Back to Journals » Journal of Multidisciplinary Healthcare » Volume 7
The difficulties of interprofessional teamwork in diabetes care: a questionnaire survey
Authors Kishimoto M, Noda M
Received 23 April 2014
Accepted for publication 27 May 2014
Published 5 August 2014 Volume 2014:7 Pages 333—339
DOI https://doi.org/10.2147/JMDH.S66712
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Miyako Kishimoto,1,2 Mitsuhiko Noda2,3
1Department of Diabetes, Endocrinology, and Metabolism, Center Hospital, National Center for Global Health and Medicine, Tokyo, Japan; 2Diabetes and Metabolism Information Center, Diabetes Research Center, Research Institute, National Center for Global Health and Medicine, Tokyo, Japan; 3Department of Diabetes Research, Diabetes Research Center, Research Institute, National Center for Global Health and Medicine, Tokyo, Japan
Background: Diabetes is a multifactorial disease and its nature means that interprofessional teamwork is essential for its treatment. However, in general, interprofessional teamwork has certain problems that impede its function. To clarify these problems in relation to diabetes care, a questionnaire survey was conducted.
Methods: The participants who were involved in diabetes-related educational seminars, and medical personnel who were engaged in diabetes care from the National Center for Global Health and Medicine, were asked to complete the questionnaire about perceptions of, and satisfaction with, interprofessional teamwork across multiple health care providers, who were actually involved in diabetes care.
Results: From 456 people who were asked to take the questionnaire, 275 people answered. The percentages of the respondents according to profession who considered multidisciplinary teamwork sufficient were as follows: physicians, 20.5%; nurses, 12.7%; registered dietitians, 29.6%; pharmacists, 21.9%; physiotherapists, 18.2%; and clinical laboratory technicians 15.4%. Insufficient interprofessional communication and inconsistency in motivation levels among staff were frequently cited as causes of insufficient teamwork. All professions considered interprofessional meetings or conferences necessary and essential for teamwork.
Conclusion: The survey revealed that interprofessional teamwork in diabetes care is currently insufficient. Continuous efforts to change each profession's perceptions about interprofessional teamwork and efforts to improve the quality of interprofessional meetings are necessary.
Keywords: diabetes, interprofessional, questionnaire survey, communication
Introduction
The number of people worldwide with diabetes has increased enormously; 382 million people were reported to have diabetes in 2013 and this is expected to rise to 592 million in 2035,1 which will create a significant health care burden worldwide. Nutrition therapy and exercise therapy are fundamental for diabetes, while pharmacotherapy is adopted when necessary. Therefore, not only are physicians and nurses greatly involved in patient treatment for people with diabetes, but so too are registered dietitians, physiotherapists, clinical laboratory technicians, and pharmacists. Thus, the disease requires the skill and talents of multiple health care providers, and as such, interprofessional teamwork is extremely important for diabetes care.2,3 Successful interprofessional teamwork – in other words, when multiple health workers from different professional backgrounds work together and are able to provide comprehensive services effectively by working with patients, their families, caregivers, and communities – leads to better patient care and safety, and improves health outcomes for patients.4–7 Therefore, it is not an exaggeration to say that the level of success of interprofessional teamwork may determine diabetes care outcomes. However, levels of perceptions of, and satisfaction with, interprofessional teamwork in multiple health care providers, who are actually involved in diabetes care, are unclear and often unexpressed. To clarify these points, a survey was conducted.
Methods
The National Center for Global Health and Medicine (NCGM) in Japan has been conducting free educational seminars five to six times per year for more than 5 years for various professional groups that are involved and interested in diabetes care.8 Participants from NCGM educational seminars and other related seminars, as well as NCGM medical personnel who are engaged in diabetes care, were asked to inform us of their profession and complete a survey featuring three questions. Question 1 (Q1) was “Do you think multidisciplinary teamwork for diabetes patients in your facility works sufficiently?” which required a “yes”, “no”, or “not sure” response. Question 2 (Q2) was “Why do you think so? Please explain the reasons for this.” Question 3 (Q3) was “Please state your ideas regarding how to resolve this problem.” Q2 and Q3 were answered by free description. The questionnaire was anonymous and its completion was voluntary. The answers for Q1 were broken down into percentages for “yes”, “no”, or “not sure” in each profession. Those who answered “no” and “not sure” to Q1 were further analyzed by combining the answers for Q2, and the substantially similar answers for Q2 were grouped and categorized into themes.
Results
From a total of 465 people who were asked to take the questionnaire (432 seminar participants and 33 NCGM medical staff) 275 people answered the questionnaire (243 seminar participants and 32 NCGM medical staff). The percentages of each occupation that answered “yes”, “no”, and “not sure” to Q1 are shown in Table 1. These figures show that less than 30% of the participants in each of the professions surveyed were satisfied regarding the current state of interprofessional teamwork. The percentages of “yes” answers in each profession were as follows: physicians, 20.5%; nurses, 12.7%; registered dietitians, 29.6%; pharmacists, 21.9%; physiotherapists, 18.2%; and clinical laboratory technicians, 15.4%.
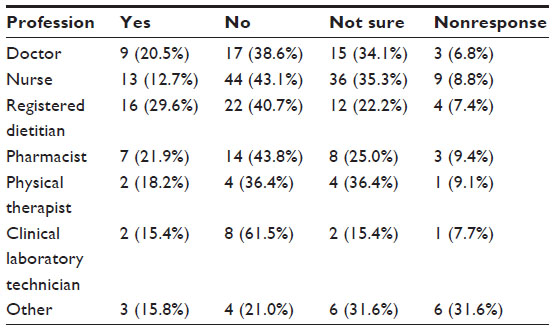 | Table 1 Answers to Question 1 |
Representative answers to Q2 and Q3 for each profession are shown in Table 2. The answers for Q2 were varied, and those who answered “no” and “not sure” to Q1 were classified into five thematic categories. The answers that considered lack of interprofessional communication as the main obstacle to interprofessional teamwork were categorized in “Insufficient communication”: for example, answers such as “Because we do not have regular interprofessional meetings, we have no opportunity to communicate and exchange patients’ information”, or “We can communicate with physicians, but it is hard to communicate with other professions, such as physical therapists or clinical laboratory technicians.” The answers that consider lack of a leader, such as a diabetologist or a certified diabetes educator, as the main problem were categorized under “Lack of leader”. The answers that considered lack of labor as the fundamental problem – in other words, that lack of labor leads to busy medical staff and makes them devote so much to their own professional daily duties that they cannot participate in any additional interprofessional teamwork – were categorized under “Lack of labor”. The answers that considered the conditions of medical facilities as the main problem – for example, “Because there are only one doctor and two nurses in our clinic, we cannot work together with dietitians or pharmacists” – were categorized under “Condition of facilities”. Finally, the answers that considered inconsistencies of staff motivation levels among relevant staff as the main problem were categorized in “Inconsistent motivation” (eg, answers such as “There are big gaps of motivation among the professions or among the individual team members. Even if I propose something, other members do not react”).
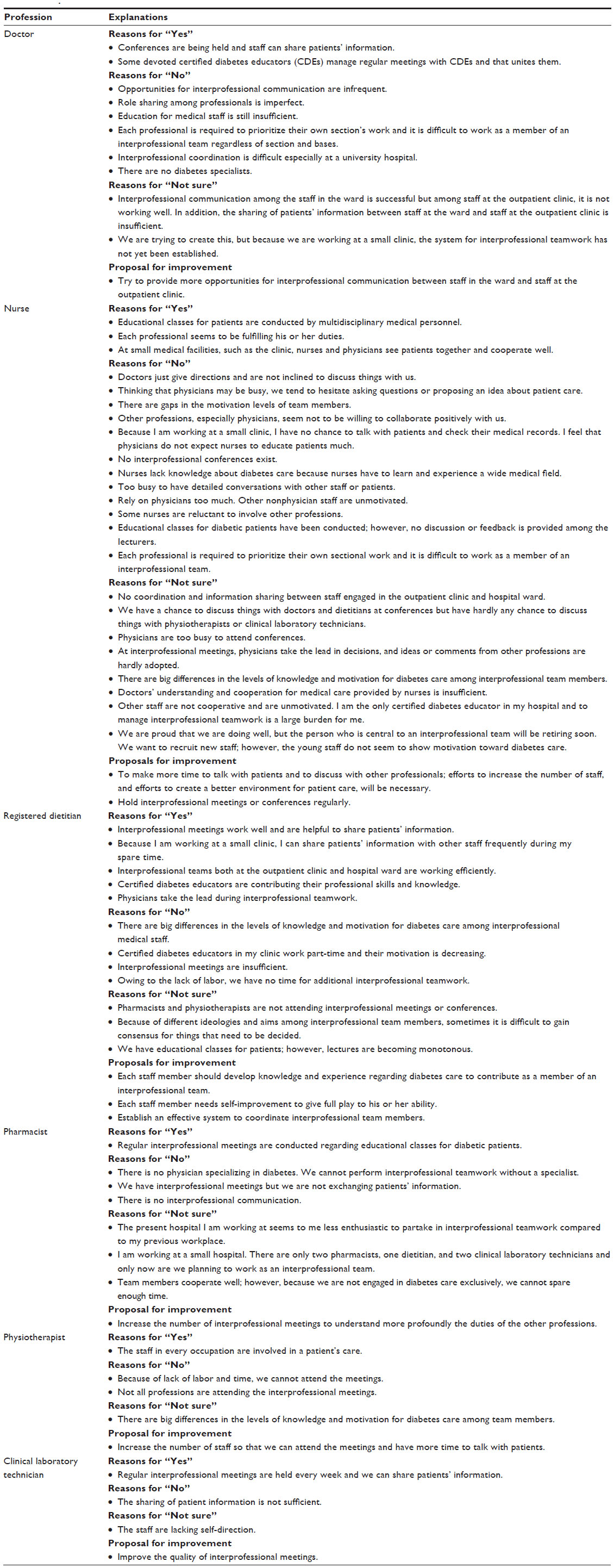 | Table 2 Representative answers to Questions 2 and 3 |
The percentages for each occupation’s answers that were classified into the thematic categories of “Insufficient communication”, “Lack of leader”, “Lack of labor”, “Condition of facilities”, and “Inconsistent motivation” are shown in Table 3. For physicians, nurses, pharmacists, and physical therapists, “Insufficient communication” is the most concerning issue as the obstacle to interprofessional teamwork, whilst registered dietitians and clinical laboratory technicians considered “Inconsistent motivation” as the most concerning issue.
 | Table 3 Thematic analysis |
Discussion
The present questionnaire survey indicated that the current situation regarding interprofessional teamwork for diabetes care is considered problematic and insufficient among the medical personnel surveyed and that there is much room for improvement. Previous research regarding multidisciplinary teamwork has shown that successful interprofessional teamwork helped to achieve intensive glycemic control in certain patient groups.4 However, interprofessional teamwork in general, not solely within diabetes care, has certain difficulties in clinical settings. Caldwell and Atwal9 summarized the problems associated with interprofessional teamwork as involving four issues: ideological differences between health care professions, unequal power relations between the health professions, communication within and between the professional groups, and role overlap and confusion. The results of the present questionnaire survey also showed the communication difficulties within diabetes care.
The Diabetes Attitudes Wishes and Needs 2 (DAWN2) study10 aims to provide a holistic assessment of diabetes care and management among people with diabetes, family members, and health care professionals. The questionnaire results in the DAWN2 study showed that 63.0% of responders recognized the need for formal training in effective communication for all diabetes care specialists, and 56.1% of responders recognized that there should be better communication within the team.11
In the present study, physicians considered insufficient interprofessional communication, condition of medical facilities they worked at, and lack of labor as problems needing to be solved. Nurses considered insufficient communication with physicians or with other professions to be the main problems, as well as inconsistencies of staff motivation levels. Both physicians and nurses considered that insufficient interprofessional communication was the main problem; physicians were not likely to realize that relationships between physician and nonphysician staff are key, while nurses specifically consider that physicians should be more cooperative with them and should understand the need for open communication with them. In addition, physicians seem not to care so much about inconsistent motivation among the team members, while nurses are very concerned about it. Other professions also considered insufficient interprofessional communication or inconsistencies of staff motivation levels as the main problem to be solved. All professions considered that interprofessional meetings or conferences were necessary and essential; however, many people were not satisfied with the ongoing meetings and considered that the meeting content and structure, as well as the members, needed to be changed.
Frequent, high-quality communication and strong relationships among health care providers are important to maximize the quality of care, improve the efficiency of care, and improve clinical outcomes.5,12–14 However, according to the present survey results, some medical personnel have difficulty communicating with other professionals or have never experienced interprofessional meetings or conferences.
Unequal power – in other words, hierarchy – is another main issue regarding teamwork and communication difficulties.5,15–19 While better communication and the development of relationships between health care professionals can be valuable, even within a hierarchical system,12 nonphysician staff remain reluctant to complain to other professionals, particularly physicians. A previous study using a questionnaire to clarify physicians’ traits that impede effective nurse–physician communication revealed that physicians’ reluctance to communicate with nurses and physicians’ emotional difficulties were the main reasons for the communication barrier.20 The authors suggested that educating future physicians or residents to have a positive attitude toward open communication with nurses might reduce the communication barrier.20 Although physicians are often the leaders of interprofessional teamwork, diabetes educators21–24 can be leaders in facilitating open communication among members and preventing the problems associated with hierarchical relationships.
Any division of health care across multiple professions can provoke conflict, particularly in areas featuring potential role overlap.12 It is desirable for professionals to support each other and assist with work that one may be unable to conduct because of a lack of labor or personal inexperience. However, when there are instances of overlapping work with two or more professions involved – for example, a nurse and a pharmacist teaching the same patient at different times how to self-inject insulin via different procedures – and each professional does not share their information with the other, the situation may become confusing, leaving the patient in a potentially dangerous situation. In order to resolve this, each profession should define its role in the team and teams should establish strategies to encourage working partnerships.9 If each profession can teach consistent content to patients, it will be beneficial for patients to obtain reinforcement from different professionals.
Previous reports suggest the effectiveness of postgraduate medical education or interprofessional training programs to educate professionals regarding the importance of interprofessional teamwork.2,6,25,26 Interprofessional education is believed to enhance learners’ understanding of other professions’ roles and responsibilities, while fostering mutual respect and understanding between members of a health care team.7 To evaluate the kinds of education or program(s) that will be effective in improving interprofessional teamwork, further study featuring a large sample size and a well-thought-out design will be necessary.
There are some limitations in the present survey. Firstly, because of the nature of the term “interprofessional teamwork”, its meaning may vary between individuals and respondents might have difficulties in answering questions. This might be one of the reasons why many respondents answered “not sure” to Q1, instead of giving more definite answers such as “yes” or “no”. Secondly, because the questionnaire was conducted for the participants of the educational diabetes seminars who might be more enthusiastic and highly motivated in diabetes care than persons who did not attend the seminars, the results might be biased and not representative in general. The lack of data regarding number of persons who refused to answer the questionnaire raises questions about the representativeness of the samples. Thirdly, the questionnaire did not ask age, sex, or type of facility at which the respondents were working. The information about these factors might give us additional insights. Actually, as shown in Tables 2 and 3, some respondents answered that interprofessional teamwork is insufficient because they are working at medical facilities that are either too small or too big – for example, a small clinic or a university hospital. Therefore, we should have asked in the questionnaire about the types of medical facilities at which respondents were working. Further study that includes this information with a larger number of medical personnel will be necessary.
Conclusion
In conclusion, the results of the questionnaire survey regarding interprofessional teamwork in diabetes care revealed some difficulties in conducting teamwork. Changing the organizational structure and team-leadership style in a short period may be difficult, but continuous efforts to change each profession’s perception of multidisciplinary teamwork and efforts to improve the quality of interprofessional meetings are vital. In addition, physicians need to be better at recognizing the need for open communication and at accepting feedback or input from other professions. To promote this, certain training in effective communication at the start of their professional career, such as when they are students, may be effective.
Disclosure
The authors report no conflicts of interest in this work.
References
International Diabetes Federation. IDF Diabetes Atlas: 6th Edition. 2013. Available from: http://www.idf.org/diabetesatlas. Accessed July 2, 2014. | |
Dounis G, Ditmyer M, Vanbeuge S, et al. Interprofessional faculty development: integration of oral health into the geriatric diabetes curriculum, from theory to practice. J Multidiscip Healthc. 2013;7:1–9. | |
Ritholz MD, Beverly EA, Abrahamson MJ, Brooks KM, Hultgren BA, Weinger K. Physicians’ perceptions of the type 2 diabetes multi-disciplinary treatment team: a qualitative study. Diabetes Educ. 2011;37(6):794–800. | |
Warrington L, Ayers P, Baldwin AM, et al. Implementation of a pharmacist-led, multidisciplinary diabetes management team. Am J Health Syst Pharm. 2012;69(14):1240–1245. | |
Minamizono S, Hasegawa H, Hasunuma N, Kaneko Y, Motohashi Y, Inoue Y. Physician’s perceptions of interprofessional collaboration in Clinical Training Hospitals in Northeastern Japan. J Clin Med Res. 2013;5(5):350–355. | |
Health Professions Network Nursing and Midwifery Office within the Department of Health Resources for Health. Framework for Action on Interprofessional Education and Collaborative Practice. Geneva: World Health Organization; 2010. Available from: http://www.who.int/hrh/resources/framework_action/en/. Accessed July 2, 2014. | |
Curran VR, Sharpe D, Forristall J. Attitudes of health sciences faculty members towards interprofessional teamwork and education. Med Educ. 2007;41(9):892–896. | |
Kishimoto M, Noda M. A report on diabetes seminars for medical staff: findings from a questionnaire survey. Diabetol Int. 2013;4(4):261–265. | |
Caldwell K, Atwal A. The problems of interprofessional healthcare practice in hospitals. Br J Nurs. 2003;12(20):1212–1218. | |
Peyrot M, Burns KK, Davies M, et al. Diabetes Attitudes Wishes and Needs 2 (DAWN2): a multinational, multi-stakeholder study of psychosocial issues in diabetes and person-centered diabetes care. Diabetes Res Clin Pract. 2013;99(2):174–184. | |
Holt RI, Nicolucci A, Kovacs Burns K, et al. Diabetes Attitudes, Wishes and Needs second study (DAWN2™): cross-national comparisons on barriers and resources for optimal care – healthcare professional perspective. Diabet Med. 2013;30(7):789–798. | |
Whitehead C. The doctor dilemma in interprofessional education and care: how and why will physicians collaborate? Med Educ. 2007;41(10):1010–1016. | |
Schmidt I, Claesson CB, Westerholm B, Nilsson LG, Svarstad BL. The impact of regular multidisciplinary team interventions on psychotropic prescribing in Swedish nursing homes. J Am Geriatr Soc. 1998;46(1):77–82. | |
Wilson SF, Marks R, Collins N, Warner B, Frick L. Benefits of multidisciplinary case conferencing using audiovisual compared with telephone communication: a randomized controlled trial. J Telemed Telecare. 2004;10(6):351–354. | |
Manser T. Teamwork and patient safety in dynamic domains of healthcare: a review of the literature. Acta Anaesthesiol Scand. 2009;53(2):143–151. | |
McCulloch P, Rathbone J, Catchpole K. Interventions to improve teamwork and communications among healthcare staff. Br J Surg. 2011;98(4):469–479. | |
Greenberg CC, Regenbogen SE, Studdert DM, et al. Patterns of communication breakdowns resulting in injury to surgical patients. J Am Coll Surg. 2007;204(4):533–540. | |
Rosenstein AH, O’Daniel M. Impact and implications of disruptive behavior in the perioperative arena. J Am Coll Surg. 2006;203(1):96–105. | |
Kennedy TJ, Regehr G, Baker GR, Lingard L. Preserving professional credibility: grounded theory study of medical trainees’ requests for clinical support. BMJ. 2009;338:b128. | |
Morinaga K, Ohtsubo Y, Yamauchi K, Shimada Y. Doctors’ traits perceived by Japanese nurses as communication barriers: a questionnaire survey. Int J Nurs Stud. 2008;45(5):740–749. | |
Kawaguchi T. Certified diabetes expert nurse and nurse educators in Japan. Diabetes Res Clin Pract. 2007;77(Suppl 1):S205–S207. | |
Kahn LS, Tumiel-Berhalter L, D’Aniello R, et al. The impact of “growing our own”: a pilot project to address health disparities by training health professionals to become certified diabetes educators in safety net practices. Diabetes Educ. 2012;38(1):86–93. | |
Moran K, Burson R, Critchett J, Olla P. Exploring the cost and clinical outcomes of integrating the registered nurse-certified diabetes educator into the patient-centered medical home. Diabetes Educ. 2011;37(6):780–793. | |
Burke SD, Sherr D, Lipman RD. Partnering with diabetes educators to improve patient outcomes. Diabetes Metab Syndr Obes. 2014;7:45–53. | |
Hojat M, Nasca TJ, Cohen MJ, et al. Attitudes toward physician-nurse collaboration: a cross-cultural study of male and female physicians and nurses in the United States and Mexico. Nurs Res. 2001;50(2):123–128. | |
Vanderwielen LM, Vanderbilt AA, Dumke EK, et al. Improving public health through student-led interprofessional extracurricular education and collaboration: a conceptual framework. J Multidiscip Healthc. 2014;7:105–110. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.