Back to Journals » International Medical Case Reports Journal » Volume 19
The Development of Choroidal Osteoma in an Eye with Punctate Inner Choroidopathy: A Case Report and Review of Literature
Authors Khan AA, Magliyah MS ![]() , Al-Dhibi HA
, Al-Dhibi HA ![]()
Received 25 January 2026
Accepted for publication 10 April 2026
Published 15 May 2026 Volume 2026:19 598774
DOI https://doi.org/10.2147/IMCRJ.S598774
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Giuseppe Giannaccare
Abdulrahman A Khan, Moustafa S Magliyah, Hassan A Al-Dhibi
Vitreoretinal and Uveitis Divisions, King Khaled Eye Specialist Hospital, Riyadh, Saudi Arabia
Correspondence: Moustafa S Magliyah, Vitreoretinal and Uveitis Division, King Khaled Eye Specialist Hospital, PO Box 7141, Riyadh, 11462, Saudi Arabia, Email [email protected]; [email protected]
Purpose: To report a case of Choroidal osteoma developing in a patient known to have punctate inner choroidopathy (PIC) and to demonstrate the development and progression of the choroidal osteoma (CO) over fifteen years of follow-up.
Methods: Retrospective case report and review of the literature.
Results: A 44-year-old male who was diagnosed with PIC in both eyes, which was complicated with a choroidal neovascular membrane (CNVM) in the left eye, received systemic treatment, including oral prednisolone and mycophenolate mofetil to treat PIC, and intravitreal injection of anti-vascular endothelial growth factors (Anti-VEGF). Over fifteen years, a progressively enlarging juxta-foveal choroidal osteoma developed, which was confirmed by B-scan ultrasonography and multimodal imaging.
Conclusion: The diagnosis of choroidal osteoma in the setting of PIC can be diagnostically challenging, especially at early stages. As both conditions can lead to the development of CNVM, a high index of suspicion is needed to diagnose these cases.
Keywords: choroidal osteoma, punctate inner choroidopathy, choroidal neovascular membrane
Introduction
Choroidal osteoma (CO) is a rare benign choroidal tumor composed of mature bone. It usually appears as a unilateral yellowish lesion in the juxtapapillary or macular area.1 The exact causes of CO are still mostly unknown. Hereditary, traumatic, and hormonal factors have been considered.1 Inflammation is another possible predisposing factor for CO development. Few studies reported inflammation before CO development.2–7 Punctate inner choroidopathy (PIC) is an idiopathic inflammatory disease involving the choroid. PIC is diagnosed based on findings on clinical examination and multimodal imaging after ruling out other infectious and inflammatory causes.8 To our knowledge, the possible link between PIC and CO has not been previously reported; therefore, we present a case of PIC with secondary CO that developed over fifteen years.
Case Presentation
A 44-year-old male, not known to have any systemic medical illnesses, presented to our services in 2010, with blurred vision and metamorphopsia in the left eye. On examination, his best corrected visual acuity (BCVA) was 20/20 in the right eye and 20/100 in the left eye. Anterior segment examination was unremarkable in both eyes. Posterior segment examination showed bilateral multiple small punctate hypopigmented choroidal lesions in the posterior pole as well as a choroidal neovascular membrane (CNVM) in the left eye (Figure 1A and B). Fundus fluorescein angiography (FFA) showed early hyperfluorescence and late staining of the choroidal lesions, as well as fluorescein leakage from the CNVM in the left eye (Figure 1C and D). Spectral domain Optical coherence tomography (OCT) of the right eye revealed non-central outer retinal hyperreflectivity and RPE nodularity, while the left eye OCT showed a subretinal hyperreflective lesion with intraretinal fluid (Figure 1E and F). His uveitis workup, including a purified tuberculin skin test, QuantiFERON, rapid plasma reagin (RPR), Treponema pallidum Hemagglutination Assay (TPHA), chest imaging, and complete blood count, was unremarkable. Thus, he was diagnosed with PIC in both eyes and active CNVM in the left eye. The patient received oral prednisolone 1mg/kg/day, which was tapered weekly until 7.5 mg/day as maintenance, and was started on mycophenolate mofetil 1.5 g twice daily. Bevacizumab intravitreal injection was given to treat his active CNVM in the left eye. On further follow-up, multiple Anti-vascular endothelial growth factor (VEGF) injections were given to treat the left eye CNVM. Table 1 summarizes the CNVM treatment received. A left eye juxtapapillary yellowish lesion temporal to the optic disc and nasal to the CNVM scar was seen during follow-up, and demonstrated slow enlargement towards the superior macula over the years, with no clear extension in other directions. Over 9 years of follow-up, his BCVA was maintained 20/20 in the right eye and 20/25 in the left eye. In 2019, he presented with progressive worsening of his vision and BCVA of 20/20 and 20/40. His anterior segment examination, including intraocular pressure, was unremarkable. Fundus examination showed inactive PIC scars in both eyes and inactive CNVM in the left eye (Figure 2A). OCT showed choroidal thickening with intact retinal layers (Figure 2B). B-scan ultrasonography disclosed hyperechoic calcification corresponding to the choroidal osteoma with posterior shadowing (Figure 2C). The patient was diagnosed with a juxtapapillary CO in the left eye. Throughout 6 years of follow-up, the patient had two episodes of reactivation of CNVM, which were treated with further intravitreal injections. On his final follow-up, he had a BCVA of 20/20 and 20/40 in the right and left eye, respectively, with slightly enlarged CO and inactive CNVM (Figure 3). The serial examinations of the left eye throughout the follow-up duration are included in Supplemental Figure 1.
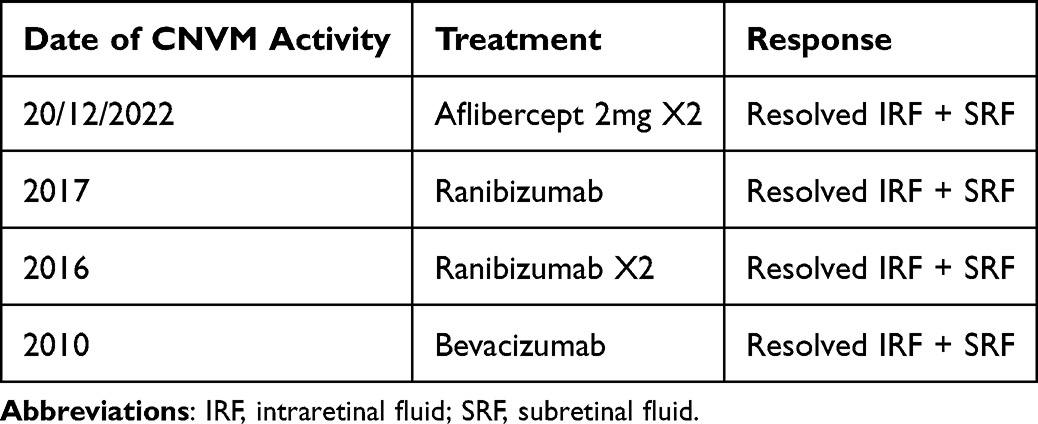 |
Table 1 Choroidal Neovascular Membrane Treatment |
 |
Figure 1 (A and B) Color fundus photos showing bilateral multiple small punctate hypopigmented choroidal lesions in the posterior pole in both eyes (asterisks), as well as a choroidal neovascular membrane (CNVM) in the left eye (white arrow). (C and D) are fundus fluorescein angiography (FFA) photos showing early hyperfluorescence and late staining of the choroidal lesions in both eyes, as well as fluorescein leakage from the CNVM in the left eye. (E and F) are spectral domain Optical coherence tomography (OCT) photos of both eyes, revealing non-central outer retinal hyperreflectivity and RPE nodularity (white arrow), while the left eye OCT showed a subretinal hyperreflective lesion with intraretinal fluid. |
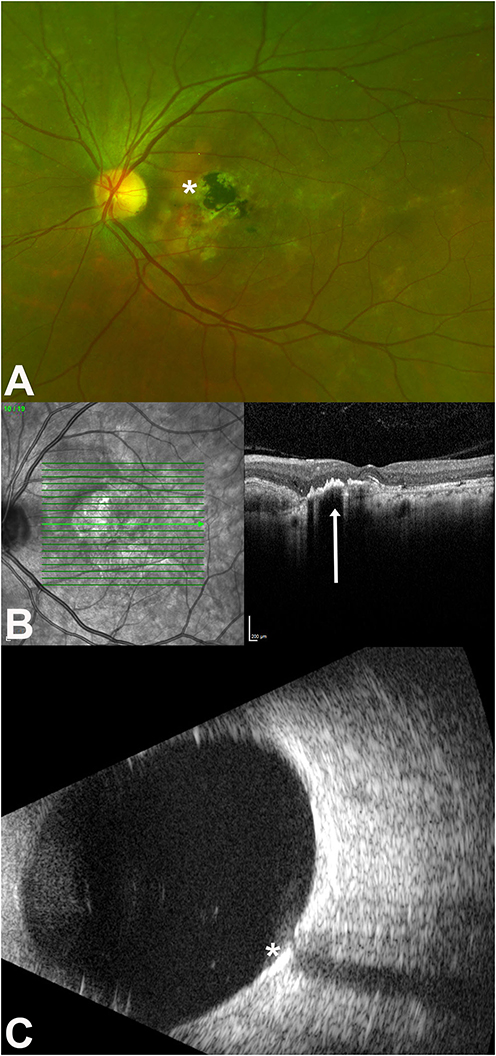 |
Figure 2 (A) is a color fundus photo showing inactive PIC scars and inactive CNVM (asterisk) in the left eye. (B) is an OCT showing choroidal thickening (white arrow) with intact retinal layers. (C) is a B-scan ultrasonography of the left eye, showing hyperechoic calcification corresponding to the choroidal osteoma with posterior shadowing (asterisk). |
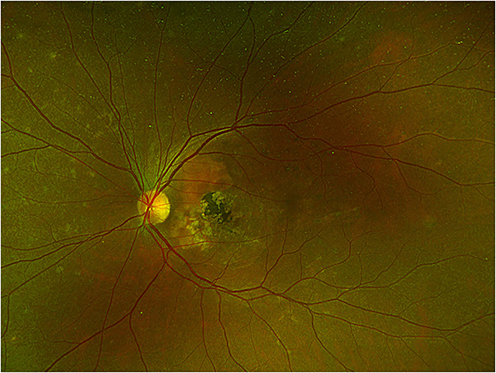 |
Figure 3 Color fundus photo of the left eye showing slightly enlarged CO and inactive CNVM. |
Discussion
We reported the longitudinal progression of choroidal osteoma over fifteen years of follow-up in a patient known to have PIC. PIC is characterized by multiple small, yellowish, well-defined macular lesions typically occurring in young myopic patients. Other differential diagnoses of PIC, including ocular tuberculosis, syphilis, and sarcoidosis, must be ruled out with appropriate laboratory investigations and imaging studies. Well-known vision-threatening complications of PIC include subretinal fibrosis and CNVM.8 Bruch’s membrane injury secondary to inner choroidal inflammation is the likely cause of CNVM occurrence in PIC. Different treatment modalities have been used in the past to treat CNVM secondary to PIC, including photodynamic therapy and surgical removal.9,10 Most recently, anti-VEGF medications have been used with favorable outcomes to treat PIC-related CNVM.11 Controlling inflammation in PIC with systemic immunomodulating therapy has been shown to decrease the recurrence of CNVM.12 Our patient was diagnosed with PIC in both eyes, which required prolonged use of mycophenolate mofetil to maintain remission. CNVM developed in his left eye, which responded well to anti-VEGF intravitreal injections, and fortunately, he can maintain good vision.
CO is a benign choroidal tumor that most commonly occurs in otherwise healthy individuals. The histopathology of CO involves bony trabeculae confined within the choroid with cavernous vascular spaces and small capillaries.12 Cellular components of the tumor include osteocytes, osteoclasts, and osteoblasts.12 The exact cause of CO is still not identified; however, hereditary, traumatic, hormonal, and inflammatory causes have been speculated.1–7 Upon reviewing the literature, we found that the development of CO after a diagnosis of PIC has not been reported. This occurrence of CO after a diagnosis of PIC suggests a possible causal relationship. Dystrophic calcification, which develops secondary to ocular inflammation, has been reported previously.13 Only a few studies reported the occurrence of CO secondary to a previous uveitis diagnosis. In particular, CO has been reported to occur in patients with a prior diagnosis of panuveitis or scleritis.2–7 Table 2 summarizes the characteristics of these cases. The cause of CO in most of these cases is thought to be related to inflammation. We believe that choroidal inflammation in our patient may have contributed to the secondary CO occurrence, with the exact pathogenesis still unknown at this time. In most previous reports, CO was diagnosed many years after the initial uveitis diagnosis. Similarly, our patient was diagnosed with CO 15 years after his initial PIC diagnosis, suggesting a possible prolonged effect and lasting impact of intraocular inflammation even when controlled with medications, and highlighting the slow growth and challenging diagnosis of CO. Three of the previously reported cases were associated with CNVM, which is a known complication of CO. CNVM secondary to CO has been reported to occur in 46% of eyes after 20 years of follow up.14 Retinal pigment epithelium and Bruch’s membrane damage are thought to cause the secondary CNVM. Treatment of CNVM associated with CO with anti-VEGF medications has been reported to improve vision.15 Our patient is considered at increased risk of developing CNVM since he has PIC, which then developed CO, both of which are well known to be associated with CNVM. Vision outcomes of previously reported cases of CO associated with uveitis are generally good, especially if not complicated by decalcification and CNVM.
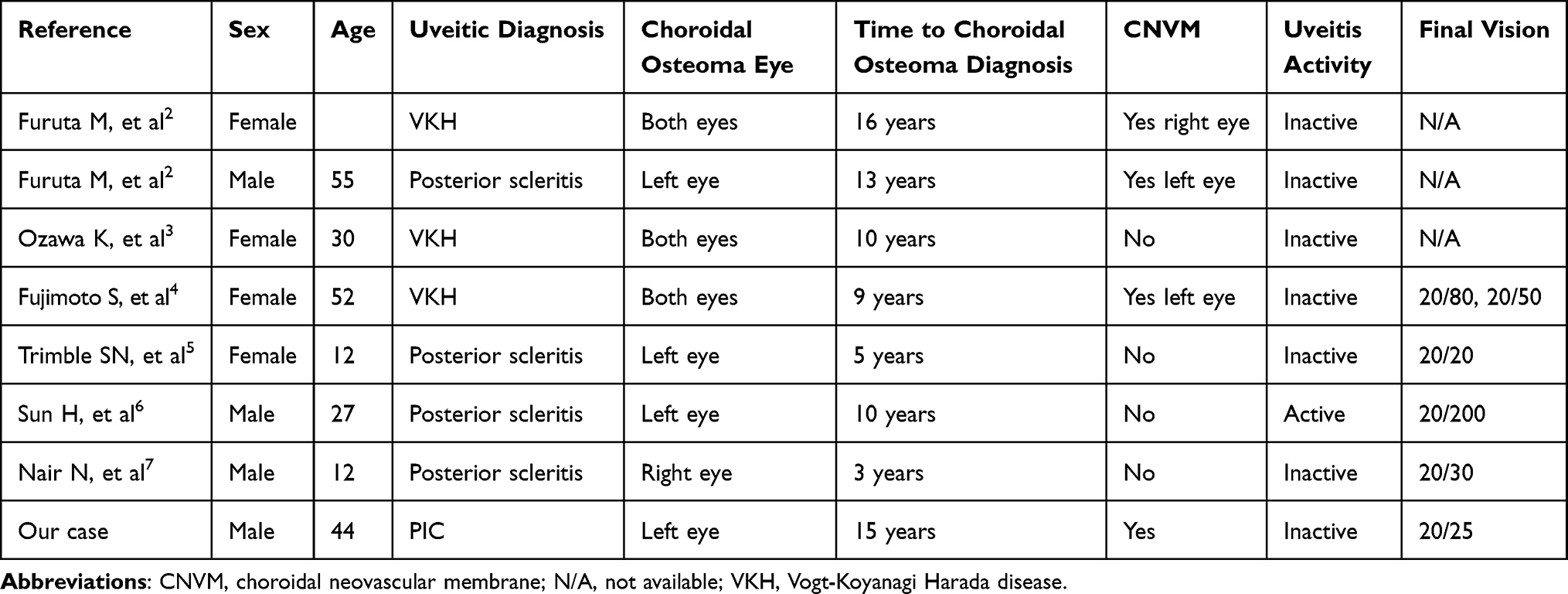 |
Table 2 Characteristics of Previously Reported Choroidal Osteoma Cases Associated with Ocular Inflammation |
The differential diagnosis of CO involves other neoplastic tumors like choroidal metastasis, choroidal hemangioma, and amelanotic melanoma Additionally, Inflammatory etiologies such as choroidal granuloma and nodular posterior scleritis are also in the differential diagnosis of CO1 Multimodal imaging can be invaluable in confirming the diagnosis of CO and differentiating it from other inflammatory and neoplastic conditions.
Patients with uveitis are at increased risk of loss of vision due to various complications, including cataract, glaucoma, and CNVM The development of CO can further lead to poor vision if complicated by CNVM, tumor decalcification, or tumor growth Recognizing CO in patients with known uveitis is crucial to closely monitor for potential complications that may require further treatment and to prevent misdiagnosing CO as a recurrence of inflammation, which can lead to unnecessary escalation of systemic immunomodulating medications.
Conclusion
To our knowledge, this is the first case that documents the development and progression of CO in the setting of PIC. As CNVM is a known complication in patients with PIC, the focus on the diagnosis and treatment of CNVM might lead to delayed discovery of CO in these patients. The progression of CO over long-term follow-ups in uveitis patients requires careful assessments using multimodal imaging. Further studies are needed to elucidate the exact pathogenesis of CO in the setting of ocular inflammation.
Ethical Approval
This study adhered to the tenets of the Declaration of Helsinki in 1964 and its amendments. The study was approved by the Institutional Review Board (IRB) at King Khaled Eye Specialist Hospital (KKESH), IRB number: RP 25196-CR.
Patient Consent
Written consent to publish this case has been obtained from the patient himself.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shields CL, Shields JA, Augsburger JJ. Choroidal osteoma. Surv Ophthalmol. 1988;33(1):17–6. PMID: 3051466. doi:10.1016/0039-6257(88)90069-0
2. Furuta M, Tanaka K, Maeda S, et al. Secondary choroidal osteoma in the setting of uveal pathology: 4 case reports and review. Ocul Oncol Pathol. 2025;11(4):237–247. PMID: 41064687. doi:10.1159/000548250
3. Ozawa K, Iwase T, Ito Y, et al. Multimodal imaging in bilateral nature of the choroidal osteoma after intraocular inflammation caused by Harada disease. Retina. 2019;39(9):e40–e41. PMID: 31306294. doi:10.1097/IAE.0000000000002611
4. Fujimoto S, Maruyama K, Shunto T, Nishida K. Serous retinal detachment secondary to bilateral choroidal osteoma successfully treated with subscleral sclerectomy: a case report. Am J Ophthalmol Case Rep. 2025;37:102249. PMID: 39877518; PMCID: PMC11773265. doi:10.1016/j.ajoc.2025.102249
5. Trimble SN, Schatz H. Choroidal osteoma after intraocular inflammation. Am J Ophthalmol. 1983;96(6):759–764. PMID: 6419617. doi:10.1016/s0002-9394(14)71921-x
6. Sun H, Yang S, Wang Q, Zhou X, Zheng Z, Zheng M. Choroidal osteoma secondary to chronic posterior scleritis: a case report and literature review. Indian J Ophthalmol Case Rep. 2024;4:506–510. doi:10.4103/IJO.IJO_2375_23
7. Nair N, Abraham S, Ganesh SK. Recurrent posterior scleritis with secondary choroidal osteoma in a child. Indian J Ophthalmol. 2020;68:2509–2511. doi:10.4103/ijo.IJO_521_20
8. Gerstenblith AT, Thorne JE, Sobrin L, et al. Punctate inner choroidopathy: a survey analysis of 77 persons. Ophthalmology. 2007;114(6):1201–1204. PMID: 17434588. doi:10.1016/j.ophtha.2006.10.047
9. Fong KC, Thomas D, Amin K, Inzerillo D, Horgan SE. Photodynamic therapy combined with systemic corticosteroids for choroidal neovascularisation secondary to punctate inner choroidopathy. Eye. 2008;22(4):528–533. PMID: 17237756. doi:10.1038/sj.eye.6702688
10. Olsen TW, Capone A, Sternberg P, Grossniklaus HE, Martin DF, Aaberg TM. Subfoveal choroidal neovascularization in punctate inner choroidopathy. Surgical management and pathologic findings. Ophthalmology. 1996;103:2061–2069. doi:10.1016/S0161-6420(96)30387-4
11. Wu W, Li S, Xu H, et al. Treatment of punctate inner choroidopathy with choroidal neovascularization using corticosteroid and intravitreal ranibizumab. Biomed Res Int. 2018;2018:1585803. PMID: 30302336. doi:10.1155/2018/1585803
12. Williams AT, Font RL, Van Dyk HJ, Riekhof FT. Osseous choristoma of the choroid simulating a choroidal melanoma. Association with a positive 32P test. Arch Ophthalmol. 1978;96(10):1874–1877. PMID: 697626. doi:10.1001/archopht.1978.03910060378017
13. Zeiter HJ. Calcification and ossification in ocular tissue. Am J Ophthalmol. 1962;53:265–274. PMID: 14010033. doi:10.1016/0002-9394(62)91174-1
14. Shields CL, Sun H, Demirci H, Shields JA. Factors predictive of tumor growth, tumor decalcification, choroidal neovascularization, and visual outcome in 74 eyes with choroidal osteoma. Arch Ophthalmol. 2005;123(12):1658–1666. PMID: 16344436. doi:10.1001/archopht.123.12.1658
15. Zhang Y, Fang J, Zhao S, She X, Wang J, Shen L. Secondary choroidal neovascularization due to choroidal osteoma after 9 years of follow-up. BMC Ophthalmol. 2021;21(1):242. PMID: 34058993. doi:10.1186/s12886-021-02004-3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.