Back to Journals » Medical Devices: Evidence and Research » Volume 19
The Design and Development of a Novel Device that Converts a Patient-Controlled Intravenous Pump into an Oral Liquid Medication Dispenser for Non-Controlled Substances
Authors El-Khalili T ![]() , Varma L, Yung KY, Li J
, Varma L, Yung KY, Li J ![]() , Wiznia D
, Wiznia D ![]()
Received 18 November 2025
Accepted for publication 4 February 2026
Published 12 February 2026 Volume 2026:19 582446
DOI https://doi.org/10.2147/MDER.S582446
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Mohamad Bashir
Taj El-Khalili,1 Lara Varma,2 Karley Yanlam Yung,2 Jinlei Li,3 Daniel Wiznia4
1Yale School of Medicine, Yale University, New Haven, CT, USA; 2Yale School of Engineering & Applied Science, Yale University, New Haven, CT, USA; 3Yale School of Medicine, Department of Anesthesiology, Yale School of Medicine, Yale University, New Haven, CT, USA; 4Yale School of Medicine, Department of Orthopedics & Rehabilitation, Yale School of Medicine, Yale University, New Haven, CT, USA
Correspondence: Taj El-Khalili, Yale School of Medicine, Yale University, New Haven, CT, USA, Tel +1 765 412 5757, Email [email protected]
Background: Timely administration of oral medications is a significant inpatient challenge, particularly in the context of postoperative pain management with limited nursing resources. Delays in delivering non-opioid analgesics, such as acetaminophen, can result in poorly controlled pain and increased opioid use.
Methods: To address this gap, we developed the Patient-Controlled Oral Liquid Dispenser (P-COLD), a novel bedside device that enables patients to self-administer non-controlled liquid medications within programmable safety parameters. The system integrates a hospital-grade intravenous patient-controlled analgesia (PCA) pump into a secure, 3D-printed housing that delivers precise doses of medication into a bedside cup upon patient request.
Results: The P-COLD was validated through laboratory testing and simulated-use evaluations without deployment in clinical patient care. Dose accuracy testing demonstrated consistent delivery within ± 5% of target volume. Simulated usability testing with healthy volunteers confirmed reliable patient operation with minimal instruction. Nursing staff successfully completed training and setup protocols, and time-motion analyses indicated potential reductions in workflow interruptions and nursing burden during as-needed (PRN) medication delivery.
Conclusion: The P-COLD was designed to enable patient-initiated delivery of non-controlled oral liquid medications without IV access and without requiring nurse presence at the bedside for each dose. Validation testing in the laboratory and through simulated use demonstrated accurate dosing, reliable usability, and favorable simulated workflow performance.
Plain Language Summary: In hospitals, patients often have to wait for a nurse to bring them medicine such as acetaminophen for pain or fever. These delays can leave patients in pain and lead to greater use of opioids to manage symptoms.
We created a new device, called the Patient-Controlled Oral Liquid Dispenser (P-COLD), that lets patients safely take certain liquid medicines by themselves at the bedside. The device uses a hospital pump placed inside a secure case. When the patient presses a button, the pump delivers a measured dose of medicine into a cup. Safety limits are built in so patients cannot take too much.
In testing, the device gave the right dose every time. Nurses and pharmacy staff were able to set it up quickly, and patients easily learned how to use it.
The P-COLD may improve comfort, reduce delays, and decrease the need for as many opioids by making timely, safer medicines available at the bedside. The platform is designed to support delivery of a range of non-controlled oral liquid medications, including antipyretics, antiemetics, bowel regimens, and electrolyte supplements.
Keywords: medical device design, oral solution medication delivery, patient-controlled analgesia, postoperative pain management, nursing staffing
Introduction
Timely administration of oral medications is a persistent challenge in hospital care, particularly in the context of the ongoing national nursing shortage and increasingly complex inpatient populations. Among the most frequently prescribed inpatient medications is acetaminophen, a non-opioid analgesic often used as a first-line agent for postoperative pain control. Despite its favorable safety profile and availability over the counter, inpatients must rely on nurses for access to oral acetaminophen, contributing to frequent delays in administration and arguably misuse of scarce nursing resources.1,2 These delays not only undermine effective pain control but may increase opioid utilization, extend hospital stays, and reduce patient satisfaction.3,4
Patient-controlled analgesia (PCA) systems have transformed pain management by allowing patients to self-administer medication based on their real-time needs. Intravenous PCA (IV-PCA) remains the most common modality, providing effective control of opioids and other analgesics. However, IV-PCA requires continuous IV access, carries risks such as infection and opioid-related side effects, and often complicates the transition to outpatient care.5,6
In response, several oral PCA devices have been developed to allow patient-controlled delivery of oral tablets.7,8 While effective in concept, these systems have not achieved widespread adoption, largely due to safety concerns surrounding pill-based opioids, including the risks of misuse, diversion, and difficulty verifying ingestion, as noted by Riemondy et al.9
Additionally, many of the medications most frequently used in inpatient care—such as acetaminophen, lactulose, magnesium hydroxide, ondansetron, and electrolyte solutions—are administered in liquid form rather than pills. These oral solutions represent a significant but under-addressed source of nursing workload and inefficiency.10–12 Compared to tablets, liquid medications often offer faster absorption, greater dosing flexibility, and easier administration for patients with swallowing difficulties, as reported by Ameer et al.11
To address this gap, we developed the Patient-Controlled Oral Liquid Dispenser (P-COLD), a bedside device that allows patients to self-administer non-controlled oral solutions safely, accurately, and without nurse assistance, as described by Wiznia et al.13 This paper describes the design and validation of the P-COLD system using acetaminophen as a model agent, with a focus on clinical usability, dosing performance, and potential impact on pain management and hospital workflow.
Methods
Design Objectives
Design criteria for the P-COLD were informed by clinical discussions with hospital staff and focused on four core goals:
- Usability: Patients with varying levels of dexterity and cognition must be able to operate the device independently.
- Safety: Medication delivery must be time-locked, accurate, and within prescribed limits.
- Security: The design must prevent tampering or unauthorized access.
- Workflow Integration: Setup should require minimal training and reduce nurse workload.
Development Process
The device was developed through iterative CAD modeling and 3D printing using materials that could be cleaned with a bleach wipe in the hospital. The final configuration included four main components: a base unit, a reinforced lid with access ports, a pump cover with a viewing window, and a tube guide to position the medication stream. These modular components are shown in Figure 1, which highlights how each piece contributes to mechanical security and clinical usability.
 |
Figure 1 Modular components of the P-COLD device. The final device configuration includes four primary parts: (1) the base unit, which provides structural integrity and includes attachment points for secure fastening. All components were designed for 3D printing using hospital-cleanable materials and optimized for rapid assembly, durability, and compatibility with standard PCA pumps and hospital bedside tables. (2) the lid assembly, which features a medication cup recess and a dedicated cradle for the PCA remote, allowing intuitive patient activation and secure wire routing; and (3) the infusion pump cover, which securely encloses the pump and includes a transparent acrylic window for display visibility while preventing unauthorized access to control buttons; (4) the tube stand, which ensures precise and stable alignment of the medication tubing with the bedside cup. |
A total of three design generations were created and evaluated, with each iteration optimized for compatibility with standard PCA pumps and bedside tables:
Generation 1: Core Layout and Interface Concept
The initial prototype established the foundational geometry and mechanical arrangement of the device, including the PCA pump housing, a basic medication cup recess, and a remote cradle for patient activation. This generation prioritized ease of assembly and initial feasibility testing. Key features included a removable lid, basic tube guide, and window cutout for pump display visibility.
Generation 2: Structural Reinforcement and Improved Delivery Path
Based on mechanical testing and usability feedback, the second generation incorporated thicker structural walls, reinforced pegs and lid attachments, and a repositioned pump slot to improve alignment with standard PCA hardware. The tube stand was extended and better aligned with the cup receptacle to ensure consistent medication stream placement and reduce spillage risk.
Generation 3 (Final): Secure, Tamper-Resistant, and Ergonomic Configuration
The final iteration focused on clinical usability, safety, and security. Screw fasteners were added for tamper resistance and modular disassembly. A custom pump cover with a clear acrylic window was developed to allow dose monitoring while blocking access to physical controls. The tube stand was integrated into the pump cover for additional rigidity, and the PCA remote cradle was reoriented for intuitive patient access. Lid tabs were also added to streamline nurse setup and maintain housing alignment. The final assembled generation of the device, including key clinical interaction features, is shown in Figure 2.
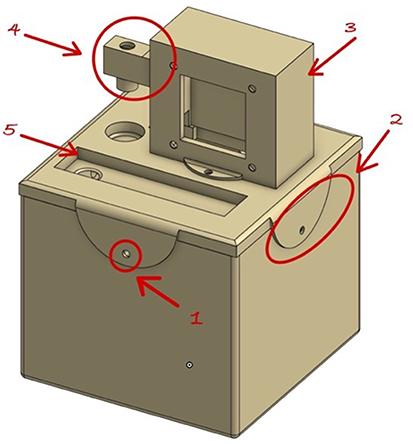 |
Figure 2 Device final assembly. (1) Nuts and screws were incorporated at major joints to enable durable, tamper-resistant assembly and allow for disassembly during maintenance or cleaning. (2) Lid tabs were added to improve alignment and mechanical stability between the lid and base during repeated use. (3) A custom pump cover was fabricated with a transparent acrylic viewing window that maintains visibility of the pump display while physically blocking access to control buttons, preserving programmed safety parameters. (4) The tube stand was integrated into the pump cover as a fixed, rigid guide to ensure precise alignment of the medication stream with the patient’s bedside cup. (5) The PCA remote cradle was repositioned to improve patient ergonomics, allowing intuitive activation while maintaining secure cable routing to the infusion pump. |
Clinical Workflow
The following steps outline the clinical workflow for integrating the P-COLD device into hospital care:
- A physician enters an order for a non-controlled liquid medication (eg, acetaminophen).
- Pharmacy staff prepare the medication, program the PCA pump with safety parameters, and load the liquid into the reservoir.
- Nursing staff retrieve the prepared P-COLD device, scan a QR code to access setup instructions, and place the system at the patient’s bedside.
- Patient uses a PCA-style remote to request doses, which are delivered into a cup within programmable safety limits.
- Dose events are logged and uploaded to the patient’s electronic health record by the Nurse.
Validation Testing
Dosing Accuracy
Bench testing was conducted to assess the precision of liquid medication delivery across multiple P-COLD devices. Calibrated pipettes and graduated cylinders were used to measure both single-dose and repeated-dose performance. Tests were conducted over 24–48-hour simulated use periods to examine consistency, accuracy, and potential mechanical drift.
Security and Tamper Resistance
Simulated unauthorized access attempts were conducted, including forceful entry, manipulation of tubing, and attempts to override pump-programmed lockout intervals. The device was evaluated for physical tamper resistance and the maintenance of PCA pump safety settings while enclosed.
Physical Compatibility
Device dimensions (approximately 8×8×10 cm) were evaluated for compatibility with standard hospital bedside tables and hospital room layouts. The visibility of the infusion pump screen was assessed under high and low ambient lighting conditions through the transparent viewing window. QR code readability was assessed using a range of smartphone models under varied lighting environments, simulating typical bedside conditions. The codes linked to setup instructions and training videos intended to support nurse and pharmacy staff during device deployment.
Usability and Workflow Testing
Simulated Patient Operation
Healthy volunteers were instructed to operate the device using only the PCA-style remote and visual prompts without external assistance. Observations focused on ease of use and successful medication request execution.
Nurse Setup and Training
Pharmacy and nursing staff participated in standardized device setup and training protocols. Instructions were accessed via QR codes on the device housing. Setup completion rates, time, and subjective usability feedback were recorded.
Time-Motion Workflow Evaluation
A time-motion study protocol was developed to compare nurse workload between standard PRN medication delivery and P-COLD-assisted delivery. The frequency and duration of staff interventions were recorded in a controlled, simulated clinical environment.
Clinical Implementation Planning
An IRB-approved pilot clinical study protocol was developed to evaluate the P-COLD system’s real-world application for acetaminophen delivery in postoperative patients. The protocol includes metrics such as medication request-to-delivery time, nurse-reported burden, patient satisfaction, and system usability. Staff training resources were made available bedside via scannable QR codes.
Results
Dosing Accuracy and Reliability
All P-COLD devices delivered single and repeated doses within ±5% of the programmed volume. Testing over extended simulated use demonstrated consistent accuracy and no measurable performance drift (Table 1). These findings exceed standard regulatory thresholds for oral liquid medication accuracy.14–16
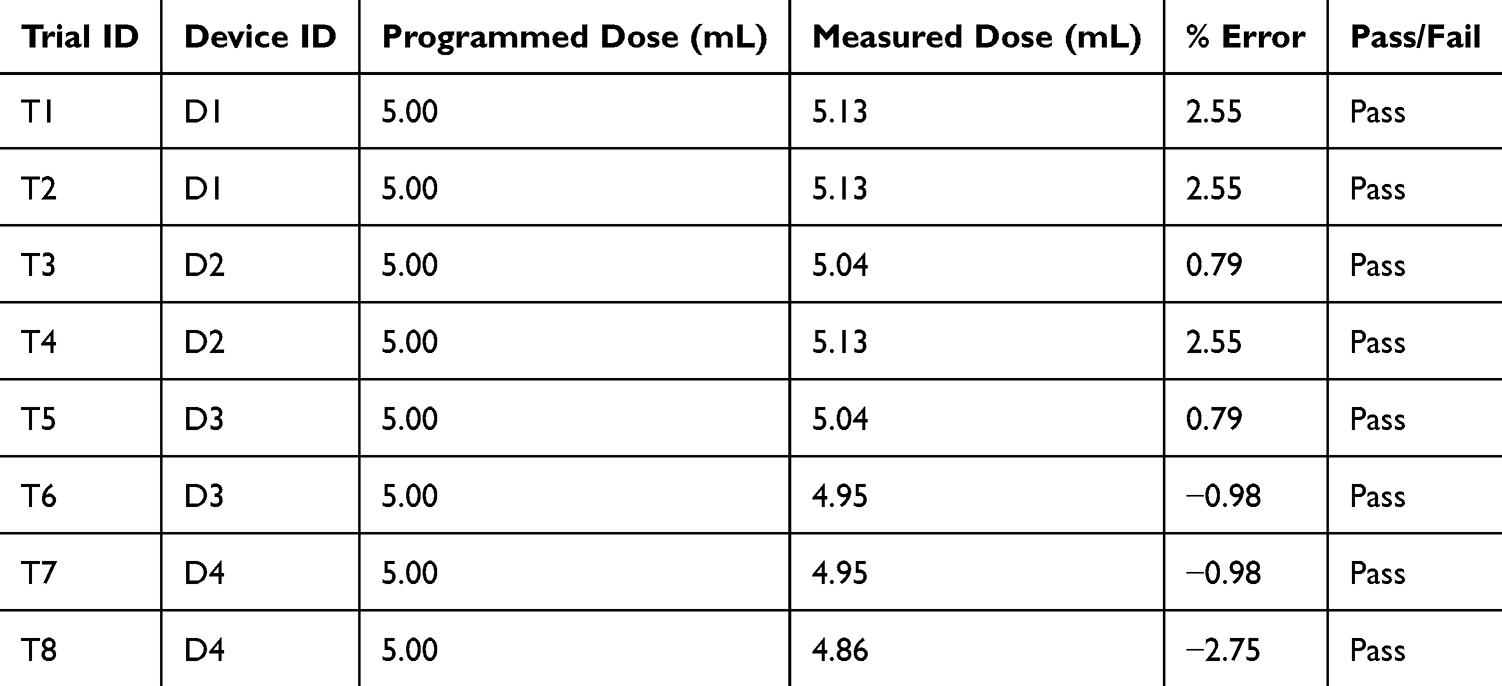 |
Table 1 Dosing Accuracy Across Simulated Use Period |
All dosing tests were conducted using high-precision analytical scales. Measured weights were converted to volume using the known density of the acetaminophen solution. Testing was performed over a 48-hour simulated-use period, and all results were evaluated against an acceptable error margin of ±5%.
Security and Tamper Resistance
In all simulated breach scenarios, the device housing prevented access to medication or override of programmed safety features (Table 2). The PCA pump’s internal dose limits and lockout parameters remained fully functional and protected throughout testing, demonstrating the mechanical security of the system.
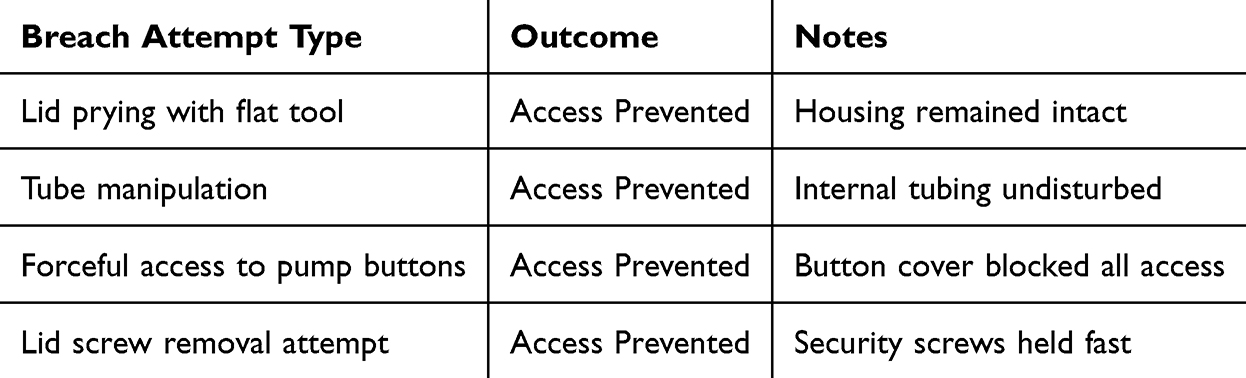 |
Table 2 Tamper Resistance Evaluation Outcomes |
Physical Compatibility and Device Visibility
The device fit securely on standard hospital bedside tables and did not interfere with adjacent equipment or room layout. The infusion pump display was visible under both low and bright light conditions. QR codes affixed to the housing were consistently scannable across multiple smartphone models, enabling access to digital training resources.
Usability Testing (Table 3)
Nurse Setup and Training
All nursing and pharmacy participants successfully completed the setup protocol independently (Table 3). Training materials accessed via QR code were rated clear and usable, and setup times were reported as shorter than traditional PRN oral medication administration.
 |
Table 3 Usability Testing Outcomes |
Simulated Patient Operation
All healthy volunteers were able to activate the device and receive a programmed dose using the PCA-style remote. The user interface was rated intuitive, with successful operation observed across a range of dexterity levels.
Workflow Integration
Time-motion analysis showed that P-COLD use reduced nurse intervention frequency and duration compared to traditional PRN oral medication administration (Table 4). Nurses were not required to be physically present at the bedside during medication delivery, and total time per event was decreased.
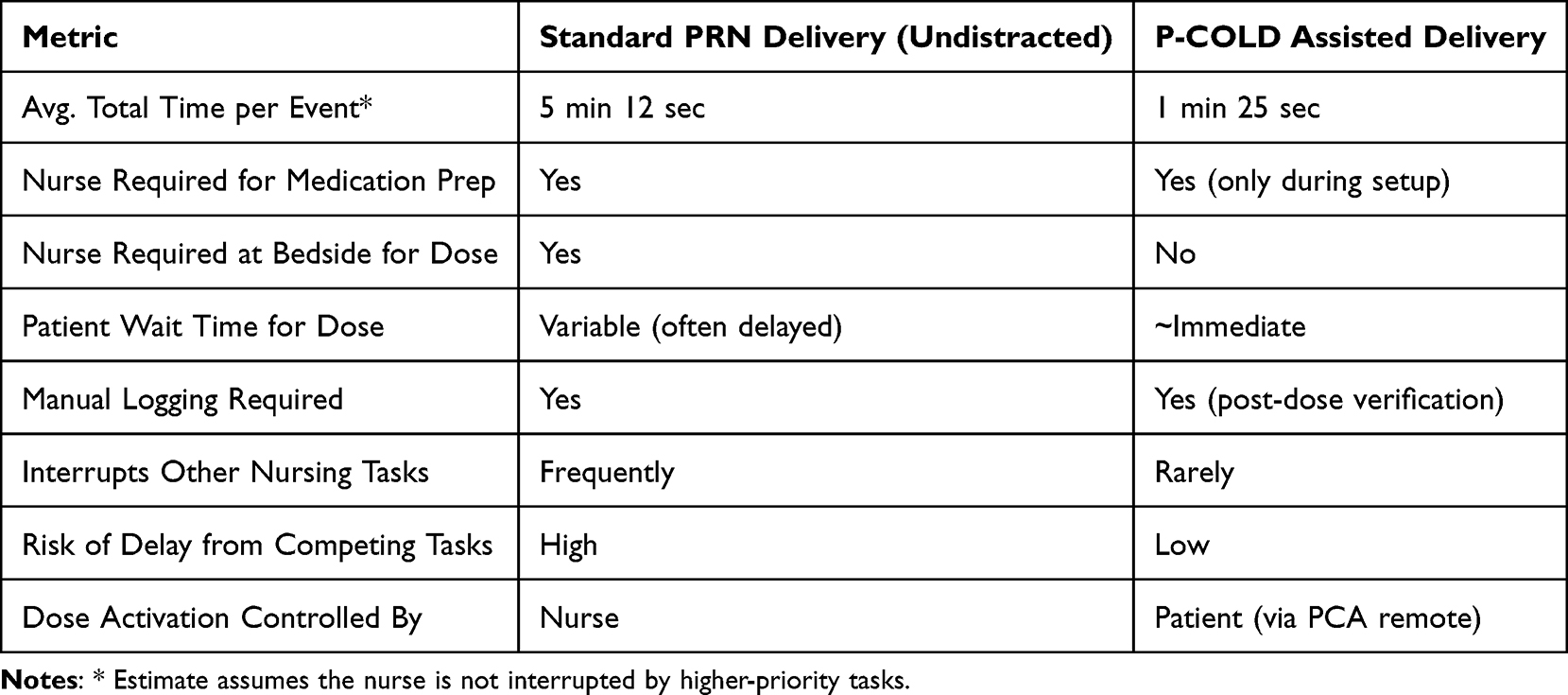 |
Table 4 Time-Motion Comparison – Nurse Involvement and Workflow Burden |
Clinical Trial Preparation
Following validation, the pilot trial began enrolling postoperative patients to evaluate clinical effectiveness, patient experience, and impact on nurse workload. Survey instruments were deployed to capture quantitative and qualitative data on medication delivery, patient satisfaction, and workflow integration.
Discussion
The P-COLD system represents a novel approach to patient-controlled oral solution medication delivery that eliminates the need for intravenous access or direct nurse involvement. By providing a mechanism for patient-initiated access to non-controlled liquid medications, the device addresses design limitations associated with traditional oral medication administration workflows —particularly for high-frequency agents such as acetaminophen. Bench and simulated-use testing confirmed that the P-COLD delivers medication with high precision, preserves programmable safety features, and can be operated reliably by both patients and nursing staff with minimal training.
Unlike traditional intravenous PCA systems, which require invasive intravenous lines and transition to oral format, P-COLD offers a non-invasive solution suited for a broad range of patients and clinical contexts. Prior oral PCA systems, such as pill-based devices like the PCoA® Acute, have demonstrated feasibility in reducing nursing burden and improving patient satisfaction.8–12 However, these systems have struggled with adoption due to concerns over pill diversion, delayed onset of action, and patient adherence. The P-COLD system mitigates many of these concerns by using liquid medications that are fast-acting, non-controlled, and difficult to divert—making the device especially attractive for inpatient use.
Liquid formulations such as acetaminophen not only provide faster absorption than tablets but also avoid the mechanical risks associated with pill ingestion, particularly in patients with dysphagia or gastrointestinal intolerance, as reported by Ameer et al.11 Furthermore, because liquid medications are already commonly administered on medical-surgical floors, the P-COLD device requires minimal adaptation to existing pharmacy workflows.
Clinically, this approach has the potential to improve patient autonomy, reduce nurse workload, and streamline postoperative care. Our time-motion observations suggest that P-COLD may meaningfully reduce the number and duration of nurse interventions for both around the clock and PRN medications, allowing staff to focus on higher-acuity tasks. In addition, the device may facilitate earlier mobilization and discharge by providing patients with greater control over their symptom management.
This study has several limitations. First, the device has not yet been used in a real-world patient population, and no clinical outcome data are reported in this study. While simulated use by healthy volunteers and staff training suggest high usability, clinical effectiveness and safety must be confirmed through ongoing trials in our health system. Second, the current generation is not integrated with electronic health record (EHR) systems, and dose logging is not yet automated. Additionally, broader clinical deployment will require alignment with FDA regulatory pathways, including a Class II 510(k) submission, as well as institutional device implementation processes such as internal review, staff training, and workflow integration. Finally, while the platform is designed for non-controlled medications, expansion to include controlled substances would require significant engineering development, to address regulatory and security requirements.
A pilot clinical study is currently underway to evaluate real-world performance in a postoperative care setting. Future work includes completing the ongoing pilot trial, evaluating patient outcomes and nurse-reported impact, and refining the system for broader hospital integration. Longer-term goals include EHR linkage, real-time monitoring, and development of a secure controlled-substance variant. The platform may also be adapted for outpatient or home use in select populations.
In summary, the P-COLD system provides a promising, patient-centered solution to a widespread clinical challenge. By combining patient-controlled access, dosing safeguards, and oral liquid delivery, it offers a scalable strategy for enhancing medication timeliness, reducing nursing burden, and improving the inpatient care experience. While clinical trials are ongoing, the current validation testing supports the feasibility of deploying this technology in hospital settings. With future integration into clinical documentation systems and potential adaptation for controlled substances, P-COLD represents a scalable platform for modernizing patient-directed medication delivery across a range of inpatient needs.
Conclusion
Unlike intravenous PCA systems, which require IV access, or pill-based oral PCA devices, which carry a higher risk of diversion, the P-COLD delivers fast-absorbing liquid medications without IV access, offering a novel, clinically practical approach to potentially improve inpatient medication delivery. By enabling patients to self-administer non-controlled liquid medications with precision and safety, the system addresses critical barriers in postoperative pain management, including delays in medication delivery due to high nursing workload. Validation testing confirmed reliable dose accuracy, mechanical security, and usability by both patients and clinical staff. The system integrates seamlessly into bedside workflows and may reduce risks of infection, diversion, and dependence while enhancing patient autonomy, ensuring timely medication delivery, and potentially improving staff efficiency. Clinical effectiveness, patient outcomes, and impacts on opioid utilization and length of stay remain to be established in ongoing and future patient-based studies.
Abbreviations
P-COLD, patient-controlled oral liquid dispenser; PCA, patient-controlled analgesia; PRN, as needed; EHR, electronic health record.
Data Sharing Statement
All data generated or analyzed during this study are included in this article and its tables and figures. No additional datasets were generated or analyzed.
Ethics Approval and Informed Consent
Device validation and usability testing with healthy adult volunteers, nursing staff, and pharmacy staff were conducted in accordance with the Declaration of Helsinki and under approval from the Yale University Institutional Review Board (Protocol #: 2000041518). All participants provided written informed consent prior to participation. A separate IRB-approved clinical pilot study evaluating the device in postoperative patients is ongoing; however, no data from that patient study are included in this manuscript.
Acknowledgments
The authors thank Professor Larry Wilen, PhD, at the Yale Center for Engineering Innovation and Design for providing prototyping guidance, access to fabrication resources, and materials support.
Funding
NIH grant R25EB030985 - Medical Device Design and Innovation; Orthopaedic Implant Failure Analysis and Redesign.
Disclosure
D. Wiznia and J. Li report patent “Patient-controlled liquid oral medicine dispenser and deactivation system”, US Patent 11,857,504, Jan. 23, 2024 issued to Yale University. The authors report no other conflicts of interest in this work.
References
1. Brown T. Excessive Acetaminophen dosing too common in hospitals. Medscape Medical News; 2012. Available from: https://www.medscape.com/viewarticle/774344.
2. Agency for Healthcare Research and Quality. Most commonly administered medications in U.S. hospitals. Healthcare Cost and Utilization Project (HCUP); 2020. Available from: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb234-Most-Common-Drugs-Hospitals.pdf.
3. Chou R, Gordon DB, de Leon-Casasola OA, et al. Management of postoperative pain: a clinical practice guideline from the American Pain Society, the American Society of Regional Anesthesia and Pain Medicine, and the American Society of Anesthesiologists’ Committee on Regional Anesthesia, Executive Committee, and Administrative Council. J Pain. 2016;17(2):131–9. doi:10.1016/j.jpain.2015.12.008
4. Joshi GP, Ogunnaike BO. Consequences of inadequate postoperative pain relief and chronic persistent postoperative pain. Anesthesiol Clin North Am. 2005;23(1):21–36. doi:10.1016/j.atc.2004.11.013
5. Pöpping DM, Zahn PK, Van Aken HK, Dasch B, Boche R, Pogatzki-Zahn EM. Effectiveness and safety of postoperative pain management: a survey of 18,925 consecutive patients between 1998 and 2006 (2nd revision): a database analysis of prospectively raised data. Br J Anaesth. 2008;101(6):832–840. doi:10.1093/bja/aen300
6. Schug SA, Ting S. Fentanyl formulations in the management of pain: an update. Drugs. 2017;77(7):747–763. doi:10.1007/s40265-017-0727-z
7. Collins L, Cata DM, Conley NS. A comparison study—oral patient-controlled analgesia versus traditional delivery of pain medication following orthopaedic procedures. Orthop Nurs. 2020;39(5):324–332. doi:10.1097/NOR.0000000000000697
8. Wirz S, Seidensticker S, Shtrichman R. Patient-controlled analgesia (PCA): intravenous administration (IV-PCA) versus oral administration (oral-PCA) by using a novel device (PCoA® Acute) for hospitalized patients with acute postoperative pain—a comparative retrospective study. Pain Res Manag. 2021;2021:2542010. doi:10.1155/2021/2542010
9. Riemondy S, Gonzalez L, Gosik K, Ricords A, Schirm V. Nurses’ perceptions and attitudes toward use of oral patient-controlled analgesia. Pain Manag Nurs. 2016;17(2):132–139. doi:10.1016/j.pmn.2016.02.051
10. Nuckols TK, Anderson LJ, Popescu I, et al. Economic evaluation of quality improvement interventions for pain management in hospitalized adults. JAMA Intern Med. 2013;173(10):904–912. doi:10.1001/jamainternmed.2013.276
11. Ameer B, Divoll M, Abernethy DR, Greenblatt DJ, Shargel L, Koch-Weser J. Absolute and relative bioavailability of oral Acetaminophen preparations. Clin Pharmacol Ther. 1983;33(3):301–306. doi:10.1038/clpt.1983.39
12. Mirza DH, Alkhatib M, Alkaissy M, et al. A single center exploratory survey of patients and nurses on post-surgical oral opioid delivery through patient-controlled analgesia. J Pain Res. 2024;17:2483–2494. doi:10.2147/JPR.S461379
13. Wiznia D, Li J, See C. Patient-controlled liquid oral medicine dispenser and deactivation system. US patent 11,857,504. Issued January 23, 2024.
14. United States Pharmacopeia. USP general chapter <905>: uniformity of dosage units; 2011. Available from: https://www.usp.org/sites/default/files/usp/document/harmonization/gen-method/q0304_stage_6_monograph_25_feb_2011.pdf.
15. US Food and Drug Administration. CFR – Code of Federal Regulations Title 21, Part 211, Subpart I – Laboratory controls; 2024. Available from: https://www.ecfr.gov/current/title-21/chapter-I/subchapter-C/part-211/subpart-I.
16. Moore RA, Derry S, Aldington D, Wiffen PJ. Single dose oral analgesics for acute postoperative pain in adults: an overview of Cochrane reviews. Cochrane Database Syst Rev. 2015;9:CD008659. doi:10.1002/14651858.CD008659.pub3
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.