")
Back to Journals » Clinical Interventions in Aging » Volume 18
The Effect and Possible Mechanism of Cardiac Rehabilitation in Partial Revascularization Performed on Multiple Coronary Artery Lesions
Authors Gao Y , Yue L , Miao Z , Wang F, Wang S , Luan B , Hao W
Received 22 November 2022
Accepted for publication 10 February 2023
Published 19 February 2023 Volume 2023:18 Pages 235—248
DOI https://doi.org/10.2147/CIA.S398732
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Yang Gao,1,* Ling Yue,2,* Zhilin Miao,1 Fengrong Wang,3 Shuai Wang,3 Bo Luan,1 Wenjun Hao1
1Department of Cardiology, The People’s Hospital of Liaoning Province, Shenyang, Liaoning Province, People’s Republic of China; 2Department of Ultrasound, The Fourth Affiliated Hospital of China Medical University, Shenyang, Liaoning Province, People’s Republic of China; 3Department of Cardiology, The First Affiliated Hospital of Liaoning University of Traditional Chinese Medicine, Shenyang, Liaoning Province, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wenjun Hao, Department of Cardiology, The People’s Hospital of Liaoning Province, NO. 33, Wenyi Road, Shenhe District, Shenyang, Liaoning Province, 110016, People’s Republic of China, Email [email protected]
Purpose: To observe the effect of cardiac rehabilitation (CR) in patients with partial revascularization performed on multiple coronary artery lesions and explore its possible mechanism.
Patients and Methods: A total of 400 patients with multiple coronary artery lesions were enrolled and randomly divided into a complete revascularization group and a CR group, with 200 cases in each group. Target lesion revascularization was performed radically in the complete revascularization group, while it was partially completed in the CR group, and postoperative CR was performed. All the patients were put under conventional treatment. Left ventricular end diastolic dimension (LVEDD), left ventricular ejection fraction (LVEF), 6-minute walking distance (6-MWD), quality-of-life scores, safety and levels of serum nitric oxide (NO), nitric oxide synthase (NOS), superoxide dismutase (SOD), and vascular endothelial growth factor (VEGF) were evaluated and compared between two groups before and after training.
Results: There was no significant difference in LVEDD, LVEF, 6-MWD, quality-of-life scores, levels of serum NO, NOS, SOD, and VEGF between two groups before training (p> 0.05). 1 year later, compared with the complete revascularization group, the occurrence of major adverse events in the CR group declined (p> 0.05); the measurements of LVEDD decreased and LVEF increased (p> 0.05), 6-MWD increased significantly (p< 0.05), quality-of-life scores were higher (p< 0.05), the levels of serum NO, NOS, and SOD increased noticeably, and the levels of serum VEGF decreased significantly in the CR group (p< 0.05). There were significant differences within the same group, before and after training (p< 0.05).
Conclusion: Cardiac rehabilitation training, not increase in the incidence of adverse events, is effective and safe after partial revascularization in patients with multiple coronary artery lesions, which has notable clinical advantages in promoting patients’ exercise endurance and quality-of-life by improving the nitric oxide synthase system and antioxidant system and reducing the level of VEGF.
Keywords: multiple coronary artery lesions, cardiac rehabilitation, coronary revascularization, 6-MWD, quality-of-life, NO/NOS
Introduction
At present, chronic diseases such as coronary heart disease (CHD) are still the leading cause of death in China and throughout the world.1 A large number of evidence-based medical studies have shown that cardiac rehabilitation can significantly reduce the days and cost of hospitalization, the mortality, and cardiovascular events in patients with CHD, which is a key measure when building a comprehensive prevention and treatment network for CHD.2,3 Studies showed that outpatient cardiac rehabilitation programmes could provide some substantive benefits for patients, such as convenience, fitness, improved functional capacity, quality-of-life, as well as lipid profile and blood pressure and endothelial function.3–5
Cardiac rehabilitation has been recognized as secondary prevention and effective treatment for CHD, which should be commenced as soon as possible after percutaneous coronary intervention (PCI) and continued after discharge, even needing to become a part of life to improve the quality-of-life.6 Left ventricle ejection fraction (LVEF) is a strong hemodynamic factor influencing the clinical outcome of patients with CHD.7 Reduced LVEF is associated with increased mortality in patients with ST-elevation myocardial infarction.8 It has been reported that nitric oxide (NO)-dependent vasodilation was impaired in patients with CHD and impaired NO-dependent vasodilation is an independent predictive factor of cardiac events in CHD patients.9 Aerobic exercise could improve LVEF and vascular endothelial dysfunction.10–12
Complete revascularization should be recommended to patients with multiple coronary artery lesions.13 Although there are many studies on cardiac rehabilitation in patients with multiple coronary artery lesions after PCI at home and abroad, it is reported that global access to cardiac rehabilitation is poor, with only 5–50% of eligible patients with cardiac disease receiving rehabilitation.14 Besides, complete revascularization for multiple coronary artery lesions may affect the anxiety and other emotional fluctuations about the effect of PCI and postoperative complications of the patients, to some extent. Furthermore, for multiple coronary artery lesions, complete revascularization is difficult to achieve due to the complexity of the lesion. In practice, there are a proportion of patients who choose partial revascularization, with many factors influencing the strategy selection, such as clinical characteristics, comorbidities of the patient, and reimbursement, etc.7 What’s more, there are few studies on cardiac rehabilitation and its related mechanisms in patients with partial revascularization performed on multiple coronary artery lesions.
In this context, compared with complete revascularization for multiple coronary artery lesions, the researchers proposed to perform cardiac rehabilitation on patients with multivessel coronary artery lesions who underwent partial revascularization and observe its efficacy and safety, and to explore the possibly protective mechanism of cardiac rehabilitation through the further determination of the levels of serum nitric oxide (NO), nitric oxide synthase (NOS), superoxide dismutase (SOD), and vascular endothelial growth factor (VEGF).
Patients and Methods
Sample Size
Through this study, we intend to test the hypothesis that the effect in the complete revascularization group and cardiac rehabilitation group would be comparable in improving cardiac function, 6-minute walking distance (6-MWD), quality-of-life, and biomarkers such as NO/NOS, SOD and VEGF, which were usually recorded at the baseline and 12th month. It has been found through calculation that the group samples of 336 patients (168 patients in each group) would provide 90% power to reject the null hypothesis of equal means at a two-sided alpha of 0.05. Given an anticipated dropout rate of 20% in this study, we initially planned to include 400 patients (200 in each group).
Patients
This was a randomized controlled single blind study. Four hundred patients with multiple coronary artery lesions treated by the the Heart Center of the people’s Hospital Of Liaoning Province from March 2017 to July 2021 were selected. Based on the inclusion and exclusion criteria, in accordance with a random number table, they were divided into a complete revascularization group and a cardiac rehabilitation group randomly, with 200 cases in each group. The complete revascularization group was the control group, while the partial revascularization & rehabilitation intervention group was the observation group. The whole process of the study is described in the flow chart in Figure 1. Baseline data were obtained from the patients before the study (Table 1). The patients’ underlying diseases and main medications after PCI are outlined in Table 1. The study was in accordance with the Declaration of Helsinki and approved by a local ethics committee, and all patients provided written informed consent. The authors had no access to any information that could identify individual participants during and after data collection.
 |
Table 1 Baseline Data of the Patients in Two Groups |
 |
Figure 1 Study design and flowchart. Abbreviations: LVEDD, left ventricular end diastolic dimension; LVEF, left ventricular ejection fraction; 6MWD, 6-min walk distance; MACE, major cardiac adverse events; NO, nitric oxide; NOS, nitric oxide synthase; SOD, superoxide dismutase; VEGF, vascular endothelial growth factor. |
Inclusion Criteria
1) Diagnosis of CHD according to the diagnostic criteria and coronary artery interventional therapy performed in accordance with the European Society of Cardiology guidelines;15 2) at least two coronary arteries (the left main, left anterior descending, left circumflex, and right coronary artery, with a target vessel diameter ≥2 mm) with ≥70% stenosis, with or without major branching lesions; 3) New York Heart Association functional class from grade I to II; 4) the ability to communicate well with the researchers and be open to rehabilitation training in this study; and 5) all selected patients were required to sign the informed consent form. The whole design of the study was in accordance with the requirements of the Declaration of Helsinki and approved by the ethics committee of the people’s Hospital Of Liaoning Province, China.
Exclusion Criteria
1) New York Heart Association functional class from grade III to IV; 2) complications of serious arrhythmia, hyperthyroid cardiopathy, congenital and idiopathic cardiomyopathy, valvular heart disease, cardiomyopathy, chronic obstructive pulmonary disease, cor pulmonale, idiopathic cardiomyopathy blood disorder, and autoimmune disease; 3) wearers of cardiac pacemakers and heart transplantation patients; 4) serious diseases of the liver, kidney, or other important organs; 5) pregnancy or lactation and family planning during trial period; 6) exercise intolerance or non-cardiac illness that might be aggravated by exercise; 7) mental illness; 8) poor compliance; 9) definitive diagnosis of malignancy; 10) surgery, trauma, gastrointestinal bleeding, or complications of PCI; and 11) refusal to sign the informed consent.
Methods
Complete Revascularization Group
Complete target lesion revascularizations were performed for the main target vessels. Postoperatively, to strictly and actively control the risk factors for CHD, coronary secondary prevention treatment, appropriate health advice, and important guidance on daily life were offered. We started a file on every selected case and called on or visited them weekly in the first 3 months and every month in the following 9 months. The whole process lasted 1 year. The outpatients were followed-up at 12 months and the relevant data was recorded.
Cardiac Rehabilitation Group
Cardiac rehabilitation is a complex form of intervention, which includes exercise training, physical activity promotion, health education, cardiovascular risk management, and psychological support, with personalized treatment to the individual needs of patients with a confirmed diagnosis of heart disease.14,16 In China, prescriptions for cardiac rehabilitation mainly include medication, exercise, nutrition, smoking cessation, and psychological management,17 as displayed in Table 2.
 |
Table 2 Cardiac Rehabilitation Components and FITT Parameters |
In this group, target lesion revascularization was partially completed. Postoperative control of risk factors of CHD, routine secondary preventive treatment of CHD, and appropriate exercise prescription for out-of-hospital rehabilitation were offered three times a week. Patients were instructed to conduct a telephone or door-to-door follow-up every week in the first 3 months and every month in the following 9 months and outpatient follow-up at 12 months and the data were recorded. The specific exercise prescriptions were in accordance with the FITT principle in this study, as described in Table 2.
The FITT Principle
The FITT principle refers to the components of exercise prescription, which involves frequency, intensity, time, and type.18
Frequency
After discharge, the average exercise prescription was 3–4 times a week.
Intensity
The intensity of exercise, assessed by heart rate, was formulated based on 6-minute walk test (6-MWT) with a wearable electrocardiogram and blood pressure monitor under professional instruction. Before discharge, 6-MWT was performed following the clinical practice guidelines with a continual electrocardiogram and blood pressure monitor and exercise prescription that was formulated depending on 6-MWD. At the same time, in order to ensure the safety and efficacy, the target heart rate did not exceed 60% to 80% of the maximal heart rate after exercise and returned to the pre-exercise level after 5 minutes.12,19,20 According to the patients’ degree of tolerance, the exercise intensity was adjusted monthly for the next 9 months.
Time
Sessions lasted 20 minutes in the first 3 months and, according to the patients’ degree of tolerance, the time was adjusted monthly for the next 9 months, to about 1 hour each session, until the patient complained of tiredness.
Type
Currently, exercise-based cardiac rehabilitation, which involves aerobic exercise supplemented with resistance training, is the primary training for most CR programs.21 Aerobic exercise mainly consisted of cycling, dancing, walking, tai chi, and housework, etc. Resistance exercise, such as dumbbells, sit-ups, etc., could also be chosen (1 time/week).
If any discomfort occurred during this period, including refractory angina, heart rate change >20 beats/min, blood pressure charge >20 mmHg, ST segment depression ≥0.1mV or elevation ≥0.2 mV during activity, or arrhythmia, chest distress, palpitation, dizziness, syncope, pallor, sweating, oxygen saturation (SpO2, measured using a portable oxygen saturation monitor) ≤85% and so on, activity was to be stopped immediately and the follow-up doctor informed to decide whether to adjust the program to continue the rehabilitation or withdraw from the study.
Observed Indicators
Evaluation of Cardiac Function and Athletic Endurance
Before and 1 year after training, the left ventricular end diastolic dimension (LVEDD) of all the enrolled patients was measured with a Doppler ultrasonic diagnostic apparatus (CX50, Philips, Holland), and LVEF was calculated along with the 6-minute walk distance (6-MWD) based on the 6-MWT according to a standardized protocol simultaneously.
Evaluation of Safety
Adverse events were recorded, including refractory angina, myocardial reinfarction, malignant arrhythmia, heart failure, stroke, sudden cardiac death, rehospitalization, revascularization, and fatal bleeding events.
Evaluation of the Quality-of-Life
The quality-of-life was measured by the Medical Outcome Survey Short Form (SF-12) questionnaire, which contained a physical component summary (PCS) and mental component summary (MCS).
Laboratory Indicators
Before and 1 year after training, the serum levels of NO, NOS, SOD, and VEGF were detected. Four milliliters of fasting blood was drawn from all the patients into tubes with separating gel. The blood was incubated for 10 minutes and then centrifuged for 10 minutes at 3,500 rpm. Levels of NO, NOS, SOD, and VEGF were detected by colorimetric assay, the xanthine oxidase method, and enzyme-linked immunosorbent assay (ELISA), respectively. All operations were carried out strictly in accordance with the kit manufacturer’s instructions. Nitrate ester medication was stopped for 2 days before testing in both groups.
Types of Outcome Measures
According to the inclusions and exclusions, the study should assess the following outcomes. We extracted the results at baseline and 12 month follow-ups (medium–long-term) to assess the efficacy and safety and explore the possible mechanism.
Primary Outcomes
Cardiac Function; 6-MWD; quality-of-life assessed by 12-item Short Form (SF-12).
Secondary Outcomes
Major adverse cardiac events.
Statistical Analysis
Measurement data were presented as means±SDs, a t-test was performed to analyze the differences between the complete revascularization and cardiac rehabilitation groups if the variance was homogeneous, or the Wilcoxon rank sum test was used. Enumeration data were presented as ratios, and the chi-square test or Fisher’s exact test was used to analyze differences between the two groups. All the data were analyzed with the Statistical Package for the Social Sciences (SPSS) version 22.0 (SPSS, Inc., Chicago, IL). The level of significance was set at p<0.05 for all results.
Results
Among the 400 enrolled patients, two cases were lost follow-up and two cases died in the complete revascularization group, while six cases were lost to follow-up in the cardiac rehabilitation group.
Evaluation of Cardiac Function and Athletic Endurance
As shown in Table 3, before training, the measurements of LVEDD, LVEF, and 6MWT in the complete revascularization group were 57.90±5.38 mm, 46.10±4.10%, and 258.70±20.15 m, respectively, lower than those in the cardiac rehabilitation group, which were 58.70±2.91 mm, 48.20±4.13%, and 267.90±14.28 m, respectively, but there was no statistically significant difference (p=0.68, 0.25, 0.25). After 1 year, the measurements of LVEDD in the complete revascularization group decreased to 49.50±3.54 mm and 48.70±2.26 mm in the cardiac rehabilitation group, and the difference between the two groups was not statistically significant (p=0.56). By contrast, the measurements of LVEF in the complete revascularization group increased to 54.20±6.05% and 56.50±3.03% in the cardiac rehabilitation group, also with no statistical significance (p=0.30). Meanwhile, 6MWD in the complete revascularization group increased to 418.80±24.42 m and 556.70±55.67 m in the cardiac rehabilitation group, with statistical significance (p=0.001). There were also significant differences within the same group before and after training because of the obvious improvement of the measurements of LVEDD, LVEF, and 6MWT (Complete revascularization group: p=0.001, 0.001, 0.001; Cardiac rehabilitation group: p=0.001, 0.001, 0.001).
 |
Table 3 The Levels of LVEDD, LVEF, and 6-MWD Before and After Training in Two Groups ( |

Evaluation of the Safety
The occurrence of major adverse cardiac events in the complete revascularization group was 16.33% (32 cases, including refractory angina (6 cases), malignant arrhythmias (6 cases), heart failure (10 cases), sudden cardiac death (2 cases), rehospitalization (20 cases), and revascularization (4 cases)), compared to 11.34% (22 cases, including refractory angina (4 cases), malignant arrhythmias (4 cases), heart failure (4 cases), rehospitalization (10 cases), and revascularization (4 cases)) in the cardiac rehabilitation group (Table 4). This difference was not statistically significant (p=1.00, 1.00, 0.45, 1.00, 0.19, 1.00, 0.31).
 |
Table 4 The Occurrence of Major Adverse Cardiac Events After the Training in Two Groups (n, %) |
Evaluation of Quality-of-Life
Before training, PCS and MCS in the complete revascularization group were 24.04±11.95 and 31.50±7.09, and they were 23.67±8.18 and 32.75±3.62 in the cardiac rehabilitation group, respectively, with no statistically significant difference (p=0.94, 0.32). However, 1 year later, PCS and MCS in the complete revascularization group increased to 55.27±7.86 and 55.50±11.95, and 78.91±16.89 and 80.75±6.35 in the cardiac rehabilitation group, respectively. The differences between the two groups were statistically significant (p=0.002, 0.001). The improvement was obvious in the same group before and after training, a difference that was also statistically significant (Complete revascularization group: p=0.001, 0.001; Cardiac rehabilitation group: p= 0.001, 0.001), as presented in Table 5.
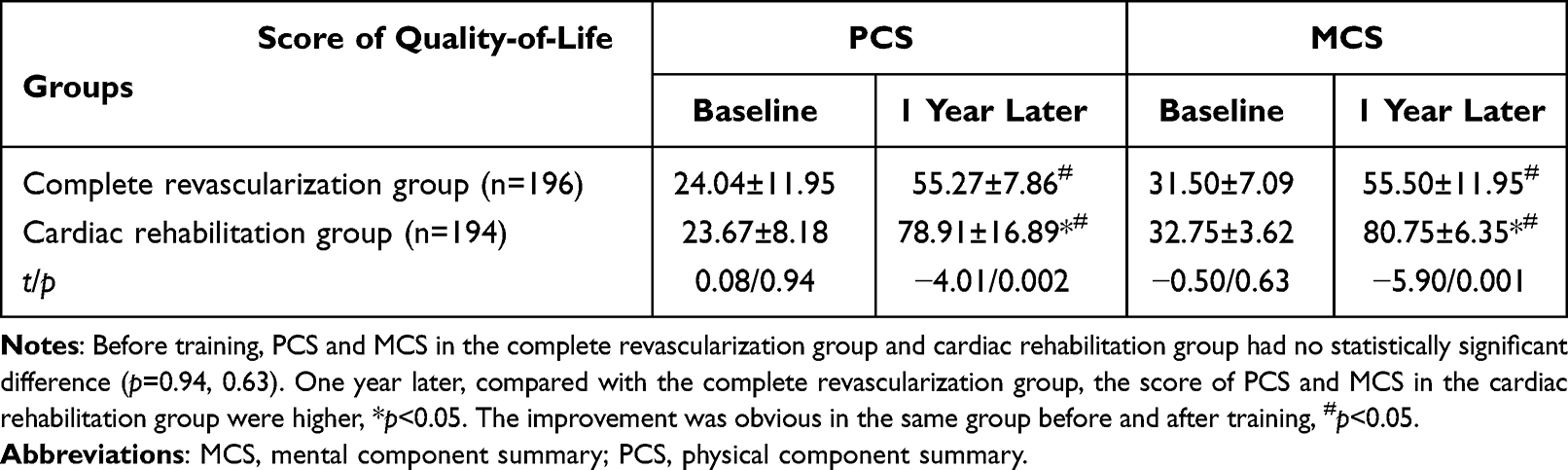 |
Table 5 The Score of PCS and MCS of Two Groups Before and After Training ( |

The Levels of Serum NO, NOS, SOD, and VEGF
Before training, the levels of serum NO, NOS, SOD, and VEGF in the complete revascularization group were 40.00±5.94 μmol/L, 37.00±4.69 U/mL, 60.40±5.36 U/mL, and 386.80±31.62 ng/L, while they were 42.90±5.47 μmol/L, 38.30±3.40 U/mL, 63.10±6.64 U/mL, and 386.90±24.08 ng/L in the cardiac rehabilitation group, respectively. There was no statistically significant difference (p=0.27, 0.49, 0.33, 0.99). One year later, the levels of serum NO, NOS, and SOD in the complete revascularization group increased to 78.80±3.94 μmol/L, 68.90±2.42 U/mL, and 101.00±2.98 U/mL, respectively, while there were noticeably higher levels of 104.80±6.80 μmol/L, 87.70±5.58 U/ mL, and 113.80±5.57 U/mL in the cardiac rehabilitation group, respectively, and the levels of serum VEGF decreased to 280.10±24.76 ng/L in the complete revascularization group and 223.10±12.07 ng/L in the cardiac rehabilitation group. The differences between two groups was statistically significant (p=0.001, 0.001, 0.001, 0.001). The levels of serum NO, NOS, SOD, and VEGF were improved obviously within the same group before and after training, a difference that was also statistically significant (p=0.001). All of the above results are displayed in Table 6.
 |
Table 6 The Levels of Serum NO, NOS, SOD, and VEGF Before and After Training in Two Groups ( |

Discussion
At present, the purpose of the treatment of CHD is to alleviate symptoms, reduce the occurrence of myocardial infarction, and improve the quality-of-life and long-term survival of patients; the means to achieve the above requirements is to perform complete revascularization.13 However, incomplete revascularization is very common clinically due to advanced age, complex coronary lesions, chronic coronary arterial total occlusion, left ventricular dysfunction, past medical history of myocardial infarction, diabetes, and chronic renal insufficiency, etc., with an incidence of about 47.2–69.0%.22 How to improve the survival rate of these patients and reduce the incidence of myocardial infarction is particularly important. Cardiac rehabilitation refers to ensuring the patients achieve the best physical, psychological, and social status through a variety of combined therapies, so that these patients suffering from chronic or acute cardiovascular diseases can maintain or regain optimal social functional status through their own efforts, and delay or reverse the disease process through healthy behaviors.23 Many studies have shown that cardiac rehabilitation can significantly reduce the morbidity and mortality of patients with CHD after myocardial infarction, PCI, and coronary artery bypass grafting (CABG),24–26 decrease the risk factors of CHD, and improve the quality-of-life of patients with CHD. Therefore, cardiac rehabilitation is recommended as a primary intervention treatment for CHD.27–29
In this study, through the observation and comparison of the patients who underwent complete revascularization and partial revascularization and cardiac rehabilitation, it was found that the 6-MWD in the cardiac rehabilitation group was superior to that in the complete revascularization group after 1 year, and the difference was significant. The possible reason for this change might be that, although it takes a long time for the formation of multi-vessel coronary artery disease, coronary blood flow and cardiac functional reserve have changed, yet, as the time is prolonged, cardiac rehabilitation could dramatically improve the coronary blood flow and cardiac functional reserve of patients after PCI so as to save more cardiomyocytes and open or establish vascular channels further, which could significantly reduce the oxygen consumption of cardiomyocytes, reduce myocardial tissue remodeling after myocardial infarction, and improve myocardial tissue compliance.30 Moreover, cardiac rehabilitation from an earlier stage after PCI could significantly strengthen cardiopulmonary functions, enhance exercise tolerance, reduce myocardial oxygen consumption, and improve quality-of-life,31 which may be related to the fact that exercise training could increase the density and volume of mitochondria, as well as the ratio of the formation of Adenosine Triphosphate (ATP), to improve the ability of oxidative metabolism and exercise tolerance. This is a greater alignment with the result of the improvement of 6-MWD in the cardiac rehabilitation group compared with it in the complete revascularization group in our study.
6-MWT, an important indicator of cardiopulmonary function in patients with CHD could be influenced by stature, age, sex, BMI, gait mechanics, comorbidities, and motivation, as well as the test operators’ encouragement and/or motivation given to patients,6,32–35 is safe, reliable, cost-effective, easy to perform, does not require specialized equipment, and also has practical value.12,36 After 1 year, 6-MWD in the cardiac rehabilitation group was improved by about 200 m, indicating that their cardiopulmonary fitness may be close to normal.16 Furthermore, the distance change in the CR group was more than the minimal clinically important difference (MCID),37 explaining that cardiac rehabilitation could improve athletic endurance.
The results of LVEDD and LVEF in our study at baseline and 1 year later showed that LVEDD and LVEF in the two groups were both improved with no statistically significant difference, indicating that cardiac rehabilitation performed on partial revascularization was not inferior to complete revascularization. Chyrchel et al7 have shown that complete revascularization could improve or maintain similar LVEF in patients with impaired or preserved LVEF. But, in other studies, it has been shown that the beneficial effect of LVEF improvement was only reached with LVEF <45% at baseline.38
At the same time, studies have shown complete revascularization among patients with preserved LVEF (>40%) is sufficient in reducing major adverse cardiac events in the long-term (3-year) follow-up.39 This study found that the incidence of major adverse cardiac events in the cardiac rehabilitation group was not higher than that in the complete revascularization group 1 year later, with no statistical significance. However, the readmission rate in the cardiac rehabilitation group was obviously lower, which could significantly reduce medical expenses and obtain better cost-effectiveness of prevention. Studies have shown that cardiac rehabilitation training from an earlier stage is safe and effective for patients after partial or complete revascularization.40 Cardiac rehabilitation could not only significantly reduce the mortality after PCI but also reduce the incidence of acute myocardial ischemia events and the hospitalization rate.41 Moreover, cardiac rehabilitation can benefit patients with CHD and stroke by controlling risk factors of cardiovascular diseases, and play an important role in controlling the occurrence and development of diseases.42 Of interest, the findings of this study were consistent with the above results, indicating that cardiac rehabilitation was safe and did not increase the incidence of major adverse cardiac events.
Up to now, it has been considered that most patients with CHD have a tendency toward anxiety and depression; exercise training could keep the excitability of the sympathetic nervous system stable and attenuate various clinical symptoms caused by increased sympathetic activation, so that the quality-of-life could be very much improved.41,43 Moreover, exercise training could improve the mental health status of patients, increase the confidence of cardiac rehabilitation,44 and further improve the quality-of-life. Our study showed that the scores of PCS and MCS of the patients in the complete revascularization group and cardiac rehabilitation group were significantly improved 1 year later. In the cardiac rehabilitation group, these scores were significantly higher than those in the complete revascularization group, and the difference was statistically significant. It may be because moderate aerobic exercise could eliminate the low mood and feelings of patients with CHD and be conducive to peace of mind, improving their athletic endurance, physical and psychological condition so as to promote their ability to care for life and social functions, thus forming a positive cycle.13,30,45 Therefore, the researchers further detected the levels of serum NO, NOS, SOD, and VEGF before and after training to explore the possible mechanism.
In recent years, it has been continuously proved that lipid peroxides and their catabolites could cause CHD via damaging the walls of the coronary arteries. SOD, as one of the most important antioxidant enzymes in vivo, can scavenge free radicals and maintain the stability and integrity of cell membranes to prevent CHD by eliminating oxygen free radicals. NO, synthesized by the catalysis of NO synthase, a key rate-limiting enzyme, going through the development of many cardiovascular diseases, is an independent physiological regulatory factor, with the effect of vasodilation, eliminating oxygen free radicals, inhibiting the aggregation and adhesion of platelets, maintaining normal cardiac output, and protecting cells. To a certain extent, a very high NO concentration reflects high vascular activity.46 When NOS is insufficient, the synthesis of NO will be reduced, causing vasoconstriction, increasing vascular smooth muscle cell proliferation, promoting atherosclerosis, leading to microcirculation disturbance, and consequently result in aggravation of coronary artery stenosis, myocardial ischemia and hypoxia, and even myocardial infarction.47 Meanwhile, NO imbalance can stimulate and release endothelin, which could not only induce the proliferation of vascular endothelial cells but also promote the synthesis and secretion of VEGF directly or indirectly.48 So far, it has been known that VEGF, the content of which is generally low in the body normally but enjoys rapid growth in hypoxia, is the most powerful cytokine in promoting vascular growth. Also, VEGF can build new blood vessels and promote the formation of a collateral circulation and the proliferation and division of endothelial cells.49,50 The level of VEGF could reflect the degree of myocardial ischemia.51 Therefore, the level of VEGF can not only be used to evaluate the degree of myocardial ischemia and reperfusion injury in clinical settings but also to evaluate the effect of post-PCI.52 This study found no significant difference in the levels of NO, NOS, SOD, and VEGF between two groups before training, while a significant improvement in two groups was found 1 year later, more obviously in the cardiac rehabilitation group, with a significant difference. It is possible that long-term cardiac rehabilitation training could increase the levels of NO and SOD in coronary artery endothelial cells, improve the endothelium-dependent vasodilatory function, promote vascular remodeling and angiogenesis, improve autonomic balance, and increase the blood flow perfusion of skeletal muscle via increasing oxygen extraction capacity,53 which could improve myocardial ischemia-reperfusion injury, myocardioprotection, and reduce the level of VEGF. In addition, local release of NO can restrain intimal hyperplasia, down-regulate the levels of interleukin-6 and c-reactive protein significantly, reduce inflammation, and inhibit the development of in-stent restenosis. The results of NO, NOS, SOD, and VEGF in two groups at baseline and 1 year later showed levels of NO, NOS, and SOD increased more noticeably and the level of VEGF decreased more obviously in the cardiac rehabilitation group with a statistically significant difference, suggesting that cardiac rehabilitation performed on partial revascularization could regulate blood vessel endothelial function.
Strengths and Limitations
This study could provide treatment recommendations for patients with multiple coronary artery lesions who cannot accept complete revascularization, it is not only a simple, safe, and operable approach but is also cost-effective and has improvements in poor cognition. In addition, another strength might be that cardiac rehabilitation could become a part of patients’ daily life and gradually improve their lifestyle.
Limitations of this study included it being a single-center study and the relatively short time of observation. Also, this study might overestimate the real effect of cardiac rehabilitation on patients’ cardiorespiratory fitness because of some spontaneous recovery after revascularization. Besides, in this study, the researchers did not enroll and observe the patients who underwent cardiac rehabilitation after complete revascularization of multi-vessel coronary artery disease and did not adopt cardiopulmonary exercise testing due to the confinement of objective conditions. The comprehensive effect of cardiac rehabilitation in patients with CHD who underwent partial revascularization performed on multiple coronary artery lesions needs to be corroborated by enlarging the population such as patients with heart failure with a preserved ejection fraction and in multiple centers and verified in a long-term follow-up as well as with cardiopulmonary exercise testing.
Conclusions
Cardiac rehabilitation training is effective, safe, and does not increase the incidence of adverse events after partial revascularization in patients with multiple coronary artery lesions, which has notable clinical advantages in promoting exercise endurance and quality-of-life by improving the nitric oxide synthase system and antioxidant system and reducing the level of VEGF, could significantly reduce medical expenses and obtain a better cost-effectiveness of prevention, providing new ideas and a new basis for the treatment of CHD.
Data Sharing Statement
The data could be obtained from this article.
Acknowledgment
Many thanks are given to the researchers for their hard work and reviewers for their valuable advice.
Funding
The authors have no funding to declare.
Disclosure
The authors have no conflicts of interest to declare.
References
1. Bravo-Escobar R, González-Represas A, Gómez-González AM, et al. Effectiveness and safety of a home-based cardiac rehabilitation programme of mixed surveillance in patients with ischemic heart disease at moderate cardiovascular risk: a randomised, controlled clinical trial. BMC Cardiovasc Disord. 2017;17(1):66. doi:10.1186/s12872-017-0499-0
2. Fattirolli F, Pratesi A. Cardiovascular prevention and rehabilitation in the elderly: evidence for cardiac rehabilitation after myocardial infarction or chronic heart failure. Monaldi Arch Chest Dis. 2016;84(1–2):731. doi:10.4081/monaldi.2015.731
3. Sandercock GR, Cardoso F, Almodhy M, Pepera G. Cardiorespiratory fitness changes in patients receiving comprehensive outpatient cardiac rehabilitation in the UK: a multicentre study. Heart. 2013;99(11):785–790. doi:10.1136/heartjnl-2012-303055
4. Lee KW, Blann AD, Jolly K, Lip GY; BRUM Investigators. Plasma haemostatic markers, endothelial function and ambulatory blood pressure changes with home versus hospital cardiac rehabilitation: the Birmingham Rehabilitation Uptake Maximisation Study. Heart. 2006;92(12):1732–1738. doi:10.1136/hrt.2006.092163
5. Skrypnik D, Skrypnik K, Suliburska J, Bogdański P. Cardiac rehabilitation may influence leptin and VEGF A crosstalk in patients after acute coronary syndrome. Sci Rep. 2022;12(1):11825. doi:10.1038/s41598-022-16053-1
6. Li J, Liu B, Wang Z, et al. Efficacy of a 6-week home-based online supervised exercise program conducted during COVID-19 in patients with post percutaneous coronary intervention: a single-blind randomized controlled trial. Front Cardiovasc Med. 2022;9:853376. doi:10.3389/fcvm.2022.853376
7. Chyrchel M, Gallina T, Januszek R, Szafrański O, Gębska M, Surdacki A. The reduction of left ventricle ejection fraction after multi-vessel PCI during acute myocardial infarction as a predictor of major adverse cardiac events in long-term follow-up. Int J Environ Res Public Health. 2022;19(20):13160. doi:10.3390/ijerph192013160
8. Ng VG, Lansky AJ, Meller S, et al. The prognostic importance of left ventricular function in patients with ST-segment elevation myocardial infarction: the HORIZONS-AMI trial. Eur Heart J Acute Cardiovasc Care. 2014;3(1):67–77. doi:10.1177/2048872613507149
9. Hotta K, Kamiya K, Shimizu R, et al. Stretching exercises enhance vascular endothelial function and improve peripheral circulation in patients with acute myocardial infarction. Int Heart J. 2013;54(2):59–63. doi:10.1536/ihj.54.59
10. Vona M, Rossi A, Capodaglio P, et al. Impact of physical training and detraining on endothelium-dependent vasodilation in patients with recent acute myocardial infarction. Am Heart J. 2004;147(6):1039–1046. doi:10.1016/j.ahj.2003.12.023
11. Vona M, Codeluppi GM, Iannino T, Ferrari E, Bogousslavsky J, von Segesser LK. Effects of different types of exercise training followed by detraining on endothelium-dependent dilation in patients with recent myocardial infarction. Circulation. 2009;119(12):1601–1608. doi:10.1161/CIRCULATIONAHA.108.821736
12. Zhang Y, Cao H, Jiang P, Tang H. Cardiac rehabilitation in acute myocardial infarction patients after percutaneous coronary intervention: a community-based study. Medicine. 2018;97(8):e9785. doi:10.1097/MD.0000000000009785
13. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on clinical practice guidelines. Circulation. 2022;145(3):e4–e17. doi:10.1161/CIR.0000000000001039
14. Taylor RS, Dalal HM, McDonagh STJ. The role of cardiac rehabilitation in improving cardiovascular outcomes. Nat Rev Cardiol. 2022;19(3):180–194. doi:10.1038/s41569-021-00611-7
15. Piepoli MF, Hoes AW, Agewall S. The Sixth Joint Task Force of the European Society of Cardiology and Other Societies on Cardiovascular Disease Prevention in Clinical Practice, 2016 European Guidelines on cardiovascular disease prevention in clinical practice. Eur Heart J. 2016;37(29):2315–2381. doi:10.1093/eurheartj/ehw106
16. Richardson CR, Franklin B, Moy ML, Jackson EA. Advances in rehabilitation for chronic diseases: improving health outcomes and function. BMJ. 2019;365:l2191. doi:10.1136/bmj.l2191
17. Chinese Society of Cardiology of Chinese Medical Association. Chinese experts consensus on cardiac rehabilitation/secondary prevention for coronary artery disease. Chin J Cardiol. 2013;41:267–275.
18. Billinger SA, Boyne P, Coughenour E, Dunning K, Mattlage A. Does aerobic exercise and the FITT principle fit into stroke recovery? Curr Neurol Neurosci Rep. 2015;15(2):519. doi:10.1007/s11910-014-0519-8
19. Thomas RJ, Beatty AL, Beckie TM, et al. Home-based cardiac rehabilitation: a scientifific statement from the American association of cardiovascular and pulmonary rehabilitation, the American heart association, and the American college of cardiology. J Am Coll Cardiol. 2019;74:133–153. doi:10.1016/j.jacc.2019.03.008
20. Tanaka H, Monahan KD, Seals DR. Age-predicted maximal heart rate revisited. J Am Coll Cardiol. 2001;37:153–156. doi:10.1016/S0735-1097(00)01054-8
21. Blumenthal JA, Wang JT, Babyak M, et al. Enhancing standard cardiac rehabilitation with stress management training: background, methods, and design for the enhanced study. J Cardiopulm Rehabil Prev. 2010;30(2):77–84. doi:10.1097/HCR.0b013e3181d0c1d3
22. Kereiakes DJ. Reassessing the importance of complete versus incomplete coronary revascularization. Rev Cardiovasc Med. 2014;15(1):24–30. doi:10.3909/ricm0714
23. La Rovere MT, Traversi E. Role and efficacy of cardiac rehabilitation in patients with heart failure. Monaldi Arch Chest Dis. 2019;89(1):69–72. doi:10.4081/monaldi.2019.1027
24. Anderson L, Oldridge N, Thompson DR, et al. Exercise-based cardiac rehabilitation for coronary heart disease: Cochrane systematic review and meta-analysis. J Am Coll Cardiol. 2016;67(1):1–12. doi:10.1016/j.jacc.2015.10.044
25. McMahon SR, Ades PA, Thompson PD. The role of cardiac rehabilitation in patients with heart disease. Trends Cardiovasc Med. 2017;27(6):420–425. doi:10.1016/j.tcm.2017.02.005
26. Pack QR, Dudycha KJ, Roschen KP, et al. Safety of early enrollment into outpatient cardiac rehabilitation after open heart surgery. Am J Cardiol. 2015;115(4):548–552. doi:10.1016/j.amjcard.2014.11.040
27. Brown TM, Hernandez AF, Bittner V, et al. Predictors of cardiac rehabilitation referral in coronary artery disease patients: findings from the American Heart Association’s Get With The Guidelines Program. J Am Coll Cardiol. 2009;54(6):515–521. doi:10.1016/j.jacc.2009.02.080
28. Sunamura M, Ter Hoeve N, Geleijnse ML, et al. Cardiac rehabilitation in patients who underwent primary percutaneous coronary intervention for acute myocardial infarction: determinants of programme participation and completion. Neth Heart J. 2017;25(11):618–628. doi:10.1007/s12471-017-1039-3
29. Simon M, Korn K, Cho L, Blackburn GG, Raymond C. Cardiac rehabilitation: a class 1 recommendation. Cleve Clin J Med. 2018;85(7):551–558. doi:10.3949/ccjm.85a.17037
30. Urbinati S, Tonet E. Cardiac rehabilitation after STEMI. Minerva Cardioangiol. 2018;66(4):464–470. doi:10.23736/S0026-4725.18.04674-1
31. Price KJ, Gordon BA, Bird SR, Benson AC. A review of guidelines for cardiac rehabilitation exercise programmes: is there an international consensus? Eur J Prev Cardiol. 2016;23(16):1715–1733. doi:10.1177/2047487316657669
32. ATS Committee on Proficiency Standards for Clinical Pulmonary Function Laboratories. ATS statement: guidelines for the six-minute walk test. Am J Respir Crit Care Med. 2002;166(1):111–117. doi:10.1164/ajrccm.166.1.at1102
33. Pepera GK, Sandercock GR, Sloan R, Cleland JJ, Ingle L, Clark AL. Influence of step length on 6-minute walk test performance in patients with chronic heart failure. Physiotherapy. 2012;98(4):325–329. doi:10.1016/j.physio.2011.08.005
34. Pepera G, Cardoso F, Taylor MJ, Peristeropoulos A, Sandercock GR. Predictors of shuttle walking test performance in patients with cardiovascular disease. Physiotherapy. 2013;99(4):317–322. doi:10.1016/j.physio.2013.01.003
35. Adedoyin RA, Adeyanju SA, Balogun MO, Adebayo RA, Akintomide AO, Akinwusi PO. Prediction of functional capacity during six-minute walk among patients with chronic heart failure. Niger J Clin Pract. 2010;13(4):379–381.
36. Lenssen AF, Wijnen LC, Vankan DG, Van Eck BH, Berghmans DP, Roox GM. Six-minute walking test done in a hallway or on a treadmill: how close do the two methods agree? Eur J Cardiovasc Prev Rehabil. 2010;17(6):713–717. doi:10.1097/HJR.0b013e32833a1963
37. Gremeaux V, Troisgros O, Benaïm S, et al. Determining the minimal clinically important difference for the six-minute walk test and the 200-meter fast-walk test during cardiac rehabilitation program in coronary artery disease patients after acute coronary syndrome. Arch Phys Med Rehabil. 2011;92(4):611–619. doi:10.1016/j.apmr.2010.11.023
38. Mehta SR, Wood DA, Storey RF, et al. Complete revascularization with multivessel PCI for myocardial infarction. N Engl J Med. 2019;381(15):1411–1421. doi:10.1056/NEJMoa1907775
39. Kang J, Zheng C, Park KW, et al. Complete revascularization of multivessel coronary artery disease does not improve clinical outcome in ST-segment elevation myocardial infarction patients with reduced left ventricular ejection fraction. J Clin Med. 2020;9(1):232. doi:10.3390/jcm9010232
40. Rechciński T, Kałowski M, Kasprzak JD, Trzos E, Kurpesa M. Beneficial effects of cardiac rehabilitation in patients with incomplete revascularization after primary coronary angioplasty. Eur J Phys Rehabil Med. 2013;49(6):785–791.
41. Goel K, Lennon RJ, Tilbury RT, Squires RW, Thomas RJ. Impact of cardiac rehabilitation on mortality and cardiovascular events after percutaneous coronary intervention in the community. Circulation. 2011;123(21):2344–2352. doi:10.1161/CIRCULATIONAHA.110.983536
42. Clark AM, Whelan HK, Barbour R, MacIntyre PD. A realist study of the mechanisms of cardiac rehabilitation. J Adv Nurs. 2005;52(4):362–371. doi:10.1111/j.1365-2648.2005.03601.x
43. Papathanasiou G, Tsamis N, Georgiadou P, Adamopoulos S. Beneficial effects of physical training and methodology of exercise prescription in patients with heart failure. Hellenic J Cardiol. 2008;49(4):267–277.
44. Menezes AR, Lavie CJ, Milani RV, Arena RA, Church TS. Cardiac rehabilitation and exercise therapy in the elderly: should we invest in the aged? J Geriatr Cardiol. 2012;9(1):68–75. doi:10.3724/SP.J.1263.2012.00068
45. Gathright EC, Busch AM, Buckley ML, et al. Improvements in Depressive Symptoms and Affect During Cardiac Rehabilitation: PREDICTORS AND POTENTIAL MECHANISMS. J Cardiopulm Rehabil Prev. 2019;39(1):27–32. doi:10.1097/HCR.0000000000000346
46. Mangiacapra F, Del Buono MG, Abbate A, et al. Role of endothelial dysfunction in determining angina after percutaneous coronary intervention: learning from pathophysiology to optimize treatment. Prog Cardiovasc Dis. 2020;63(3):233–242. doi:10.1016/j.pcad.2020.02.009
47. Glueck CJ, Valdes A, Bowe D, Munsif S, Wang P. The endothelial nitric oxide synthase T-786c mutation, a treatable etiology of Prinzmetal’s angina. Transl Res. 2013;162(1):64–66. doi:10.1016/j.trsl.2013.03.003
48. Hong XY, Hong X, Gu WW, Lin J, Yin WT. Cardioprotection and improvement in endothelial-dependent vasodilation during late-phase of whole body hypoxic preconditioning in spontaneously hypertensive rats via VEGF and endothelin-1. Eur J Pharmacol. 2019;842:79–88. doi:10.1016/j.ejphar.2018.10.033
49. Husain K, Vazquez-Ortiz M, Lalla J. Down regulation of aortic nitric oxide and antioxidant systems in chronic alcohol-induced hypertension in rats. Hum Exp Toxicol. 2007;26(5):427–434. doi:10.1177/0960327106072993
50. Brunt VE, Weidenfeld-Needham KM, Comrada LN, Francisco MA, Eymann TM, Minson CT. Serum from young, sedentary adults who underwent passive heat therapy improves endothelial cell angiogenesis via improved nitric oxide bioavailability. Temperature. 2019;6(2):169–178. doi:10.1080/23328940.2019.1614851
51. Bekler A, Gazi E, Yılmaz M, et al. Could elevated platelet-lymphocyte ratio predict left ventricular systolic dysfunction in patients with non-ST elevated acute coronary syndrome? Anatol J Cardiol. 2015;15(5):385–390. doi:10.5152/akd.2014.5434
52. Ikhapoh IA, Pelham CJ, Agrawal DK. Atherogenic cytokines regulate VEGF-A-induced differentiation of bone marrow-derived mesenchymal stem cells into endothelial cells. Stem Cells Int. 2015;2015:498328. doi:10.1155/2015/498328
53. Tsukakoshi D, Yamamoto S, Takeda S, Furuhashi K, Sato M. Clinical perspectives on cardiac rehabilitation after heart failure in elderly patients with frailty: a narrative review. Ther Clin Risk Manag. 2022;18:1009–1028. doi:10.2147/TCRM.S350748
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.