Back to Journals » Journal of Pain Research » Volume 19
The Effect of ACT on Experiential Avoidance and Pain Acceptance: A Study on Women with Myofascial Pain Syndrome
Authors Yadollaee S ![]() , Zanjani Z, Alvani SR
, Zanjani Z, Alvani SR ![]() , Jalalati N
, Jalalati N
Received 9 February 2026
Accepted for publication 3 July 2026
Published 15 July 2026 Volume 2026:19 593631
DOI https://doi.org/10.2147/JPR.S593631
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor King Hei Stanley Lam
Sanaz Yadollaee,1 Zahra Zanjani,2 Seyed Reza Alvani,1 Nayyereh Jalalati3
1Department of Clinical Psychology, Faculty of Medicine, Kashan University of Medical Sciences, Kashan, Iran; 2Social Determinants of Health (SDH) Research Center, Kashan University of Medical Sciences, Kashan, Iran; 3Department of Physical Medicine and Rehabilitation, Faculty of Medicine, Kashan University of Medical Sciences, Kashan, Iran
Correspondence: Seyed Reza Alvani, Department of Clinical Psychology, Faculty of Medicine, Kashan University of Medical Science, Kashan, Iran, Email [email protected]
Purpose: Chronic pain can be considered one of the most serious medical problems worldwide due to the problems it causes in various aspects such as social and economic aspects. Myofascial pain syndrome is also known as a chronic pain-related disease. Considering the prevalence and importance of this disease, the present study aims to investigate the effectiveness of acceptance and commitment therapy on experiential avoidance and pain acceptance in people with myofascial pain syndrome.
Patients and Methods: The present study was a pre-test and post-test clinical trial with intervention and control groups. The population of this study included people with myofascial pain syndrome referred to the Shahid Beheshti Hospitals in Kashan in 2024. Through a purposive sampling method, 56 people were selected and randomly divided into two groups, namely, intervention (n = 28) and control (n = 28). In the intervention group, eight 90-minute sessions were conducted based on the acceptance and commitment therapy (ACT) protocol for chronic pain. The applied tools included the Experiential Avoidance Questionnaire (MEAQ) and the Pain Acceptance Questionnaire (CPAQ). Data were analyzed by SPSS using ANCOVA while controlling baseline scores.
Results: Participants receiving ACT showed a significant reduction in experiential avoidance compared with the control group, F(1,53) = 10.11, p = 0.002. Pain acceptance significantly increased in the intervention group, F(1,53) = 34.79, p < 0.001.
Conclusion: ACT can be considered as an effective therapeutic approach to reduce experiential avoidance and increase pain acceptance in patients with myofascial pain syndrome. These changes appear to be due to improved acceptance of thoughts and feelings associated with pain and reduce experiential avoidance, which is one of goal of ACT treatment.
Keywords: acceptance and commitment therapy, myofascial pain syndrome, experiential avoidance, pain acceptance
Introduction
Pain is one of the most common reasons individuals seek medical or psychological help.1 It is a subjective and unpleasant experience that serves as a protective signal against potential or actual tissue damage.2 In 2020, the International Association for the Study of Pain (IASP) updated its definition of pain as “an unpleasant sensory and emotional experience associated with, or resembling that associated with, actual or potential tissue damage”. The accompanying explanations emphasize that pain is a personal and multidimensional experience shaped by biological, psychological, and social factors; that pain is distinct from nociception; that individuals develop the concept of pain through life experiences; that the person’s own report should be respected; that pain, while often adaptive, can negatively affect functioning and well‑being; and that the inability to communicate does not preclude the presence of pain.3 Chronic pain is not merely acute pain persisting beyond three months; rather, it involves qualitative changes in cognition, emotion, and behavior that contribute to functional impairment and reduced well‑being.4
Myofascial pain syndrome (MPS) is a prevalent chronic pain condition involving muscles and surrounding connective tissues. It is characterized by trigger points, taut bands, and localized tenderness, with a lifetime prevalence of up to 85% in the general population.2,5 MPS arises from abnormal acetylcholine release at the motor endplate, leading to sustained muscle fiber contraction, ischemia, and the formation of taut bands.6 Despite its high prevalence, MPS is often underdiagnosed and inadequately treated.7,8 Current treatment options include pharmacological interventions—such as nonsteroidal anti‑inflammatory drugs, tricyclic antidepressants, muscle relaxants, local anesthetics, and botulinum toxin9–13 and non‑pharmacological interventions such as myofascial release, dry needling, acupuncture, transcutaneous electrical nerve stimulation, biofeedback, and trigger point injections.14–19 Given the biopsychosocial nature of chronic pain, combining psychological and medical interventions is essential.20,21
Experiential avoidance (EA) refers to attempts to escape or suppress unwanted internal experiences such as emotions, thoughts, memories, and bodily sensations.22 Although avoidance may provide temporary relief, it contributes to long‑term functional impairment and diminished quality of life.23,24 Pain acceptance, in contrast, involves reducing efforts to control or avoid pain and engaging in meaningful activities despite discomfort.25–27 Higher pain acceptance has been consistently linked to better psychological, social, and physical functioning in individuals with chronic pain.28
Acceptance and commitment therapy (ACT), a third‑wave cognitive‑behavioral therapy, aims to increase psychological flexibility through acceptance, mindfulness, and value‑based action.28 ACT has shown promising results in chronic pain populations, including Iranian samples29 and cancer pain trials.30 However, prior studies have important limitations, such as non‑random sampling,29 lack of standardized intervention protocols,30 or focus on other chronic pain populations rather than MPS. Based on existing evidence, no randomized clinical trial has specifically evaluated the effectiveness of ACT on experiential avoidance and pain acceptance in women with myofascial pain syndrome.
To address these gaps, the present study aimed to evaluate whether ACT reduces experiential avoidance and increases pain acceptance in Iranian women with MPS through a randomized clinical trial design.
Materials and Methods
Trial Design
The present study was a pre- and post-test clinical trial with intervention and control groups. The intervention group received ACT and was then been compared with patients in a waiting list (control group). The research population consisted of people with myofascial pain syndrome referred to Shahid Beheshti Hospitals in Kashan in 2024. Using a purposive sampling method, 56 people were selected and randomly assigned to the intervention (n = 28) and control groups (n = 28) using a random number table. They were motivated to participate in the program and willing to cooperate with the research team. Informed consent forms were obtained before the initial interview.
Selection of Participants
Inclusion criteria for the study are: 1) No history of severe psychiatric disorders (psychosis, delirium, cognitive disorders) or recent substance abuse, 2) No history of chronic pain due to severe arthritis, severe discopathy, rheumatological and infectious diseases, MS, and cancer, 3) Having myofascial pain syndrome as diagnosed by a physician for more than 3 months, 4) Having informed consent to participate in the study, 5) Having at least primary school education level, 6) Being aged 18 to 65 years (adult). The exclusion criteria included 1) The need for a change in the medication regimen, 2) More than two missed sessions, 3) Unwillingness to continue participation, 4) The onset of pain due to new underlying issues such as discopathy, rheumatological or infectious diseases, or musculoskeletal injuries during the screening period.
Sample Size Calculation
The sample size was determined based on previous studies investigating the efficacy of Acceptance and Commitment Therapy (ACT) in reducing pain intensity in women with chronic headache disorder.31
Procedure
In the pretest phase, all participants completed the Experiential Avoidance Questionnaire (MEAQ) and Pain Acceptance Questionnaire (CPAQ) questionnaires. After the treatment sessions ended, the MEAQ and CPAQ questionnaires were administered again. In the treatment group, participants received eight weekly 90-minute ACT sessions with a therapist, and in the control group, participants completed the MEAQ and CPAQ questionnaires at baseline and again after eight weeks (coinciding with the eight weekly sessions received by the intervention group) as a posttest.
Intervention: ACT
In the intervention group, a specialist therapist with a master’s degree in clinical psychology who had received formal training in ACT conducted acceptance and commitment therapy (ACT). The therapist received supervised training before the start of the trial. To ensure treatment fidelity and consistency, the supervisor, who reviewed session recordings and used the therapist adherence rating scale, conducted weekly supervision sessions. This process was implemented to enhance consistency between the therapist and adherence to the protocol. The treatment sessions were based on the Acceptance and Commitment Therapy (ACT) protocol by Hayes, Strosahl, and Wilson, conducted over 8 consecutive weeks in 90-minute sessions.32 A summary of the content of each session is presented in Table 1.
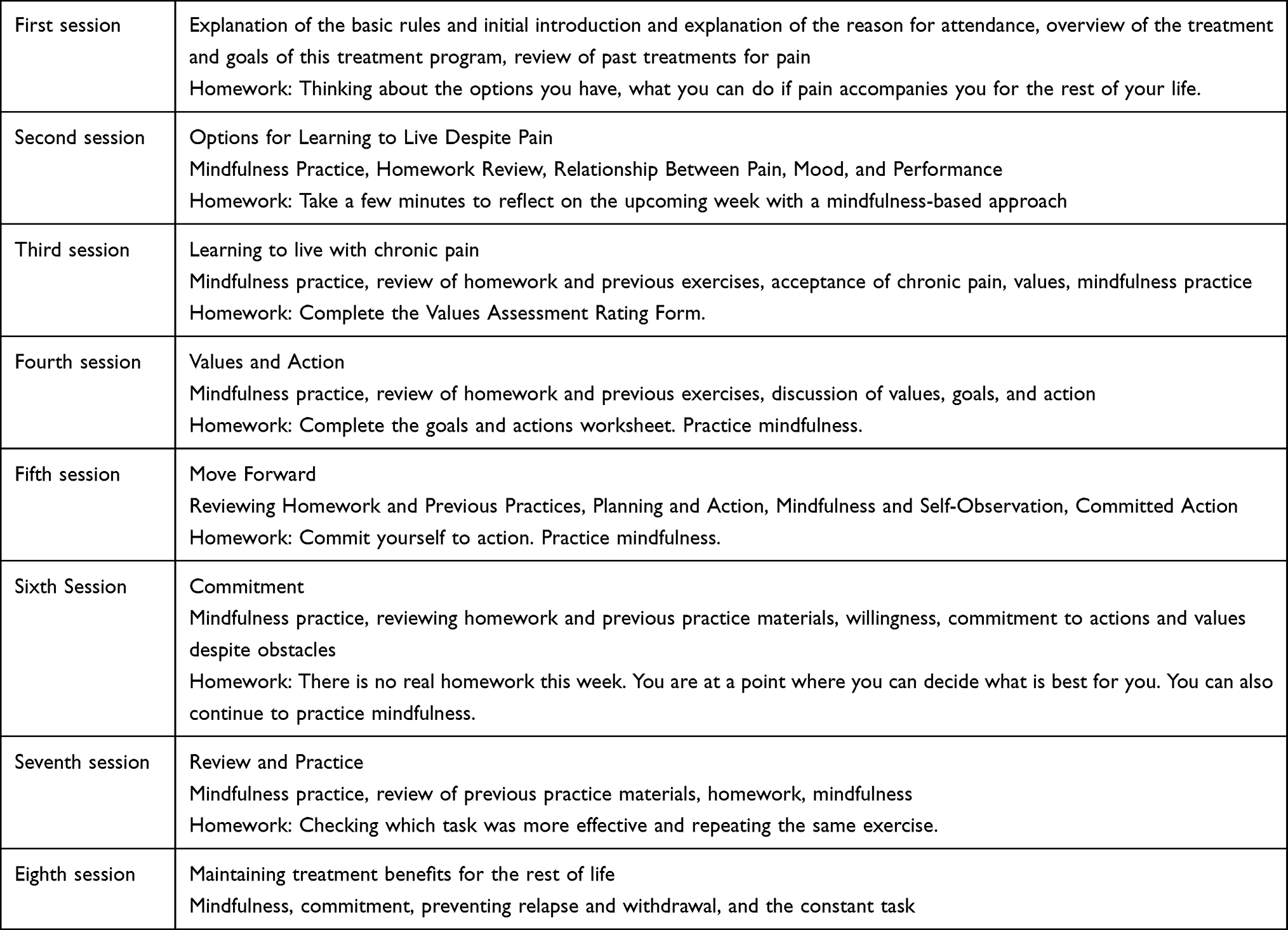 |
Table 1 ACT Intervention: Contents per Session |
Control Group
Individuals in the control group, like those in the intervention group, received their medication, exercise, and acupuncture treatments according to standard procedure, and the patients’ standard treatments were not changed. In the control group, individuals did not receive acceptance and commitment therapy.
Measures
Chronic Pain Acceptance Questionnaire (CPAQ)
The Chronic Pain Acceptance Questionnaire was developed in 2004 by McCracken and Vowles.33 This questionnaire has 20 items that are scored on a 7-point scale from 0 (Not at all true for you) to 6 (Always true for you). The Persian version of this tool, like its original version, assesses chronic pain acceptance in two subscales focusing on committed action (11 items) and reluctance to accept pain (9 items). In this scale, scores vary between 0 and 120, and higher scores indicate higher pain acceptance. For descriptive purposes, mean item scores were reported in Table 2 (total score divided by number of items). Mean item scores range from 0 to 6.
The instrument has good internal consistency, with a Cronbach’s alpha of 0.82 for committed action and 0.78 for pain acceptance. Moreover, a Cronbach’s alpha coefficient of 0.89 and a test-retest coefficient of 0.71 were reported in the evaluation of the psychometric properties of the Persian version of CPAQ.
Multidimensional Experiential Avoidance Questionnaire (MEAQ)
This questionnaire was designed by Gámez34 et al in 2011 to measure experiential avoidance and consists of 62 questions and 6 components: behavioral avoidance, confusion disgust, procrastination, distraction/stop, denial/repression, and distress tolerance. The Persian version of the questions are scored on a Likert scale from strongly disagree (1) to strongly agree (6). The minimum score is 62 and the maximum score is 372; higher scores indicate greater experiential avoidance. For descriptive purposes, mean item scores were reported in Table 2 (total score divided by number of items). For the MEAQ (62 items), mean item scores range from 1 to 6. Moradi et al35 reported The Cronbach’s alpha coefficient for total of the questionnaire 0.84, behavioral avoidance 0.89, confusion disgust 0.82, procrastination 0.79, distraction/stop 0.68, denial/repression 0.82, and for distress tolerance 0.81.
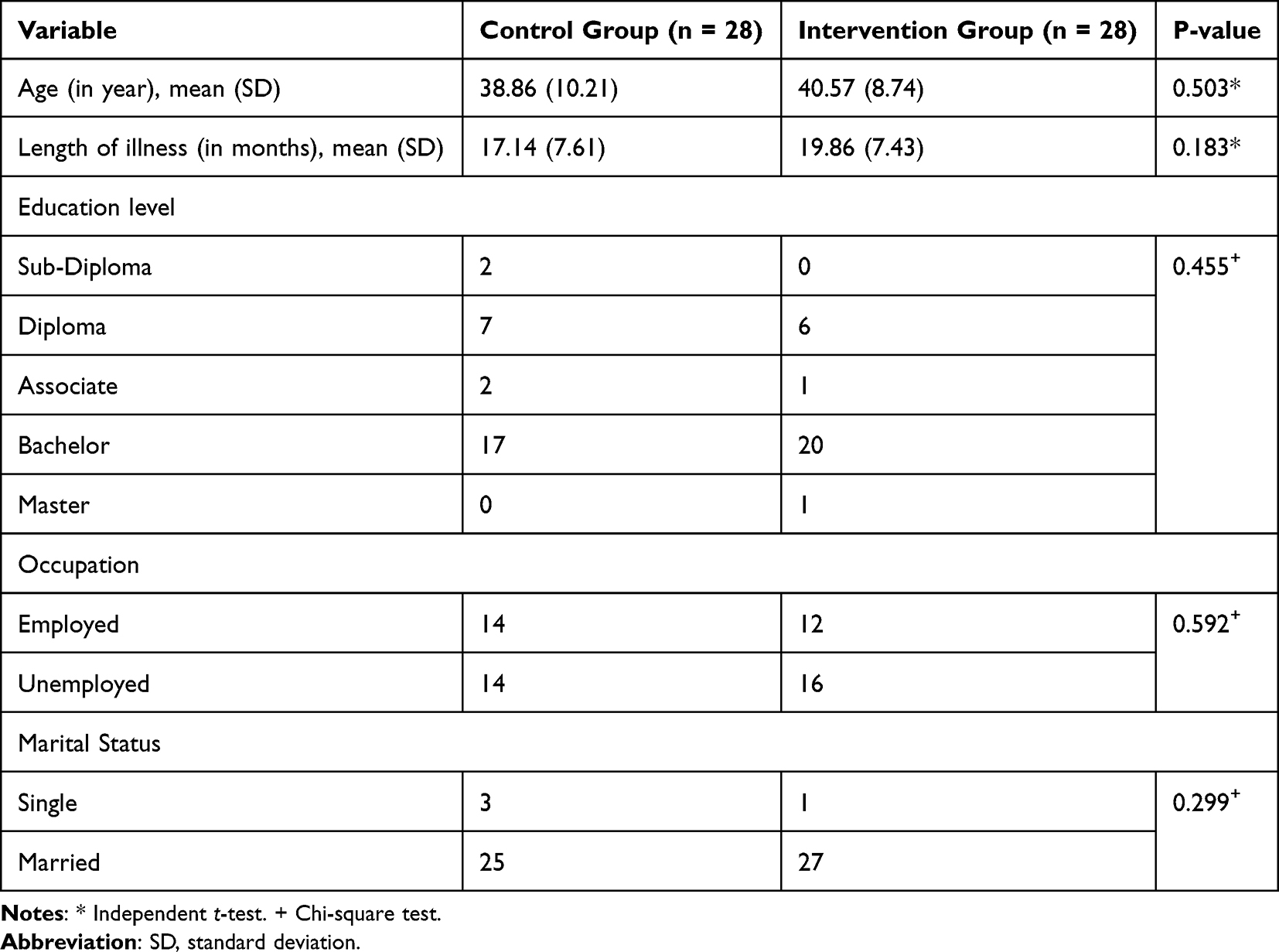 |
Table 2 Demographic Characteristics of the Study Groups |
Statistical Analysis
Initially, statistical evaluation of demographic information including mean, frequency, and standard deviation was performed. Subsequently, an Analysis of Covariance (ANCOVA) was performed using SPSS software version 27 to compare the groups, with a significance level of p = 0.05. To ensure the validity of this analysis, several key assumptions were assessed: the interval nature of the dependent variable was met, normality of the distribution of scores was confirmed through the Kolmogorov–Smirnov test, and the equality of variances between groups for the pre-test scores was examined using Levene’s test. Furthermore, participants were randomly assigned to the two groups, supporting the assumption of independence of observations. The use of ANCOVA allowed for the adjustment of post-test scores based on pre-test scores (covariate), providing a more precise estimate of the intervention’s effect.
Ethical Considerations
Before the study began, a consent form was distributed to all patients stating that the results and the names of the participants would remain anonymous and that their medical information would not be disclosed under any circumstances.
The present study was conducted by the Ethics Committee of Kashan University of Medical Sciences with the number IR. KAUMS. MEDNT. REC.1403.152 Approved. Informed written consent was obtained from all participants. The study was registered in the irct.ir database with IRCT20241105063611N1 registration number.
This study was conducted in accordance with the Declaration of Helsinki.
Results
In this study, 65 patients with myofascial pain syndrome were included. Table 3 presents the mean, standard deviation, and frequency distribution of demographic variables. Independent samples t‑tests showed no significant differences between the intervention and control groups in age or duration of illness. Likewise, chi‑square analyses indicated no significant group differences in education level, occupation, or marital status.
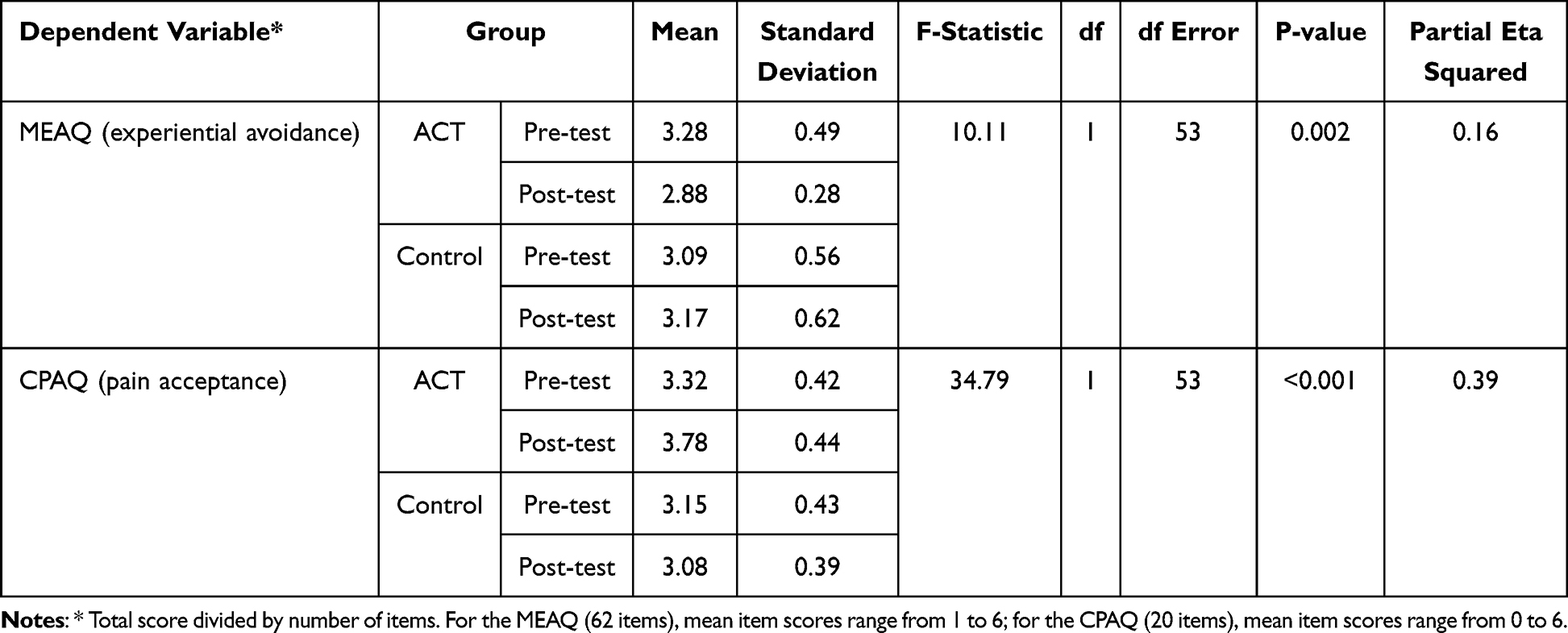 |
Table 3 Mean, Standard Deviation Values and ANCOVA Results for Experiential Avoidance and Pain Acceptance |
The descriptive statistics for experiential avoidance (MEAQ) and pain acceptance (CPAQ) in the pre‑test and post‑test phases are provided in Table 2. As shown, the intervention group exhibited a decrease in experiential avoidance from pre‑test (M = 3.28) to post‑test (M = 2.88), whereas the control group showed a slight increase (from M = 3.09 to M = 3.17). For pain acceptance, the intervention group demonstrated an increase from pre‑test (M = 3.32) to post‑test (M = 3.78), while the control group showed a small decrease (from M = 3.15 to M = 3.08).
To evaluate the effect of the intervention while controlling for pre‑test scores, one‑way ANCOVA was conducted for each outcome. The assumptions of ANCOVA—including independence of observations, normal distribution of the dependent variables (Kolmogorov–Smirnov test), and homogeneity of variances (Levene’s test)—were met.
The ANCOVA results indicated a significant group effect on experiential avoidance, (1, 53) = 10.11, p = 0.002, partial η2 = 0.16, showing that the intervention led to a greater reduction in experiential avoidance compared to the control group.
Similarly, a significant group effect was found for pain acceptance, F(1, 53) = 34.79, p < 0.001, partial η2 = 0.39, indicating that the intervention produced a greater increase in pain acceptance relative to the control condition.
Overall, these findings suggest that the observed reductions in experiential avoidance and increases in pain acceptance can be attributed to the intervention.
Discussion
This study was a clinical trial and included pre-test and post-test phases with a control group, which aimed to investigate the effectiveness of Acceptance and Commitment Therapy (ACT) on experiential avoidance and pain acceptance in people with myofascial pain syndrome. The findings of this study showed that Acceptance and Commitment Therapy (ACT) significantly reduces experiential avoidance in people with myofascial pain syndrome. This finding is consistent with the results of numerous studies on the effectiveness of ACT on experiential avoidance. For example, a meta-analysis by Hughes et al (2017) confirmed the effectiveness of ACT in reducing experiential avoidance across a wide range of psychological disorders.36
To explain this finding, we can refer to the theoretical mechanisms of ACT. Experiential avoidance is known as one of the main processes in the development and maintenance of psychopathology.37 Hayes et al (1996) defined experiential avoidance as the unwillingness to remain in contact with painful private experiences and the attempt to change the form, frequency, or sensitivity of these experiences.23 Patients with chronic pain often try to escape the experience of pain and the negative emotions associated with it by adopting avoidance strategies. Although these strategies may provide temporary relief in the short term, in the long term they lead to increased psychological distress and limitations in life activities.37 One of the techniques used in this study was mindfulness exercises, which were taught in each session. These exercises helped patients focus their attention on the present moment and distance themselves from automatic thought patterns and avoidance responses. A study by Arch and Craske (2006) showed that mindfulness can significantly reduce experiential avoidance and increase distress tolerance.38 In the context of chronic pain, experiential avoidance plays an important role in the persistence and exacerbation of pain. In their influential study, McCracken and Eccleston (2003) showed that experiential avoidance is a stronger predictor of disability in patients with chronic pain than the severity of the pain itself.39 Patients with myofascial pain often avoid physical activities, social situations, and even thoughts related to pain. This avoidance pattern can lead to decreased activity, loss of muscle strength, increased sensitivity to pain, and ultimately increased disability.40 The findings of this study also showed that (ACT) significantly increases pain acceptance in people with myofascial pain syndrome. This finding is consistent with the results of numerous studies on the effectiveness of ACT on pain acceptance. A meta-analysis by Martinez-Calderon et al (2024), which examined25 randomized studies, showed that ACT has a moderate to large effect on increasing pain acceptance in patients with chronic pain.41 A meta-analysis by Hughes et al (2017) also confirmed the effectiveness of ACT on increasing pain acceptance and showed that these effects were maintained at long-term follow-ups.36 To explain this finding, it is necessary to address the concept of pain acceptance and its role in chronic pain management. Pain acceptance refers to the willingness to experience pain without trying to reduce or avoid it while continuing to engage in valued life activities. McCracken et al (2004) showed in their classic study that pain acceptance has two main components: willingness to experience pain and engagement in activity.33 These two components are measured in the CPAQ questionnaire used in this study. One of the fundamental principles of ACT is the distinction between pain and suffering. Hayes et al (2006) explained this distinction: Pain is an unavoidable sensory experience that is part of human life, while suffering is the result of struggling with pain and trying to control it.42 Active participation in valued areas of life leads to improved medical and psychological outcomes.43 ACT helps patients accept pain as a sensory experience and not spend their energy futilely fighting it, but rather dedicating it to living a meaningful life. One of the key mechanisms through which ACT increases pain acceptance is the reduction of experiential avoidance. As seen in the explanation of experiential avoidance, ACT significantly reduced experiential avoidance. This reduction in experiential avoidance provides the basis for increased acceptance. McCracken and Vowles (2008) demonstrated in their longitudinal study that reduced experiential avoidance is a prerequisite for increased pain acceptance.44
This study’s limitations are the use of self-report tools, short intervention period, and the small sample size which may restrict the generalizability of the findings and increase the risk of overestimating effect sizes due to low statistical power. For future research, it is recommended to include a follow-up phase to assess the long term sustainability of the treatment effects. Moreover, comparing the ACT with other treatments could provide valuable insights into its relative effectiveness.
Conclusion
The results of this study clearly showed that ACT can significantly reduce experiential avoidance (12% reduction in mean score of post-test in comparison with pre-test) and increase pain acceptance (14% increase in mean score of post-test in comparison with pre-test) in ACT group. Through ACT patients are helped to accept and engage in behavior that incorporates their values, rather than fighting their thoughts and feelings. Therefore, clinicians working in health centers can use this treatment along with pharmacotherapy.
Data Sharing Statement
The detailed treatment protocol used in this research is available from the corresponding author upon reasonable request. Anonymized data will be shared after a written request is submitted to the corresponding author. Data will be available for sharing for one year following the publication of this study.
Acknowledgments
The authors are acknowledging all the participants and those who have cooperated in the design and conduct of the study. The authors would also like to thank Shahid Beheshti Hospital, Kashan University of Medical Science.
Funding
The Kashan University of Medical Sciences, vice chancellor for research and technology (GR-9599), financially supported this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mohammad Ali Asghari M. Handbook of Psychological Approaches to Pain Management.
2. Aredo JV, Heyrana KJ, Karp BI, Shah JP, Stratton P. Relating chronic pelvic pain and endometriosis to signs of sensitization and myofascial pain and dysfunction. Semin Reprod Med. 2017;35(1):088–9. doi:10.1055/s-0036-1597123
3. Pain international association for the study of. IASP announces revised definition of pain. IASP; 2020. Available from: https://www.iasp-pain.org/resources/terminology/#pain.
4. Brillhart D. Acceptance and commitment therapy. In: Individual Psychological Therapies in Forensic Settings. Routledge; 2017:11–27. doi:10.4324/9781315666136-2
5. Cao QW, Peng BG, Wang L, et al. Expert consensus on the diagnosis and treatment of myofascial pain syndrome. World J Clin Cases. 2021;9(9):2077–2089. doi:10.12998/wjcc.v9.i9.2077
6. Galasso A, Urits I, An D, et al. A comprehensive review of the treatment and management of myofascial pain syndrome. Curr Pain Headache Rep. 2020;24(8):43. doi:10.1007/s11916-020-00877-5
7. Fricton J. Myofascial pain. Oral Maxillofac Surg Clin North Am. 2016;28(3):289–311. doi:10.1016/j.coms.2016.03.010
8. Evcik D. Comparison of kinesiotaping, trigger point injection, and neural therapy in the treatment of acute myofascial pain syndrome: a randomized controlled study. Agri - J Turkish Soc Algol. 2024;36(4):134–141. doi:10.14744/agri.2022.39259
9. Hsieh LF, Hong CZ, Chern SH, Chen -C-C. Efficacy and side effects of diclofenac patch in treatment of patients with myofascial pain syndrome of the upper trapezius. Pain Symptom Manag. 2010;39(1):116–125. doi:10.1016/j.jpainsymman.2009.05.016
10. Annaswamy TM, De Luigi AJ, O’Neill BJ, Keole N. Emerging concepts in the treatment of myofascial pain: a review of medications, modalities, and needle-based interventions. Pm&r. 2011;3:940–961.
11. Haviv Y, Zini A, Sharav Y, Almoznino G, Benoliel R. Nortriptyline compared to amitriptyline for the treatment of per sistent masticatory myofascial pain. Oral Facial Pain Headache. 2018;33(1):7–13.
12. Huang-Lionnet JH, Hameed H, Cohen SP. Pharmacologic man agement of myofascial pain. In: Essentials Pain Medicine.
13. Firmani M, Miralles R, Casassus R. Effect of lidocaine patches on upper trapezius EMG activity and pain intensity in patients with myofascial trigger points: a randomized clinical study. Acta Odontol Scand. 2015;73(3):210–218. doi:10.3109/00016357.2014.982704
14. Ajimsha MS, Al-Mudahka NR, Al-Madzhar JA. Effectiveness of myofascial release: systematic review of randomized controlled tri als. Bodyw Mov Ther. 2015;19(1):102–112. doi:10.1016/j.jbmt.2014.06.001
15. Espejo-Antúnez L, Tejeda JFH, Albornoz-Cabello MR, et al. Dry needling in the management of myofascial trigger points: a systematic review of randomized controlled trials. Complementary Ther Med. 2017;33:46–57. doi:10.1016/j.ctim.2017.06.003
16. Wang R, Li X, Zhou S, Zhang X, Yang K, Li X. Manual acupuncture for myofascial pain syndrome: a systematic review and meta analysis. Acupunct Med. 2017;34(4):241–250.
17. Gibson W, Wand BM, Meads C, Catley MJ, O’Connell NE. Transcutaneous electrical nerve stimulation (TENS) for chronic pain- an overview of cochrane reviews. Cochrane Database Syst Rev. 2019. doi:10.1002/14651858.CD011890.pub2
18. Giggins OM, Persson UM, Caulfield B. Biofeedback in rehabilitation. J Neuroeng Rehabil. 2013;10(60):60. doi:10.1186/1743-0003-10-60
19. Robbins MS, Kuruvilla D, Blumenfeld A, et al. Trigger point injections for headache disorders: expert consensus methodology and narrative review. Headache. 2014;54:1441–1459.
20. Day MA. Mindfulness-Based Cognitive Therapy for Chronic Pain: A Clinical Manual and Guide. Hoboken John Wiley Sons; 2017.
21. Okifuji A, Ackerlind S. Behavioral medicine approaches to pain. Anesth Clin. 2007;25(4):709–719. doi:10.1016/j.anclin.2007.07.009
22. Hayes SC, Strosahl K, Wilson KG, et al. Measuring experiential avoidance: a preliminary test of a working model. Psychol Rec. 2004;54(4):553–578. doi:10.1007/BF03395492
23. Hayes SC, Wilson KG, Gifford EV, Follette VM, Strosahl K. Experiential avoidance and behavioral disorders: a functional dimensional approach to diagnosis and treatment. J Consult Clin Psychol. 1996;64(6):1152–1168. doi:10.1037/0022-006X.64.6.1152
24. Asadpour E, Veisi S. The effectiveness of acceptance and commitment therapy on marital satisfaction, sexual self-esteem and burnout martial among women with type 2 diabetes. J Arak Univ Med Sci. 2019;21(7):8–17.
25. Kashdan TB, Barrios V, Forsyth JP, Steger MF. Experiential avoidance as a generalized psychological vulnerability: comparisons with coping and emotion regulation strategies. Behav Res Ther. 2006;44(9):1301–1320. doi:10.1016/j.brat.2005.10.003
26. Moitra E, Stein MD, Busch AM, et al. Acceptance of chronic pain in depressed patients with HIV: correlations with activity, functioning, and emotional distress. AIDS Care. 2022;34(10):1338–1346. doi:10.1080/09540121.2021.1981819
27. Henriksson J, Wasara E, Rönnlund M. Effects of eight-week-web-based mindfulness training on pain intensity, pain acceptance, and life satisfaction in individuals with chronic pain. Psychol Rep. 2016;119(3):586–607. doi:10.1177/0033294116675086
28. Davoudi M, Omidi A, Sehat M, Sepehrmanesh Z. The effects of acceptance and commitment therapy on man smokers’ comorbid depression and anxiety symptoms and smoking cessation: a randomized controlled trial. Addict Heal. 2017;9(3):129.
29. Kandi M, Farokhzad P, Taheri A. Comparing the effectiveness of treatment based on acceptance and commitment and mindfulness therapy on chronic pain in People with drug addiction. Shenakht J Psychol Psychiatry. 2023;10(3):119–133. doi:10.32598/shenakht.10.3.119
30. Hadlandsmyth K, Dindo LN, Wajid R, Sugg SL, Zimmerman MB, Rakel BA. A single-session acceptance and commitment therapy intervention among women undergoing surgery for breast cancer: a randomized pilot trial to reduce persistent postsurgical pain. Psychooncology. 2019;28(11):2210–2217. doi:10.1002/pon.5209
31. Gharaei-Ardakani MA, Azadfallah P, Tavallaei APD. The effectiveness of acceptance and commitment therapy on pain experience in women with chronic pain. J Clin Psychol. 2012;4(2):39–51. doi:10.22075/jcp.2017.2087
32. Vowles KE, Sorrell JT. Life with chronic pain: an acceptance-based approach therapist guide and patient workbook. Clin Trials Res VA Palo Alto Heal Care Syst. 2016;18(2):33–37.
33. McCracken LM, Vowles KE, Eccleston C. Acceptance of chronic pain: component analysis and a revised assessment method. Pain. 2004;107(1):159–166. doi:10.1016/j.pain.2003.10.012
34. Gámez W, Chmielewski M, Kotov R, Ruggero C, Watson D. Development of a measure of experiential avoidance: the multidimensional experiential avoidance questionnaire. Psychol Assess. 2011;23(3):692–713. doi:10.1037/a0023242
35. Moradi A, Barghi Irani Z, Bagiyan Koulemarz MJ, Kariminejad K, Zabet M. Factor determination and psychometric features of the multidimensional experiential avoidance questionnaire (MEAQ). Soc Cogn. 2018;6(2):57–82.
36. Hughes LS, Clark J, Colclough JA, Dale E, McMillan D. Acceptance and commitment therapy (ACT) for chronic pain. Clin J Pain. 2017;33(6):552–568. doi:10.1097/AJP.0000000000000425
37. Chawla N, Ostafin B. Experiential avoidance as a functional dimensional approach to psychopathology: an empirical review. J Clin Psychol. 2007;63(9):871–890. doi:10.1002/jclp.20400
38. Arch JJ, Craske MG. Mechanisms of mindfulness: emotion regulation following a focused breathing induction. Behav Res Ther. 2006;44(12):1849–1858. doi:10.1016/j.brat.2005.12.007
39. McCracken LM, Eccleston C. Coping or acceptance: what to do about chronic pain? Pain. 2003;105(1–2):197–204. doi:10.1016/S0304-3959(03)00202-1
40. Vlaeyen JWS, Linton SJ. Fear-avoidance and its consequences in chronic musculoskeletal pain: a state of the art. Pain. 2000;85(3):317–332. doi:10.1016/S0304-3959(99)00242-0
41. Martinez-Calderon J, García-Muñoz C, Rufo-Barbero C, Matias-Soto J, Cano-García FJ. Acceptance and commitment therapy for chronic pain: an overview of systematic reviews with meta-analysis of randomized clinical trials. J Pain. 2024;25(3):595–617. doi:10.1016/j.jpain.2023.09.013
42. Hayes SC, Luoma JB, Bond FW, Masuda A, Lillis J. Acceptance and commitment therapy: model, processes and outcomes. Behav Res Ther. 2006;44(1):1–25. doi:10.1016/j.brat.2005.06.006
43. Ghorbani V, Zanjani Z, Omidi A, Sarvizadeh M. Efficacy of acceptance and commitment therapy (ACT) on depression, pain acceptance, and psychological flexibility in married women with breast cancer: a pre- and post-test clinical trial. Trends Psychiatry Psychother. 2021;43(2):126–133. doi:10.47626/2237-6089-2020-0022
44. McCracken LM, Vowles KE. A prospective analysis of acceptance of pain and values-based action in patients with chronic pain. Heal Psychol. 2008;27(2):215–220. doi:10.1037/0278-6133.27.2.215
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.