Back to Journals » Journal of Asthma and Allergy » Volume 16
The Effect of Biologic Therapy in Severe Asthmatics and ER Admissions During COVID-19: A Retrospective Study
Authors Cleland D, Arias C, Alismail A ![]() , Daher N
, Daher N ![]() , Leeper L, Casillas P, Tan LD
, Leeper L, Casillas P, Tan LD ![]()
Received 20 April 2023
Accepted for publication 27 July 2023
Published 10 August 2023 Volume 2023:16 Pages 833—837
DOI https://doi.org/10.2147/JAA.S416054
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Derrick Cleland,1 Christian Arias,1,2 Abdullah Alismail,2,3 Noha Daher,4 Lan Leeper,5 Paul Casillas,2 Laren D Tan2,3
1Department of Internal Medicine, Loma Linda University Health, Loma Linda, CA, USA; 2Department of Cardiopulmonary Sciences, School of Allied Health Professions, Loma Linda University Health, Loma Linda, CA, USA; 3Department of Medicine, School of Medicine, Loma Linda University Health, Loma Linda, CA, USA; 4Allied Health Studies, School of Allied Health Professions, Loma Linda University Health, Loma Linda, CA, USA; 5Enterprise Data Intelligence Services, Department of Information Services, Loma Linda University Health, Loma Linda, CA, USA
Correspondence: Laren D Tan, Department of Medicine, School of Medicine, Loma Linda University Health, Loma Linda, CA, USA, Email [email protected]
Introduction
The COVID-19 (SARS-CoV-2) pandemic and the resulting respiratory illnesses have emphasized the importance of managing and preventing this infection among patients at greatest risk of mortality (eg, patients with predisposing respiratory conditions, such as asthma). Severe asthmatics are of particular concern when considering this illness, because treatment options for this cohort are already limited due to the fact their disease is characterized by the Global Initiative for Asthma as an inability to control asthma with non-biologics.1 Current available biologics for asthmatics include omalizumab, mepolizumab, benralizumab, reslizumab, and dupilumab. Biologics decrease the immunoresponse of the body by binding monoclonal antibodies to IgE and interleukins, causing a decline in circulating IgE levels and inhibition of the signaling process of interleukins. In the SARS-CoV-2 disease process, cytokines and chemokines are released excessively and drive the hyperinflammation (eg, cytokine-release storm) that ultimately leads to acute respiratory distress syndrome, a major complication leading to death in about 40% of intensive care unit (ICU) cases.2 Several studies have identified elevated levels of IL6 as it relates to SARS-CoV-2, thus making the anti-IL6 properties of tocilizumab favorable for treating severe illness.2,3 Therefore, we theorize that asthmatics on biologics are at less risk of developing severe infections due to concurrent biologic treatment than those not on biologics.
Materials and Methods
This was a retrospective study that was approved by Loma Linda University Health Institutional Review Board. Informed consent was waived as per 45 CFR 46.116(d) and HIPAA authorization waived as per 45 CFR 164.512. The study was in compliance with Declaration of Helsinki. We extracted and analyzed data from a large single academic center in the United States from January 2020 to March 2021. Inclusion criteria were asthmatic patients aged 18 years and older, COVID-19 diagnosis, admitted or presented at the emergency room or affiliated urgent care center, and use of biologics. No exclusion criteria were utilized for this study. Severe asthmatics were compared to less severe asthmatics to better understand if there were a clinically significant difference between the severity level of COVID-19 infections between these cohorts. The ICD-10 codes used as part of the inclusion criteria and data extraction were J45 and subcategories, U07.1, Z86.16, M35.81, J12.82, J98.4, R06.00, Z86.16, J96, J80, J40, and J06.9.
Data were analyzed using SPSS 28.0.0. Patients’ characteristics were summarized using counts and percentages for categorical variables and means ± SD or medians (range) for continuous variables. Normality of variables was examined using the Shapiro test and box plots. To examine the association between likelihood of being hospitalized and being on biologics (yes/no), χ2 analysis was used. The level of significance was set at p ≤0.05.
Results
A total of 189 patients met the inclusion criteria, of whom 53 (28%) were on biologics and 136 (72%) were not. Of the sample, 143 (76%) had an emergency room (ER) visit, of whom 108 (75.5%) were female and 35 (24.5%) male. Of that 143, only seven (4.9%) were on biologics (four took benralizumab, two dupilumab, and one omalizumab). Of those who had ER visits, 125 (87.4%) were hospitalized, of whom 51 (35.7%) had an ICU admission. The mean age of those who had an ER visit was 51.3±19.9 years. Of those who were hospitalized, the median inpatient length of stay (LOS) was 5 (0.3–70.9) days. The median length of ICU stay was 2.6 (0.1–41.2) days (Table 1 and Table 2), while χ2 analysis revealed that those on biologics were less likely to be hospitalized than those who were not (4.8% vs 95.2%, χ2=98.8; P<0.001).
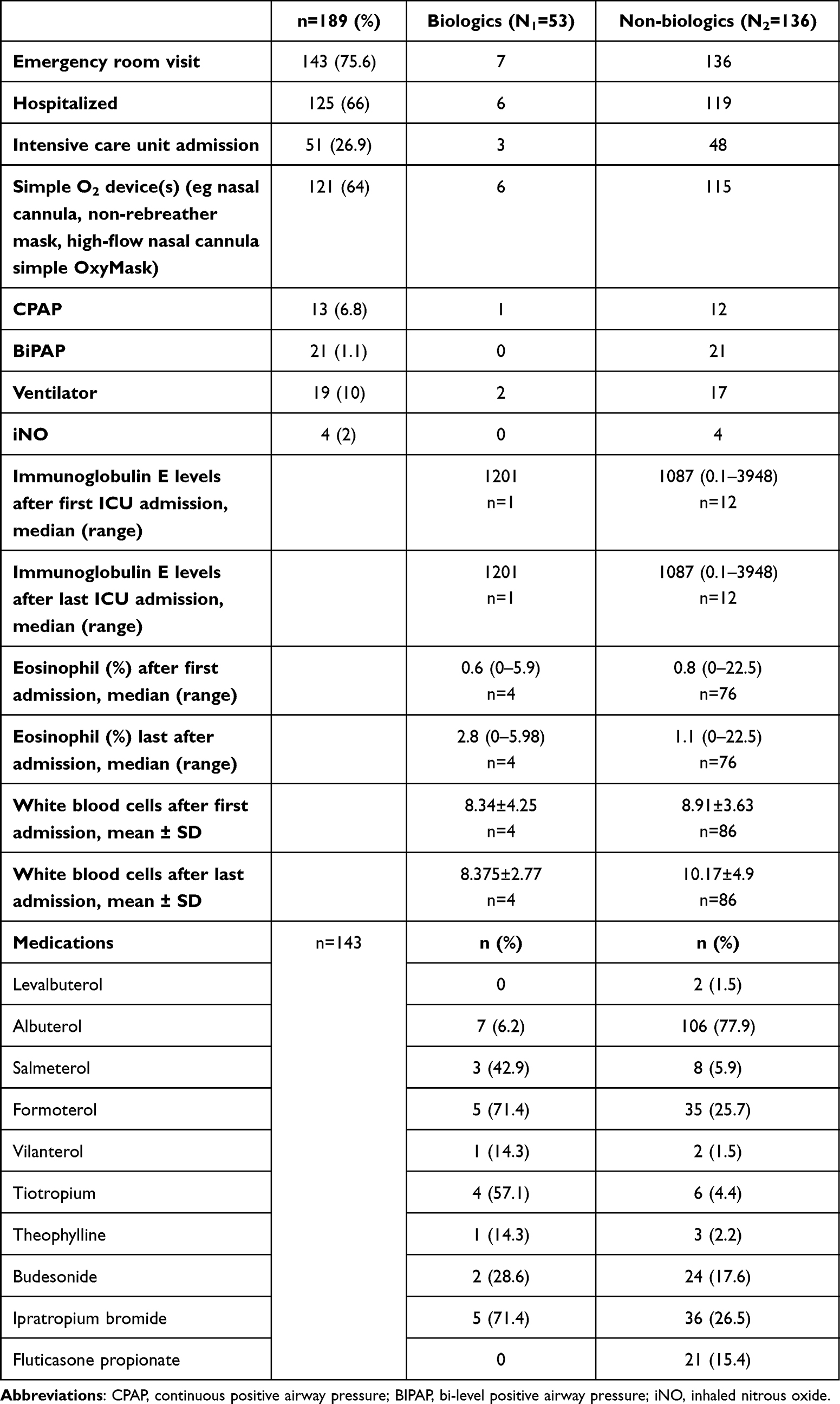 |
Table 1 Comparison of asthmatics’ vs severe asthmatics’ hospital data for COVID-19 infections (N=189) |
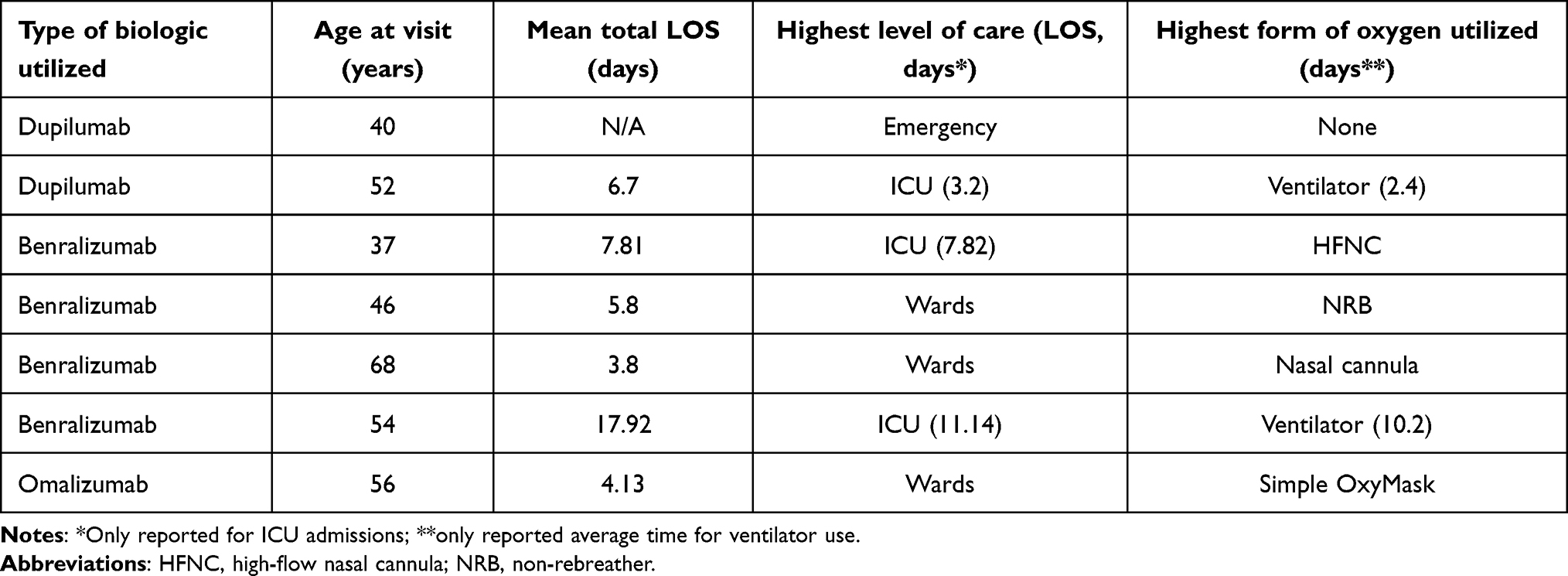 |
Table 2 Hospitalization data of severe asthmatics |
Discussion
Review of the chart data revealed that severe asthmatics had less likelihood of being hospitalized due to COVID-19 and were less likely to develop severe illness. These results may be due to the depressed immunoresponse seen with use of biologics and prevention of the cytokine-release storm commonly seen with SARS-CoV-2 infections. Similar findings were observed among severe asthmatics within Italy when compared to the general population in 2020.4 Prior studies have proposed that dupilumab can lead to reductions in IL4 and IL13, thus leading to less severe COVID-19 reactions among those previously on this treatment and improved survival rates among those initiated on this therapy thereafter.5,6 Another proposed explanation is that the elevated levels of T cells (eg, CD4+ and CD8+), as observed in the TH2-cell inflammatory pathway among severe asthmatics, may offset the lymphopenia effects of SARS-CoV-2, thus leading to less severe reactions.7,8 Reduction in the expression of ACE2, the main point of entry for SARS-CoV-2, has also been linked with the TH2-cell inflammatory pathway and may have protective effects.9 In contrast, prior studies have linked eosinopenia with more severe COVID-19 reactions, as well as increased mortality.7 However, as observed in our study, the lower eosinophil and IgE levels among asthmatics on biologics did not in fact result in more severe illness. Additionally, we theorize that severe asthmatics are less likely to be hospitalized due to closer follow-up intervals with specialists leading to closer monitoring during the COVID-19 pandemic, thus allowing for enhanced preventive measures.
Analyzing the data further (see Table 1) revealed that 13.2% of those classified as severe asthmatics presented to the hospital and those on mepolizumab and reslizumab did not seek medical attention at our hospital during our study period. Among severe asthmatics that were hospitalized (see Table 2), the predominant biologic that was utilized was benralizumab (57%, n=4), of whom two were admitted to the ICU for an average LOS of 9.5 days and average total LOS of 8.8 days. Only one required mechanical ventilation for an average of 10.2 days. Dupilumab was another biologic utilized by one severe asthmatic that was admitted to the ICU for an average LOS of 3.2 days in ICU and total LOS of 6.7 days, and required mechanical ventilation for an average of 2.4 days. Also of note, patients using omalizumab were hospitalized to general wards for an average of 4.13 days. Prior research has shown minimal difference among the efficacy of mepolizumab, benralizumab, and dupilumab when treating severe asthmatics.8 Therefore, it is unclear if the differences in our hospitalization data were due to the difference in biologics utilized. Further retrospective data will need to be analyzed to examine differences among biologics and associated outcomes related to COVID-19. In addition, sex differences in the severity of COVID-19 might have an effect, as reported in previous studies.10–12 Future studies should consider investigating this.
Several limitations of this research have been identified that need to be further analyzed in future studies to determine why severe asthmatics were less likely to be hospitalized due to COVID-19. First, vaccination status and comorbidities were not analyzed as part of this study and may have been confounding variables, leading to differences in hospitalization rates. We believe future researchers should look at comorbidities. Second, our findings did not analyze the levels of various cytokines associated with the cytokine-release storm in COVID-19. Further, larger studies should evaluate how cytokine levels vary among asthmatics to confirm if prior treatment with biologics led to protective effects against SARS-CoV-2 infections. Lastly, our preliminary findings only analyzed absolute white blood cell counts and did not evaluate specific cell-type levels (eg CD4+ and CD8+), and thus future studies should assess if these cell-type levels vary among asthmatics infected with COVID-19 to better understand the effect of the TH2-cell inflammatory pathway as it relates to asthmatics.
Conclusion
Within our study, severe asthmatics had a lower likelihood of being hospitalized due to COVID-19 infections than asthmatics not requiring biologics. We believe the results of our study were likely due to enhanced preventive measures and immunosuppression leading to less severe COVID-19 infections among this cohort. Therefore, multicenter studies are needed to better account for variancing geography and hospital settings. More comprehensive studies also need be undertaken to account for differences among these patient populations when considering sex and comorbidity differences.
Data Sharing
All data related to this study are included in this letter. Data are available from the corresponding author upon reasonable request.
Author Contributions
All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis, interpretation, or all these areas, took part in drafting, revising, or critically reviewing the article, gave final approval to the version to be published, have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Reddel HK, Bacharier LB, Bateman ED, et al. Global initiative for asthma strategy 2021: executive summary and rationale for key changes. Am J Respir Crit Care Med. 2022;205(1):17–35. doi:10.1164/rccm.202109-2205PP
2. Sinha P, Matthay MA, Calfee CS. Is a “Cytokine Storm” Relevant to COVID-19? JAMA Intern Med. 2020;180(9):1152–1154. doi:10.1001/jamainternmed.2020.3313
3. Arias M, Oliveros H, Lechtig S, Bustos RH. Biologics in COVID-19 so far: systematic review. Pharmaceuticals. 2022;15(7):783. doi:10.3390/ph15070783
4. Heffler E, Detoraki A, Contoli M, et al. COVID‐19 in Severe Asthma Network in Italy (SANI) patients: clinical features, impact of comorbidities and treatments. Allergy. 2021;76(3):887–892. doi:10.1111/all.14532
5. Donlan AN, Mallawaarachchi I, Sasson JM, Preissner R, Loomba JJ. Dupilumab use is associated with protection from coronavirus disease 2019 mortality: a retrospective analysis. Clin Infect Dis. 2023;76(1):148–151. doi:10.1093/cid/ciac745
6. Sasson J, Donlan AN, Ma JZ, et al. Safety and efficacy of dupilumab for the treatment of hospitalized patients with moderate to severe coronavirus disease 2019: a phase 2a trial. Open Forum Infect Dis. 2022;9(8):ofac343. doi:10.1093/ofid/ofac343
7. Yan B, Yang J, Xie Y, Tang X. Relationship between blood eosinophil levels and COVID-19 mortality. World Allergy Org J. 2021;14(3):100521. doi:10.1016/j.waojou.2021.100521
8. Akenroye A, Lassiter G, Jackson J, et al. Effectiveness of mepolizumab, benralizumab, and dupilumab in eosinophilic asthma: a Bayesian network meta-analysis. J Allergy Clin Immunol. 2022;149(2):AB147. doi:10.1016/j.jaci.2021.12.496
9. Jackson DJ, Busse WW, Bacharier LB, et al. Association of respiratory allergy, asthma, and expression of the SARS-CoV-2 receptor ACE2. J Allergy Clin Immunol. 2020;146(1):203–206.e3. doi:10.1016/j.jaci.2020.04.009
10. Cruz R, Diz-de Almeida S, López de Heredia M, et al. Novel genes and sex differences in COVID-19 severity. Hum Mol Genet. 2022;31(22):3789–3806. doi:10.1093/hmg/ddac132
11. Kalidhindi RSR, Borkar NA, Ambhore NS, Pabelick CM, Prakash YS, Sathish V. Sex steroids skew ACE2 expression in human airway: a contributing factor to sex differences in COVID-19? Am J Physiol Lung Cell Mol Physiol. 2020;319(5):L843–7. doi:10.1152/ajplung.00391.2020
12. Takahashi T, Ellingson MK, Wong P, et al. Sex differences in immune responses that underlie COVID-19 disease outcomes. Nature. 2020;588(7837):315–320. doi:10.1038/s41586-020-2700-3
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Characterization of Patients in the International Severe Asthma Registry with High Steroid Exposure Who Did or Did Not Initiate Biologic Therapy
Chen W, Sadatsafavi M, Tran TN, Murray RB, Wong CBN, Ali N, Ariti C, Garcia Gil E, Newell A, Alacqua M, Al-Ahmad M, Altraja A, Al-Lehebi R, Bhutani M, Bjermer L, Bjerrum AS, Bourdin A, Bulathsinhala L, von Bülow A, Busby J, Canonica GW, Carter V, Christoff GC, Cosio BG, Costello RW, FitzGerald JM, Fonseca JA, Yoo KH, Heaney LG, Heffler E, Hew M, Hilberg O, Hoyte F, Iwanaga T, Jackson DJ, Jones RC, Koh MS, Kuna P, Larenas-Linnemann D, Lehmann S, Lehtimäki LA, Lyu J, Mahboub B, Maspero J, Menzies-Gow AN, Sirena C, Papadopoulos N, Papaioannou AI, Pérez de Llano L, Perng DW, Peters M, Pfeffer PE, Porsbjerg CM, Popov TA, Rhee CK, Salvi S, Taillé C, Taube C, Torres-Duque CA, Ulrik CS, Ra SW, Wang E, Wechsler ME, Price DB
Journal of Asthma and Allergy 2022, 15:1491-1510
Published Date: 21 October 2022
Asthma and COVID-19 Outcomes: A Prospective Study in a Large Health Care Delivery System

Finkas LK, Ramesh N, Block LS, Yu BQ, Lee MT, Lu M, Skarbinski J, Iribarren C
Journal of Asthma and Allergy 2023, 16:1041-1051
Published Date: 26 September 2023
Adult Severe Asthma Registries: A Global and Growing Inventory
Cushen B, Koh MS, Tran TN, Martin N, Murray R, Uthaman T, Goh CYY, Vella R, Eleangovan N, Bulathsinhala L, Maspero JF, Peters MJ, Schleich F, Pitrez P, Christoff G, Sadatsafavi M, Torres-Duque CA, Porsbjerg C, Altraja A, Lehtimäki L, Bourdin A, Taube C, Papadopoulos NG, Zsuzsanna C, Björnsdóttir U, Salvi S, Heffler E, Iwanaga T, al-Ahmad M, Larenas-Linnemann D, van Boven JF, Aarli BB, Kuna P, Loureiro CC, Al-lehebi R, Lee JH, Marina N, Bjermer L, Sheu CC, Mahboub B, Busby J, Menzies-Gow A, Wang E, Price DB
Pragmatic and Observational Research 2023, 14:127-147
Published Date: 20 October 2023
Multiple Biologics for Multiple T2 Diseases: A Pharmacoepidemiological Algorithm for Sorting Out Patients by Indication
Charriot J, Descamps V, Jankowski R, Maravic M, Bourdin A
Journal of Asthma and Allergy 2023, 16:1287-1295
Published Date: 29 November 2023
Real-World Biologic Use Patterns in Severe Asthma, 2015–2021: The CLEAR Study
Tran TN, Chen S, Emmanuel B, Altraja A, Bourdin A, Sheu CC, Tsai MJ, Hoyte FC, Quinton A, Cook B, Bulathsinhala L, Henley W, Goh CYY, Liu Y, Ariti C, Carter V, Price DB
Pragmatic and Observational Research 2025, 16:51-66
Published Date: 18 March 2025