")
Back to Journals » International Journal of Women's Health » Volume 15
The Effect and Safety Assessment of Metformin and DLBS3233 (A Bioactive Fraction of Lagerstroemia speciosa and Cinnamomum burmannii) on Improving Metabolic Parameters in Women with Polycystic Ovary Syndrome
Authors Hidayat ST, Mulyantoro I, Damas S, Tjandrawinata RR
Received 7 March 2023
Accepted for publication 29 June 2023
Published 4 July 2023 Volume 2023:15 Pages 971—985
DOI https://doi.org/10.2147/IJWH.S409685
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Everett Magann
Syarief Thaufik Hidayat,1,2 Inu Mulyantoro,1,2 Suhartono Damas,3 Raymond R Tjandrawinata4
1Obstetric Gynecology Department, Faculty of Medicine, Diponegoro University, Semarang, Indonesia; 2Obstetric Gynecology Department, Dr. Kariadi Hospital, Semarang, Indonesia; 3Enviromental Health Department, Diponegoro University, Semarang, Indonesia; 4Research and Business Development, Dexa Laboratories of Biomolecular Science Research, Tangerang, Indonesia
Correspondence: Syarief Thaufik Hidayat, Department of Obgyn, Faculty of Medicine, Diponegoro University, Kariadi Hospital Semarang, Central Java, Jalan dr. Sutomo No. 16, Randusari, Kecamatan Semarang Selatan, Kota Semarang, Semarang, 50244, Indonesia, Tel +62 812 2924 346, Email [email protected]
Background: Polycystic ovary syndrome (PCOS) can lead to compensatory hyperinsulinemia with consequent metabolic abnormalities in women. In this study, DLBS3233 and Metformin were used to be tested. DLBS3233 itself is the new insulin-sensitizing drug, a combination-bioactive-fraction derived from two Indonesian herbals, Lagerstroemia speciosa and Cinnamomum burmannii. DLBS3233 alone and in combination with metformin were evaluated for efficacy and safety in insulin-resistant women with polycystic ovary syndrome (PCOS).
Methods: A randomized, double-blind, 3-arm, double-dummy, non-inferiority, and also a controlled clinical study was conducted at the Dr. Kariadi Hospital, Indonesia, between October 2014 and February 2019. The study involved 60 female subjects (with 20 female subjects in each group) that had polycystic ovary syndrome (PCOS).Treatment I consists of one placebo capsule twice per day and one 100 mg DLBS3233 capsule once per day. Treatment II consists of one placebo caplet once per day and one 750 mg Metformin XR caplet twice per day. Treatment III consists of one 750 mg Metformin XR caplet twice per day and one 100 mg DLBS3233 capsule once per day.
Results: In treatment I, the homeostatic model assessment for insulin resistance (HOMA-IR) levels were 3.55, 3.59, and 3.80 at pretest, 3 months, and 6 months after intervention, respectively. In treatment II, the HOMA-IR level were 4.00, 2.21, and 4.40 at pretest, 3 months, and 6 months after intervention respectively. In treatment III, the HOMA-IR levels were 3.30, 2.86, and 3.12 at pretest, 3 months, and 6 months after intervention, respectively. There was no apparent difference existed in the fasting plasma glucose (FPG), high-density lipoprotein (HDL), triglycerides, ferriman-gallwey scores (FGS), and safety assessment on vital signs and laboratory examinations (liver function and renal function) in all groups.
Conclusion: Either DLBS3233 alone or the DLBS3233/Metformin combination showed no significant efficacy and did not negatively affect cardiovascular function, liver and kidney function in PCOS subjects.
ClinicalTrials.gov Identifier: NCT01999686 Date: 3rd of December, 2013.
Keywords: homeostatic model assessment for insulin resistance, metabolic parameters, DLBS3233, metformin, polycystic ovary syndrome
Introduction
The most prominent endocrine condition affecting women is polycystic ovary syndrome (PCOS). This 5% to 10% of procreative women are affected by it. It can cause anovulation in 15% to 20% of infertile women.1–6 Hyperandrogenic characteristics, prolonged oligoanovulation, or polycystic ovarian morphology (PCOM) are used to define PCOS. But during the past 35 years, it has grown increasingly obvious that PCOS is also a major metabolic disorder associated with significant insulin action abnormalities and dysfunction of the pancreatic β-cell.7,8 A major risk factor for dysglycemia and Type 2 Diabetes Mellitus (T2DM) in women is PCOS. Instead of impaired fasting glucose, dysglycemia in PCOS often manifests as impaired glucose tolerance (IGT). Obesity, PCOS, and T2DM are frequent complex illnesses linked to reactive fasting hyperinsulinemia and insulin resistance.9
A powerful anabolic hormone, insulin, has a variety of impacts on numerous cell types. Insulin’s primary metabolic effects include increasing glucose absorption by skeletal muscle and fat cells, boosting skeletal muscle glycogen synthesis, limiting the creation of glucose in the liver, and preventing lipolysis in adipocytes.10 Although it is generally accepted that insulin’s primary target tissues are the liver, skeletal muscle, and adipose tissue, there is mounting evidence that insulin also serves critical physiological and biological roles in a variety of other tissues and cell types, including the brain, the heart, pancreatic beta-cells, and endothelial cells.11 Insulin sensitizers have been suggested as a potential treatment for this illness since insulin resistance and hyperinsulinemia have an important role in its pathophysiology.12,13 Consequently, improving insulin resistance with lifestyle changes or by taking a diabetes medication is part of the current PCOS treatment.14
Metformin, an oral biguanide insulin-sensitizing agent, is widely used in PCOS treatment. Metformin affects glucose production, peripheral glucose utilization, insulin levels, insulin receptors, significantly decreasing hepatic glucose production, fatty acid levels, and insulinemia. Moreover, metformin boosts the expression of the glucose transporter (GLUT-4), insulin receptor binding, intracellular glucose transport, and insulin receptor tyrosine kinase activity. It also increases peripheral glucose uptake and oxidative and non-oxidative glucose metabolism.15–18 Together, these effects may improve insulin resistance. However, up to 50% of people who use metformin experience gastrointestinal side symptoms like vomiting, diarrhea, and abdominal discomfort. Those with renal impairment should not use metformin.19–21 Patients with renal dysfunction receiving metformin therapy (as evidenced by reduced creatinine clearance) should be accompanied by close monitoring of renal function.22–24 Therefore, there is a necessity to find an alternative agent that is more tolerable for patients and effective in alleviating insulin resistance in PCOS patients, thus improving pregnancy rates.5,25
The National Agency of Drug and Food Control, Republic of Indonesia, has approved the new insulin-sensitizing drug DLBS3233, which is presently being sold for the treatment of type 2 diabetes. DLBS3233 is a combination-bioactive-fraction generated from Lagerstroemia speciosa and Cinnamomum burmannii, two Indonesian herbs.26,27 PI-3-kinase (phosphatidylinositol-3-kinase), GLUT-4 (glucose transporter-4), Akt, PPAR-gamma, and PPAR-delta were all expressed at the mRNA level in 3T3 Swiss Albino preadipocyte cells as a result of DLBS3233, according to preclinical investigations. At the mRNA level, it also decreased the expression of the resistin gene and raised the expression of GLUT-4 and adiponectin.28 When DLBS3233 was administered to insulin-resistant Wistar rats, the levels of blood glucose, insulin, as well as triglycerides, total cholesterol, high-density lipoprotein, and low-density lipoprotein, were all found to be under control. Studies on teratogenicity, subchronic poisoning, and toxic effect have validated the reliability of DLBS3233.29
Based on the pharmacological activities of DLBS3233, known to improve insulin-signal transduction sensitivity, DLBS3233 may also benefit women with PCOS.27,30 So far, there are no studies investigating the application of DLBS3233 to PCOS treatment. Therefore, in this study, DLBS3233 and its comparator (Metformin XR) will be used as a single pharmacological therapy on top of a lifestyle modification intervention.31
Materials and Methods
A randomized, double-blind, 3-arm, double-dummy, non-inferiority and also a controlled clinical study was conducted from October 2014 until February 2019 at the Kariadi Hospital, Semarang. Participants were recruited using consecutive sampling and were randomly allocated by a third party to prevent bias and produce high internal validity. To maintain a double-blind procedure, we used double dummies in this study. The inclusion criteria were women of reproductive age (18–40 years), wished to conceive, came to Kariadi Hospital, had body mass index (BMI) of 19 to 35 and a HOMA-IR of more than 2.00, had menstrual irregularity (cycles more than 35 days or no menses in the last of 3 months), had polycystic ovary shown by ultrasonography (USG), and consented to be included in this study.
The exclusion criteria covered pregnant or nursing women. The conditions causing hyperandrogenism were also excluded, such as congenital adrenal hyperplasia, Cushing syndrome, androgen-secreting tumors, hyperprolactinemia, uncontrolled thyroid disease, and any severe conditions like diabetes mellitus, uncontrolled hypertension, cardiovascular diseases, and impaired renal or liver function that could adversely impact the subject’s health or interrupt the study’s assessment.
The participants were divided into three treatment groups. The Treatment I group was given one 100 mg DLBS3233 capsule once per day and 1 Metformin XR placebo caplet twice per day. Treatment II group was given 1 DLBS3233 placebo capsule once per day and one 750 mg Metformin XR caplet twice per day. Treatment III group was given one 100 mg DLBS3233 capsule once per day and one 750 mg Metformin XR caplet twice per day. The investigational drug’s efficacy was assessed clinically at baseline and at one-month intervals. At the start of the trial, in the middle (month 3), and at the end (month 6), laboratory tests were done to assess the metabolic efficacy indicators. The designated nutritionist counseled the subjects on general lifestyle adjustments. Throughout their involvement in the study, all subjects adhered to behavioral, nutritional, and exercise programs that involved lifestyle adjustments. Every time a follow-up visit was made, the Investigator and Nutritionist evaluated how well the individuals had been doing with their lifestyle changes. These evaluations were especially thorough at the baseline, month 3, and month 6 of the study.
The primary efficacy endpoint was the metabolic parameter HOMA-IR decline from baseline at the study’s conclusion. The metabolic endpoints served as the secondary efficacy endpoints. (a. Lipid profile improvement from baseline, month 3, and final study results: levels of triglycerides, total cholesterol, HDL cholesterol, and LDL cholesterol. b. Development in glucose tolerance from baseline, month 3, and final study results: decreasing of 2-hour post-meal and fasting glucose levels c. A decrease in body mass index from the initial measurement and at each consecutive time point of assessment. d. Any variations in waist measurement from the initial measurement and at each consecutive time point of assessment. Vital signs were monitored at baseline and at each study visit, and safety inspections were assessed both at the beginning and completion of the trial. Throughout the study, adverse events were closely monitored. Vital signs (blood pressure, pulse rate, respiration rate), electrocardiography (ECG), Liver function: serum ALT, serum AST, serum alkaline phosphatase, Renal function: blood urea nitrogen (BUN), serum creatinine and adverse occurrences were tracked and observed during the assessment. For the liver function and renal function assessment, the blood sample taken will be mixed with their respective reagents and serum, and result can be read on photometer (in AST assessment, before mixing with the serum with sample and reagent, being incubated first for 10 minutes in 37° Celcius). For other laboratory parameters, the photometer was used to obtain the data, with added blood sample and the respective reagents. HOMA-IR result determined by the formula of fasting insulin in mU/L times fasting glucose in mg/dL, then divided by 405. And for the glucose assessment, the subjects must prepare before the blood sample taken by fasting (8 hours for FPG and 2 hours for 2h-PG).
IBM SPSS Statistics for Windows, version 20.0, was used to conduct the statistical analysis. Descriptive statistics were used to tabulate and summarize the demographic data and baseline traits of the study population. After 6 months of treatment, the improvement (reduction) in HOMA-IR in subjects receiving DLBS3233 was not non-inferiority if the estimated 95% upper confidence limit of the difference between groups was below 0.5 points. Vital signs and all laboratory examinations at each visit were descriptively summarized in the table of means. The parameters at the end of the study were observed between groups by analysis of variance (ANOVA). To correspond to the underlying distributional assumptions of the statistical models, the variables required log transformations. Alternatively, the matching non-parametric test was applied. At a significance threshold of 0.05, every statistical analysis was conducted. Kariadi Hospital Ethics Committee gave their approval for this study.
Results
There were 70 subjects who fulfilled the inclusion criteria. Three treatment groups for the subjects were assigned at random. Subjects were given the 100 mg DLBS3233 capsule once per day and 1 Metformin XR placebo caplet twice per day, the DLBS3233 placebo capsule once per day and one 750 mg Metformin XR caplet twice per day, and the 100 mg DLBS3233 capsule once per day and one 750 mg Metformin XR caplet twice per day, according to their treatment groups. A total of 10 subjects dropped out of the study (Figure 1). Seven subjects were not followed up on, one subject relocated, and two subjects felt the duration of treatment was too long. There were 60 subjects available for analysis in total, divided into 20 subjects in each group.
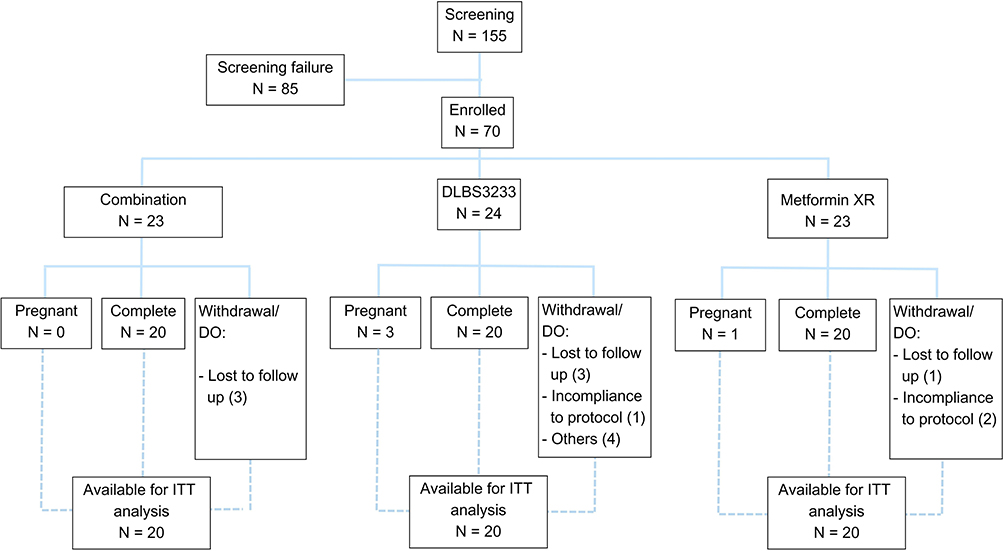 |
Figure 1 Flow of study. |
The mean ages were 27.40 ± 2.44 years in the combination group, 28.60 ± 4.63 years in the DLBS3233 group, and 27.80 ± 2.55 in the metformin group. More than 75% of the subjects were obese. Ferriman-Gallwey scores in the three groups were 7.85 ± 2.54, 9.85 ± 3.03, and 9.25 ± 1.33, respectively. The mean baseline HOMA-IR in the three groups were 3.30 ± 1.14, 3.55 ± 1.09, and 4.00 ± 1.78, respectively. The characteristics of the groups did not significantly differ from one another (Table 1). Despite substantial contrasts between the groups for 2h-PG and total cholesterol at baseline, meaningful differences were often not detected in a statistically significant manner. Table 2 shows the results of both tests comparing HOMA-IR reductions from baseline in all subjects. Meanwhile, Table 3 displays the result of between- and within-group analysis of the HOMA-IR absolute value. Figure 2 plots the absolute value of HOMA-IR at each time point for each group.
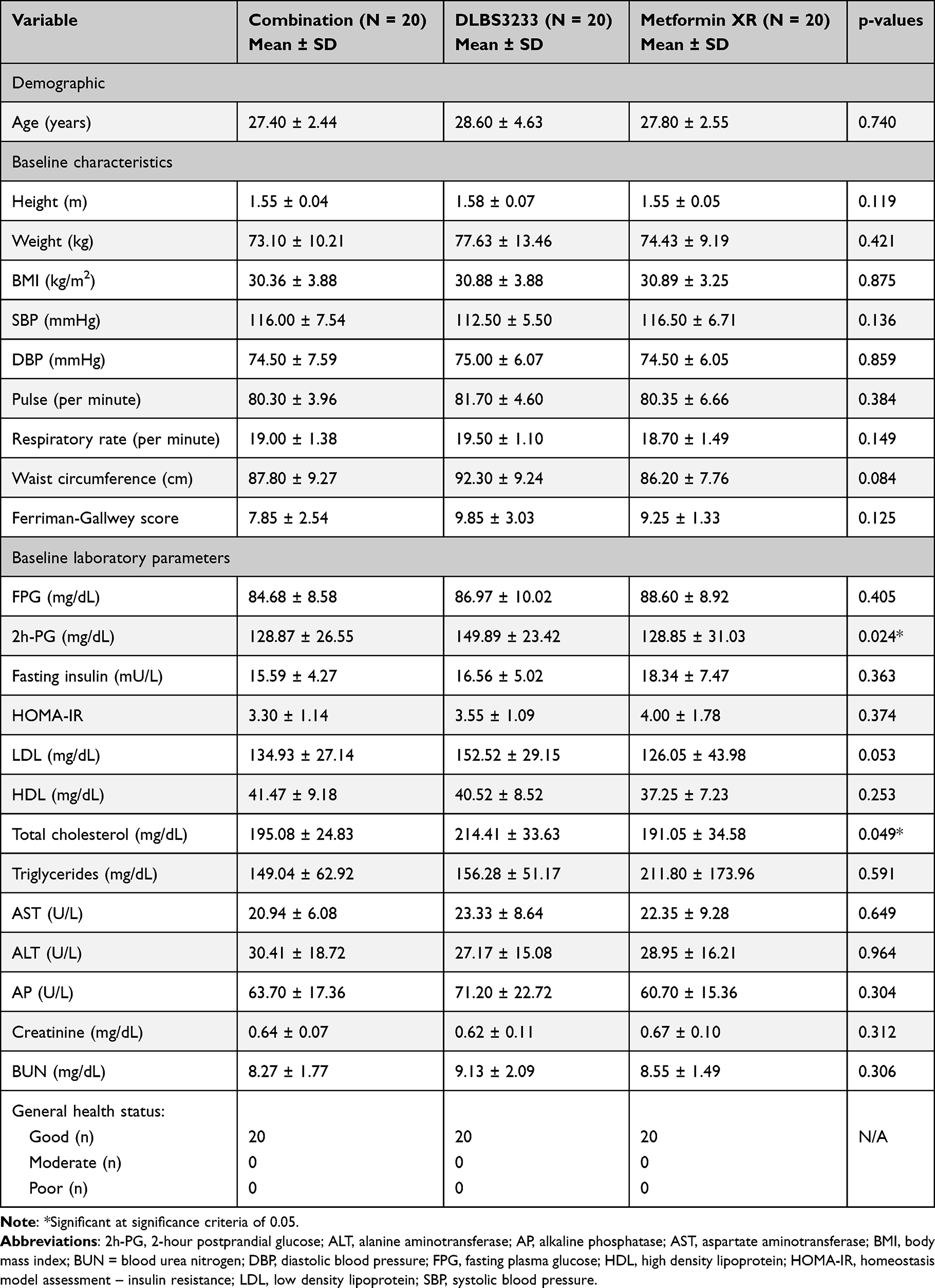 |
Table 1 Demographics and Biochemical Characteristics |
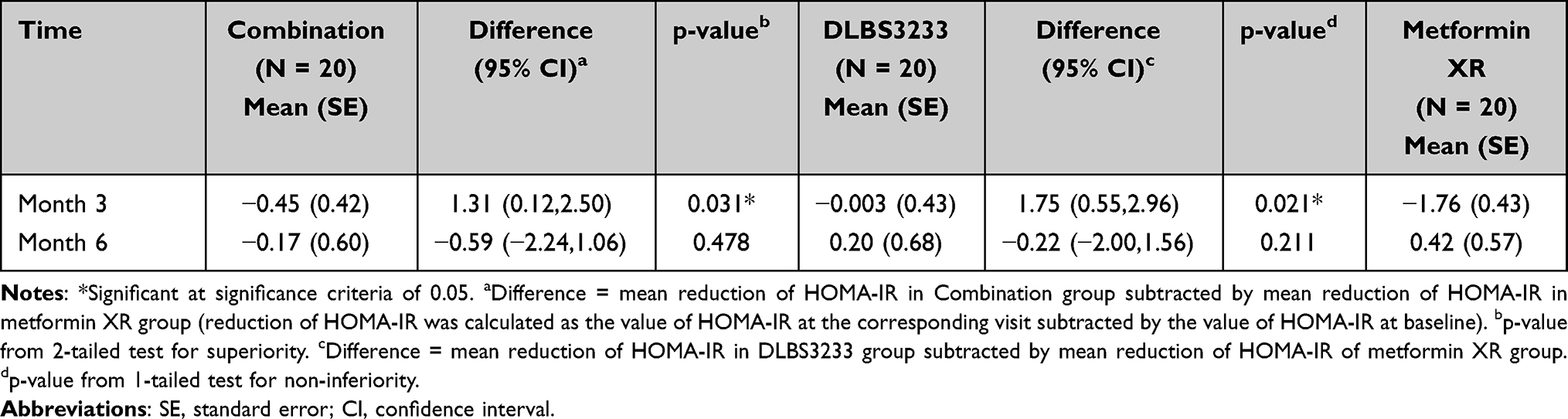 |
Table 2 Test of Primary Efficacy Endpoint: the Improvement (Reduction) of HOMA-IR from Baseline |
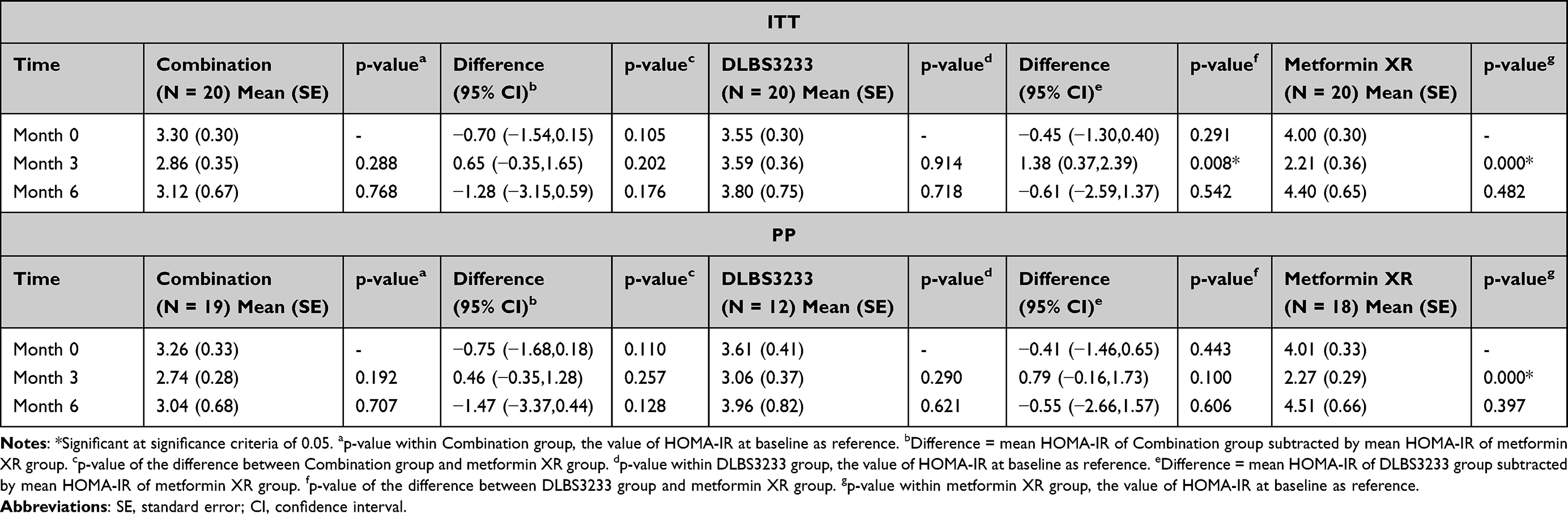 |
Table 3 Comparison of HOMA-IR Value Between- and Within-Group |
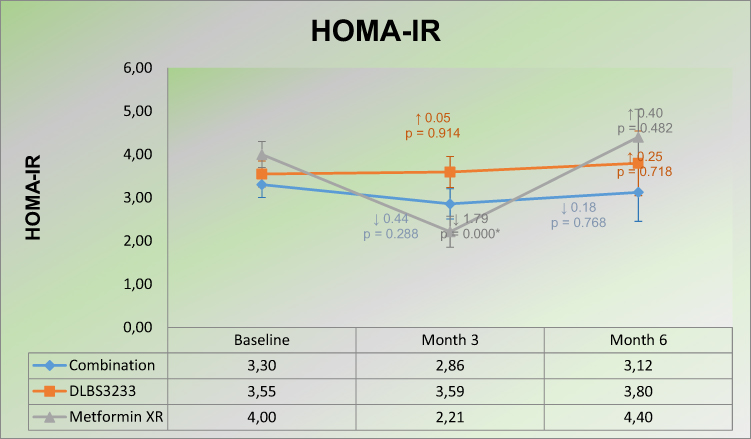 |
Figure 2 Absolute values of HOMA-IR at each time point. |
However, the trend observed in the 3rd and 6th months was different. In the earlier time point, reductions in HOMA-IR were surprisingly lower in the combination group than in the control (Metformin XR) group. It reversed in the latter time point, though superiority was not proven. As for the non-inferiority hypothesis, the 95% CI of the difference included zero and a delta of 0.5 points (non-inferiority margin), showing that no significant difference existed between the groups; however, the result regarding non-inferiority was inconclusive. The disagreement in these results was only observed in the 3rd-month time-point in the ITT set, whereby HOMA-IR improvement was noticeably better in the control group (Table 2). The absolute values of HOMA-IR at each time point in either the combination or the DLBS3233 group were not notably different from the Metformin XR group, respectively. When compared to the value at baseline, the HOMA-IR value in the Metformin XR group was considerably lower three months after the treatment, but it bounced back afterward. Finally, the HOMA-IR value in the DLBS3233 group seemed stable over time (Table 3, Figure 2). Metformin alone showed significant improvement at month 3, but these improvements could not be sustained (rebound effect). HOMA-IR rose again from month 3 to month 6. Single Inlacin also provided improvement, although the results were not significant. Meanwhile, when Metformin was combined with Inlacin, HOMA-IR was significantly improved after 3 and 6 months, suggesting the role of Inlacin in maintaining the improvement in insulin resistance by Metformin (resisting the rebound effect) in long-term Metformin use. These results show a long-term synergy between Inlacin and Metformin. Therefore, the improvement of HOMA-IR with the combination of Inlacin/Metformin after 6 months tends to be superior to Metformin alone.
Table 4 presents the values of each variable at each time point. These values were also compared between groups and within-group. The outcomes referred to the improvement (reduction or increase) of each variable at each time point in contrast to the baseline value.
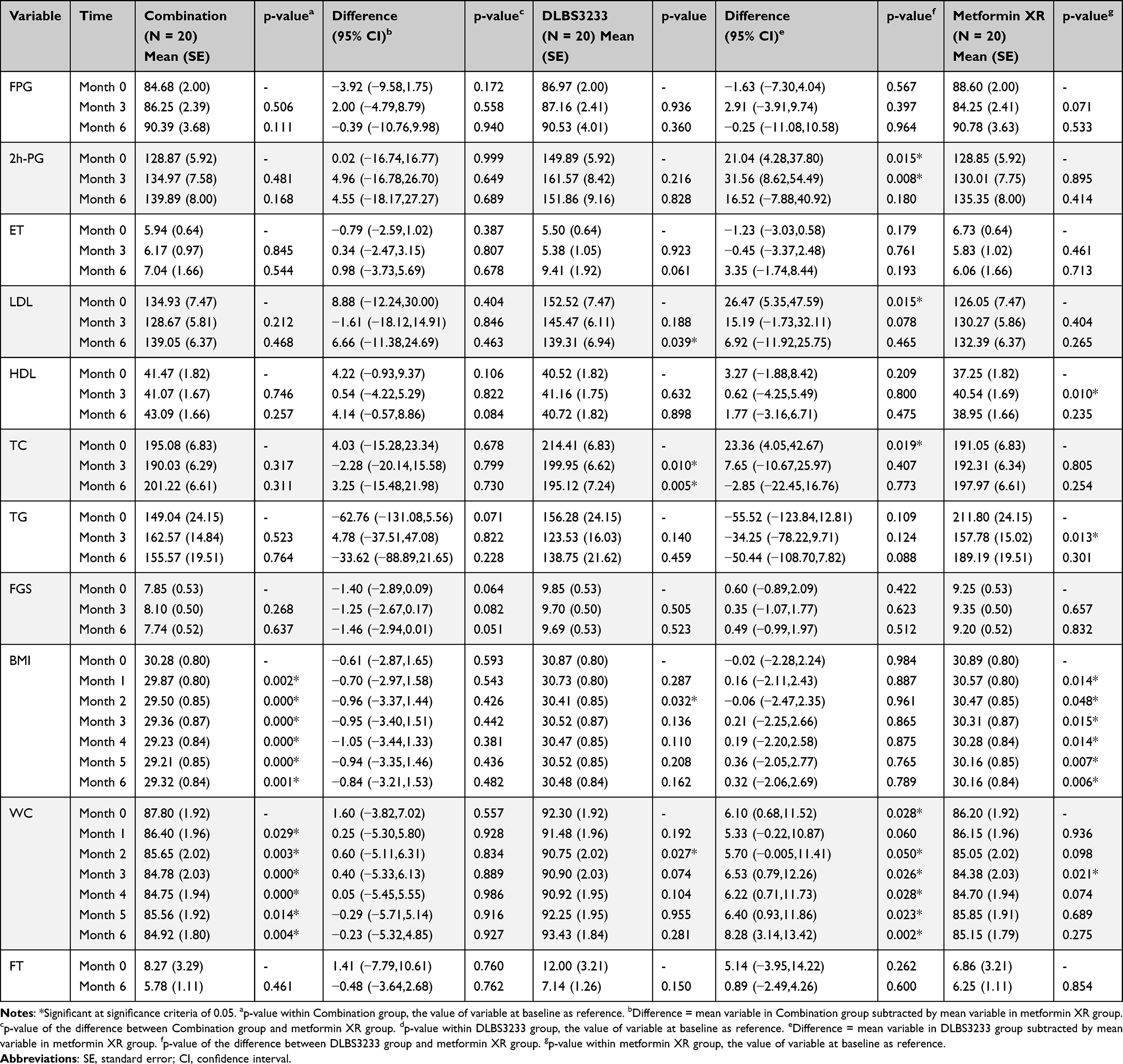 |
Table 4 Secondary Efficacy Endpoints: Comparison of the Absolute, Between- and Within-Group Values |
No noticeable difference was seen in the improvement of FPG in either the combination or the DLBS3233 group compared to the Metformin XR. The value of FPG in both treatment groups slightly increased over time, while it decreased in the 3rd month in the control group before increasing again in the 6th month. The value of 2h-PG in the combination and the Metformin XR group tended to increase after treatment, although no significant within-group analysis was observed. It was also observed that the 2h-PG value in the DLBS3233 had a considerably greater in the comparison to the control group at baseline and in the 3rd month, respectively (Table 4).
After a 6-month treatment period, DLBS3233 showed a substantial increase in LDL levels compared to the control group. The combination group’s LDL levels first dropped in the third month before rising afterwards, while levels consistently increased in the Metformin XR group. It was only the DLBS3233 group that succeeded in lowering LDL levels, leading to significant within-group analysis at the end of the study. Of note, significantly increased LDL values were found in the DLBS3233 group than the control group at baseline. A significant difference was found in the change in HDL in the 3rd month between the combination and the Metformin XR group, implying better results in the Metformin XR group. No significant within- and between-groups analysis was observed in all treatment groups; however, in the third month after treatment, a substantial change was seen in the Metformin XR group.
The change in total cholesterol was similar to that of LDL. Interestingly, the significant improvement in total cholesterol in the DLBS3233 group was evident since the 3-month treatment period. As for triglycerides, the DLBS3233 group’s pattern in changes matched that of the control group, where levels decreased in the 3rd month and then increased afterward. However, a significant reduction was found at 3 months in the Metformin XR group only. In contrast, in both groups, the triglycerides value in the combination group changed in the opposite direction, leading to a significant increase in the 3rd month versus the control group. The value of FGS in the DLBS3233 and the Metformin XR group was similar at each time point and in the combination group. However, the absolute value of FGS at each time points in this group, compared to the control group, was noticeably lower. The BMI and waist circumference measurements were conducted every month during the study period (Figure 3). Because there were more repeated measurements per subject, a compound symmetry structure was applied instead of the unstructured covariance matrix in the analysis of within- and between-groups comparison to prevent over-parameterization. Meanwhile, analysis on the improvement of the value was performed only in the 3rd and 6th months. BMI and waist circumference reductions did not differ significantly from one another at each time point between the combination and the DLBS3233 group, respectively, versus the Metformin XR group. Within-group analysis showed a consistent significant difference of BMI and waist circumference at each time point compared to baseline only in the combination group. It was also worth mentioning that the absolute values of waist circumference were considerably higher in the DLBS3233 group compared to the control (Metformin XR) group from baseline onward.
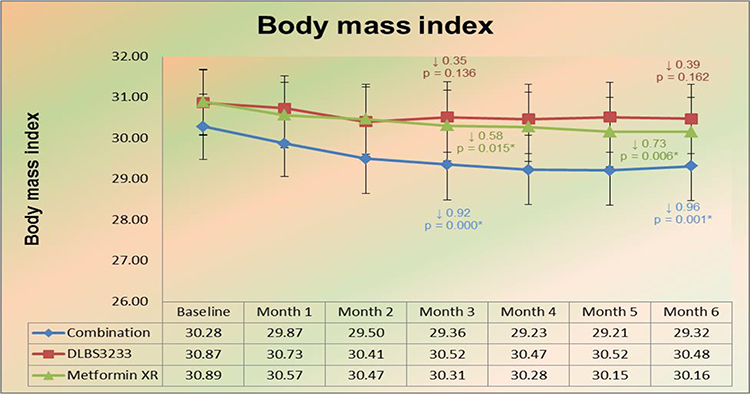 |
Figure 3 Absolute BMI values at each time point. |
DLBS3233, Metformin, and the combination of DLBS3233/Metformin reduced BMI and waist circumference. Safety assessment on vital signs and laboratory examinations (liver function and renal function) between groups were compared by ANOVA at the conclusion of the study, assuming normality (using either Kolmogorov–Smirnov or Shapiro–Wilk test) and equality of the variances. The results are displayed in Table 5.
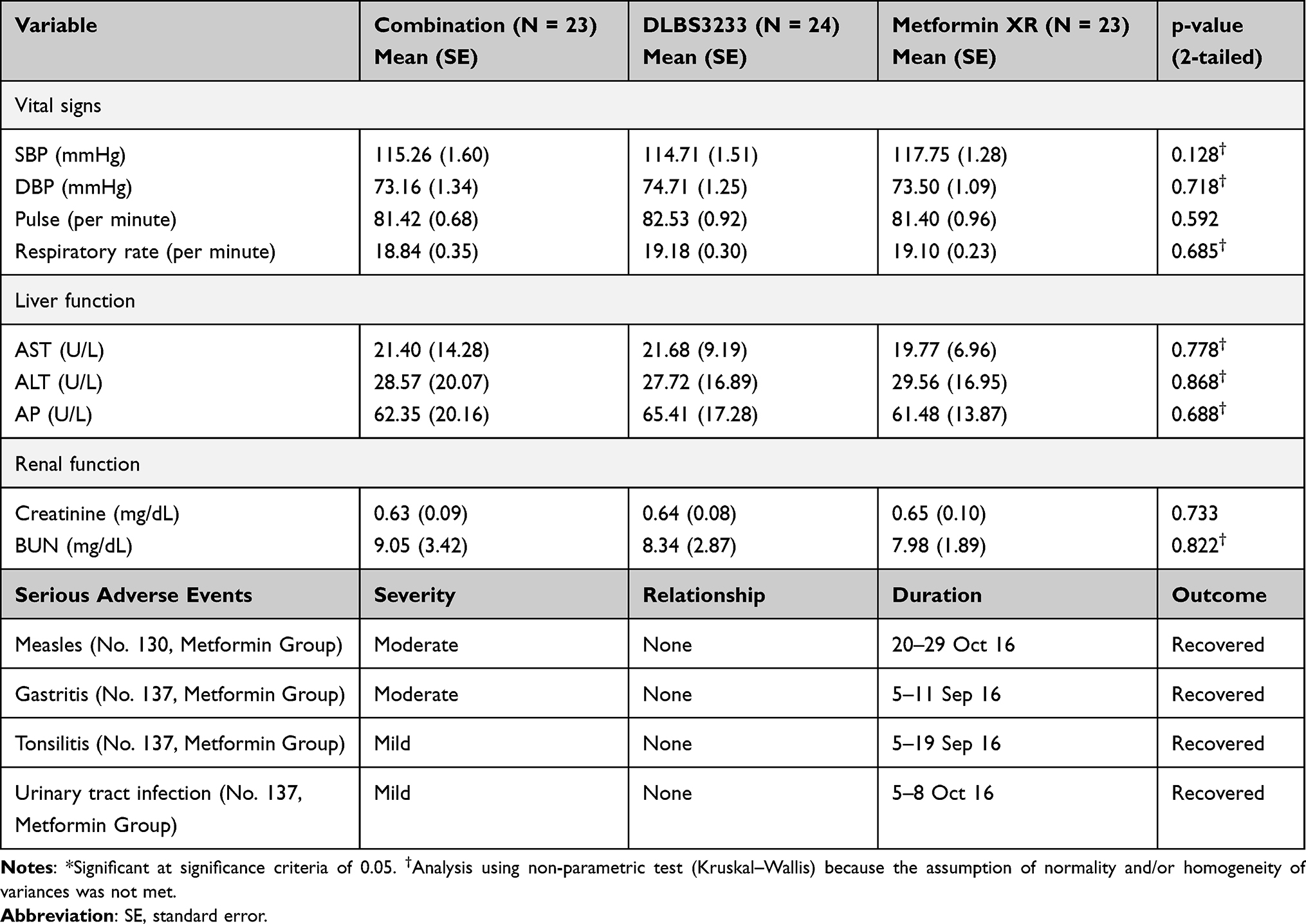 |
Table 5 Comparison of Safety Between Groups |
There was no significant difference in all safety parameters between the groups at the conclusion of the study. The values in all groups were considered normal clinically, suggesting that the treatments did not adversely affect any laboratory safety parameters. This result concludes the safety of DLBS3233 in PCOS subjects. Inlacin and the DLBS3233/Metformin combination did not negatively affect cardiovascular function, liver and kidney function in PCOS subjects.
Most adverse events were considered mild and unrelated to the investigational drug. There were two adverse events in the DLBS3233 group that were considered moderate but unrelated to the investigational drug: nausea (1 event) and diarrhea (1 event). In the Metformin XR group, these events were considered moderate and possibly/probably related to the drug use: appetite decreased (1 event), vomiting (1 event), diarrhea (1 event), and watery stools (1 event); while other events were moderate and unrelated to the investigational drug: gastritis (1 event), fever (1 event), and measles (1 event).
Several adverse events that were considered related to the treatment in the combination group were dizziness, vomiting, diarrhea, generalized weakness, shivering. In the DLBS3233 group, it was gastritis. In the Metformin XR group, subjects reported dizziness, decreased appetite, nausea, diarrhea, vomiting, watery stools, pounding heart, menorrhagia, generalized weakness, and shivering. Common adverse events experienced by subjects during the study included dizziness, nausea, general weakness, diarrhea, and bloating. Adverse outcomes were substantially less frequent in the Inlacin group. All adverse outcomes were tolerated well during the study.
Discussion
Lagerstroemia speciosa and Cinnamomum burmannii are two components of the standardized extract blend known as DLBS3233, which is thought to have anti-diabetic properties. According to earlier research, these extracts can help lower blood glucose levels. Preclinical research on DLBS3233 showed higher expression of genes linked to better insulin signaling and sensitivity, including PPARγ, PPARδ, phosphatidylinositol-3 kinase (PI3kinase), Akt, as well as GLUT4.26,28,32,33 Also, in comparison to control cells, this bioactive fraction considerably reduced resistin while significantly increasing glucose absorption and adiponectin secretion. Furthermore, DLBS3233 treatment improved levels of total cholesterol, triglycerides, HDL, and LDL lipoproteins, as well as blood glucose and insulin in Wistar breed rats with insulin resistance (Rattus norvegicus). Moreover, DLBS3233 reduced fasting blood sugar, insulin levels, and lipid profile more in combination with metformin or glimepiride. Hence, DLBS3233 is an excellent mixture of herbal extract with therapeutic uses for the treating T2DM and perhaps in the prevention of diabetes.
The GLUT4 gene expression was analyzed to find out how DLBS233 supports glucose transport. The concentration of DLBS3233 that most strongly induced GLUT4 expression in 3T3 cells was 5 μg/mL. When compared to control cells, the concentration increased GLUT4 expression by 1.9 times. According to this finding, DLBS3233 markedly enhanced GLUT4 expression, which in turn improved glucose absorption by cells. Moreover, both with and without the presence of insulin, the up-regulation of GLUT4 expression by DLBS3233 was contrasted with that of pioglitazone. The expression of GLUT4 was shown to be up to twice as high in response to DLBS3233 at a concentration of 5 μg/mL than the control, surpassing the effects of pioglitazone (1.25 times) and insulin alone (1.35 times).
In our study, the combination of DLBS3233 and metformin reduced plasma glucose levels, even though neither agent alone induced hypoglycemia in normoglycemic subjects. A number of glycemic indicators and lipid profiles were improved by the agent in earlier clinical studies examining its safety and effectiveness, it can be summarized that DLBS3233 is safe and effective in lowering blood glucose and improving other glycemic parameters in T2DM. In patients with metabolic syndrome, characterized by insulin resistance and dyslipidemia, DLBS3233 offers a possibility for better type-2-diabetes management by addressing the root of the problem rather than just treating the disease symptoms. Glycemic control improvement by DLBS3233 was also shown by the reduction of HbA1c level, observed after six weeks of treatment. However, as an insulin sensitizer, DLBS3233 showed little effect on 2 hour- PPPG in the study. Besides enhancing insulin sensitivity and glycemic control, DLBS3233 also showed additional benefits in improving the lipid profile. The DLBS3233 treatment in this study decreased levels of LDL cholesterol, triglycerides, and total cholesterol, but it appeared to have no effect on HDL cholesterol levels.26 Insulin-resistant pre-adipocytes and mature adipocytes uptake glucose at a considerably lower level than their non-insulin-resistant counterparts in the 3T3 fibroblast Swiss albino cells used in earlier animal research. Also, in comparison to those who are insulin-resistant, normal pre-adipocytes and adipocytes were observed to begin absorbing glucose earlier.28
Less than 5% of 3T3 insulin-resistant Swiss albino adipocyte cells could absorb glucose before therapy (control cells). The uptake ability was improved by up to four times, or around 20%, after treatment with DLBS3233. Thus, it is said that DLBS3233 to be just as effective as metformin at encouraging absorption of glucose.28,34,35 In a Phase 1 clinical trial, eligible participants were used to compare the safety of DLBS3233 to that of the active control, pioglitazone 30 mg, and the negative control.26 According to DLBS3233’s safety profile, the product was secure and quite well by fit, normoglycemic, and non-obese participants. The research showed that there was a very small chance that DLBS3233 would cause hypoglycemia and that the extract was both harmless and highly acceptable. Earlier research demonstrated the presence of novel active chemicals in the leaf extract of Lagerstroemia speciosa, which can activate tyrosine kinase, control glucose transport, and suppress adipogenesis. Recent research has shown that cinnamon extract has anti-diabetic impacts on type-2 diabetic people and db/db mice.36
Metformin plus DLBS3233 decreased the levels of plasma total cholesterol and triglycerides. However, the effect of metformin was rebound. The effect of DLBS3233 was consistent during the 6 months of treatment. The combination of DLBS3233/metformin attenuated the rebound effect of metformin. The effect of DLBS3233 (9mg/kg) on lipid profile compared with metformin (90mg/kg) and glimepiride (0.72mg/kg), regarded as the standard medication for diabetes mellitus, was investigated in the serum of rats with induced diabetes. According to the study, taking DLBS3233 once a day for two weeks caused a significant (p < 0.05) decrease in total cholesterol (17.12%) and triglycerides (47.72%) compared to diabetic control (induced-diabetic rats which were untreated). Total cholesterol, LDL cholesterol, and triglyceride levels were greatly decreased by DLBS3233, which also enhanced the lipid profile.28
Both treatment and their combination did not significantly affect LDL and HDL. Consistent with other lipid profiles, the profile of metformin effect on LDL seemed to rebound from month 3 to 6. The effect of DLBS3233 was consistent during the 6 months of treatment. DLBS3233 also lowered the fasting blood glucose, insulin level, and lipid profile when given together with metformin. In diabetic rats given metformin, fasting blood glucose reduced by 14.36%, total cholesterol by 17.66%, and triglycerides by 36.87%. In diabetic rats given both metformin and DLBS3233, fasting blood glucose was reduced by 18.16%, total cholesterol by 27.86%, and triglycerides by 50.99%. In diabetic rats given glimepiride, fasting blood glucose was reduced by 18.66% and total cholesterol by 12.41%.In diabetic rats given glimepiride and DLBS3233, fasting blood glucose was reduced by 24.24% and total cholesterol by 13.81%.28
Taken together, the results of the study showed that DLBS3233 can regulate levels of triglycerides, total cholesterol, high-density lipoprotein (HDL), low-density lipoprotein (LDL), and blood glucose, insulin, and other lipoproteins. Our study showed that DLBS3233, metformin, and the combination of DLBS3233/metformin reduced BMI and waist circumference. Weight increase was not a result of combining DLBS3233 with additional oral anti-diabetic medications. In a previous study, DLBS3233 influenced lipid metabolism via PPAR delta, and no body weight changes occurred.28
Edema was never reported by study participants, indicating safety for diabetic patients with heart failure who take DLBS3233. Moreover, acute toxicology, sub-chronic toxicology, chronic toxicology, and teratogenic studies also proved that DLBS3233 is safe and well-tolerated.
Conclusion
No apparent differences existed in the absolute value of HOMA-IR at each time point between the combination group and the Metformin XR group. Meanwhile, as comparison to the Metformin XR group, the HOMA-IR value in the DLBS3233 group was considerably greater in the third month. Within the combination group, the HOMA-IR value significantly decreased in the third month and sixth month, respectively. The HOMA-IR value in the DLBS3233 group was stable over time, showing no significant reduction at each time point. In the Metformin XR group, in the third month, the HOMA-IR value considerably decreased, but tended to increase after three months, showing no significant difference with the value at baseline.
In general, the improvement of each secondary endpoint compared to baseline for the combination group and the DLBS3233 group, respectively, was not significantly different during the 6-month study period. However, only in the DLBS3233 group, the value of triglycerides reduced stably, though it was only statistically significant at the third month in the ITT set of subjects. Another interesting remark was the analysis of the pregnancy rate, which showed higher odds of being pregnant when a subject was treated with either the DLBS323 or combination of DLBS3233 and the Metformin XR compared to Metformin XR alone, respectively.
Concerning the safety analysis, there was no significant difference in all safety parameters between groups at the conclusion of the study. All values of vital signs and laboratory examinations in both groups were considered normal clinically at each time point. Most adverse events were considered as mild and unrelated to the investigational drug.
Limitation of the Study
This study has two significant flaws that could be fixed in follow-up investigations. First, the sample size is relatively limited. Second, the lack of cooperation from some participants. By gathering more samples, the result expects to be more satisfactory.
Data Sharing Statement
The research data supporting the publication was available to all authors. The collection of data for the present work are not generally accessible but are available upon acceptable request to the corresponding author, Syarief Thaufik Hidayat.
Ethics Approval
This study was approved by the Ethical Committee of Kariadi Hospital. All participants agreed to participate in this study prior to trial. They provided informed consent. The current study was conducted in accordance with the Declaration of Helsinki. The information and data were encrypted and kept confidential.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Deswal R, Narwal V, Dang A, Pundir CS. The prevalence of polycystic ovary syndrome: a brief systematic review. J Hum Reprod Sci. 2020;13(4):261. doi:10.4103/jhrs.JHRS_95_18
2. Khan MJ, Ullah A, Basit S. Genetic basis of polycystic ovary syndrome (PCOS): current perspectives. Appl Clin Genet. 2019;12:249. doi:10.2147/TACG.S200341
3. Neven ACH, Laven J, Teede HJ, Boyle JA. A summary on polycystic ovary syndrome: diagnostic criteria, prevalence, clinical manifestations, and management according to the latest international guidelines. In: Seminars in Reproductive Medicine. Thieme Medical Publishers; 2018.
4. Deshpande PS, Gupta AS. Causes and prevalence of factors causing infertility in a public health facility. J Hum Reprod Sci. 2019;12(4):287. doi:10.4103/jhrs.JHRS_140_18
5. Group TEA-SPCW. Consensus on infertility treatment related to polycystic ovary syndrome. Human Reprod. 2008;23(3):462–477. doi:10.1093/humrep/dem426
6. Li Y, Chen C, Ma Y, et al. Multi-system reproductive metabolic disorder: significance for the pathogenesis and therapy of polycystic ovary syndrome (PCOS). Life Sci. 2019;228:167–175.
7. Diamanti-Kandarakis E, Dunaif A. Insulin resistance and the polycystic ovary syndrome revisited: an update on mechanisms and implications. Endocr Rev. 2012;33(6):981–1030. doi:10.1210/er.2011-1034
8. Dahan MH, Reaven G. Relationship among obesity, insulin resistance, and hyperinsulinemia in the polycystic ovary syndrome. Endocrine. 2019;64(3):685–689. doi:10.1007/s12020-019-01899-9
9. Torchen LC. Cardiometabolic risk in PCOS: more than a reproductive disorder. Curr Diab Rep. 2017;17(12):137. doi:10.1007/s11892-017-0956-2
10. LeRoith D, Taylor SI, Olefsky JM. Diabetes Mellitus: A Fundamental and Clinical Text. Lippincott Williams & Wilkins; 2004.
11. Muniyappa R, Sowers JR. Role of insulin resistance in endothelial dysfunction. Rev Endocr Metab Disord. 2013;14(1):5–12. doi:10.1007/s11154-012-9229-1
12. Soni A, Singla S, Goyal S. Polycystic ovary syndrome: pathogenesis, treatment and secondary associated diseases. J Drug Deliv Therap. 2018;8(5):107–112. doi:10.22270/jddt.v8i5.1892
13. Armanini D, Boscaro M, Bordin L, Sabbadin C. Controversies in the pathogenesis, diagnosis and treatment of PCOS: focus on insulin resistance, inflammation, and hyperandrogenism. Int J Mol Sci. 2022;23(8):4110. doi:10.3390/ijms23084110
14. Morgante G, Massaro M, Di Sabatino A, Cappelli V, De Leo V. Therapeutic approach for metabolic disorders and infertility in women with PCOS. Gynecol Endocrinol. 2018;34(1):4–9. doi:10.1080/09513590.2017.1370644
15. Song R. Mechanism of metformin: a tale of two sites. Diabetes Care. 2016;39(2):187–189. doi:10.2337/dci15-0013
16. Rena G, Pearson ER, Sakamoto K. Molecular mechanism of action of metformin: old or new insights? Diabetologia. 2013;56(9):1898–1906. doi:10.1007/s00125-013-2991-0
17. Agius L, Ford BE, Chachra SS. The metformin mechanism on gluconeogenesis and AMPK activation: the metabolite perspective. Int J Mol Sci. 2020;21(9):3240. doi:10.3390/ijms21093240
18. Sansome DJ, Xie C, Veedfald S, Horowitz M, Rayner CK, Wu T. Mechanism of glucose‐lowering by metformin in type 2 diabetes: role of bile acids. Diabetes Obes Metab. 2020;22(2):141–148. doi:10.1111/dom.13869
19. Altintas KZ, Dilbaz B, Cirik DA, et al. The incidence of metabolic syndrome in adolescents with different phenotypes of PCOS. Ginekol Pol. 2017;88(6):289–295. doi:10.5603/GP.a2017.0055
20. McCreight LJ, Bailey CJ, Pearson ER. Metformin and the gastrointestinal tract. Diabetologia. 2016;59(3):426–435. doi:10.1007/s00125-015-3844-9
21. Fatima M, Sadeeqa S, Nazir SUR. Metformin and its gastrointestinal problems: a review. Biomed Res. 2018;29(11). doi:10.4066/biomedicalresearch.40-18-526
22. Heaf J. Metformin in chronic kidney disease: time for a rethink. Peritoneal Dial Int. 2014;34(4):353–357. doi:10.3747/pdi.2013.00344
23. Tanner C, Wang G, Liu N, Andrikopoulos S, Zajac JD, Ekinci EI. Metformin: time to review its role and safety in chronic kidney disease. Med J Austr. 2019;211(1):37–42. doi:10.5694/mja2.50239
24. Holstein A, Stumvoll M. Contraindications can damage your health—is metformin a case in point? Diabetologia. 2005;48(12):2454–2459. doi:10.1007/s00125-005-0026-1
25. Penzias A, Bendikson K, Butts S; Medicine PCot ASfR. Role of metformin for ovulation induction in infertile patients with polycystic ovary syndrome (PCOS): a guideline. Fertil Steril. 2017;108(3):426–441. doi:10.1016/j.fertnstert.2017.06.026
26. Goswami PK, Khale A, Ogale S. Natural remedies for polycystic ovarian syndrome (PCOS): a review. Int J Pharm Phytopharmacol Res. 2012;1(6):396–402.
27. Wiweko B, Susanto CA. The effect of metformin and cinnamon on serum anti-mullerian hormone in women having PCOS: a Double-blind, randomized, controlled trial. J Hum Reprod Sci. 2017;10(1):31. doi:10.4103/jhrs.JHRS_90_16
28. Nailufar F, Tandrasasmita OM, Tjandrawinata RR. DLBS3233 increases glucose uptake by mediating upregulation of PPARγ and PPARδ expression. Biomed Prevent Nutr. 2011;1(2):71–78. doi:10.1016/j.bionut.2010.12.002
29. Tandrasasmita OM, Wulan DD, Nailufar F, Sinambela J, Tjandrawinata RR. Glucose-lowering effect of DLBS3233 is mediated through phosphorylation of tyrosine and upregulation of PPARγ and GLUT4 expression. Int J Gen Med. 2011;4:345. doi:10.2147/IJGM.S16517
30. Manaf A, Tjandrawinata RR, Malinda D. Insulin sensitizer in prediabetes: a clinical study with DLBS3233, a combined bioactive fraction of Cinnamomum burmanii and Lagerstroemia speciosa. Drug Des Devel Ther. 2016;10:1279. doi:10.2147/DDDT.S97568
31. Ehrmann DA, Liljenquist DR, Kasza K, et al. Prevalence and predictors of the metabolic syndrome in women with polycystic ovary syndrome. J Clin Endocrinol Metab. 2006;91(1):48–53. doi:10.1210/jc.2005-1329
32. Takada I, Makishima M. Peroxisome proliferator-activated receptor agonists and antagonists: a patent review (2014-present). Expert Opin Ther Pat. 2020;30(1):1–13. doi:10.1080/13543776.2020.1703952
33. Sheng X, Zhang Y, Gong Z, Huang C, Zang YQ. Improved insulin resistance and lipid metabolism by cinnamon extract through activation of peroxisome proliferator-activated receptors. PPAR Res. 2008;2008:1–9. doi:10.1155/2008/581348
34. Al-Snafi A. Medicinal value of Lagerstroemia speciosa: an updated review. Int J Curr Pharm Res. 2019;11(5):18–26. doi:10.22159/ijcpr.2019v11i5.35708
35. Orio F, Vuolo L, Palomba S, Lombardi G, Colao A. Metabolic and cardiovascular consequences of polycystic ovary syndrome. Minerva Ginecol. 2008;60(1):39–51.
36. Dash R, Lamia SS, Khan F, Sarah H, Islam SS. Phytochemistry and medicinal properties of Lagerstroemia speciosa (Lythraceae) extracts: a review. J Life Sci Rev. 2018;1:1–9.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.