 To eliminate possible effects of tamoxifen on inflammatory cytokine serum levels, patients who did not take tamoxifen should enroll, but for ethical reasons, healthy subjects were enrolled as third and fourth groups, which were given supplements (Group 1.B) and placebos (group 2.B), respectively.
Blood samples were collected after 8–12 hrs of overnight fasting, in the beginning and at the end of the study, respectively. Serum levels of IL-6, IL-8, VEGF, and CoQ10 were determined using the enzyme-linked immunosorbent (ELISA) kit according to the instructions provided by the manufacturer. All biochemical assessments were performed by a skilled assessor who was blind to the group assignment.
All the subjects were commanded by a dietitian to maintain a 3-day dietary record, including two weekdays and one weekend day before and after the end of the study period. Dietary energy and nutrient intake were analyzed by Nutritionist IV software. All the subjects were asked to avoid using soy products thoroughly because of estrogen agonistic/antagonistic effects.16
Sample Size
According to the paper Premkumar et al (2007), using mini-tab software with a confidence interval of 95% and test power of 90%, the sample size in each group was set at 10 persons. To increase the accuracy of the study and to prevent a 50% drop, the sample size was increased to 15 individuals.
Statistical Analysis
Statistical analysis was performed using Statistical Package for Social Science version 22 (SPSS, Chicago, IL, USA). The normality of the distribution of the variables was evaluated using the Shapiro–Wilk test. Chi-square and Kruskal–Wallis H-tests were employed to assess baseline group differences in categorical and continuous variables. Analysis of covariance (ANCOVA) followed by the least significant difference (LSD) test was used to compare the mean of BMI, dietary intake, IL-6, IL-8 and VEGF serum levels between groups at the beginning and end of the study. Paired sample t-test was assessed the differences in each group of mean serum levels of coenzyme Q10 before and after the intervention. Statistical analysis was performed using Statistical Package for Social Science version 22 (SPSS, Chicago, IL, USA). Values are expressed as mean±SD and were considered statistically significant if the P-value was less than 0.05.
Results
A total of 59 subjects were randomized in this trial (Figure 1). Baseline characteristics for all participants are summarized in Table 1. Patient features did not differ significantly between the treatment groups. None of the participants in the study had specific illnesses such as diabetes, hypertension, and thyroid disorders. Menstrual cycle status in the healthy/placebo group (100%) 15 and the healthy/CoQ10 group (15%) was regular, and there is no menstrual cycle in the patient/placebo group (93.3%) 14, and the patient/CoQ10 group (93.3%). Fourteen percent, with the exception of one person in each group with regular menstrual cycles. All patients were at stage 1 or 2 of breast cancer.
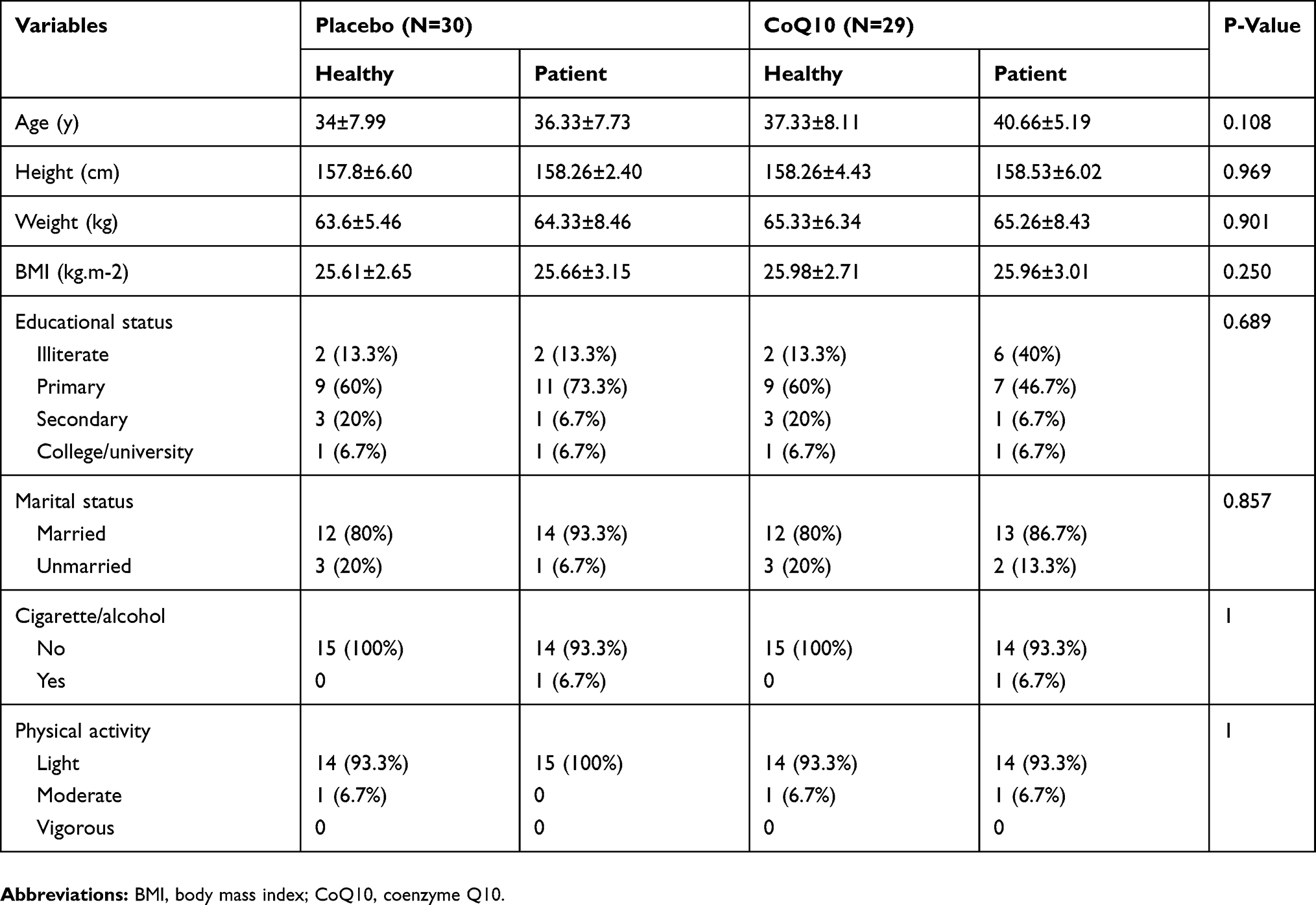 |
Table 1 Anthropometric and Demographic Characteristics in Participants Under Study |
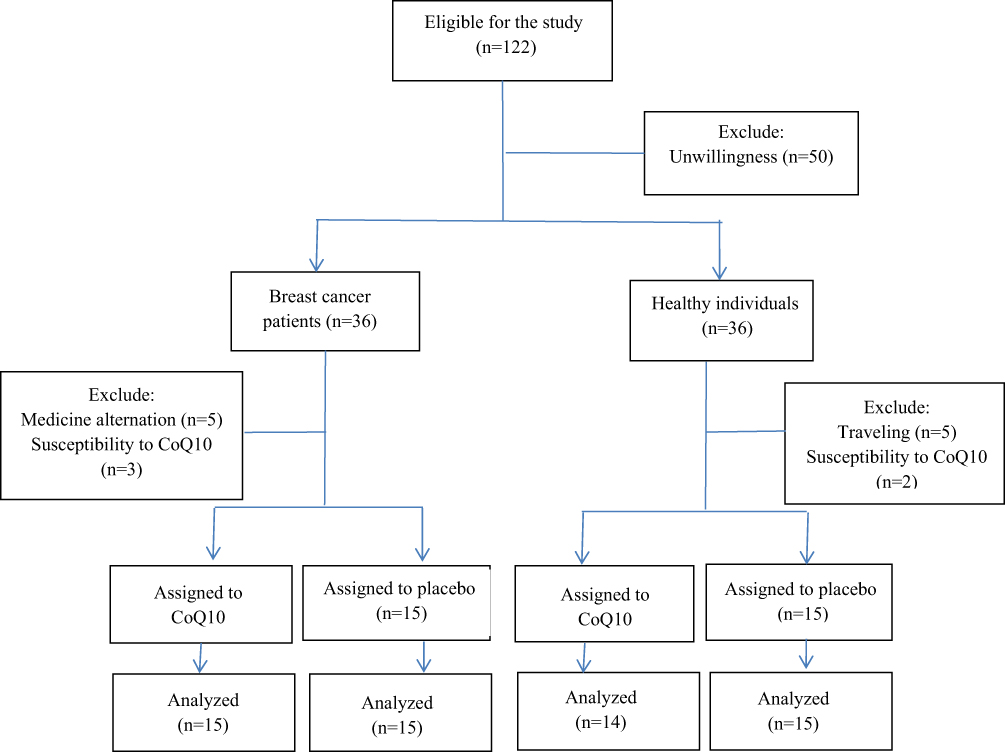 |
Figure 1 Subject’s flowchart. One hundred twenty-two subjects were included in the study. After the exclusion of 63 subjects due to unwillingness, travelling, medication alteration, and susceptibility to CoQ10, 30 breast cancer patients and 29 healthy persons remained and randomized to four groups. Fifteen breast cancer patients and 14 healthy subjects took the CoQ10 supplement and 15 breast cancer patients and 15 healthy subjects took the placebo. Serum samples were sent to the laboratory for evaluation of inflammatory factors before and 8 weeks after the intervention. |
In addition, dietary intake of energy and macronutrients was assessed before and after supplementation. No difference was observed between groups at baseline and no change was detected at the end of 2 months. The average compliance was estimated to be approximately 95.5%. CoQ10 serum levels were measured at baseline and following the 8 weeks of therapy. These data are summarized in Table 2. As can be seen, patients had lower levels of CoQ10 than healthy people. On average, supplementation resulted in more than threefold increase in serum levels of CoQ10, from a mean±SD of 18.40±4.04 ng/L at baseline to 62.40±4.67 ng/L at 8 weeks for patients and approximately twofold elevation from 35.14±7.35 ng/L to 74.50±3.75 ng/L for healthy subjects (p<0.0001). The serum concentrations of IL-6, IL-8, and VEGF were compared between all the study groups and are shown in Table 3. IL-6 serum levels were high in four groups at baseline. After the supplementation, IL-6 serum levels significantly decreased (P=0.043). Hence, paired comparisons of IL-6 serum levels between Group 1.A/Group 2.A (P=0.009) and Group 1.B/Group 2.A (P=0.014) were significant. IL-8 serum levels in subjects who received CoQ10 supplement showed a significant reduction (p<0.0001). Also, paired comparisons of IL-8 serum levels between Group 1.A/Group 2.A, Group 1.B/Group 2.A and Group 1.B/Group 2.B were significant (P<0.001). In this clinical trial, despite the evident downward trend, CoQ10 supplementation did not reveal any significant effect on serum VEGF concentration (p>0.05).
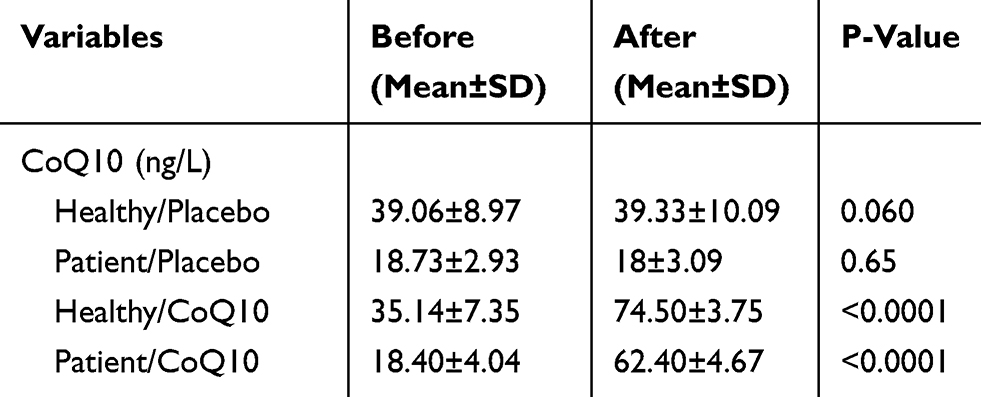 |
Table 2 CoQ10 Status in Participants Before and After Supplementation |
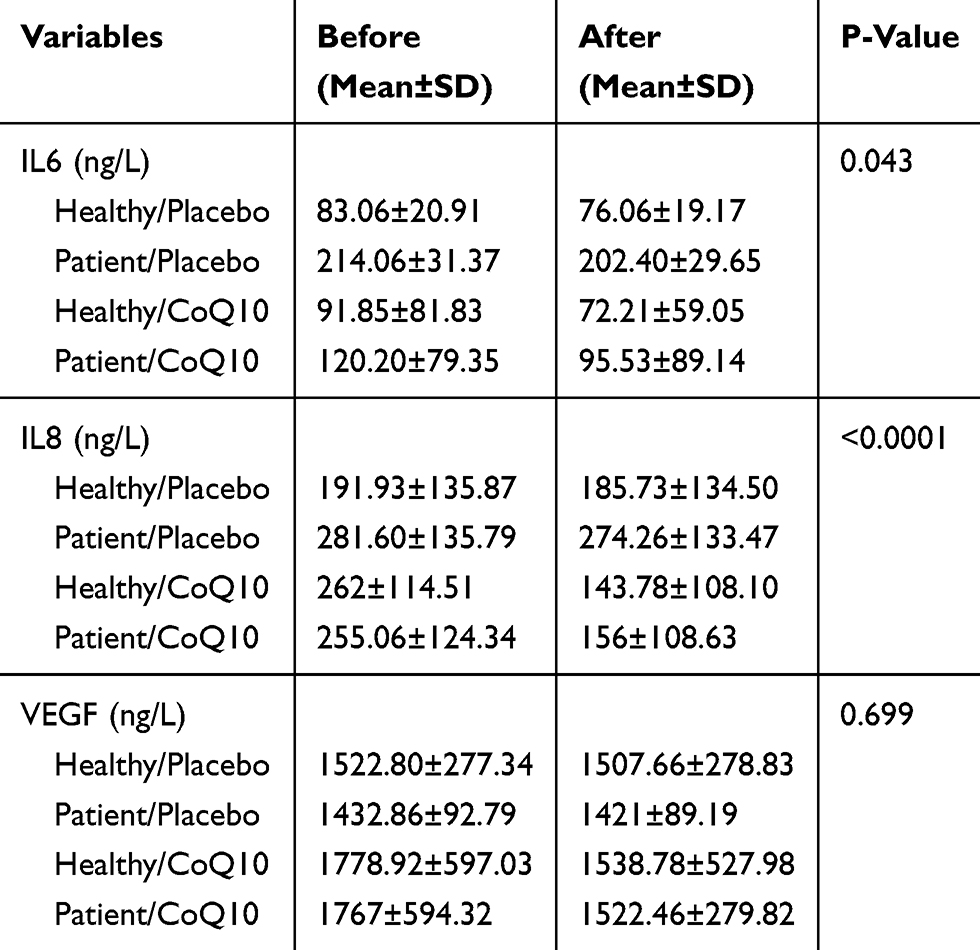 |
Table 3 Effect of Coenzyme Q10 Supplementation on Serum Cytokine Levels in Healthy Subjects and Breast Cancer |
Discussion
The aim of the current study was to evaluate the effects of oral CoQ10 supplementation on serum concentrations of IL-6, IL-8, and VEGF in breast cancer patients, taking 20 mg/day tamoxifen. This trial demonstrated that CoQ10 supplementation for 8weeks in breast cancer patients led to a significant decrease in IL-8 and IL-6 concentrations compared to placebo. Moreover, a non-significant decline was observed in VEGF in four groups. Although the reduction was larger in the supplemented groups than in placebo groups, the difference between the groups was not significant.
The circulating levels of CoQ10 associated with breast cancer risk. SWHS study, with a relatively larger sample size and longer follow-up time, shows an inverse association for plasma CoQ10 levels with breast cancer risk in Chinese women.17 One reason for the prevalent use of CoQ10 supplementation by patients with breast and other cancers is due to the correction of supposed CoQ10 deficiency that could increase treatment-related toxicity tolerance.18
Despite the conflicting effects of IL-6 on breast cancer cells exhibited in many in vitro studies, there is a growing number of trials indicating that the up-regulated serum IL-6 level which demonstrates high IL-6 serum level is a negative prognostic indicator in breast cancer patients. Interleukin 8 could be an essential factor in breast cancer and could influence the efficiency of the treatment by tamoxifen. Therefore, IL-8 and IL-8 receptors are crucial.6 VEGF is one of the most powerful angiogenic cytokines. Proliferation of endothelial cells and promotion of blood vessel permeability is caused by VEGF. Finally, it caused endothelial cells’ organization and tumor cells’ migration that is correlated with decreased relapse-free survival.8
The effects of CoQ10 on oxidative stress and inflammation in other diseases are examined by many researchers, but the results are not consistent. In studies that have been conducted on rheumatoid arthritis19 and hepatocellular carcinoma20 and non-alcoholic fatty liver diseases,21 patients showed no significant reduction in IL-6 between groups. On the other hand, in trials on multiple sclerosis22 and acute myocardial infarction,23 patients experienced a significant decrease in the inflammatory marker (TNF-α and IL-6) plasma levels. There was a statistically significant relationship between plasma CoQ10 levels and levels of vascular cell adhesion molecules, TNF-α, IL-8, IL-10, E-selectin, IL-1ra, IL-6 and IL-2 in septic shock patients.24 Fan et al review detected significant effects of CoQ10 on lowering CRP, IL-6, and TNF-α.25 A different review revealed a significant decrease in TNF-α levels after CoQ10 supplementation but no considerable alteration in IL-6 and CRP serum levels was found.11
Almost consistent with our results, Premkumar et al observed a significant decrease in IL-1 β, IL-6, IL-8, TNF- α and VEGF in patients who were supplemented with CoRN (CoQ10, Riboflavin, and Niacin) along with tamoxifen for 45 and 90 days, respectively, when compared to other groups.13 In the same dose of this study, Rahmani et al found that taking 100 mg/d CoQ10 for 12 weeks in subjects with PCOS downregulated gene expression of IL-1, IL-8, and TNF-a compared with the placebo.26
On the other hand, Michael W. Donnino’s clinical trial in patients with severe sepsis or septic shock showed no difference between the ubiquinol and placebo groups in levels of VEGF, VCAM-1, TNF-α, IL-2 or IL-10 over time. Surprisingly IL-6 levels at 12, 24, 48, and 72 hrs were significantly higher in patients receiving ubiquinol when compared to the placebo group.27
Antioxidant activity is the most prominent biological characteristic of CoQ10, which can scavenge free radicals, also reform the antioxidant defense system by reducing oxidized antioxidants.28 Moreover, numerous in vitro and animal studies have recommended the CoQ10 anti-inflammatory action, suppressing the inflammatory response by reducing the expression of the nuclear factor-kappa B dependent gene.11,29,30 NF-κB can be activated by the ROS and then leads to the upregulation of the pro-inflammatory cytokines expression. However, the activation cascade could be blocked by antioxidants such as Q10.11,30 Promoter analysis of the miR-146a gene proposes a role of NF-κB in LPS-dependent upregulation of miR-146a.31 Supplementation with reduced form of Q10 could be an approach in order to adjust the inflammatory response by modulation of the LPS, reactive oxygen species (ROS), NF-κB signalling pathway and dependent miR-146a expression.12 Moreover, the ability of tube formation, migration, and invasion in endothelial cells decreased by CoQ10. CoQ10 inhibits angiogenesis in endothelial cells via reduction of vascular endothelial growth factor (VEGF) expression and the ERK phosphorylation.32
Conclusions
The first study conducted on CoQ10 supplementation efficacy individually was successful in inflammatory status amelioration in breast cancer patients. Further studies as larger and longer clinical trials with higher safe doses are suggested to generalize results.
Abbreviations
BC, breast cancer; CA15-3, carcinoma Antigen 15-3; CEA, carcinoembryonic antigen; CoQ10, Coenzyme Q10; CRP, C-reactive protein; ELISA, enzyme-linked immunosorbent assay; ER, estrogen receptor; ERK, extracellular signal-regulated kinases; GHS, Global Health Status; HER2, human epidermal growth factor receptor 2; IL-1β, interleukin1-β; IL-6, interleukin-6; IL-8, interleukin-8; LPS, lipopolysaccharide; LSD, least significant difference; NF-κB, nuclear factor-kappa B; ROS, reactive oxygen species; TNF-α, tumor necrosis factor; VCAM-1, vascular cell adhesion molecule-1; VEGF, vascular endothelial growth factor.
Availability of Data and Material
The datasets used and analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This clinical protocol was approved by the Research Ethics Committee of the Ahvaz Jundishapur University of Medical Science (protocol number IRAJUMS.REC.1394.246 July 25,215) which is in accordance with the principles of the Declaration of Helsinki. Signed informed consent was obtained from all individual participants included in the study.
Acknowledgments
This work is a part of Nazanin Zahrooni’s MSc thesis. Special thanks to the staff of Shafa Hematology Clinic, Nutrition, and Metabolic Disease Research Center, and Mr. Karbalai for his contribution in laboratory analyses, and Mrs. Maraghi for cooperation in conducting the statistical analysis of data.
Author Contributions
All authors contributed to data analysis, drafting, and revising the article, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Rodick TC, Seibels DR, Babu JR, et al. Potential role of coenzyme Q10 in health and disease conditions. Nutri Dietary Suppl. 2018;(10):1–11. doi:10.2147/NDS.S112119
2. Garrido-Maraver J, Cordero MD, Oropesa-Avila M, et al. Coenzyme Q10 therapy. Mol Syndromol. 2014;5(3–4):187–197. doi:10.1159/000360101
3. Pinto L, Sloan A, Persaud I, Narain NR. Normalization of Bcl-2 family members in breast cancer by coenzyme Q10. Ethnicity Dis. 2009;19.
4. FARHOOD B, GERAILY G, ALIZADEH A. Incidence and mortality of various cancers in iran and compare to other countries: a review article. Iran J Public Health. 2018;47(3):309–316.
5. Farhood B, Raei B, Malekzadeh R, Shirvani M, Najafi M, Mortezazadeh T. A review of incidence and mortality of colorectal, lung, liver, thyroid, and bladder cancers in Iran and compared to other countries. Contemp Oncol (Pozn). 2019;23(1):7–15. doi:10.5114/wo.2019.84112
6. Kumar RV, Panwar D, Amirtham U, et al. Estrogen receptor, Progesterone receptor, and human epidermal growth factor receptor-2 status in breast cancer: a retrospective study of 5436 women from a regional cancer center in South India. South Asian J Cancer. 2018;7(1):7–10. doi:10.4103/sajc.sajc_211_17
7. Hayes EL, Lewis-Wambi JS. Mechanisms of endocrine resistance in breast cancer: an overview of the proposed roles of noncoding RNA. Breast Cancer Res. 2015;17:40.
8. Heer K, Kumar H, Read JR, Fox JN, Monson JR, Kerin MJ. Serum vascular endothelial growth factor in breast cancer: its relation with cancer type and estrogen receptor status. Clin Cancer Res. 2001;7(11):3491–3494.
9. Lopes CM, Dourado A, Oliveira R. Phytotherapy and nutritional supplements on breast cancer. Biomed Res Int. 2017;2017:7207983. doi:10.1155/2017/7207983
10. Tawara K, Scott H, Emathinger J, et al. Co-expression of VEGF and IL-6 family cytokines is associated with decreased survival in HER2 negative breast cancer patients: subtype-specific IL-6 family cytokine-mediated VEGF secretion. Transl Oncol. 2019;12(2):245–255. doi:10.1016/j.tranon.2018.10.004
11. Zhai J, Yacong B, Yan L, Liu C, Zhang L. Effects of coenzyme Q10 on markers of inflammation: a systematic review and meta-analysis. PLoS ONE. 2017;12(1):e0170172. doi:10.1371/journal.pone.0170172
12. Schmelzer C, Kitano M, Rimbach G, et al. Effects of Ubiquinol-10 on microrna-146a expression in vitro and in vivo. Mediator Inflammation. 2009.
13. Premkumar VG, Yuvaraj S, Vijayasarathy K, Sachdanandam P, Govindaswamy S, Gangadaran D. Serum cytokine levels of interleukin-1β, −6, −8, tumour necrosis factor-α and vascular endothelial growth factor in breast cancer patients treated with tamoxifen and supplemented with co-enzyme Q 10, Riboflavin and Niacin. Nord Pharmacol Soc Basic Clin Pharmacol Toxicol. 2007;100:387–391. doi:10.1111/j.1742-7843.2007.00065.x
14. Hathcock JN, Shao A. Risk assessment for coenzyme Q10 (Ubiquinone). Regul Toxicol Pharmacol. 2006;45(3):282–288. doi:10.1016/j.yrtph.2006.05.006
15. Ikematsu H, Nakamura K, Harashima S, Fujii K, Fukutomi N. Safety assessment of coenzyme Q10 (Kaneka Q10) in healthy subjects: a double-blind, randomized, placebo-controlled trial. Regul Toxicol Pharmacol. 2006;44(3):212–218. doi:10.1016/j.yrtph.2005.12.002
16. Kwon Y. Effect of soy isoflavones on the growth of human breast tumors: findings from preclinical studies. Food Sci Nutri. 2014;2(6):613–622. doi:10.1002/fsn3.2014.2.issue-6
17. Cooney RV, Dai Q, Gao YT, et al. Low plasma coenzyme Q(10) levels and breast cancer risk in Chinese women. Cancer Epidemiol Biomarkers Prev. 2011;20(6):1124–1130. doi:10.1158/1055-9965.EPI-10-1261
18. Lesser GJ, Case D, Stark N, Williford S, Giguere J, Garino LA. A randomized, double-blind, placebo-controlled study of oral coenzyme Q10 to relieve self-reported treatment-related fatigue in newly diagnosed patients with breast cancer. J Support Oncol. 2012. 11(1):31. doi:10.1016/j.suponc.2012.03.003
19. Abdollahzad H, Aghdashi MA, Asghari Jafarabadi M, Alipour B. Effects of coenzyme Q10 supplementation on inflammatory cytokines (TNF-alpha, IL-6) and oxidative stress in rheumatoid arthritis patients: a randomized controlled trial. Arch Med Res. 2015;46(7):527–533. doi:10.1016/j.arcmed.2015.08.006
20. Liu HT, Huang YC, Cheng SB, Huang YT, Lin PT. Effects of coenzyme Q10 supplementation on antioxidant capacity and inflammation in hepatocellular carcinoma patients after surgery: a randomized, placebo-controlled trial. Nutr J. 2016;15(1):85. doi:10.1186/s12937-016-0205-6
21. Farsi F, Mohammadshahi M, Alavinejad P, Rezazadeh A, Zarei M, Ahmadi-Engali K. Functions of Coenzyme Q10 supplementation on liver enzymes, markers of systemic inflammation, and adipokines in patients affected by nonalcoholic fatty liver disease: a double-blind, placebo-controlled, randomized clinical trial. J Am Coll Nutr. 2016;35(4):346–353. doi:10.1080/07315724.2015.1021057
22. Sanoobar M, Eghtesadi S, Azimi A, et al. Coenzyme Q10 supplementation ameliorates inflammatory markers in patients with multiple sclerosis: a double blind, placebo, controlled randomized. Nutr Neurosci. 2015;18:169–176. doi:10.1179/1476830513Y.0000000106
23. Mohseni M, Vafa MR, Hajimiresmail SJ, Zarrati M, Shidfar F, Rahimi-Forushani A. Beneficial effects of coenzyme q10 supplementation on lipid profile and interleukin‑6 and intercellular adhesion molecule‑1 reduction, preliminary results of a double‑blind trial in acute myocardial infarction. Int J Prev Med. 2015;6(1):73. doi:10.4103/2008-7802.162461
24. Donnino MW, Cocchi MN, Salciccioli JD, et al. Coenzyme Q10 levels are low and may be associated with the inflammatory cascade in septic shock. Crit Care. 2011;15(4):R189. doi:10.1186/cc10343
25. Fan L, Feng Y, Chen G-C, Qin L-Q, Fu C-L, Chen L-H. Effects of coenzyme Q10 supplementation on inflammatory markers: a systematic review and meta-analysis of randomized controlled trials. Pharmacol Res. 2017;119:128–136. doi:10.1016/j.phrs.2017.01.032
26. Rahmani EJM, Samimi M, Zarezade-Mehrizi M, et al. The effects of coenzyme Q10 supplementation on gene expression related to insulin, lipid and inflammation in patients with polycystic ovary syndrome. Gynecol Endocrinol. 2017:1–6.
27. Donnino MW, Mortensen SJ, Andersen LW, et al. Ubiquinol (Reduced Coenzyme Q10) in patients with severe sepsis or septic shock: a randomized, double-blind, placebo-controlled, pilot trial. Crit Care. 2015;19:275. doi:10.1186/s13054-015-0989-3
28. Alam A, Rahman M. Mitochondrial dysfunction in obesity: potential benefit and mechanism of Co-enzyme Q10 supplementation in metabolic syndrome. J Diabetes Metabol Disord. 2014;13:60. doi:10.1186/2251-6581-13-60
29. Morris G, Anderson G, Berk M, Maes M. Coenzyme Q10 depletion in medical and neuropsychiatric disorders: potential repercussions and therapeutic implications. Mol Neurobiol. 2013;48(3):833–903.
30. Schmelzer C, Lorenz G, Rimbach G, Doring F. In vitro effects of the reduced form of coenzyme Q10 on secretion levels of TNF-α and chemokines in response to LPS in the human monocytic cell line THP-1. J Clin Biochem Nutr. 2009;44:62–66. doi:10.3164/jcbn.08-182
31. Taganov KD, Boldin MP, Chang K-J, Baltimore D. NF-κB-dependent induction of microRNA miR-146, an inhibitor targeted to signaling proteins of innate immune responses. Proc Natl Acad Sci U S A. 2006;103(33):12481–12486. doi:10.1073/pnas.0605298103
32. Choi JS, Park SY, Yi EY, Kim YJ, JW J. Coenzyme Q10 decreases basic fibroblast growth factor (bFGF)-induced angiogenesis by blocking ERK activation. Oncol Res. 2011;19(10–11):455–461. doi:10.3727/096504012X13285365944256
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.