Back to Journals » Clinical Ophthalmology » Volume 17
The Current Burden and Future Solutions for Preoperative Cataract-Refractive Evaluation Diagnostic Devices: A Modified Delphi Study
Authors Henderson BA, Aramberri J, Vann R ![]() , Abulafia A, Ainslie-Garcia M, Berdahl J, Ferko N, Gundersen KG
, Abulafia A, Ainslie-Garcia M, Berdahl J, Ferko N, Gundersen KG ![]() , Goto S, Gupta P
, Goto S, Gupta P ![]() , Multack S, Persaud E, Raoof D, Savini G, Shammas HJ
, Multack S, Persaud E, Raoof D, Savini G, Shammas HJ ![]() , Wang L, Wang WZ
, Wang L, Wang WZ ![]()
Received 21 March 2023
Accepted for publication 11 July 2023
Published 24 July 2023 Volume 2023:17 Pages 2109—2124
DOI https://doi.org/10.2147/OPTH.S412847
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Bonnie An Henderson,1 Jaime Aramberri,2 Robin Vann,3 Adi Abulafia,4 Margaret Ainslie-Garcia,5 John Berdahl,6 Nicole Ferko,5 Kjell Gunnar Gundersen,7 So Goto,8,9 Preeya Gupta,10,11 Samuel Multack,12– 14 Elizabeth Persaud,5 Duna Raoof,15 Giacomo Savini,16 H John Shammas,17 Li Wang,18 Wendy Zhi Wang5
1Department of Ophthalmology, Tufts University School of Medicine, Boston, MA, USA; 2Ophthalmology Clinic Miranza Begitek, San Sebastian, Spain; 3Department of Ophthalmology, Duke University School of Medicine, Durham, NC, USA; 4Department of Ophthalmology, Shaare Zedek Medical Center, Hadassah Faculty of Medicine, the Hebrew University, Jerusalem, Israel; 5EVERSANA, Burlington, ON, Canada; 6Vance Thompson Vision, Sioux Falls, SD, USA; 7IFocus Øyeklinikk AS, Haugesund, Norway; 8Herbert Wertheim School Optometry and Vision Science, University of California, Berkeley, CA, USA; 9Department of Ophthalmology, National Hospital Organization, Tokyo Medical Center, Meguro-ku, Tokyo, Japan; 10Triangle Eye Consultants, Raleigh, NC, USA; 11Department of Ophthalmology, Tulane University, New Orleans, LA, USA; 12Laser and Cataract Institute, Frankfort, IL, USA; 13Advocate South Suburban Hospital, Hazel Crest, IL, USA; 14Advocate Trinity Hospital, Chicago, IL, USA; 15NVISION Eye Center, Newport Beach, CA, USA; 16IRCCS - G.B. Bietti Foundation, Rome, Italy; 17Department of Ophthalmology, University of Southern California, Los Angeles, CA, USA; 18Cullen Eye Institute, Department of Ophthalmology, Baylor College of Medicine, Houston, TX, USA
Correspondence: Bonnie An Henderson, Tufts University School of Medicine, Boston, MA, USA, Tel +1 617 957 9279, Email [email protected]
Purpose: To obtain consensus on the key areas of burden associated with existing devices and to understand the requirements for a comprehensive next-generation diagnostic device to be able to solve current challenges and provide more accurate prediction of intraocular lens (IOL) power and presbyopia correction IOL success.
Patients and Methods: Thirteen expert refractive cataract surgeons including three steering committee (SC) members constituted the voting panel. Three rounds of voting included a Round 1 structured electronic questionnaire, Round 2 virtual face-to-face meeting, and Round 3 electronic questionnaire to obtain consensus on topics related to current limitations and future solutions for preoperative cataract-refractive diagnostic devices.
Results: Forty statements reached consensus including current limitations (n = 17) and potential solutions (n = 23) associated with preoperative diagnostic devices. Consistent with existing evidence, the panel reported unmet needs in measurement accuracy and validation, IOL power prediction, workflow, training, and surgical planning. A device that facilitates more accurate corneal measurement, effective IOL power prediction formulas for atypical eyes, simplified staff training, and improved decision-making process for surgeons regarding IOL selection is expected to help alleviate current burdens.
Conclusion: Using a modified Delphi process, consensus was achieved on key unmet needs of existing preoperative diagnostic devices and requirements for a comprehensive next-generation device to provide better objective and subjective outcomes for surgeons, technicians, and patients.
Keywords: next-generation diagnostic device, measurement accuracy and validation, IOL power prediction, surgical planning, cataract surgery
Introduction
A preoperative evaluation for refractive cataract surgery includes collection of eye measurements, identification of underlying eye conditions, calculation of intraocular lens (IOL) power, and selection of the IOL intended to correct aphakia and pre-existing refractive errors such as presbyopia or astigmatism. Despite recent innovations, refractive cataract surgeons still encounter limitations of existing preoperative evaluation diagnostic devices that may lead to challenges in measurement accuracy and validation,1–3 IOL power prediction,3–5 surgeon confidence in IOL selection,6–9 and achieving target refractive outcomes for patients.2,3 Current literature suggests that on average, surgeons achieve within ±0.5 Diopters (D) of target 76% of the time, with a range from 70% to 90%.5,10–12 In addition, there is a clear unmet need to improve and standardize the preoperative diagnostic process to increase the predictability of refractive outcomes for eyes with atypical measurements.5,10,11,13 Multiple devices are typically needed to complete a preoperative evaluation for refractive cataract surgery, which can negatively impact workflow efficiency, technician training requirements, and increase costs associated with equipment maintenance.6,14–18
Existing burden of preoperative refractive cataract evaluations has not been holistically reviewed in the literature. This study used a modified Delphi process to obtain consensus on the key burden associated with existing preoperative diagnostic devices and to understand what the requirements may be for a comprehensive next-generation diagnostic device to solve current challenges, generate new parameters for more accurate IOL power predictions, prediction of patient reported outcomes, and provide benefits for surgeons, technicians, and patients. Due to variation in practice across regions, reaching consensus on these topics is important to help optimize future decision-making and solutions.
Materials and Methods
Modified Delphi Method
The Delphi method uses an iterative approach for the purpose of attaining consensus of opinions from a panel of experts in the subject area under consideration.19,20 In medicine, the Delphi method can be used to forecast trends, develop clinical guidelines, inform policy, and aid in decision-making.21 The method consists of consecutive rounds of consensus building combined with controlled feedback of information to panelists.19 For each round, responses are collected through anonymous polling, the results are qualitatively and/or quantitatively summarized, and panelists are provided an opportunity to revise earlier answers after a review of other panelist responses.20 A descriptive statistical summary of the quantitative results (ie, measures of central tendency and level of dispersion) allows for an objective analysis.20
This study was conducted from September 2021 to December 2021 and used a modified Delphi method with 3 rounds of voting, including a Round 1 structured electronic questionnaire, Round 2 virtual Delphi panel meeting, and Round 3 electronic questionnaire (Figure 1). Traditionally, the first round of a Delphi study begins with an open-ended questionnaire to solicit specific information about the content area from the Delphi subjects.22 This approach was modified in the current study to use a structured questionnaire based on literature review and input from the steering committee (SC) members to initiate consensus building in Round 1. This modification is common when basic information is available for the subject matter of the study.22 The subsequent rounds of a traditional Delphi use structured questionnaires and provide controlled feedback to panelists from previous rounds for response modification. In this study, a virtual “face-to-face” meeting was used in place of a structured questionnaire to facilitate interactive discussions in real time to modify, eliminate, prioritize, or develop new messages. This approach helped to generate discussion between panelists and provide efficiency in the consensus-building process while maintaining anonymous voting.
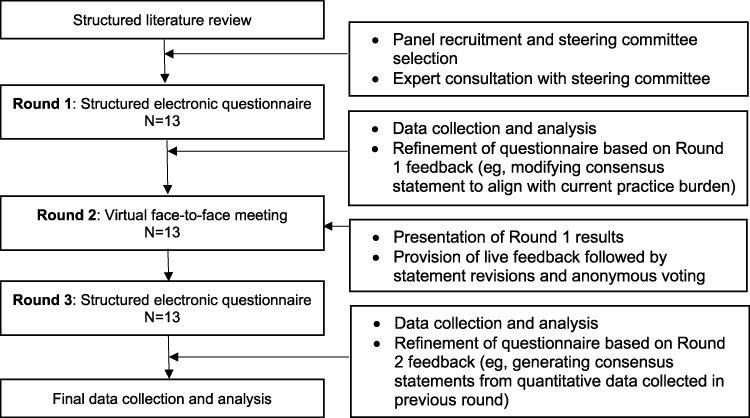 |
Figure 1 Schematic of the modified Delphi method utilized in the study. |
For this study, a next-generation device was defined as a comprehensive, whole eye analyzer that captures all the data required to complete a preoperative evaluation for refractive cataract surgery. Data required for a complete preoperative evaluation included biometry, refraction, two methods of measuring the corneal curvature, measurement of eye optical quality, tear film assessment, and high-resolution macula imaging.
Participant Selection and Recruitment
Criteria for participant selection included locally or internationally recognized expertise, a minimum of 5 years of experience and at least 1 peer reviewed publication or congress educational presentation on cataract refractive surgery, diagnostics, IOL power calculations, and premium IOLs. Thirteen refractive cataract surgeons were recruited including three SC members (Bonnie An Henderson, Jaime Aramberri, and Robin Vann) and ten panel members. The number of participants was chosen based on ranges suggested by literature20,23 and by the feasibility of having all participants attend the Round 2 virtual Delphi panel meeting. All SC members and panelists participated in voting during each round. This research was exempt from review and approval by an institutional review board or ethics committee, as it did not involve patients/people, medical records, or human samples.
Steering Committee and Round 1 Structured Electronic Questionnaire
Virtual meetings were conducted by the SC to discuss the findings of a structured literature review of limitations of diagnostic devices used in preoperative cataract-refractive evaluation and identify key burden and solution topics to inform the Round 1 structured electronic questionnaire. The questionnaire included three question types: qualitative, quantitative, and information-gathering. Panelists responded to qualitative questions with a level of agreement using a 5-point Likert scale ranging from 1 (strongly disagree) to 5 (strongly agree), and the percentage of scores, mean, median, mode, standard deviation, and range were calculated for each statement in each voting round. Additionally, other qualitative questions used a multi-point Likert scale to assess the level of improvement, level of importance, or level of need (Figure 2). Quantitative questions requested an estimate of burden or value, and information-gathering questions were open-ended and related to panelist experience in areas that were under-represented in the literature.
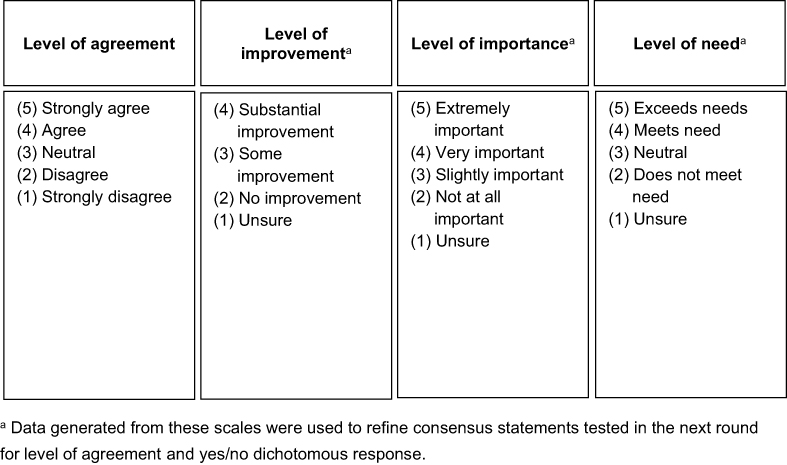 |
Figure 2 Illustration of the multi-point Likert scales utilized to assess consensus. |
Round 2 Virtual Meeting
Aggregated results from the Round 1 questionnaire were presented to the panel at a video conference for review and discussion. When consensus was not achieved in Round 1, clinical discussions were facilitated by the SC to revise statements in real time, followed by a second voting round. Quantitative estimate queries were refined or clarified to help with precision of panelist responses.
Round 3 Structured Electronic Questionnaire
A third voting round included an electronic questionnaire based on results from Round 2. Panelists were presented with qualitative and quantitative data from previous rounds of the study and rated their level of agreement on a newly developed statement.
Consensus
A pre-specified threshold of ≥70% agreement was required for consensus on a multi-point Likert scale or a yes/no dichotomous response.24,25 The decision to stop the Delphi process for a given topic was based on reaching the consensus threshold and/or completion of 3 rounds. For quantitative estimates, at least one opportunity was provided for panelists to revise a previous estimate based on review of an aggregate panel result.
Results
Thirteen surgeon panelists participated in the study. Participating regions included USA (n = 8 surgeons), Israel, Italy, Japan, Norway, and Spain (n = 1 surgeon each). A total of 40 consensus statements collected from Round 1 to 3 of the study were included and discussed. Seventeen consensus statements were related to current limitations associated with existing preoperative cataract diagnostic devices (Table 1, Statements 1 to 17), and 23 consensus statements were related to future solutions (Table 2, Statements A to W).
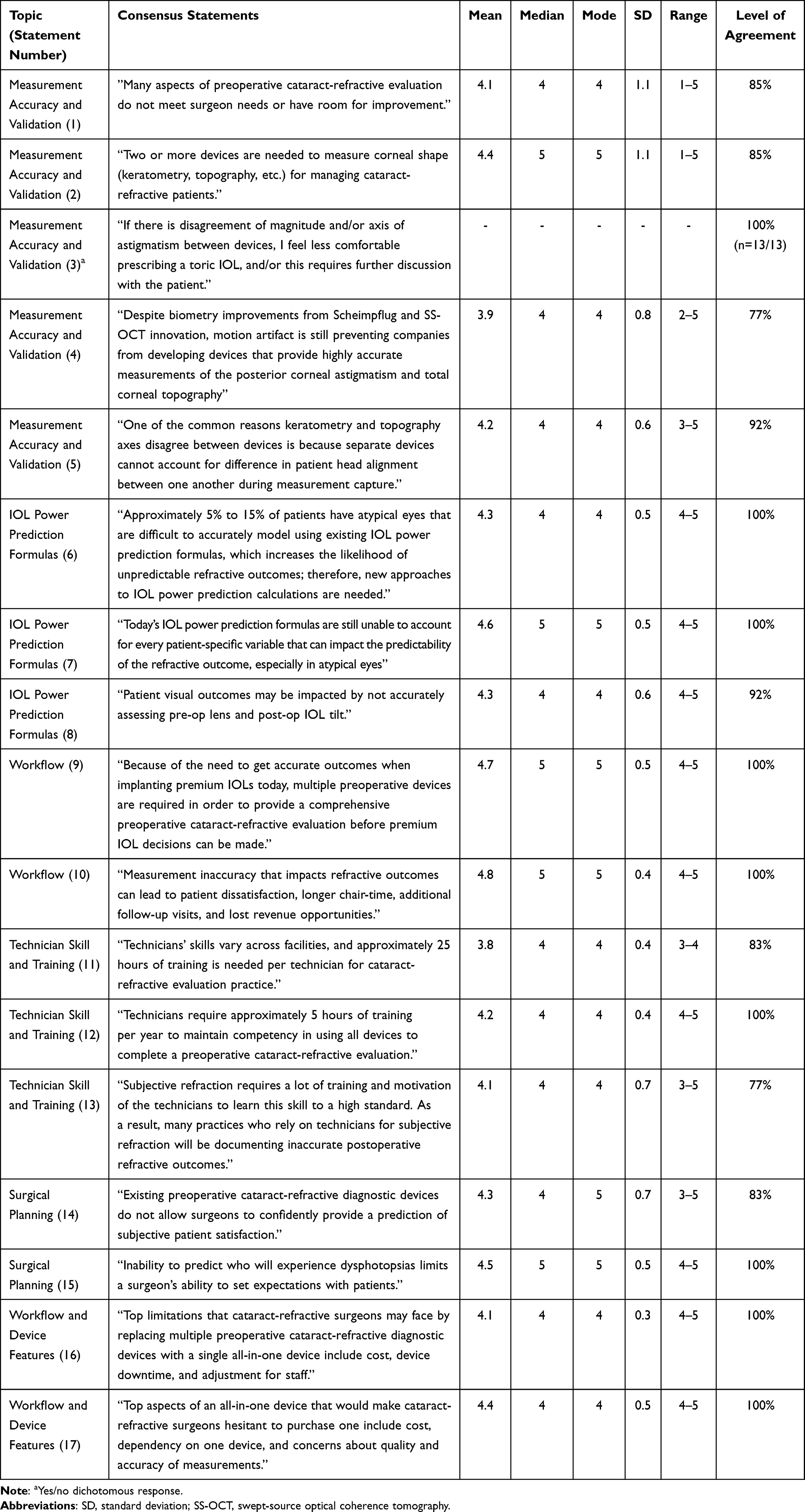 |
Table 1 Consensus Statements Related to Current Limitations Associated with Existing Preoperative Cataract-Refractive Diagnostic Devices |
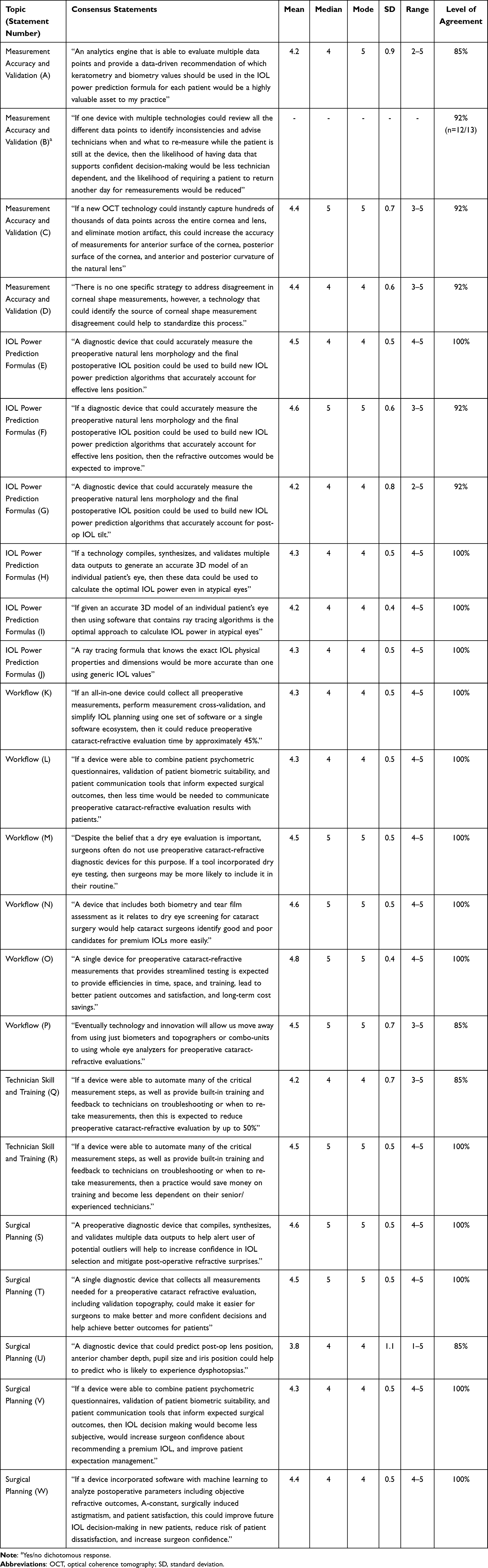 |
Table 2 Consensus Statements Related to Future Solutions Provided by an All-in-One Preoperative Cataract-Refractive Diagnostic Device |
Measurement Accuracy and Validation
Current Limitations: Statements 1 to 5
Many aspects of existing technologies for preoperative refractive cataract evaluation do not meet surgeon needs or have room for improvement (statement 1; median: 4; range: 1–5) (Table 1). Limitations of existing technologies included an inability of optical biometers and anterior eye analyzers to produce accurate measurements of posterior corneal astigmatism and total corneal topography (statement 4; median: 4; range: 2–5), inability of devices to account for patient factors such as head alignment variation between measurements (statement 5; median: 4; range: 3–5), and inability to achieve inter-device agreement which impacts confidence in IOL selection (statement 3; 100% agreement).
Panelists estimated ≥2 devices per practice are used to collect corneal measurements (statement 2; median: 5; range: 1–5). Eighty-five percent (n=11/13) of panelists were unsatisfied with the consistency of axis of corneal astigmatism between devices. When measurements between devices result in disagreement, strategies to address the problem included treating a related underlying pathology and remeasuring another day or using the average measurement sourced from multiple devices. Thirty-eight percent (n=5/13) of panelists reported no gold standard approach to address measurement disagreement. An average of 39 additional minutes (median: 30 minutes; range: 10–120 minutes) and an average of 11 additional minutes (median: 10 minutes; range: 5–20 minutes) were required to collect remeasurements on a separate day (including patient check-in, measurement collection by technician) and complete a second review of the measurement data, respectively. On average, 13% (median: 5%, range: 0–90%) of patients with astigmatism receive a non-toric IOL due to disagreement of astigmatism magnitude and axis between devices.
Potential Solutions: Statements A to D
Panelists agreed an ideal device would have several innovative features. This includes the ability to evaluate different data points collected by multiple technologies to inform accurate IOL power calculation (statement A; median: 4; range: 2–5). It should incorporate a technology for primary corneal measurement and a technology for corneal measurement validation. By identifying the source of measurement disagreements and providing guidance on when to remeasure, the device would become less technician dependent and minimize the need for patients to return for remeasurements (statement B; 92% agreement). Furthermore, the device should be able to remove motion artifact to improve anterior and posterior corneal measurement accuracy, and provide a recommendation on which keratometry and biometric values from the different technologies to utilize for the IOL calculation (statement C; median: 5; range: 3–5). Such a device could standardize assessment and decision-making in the preoperative refractive cataract evaluation (statement D; median: 4; range: 3–5). The panel proposed 9 future innovation needs associated with a cataract diagnostic technology (Figure 3), including a technology that could instantly capture a snapshot of hundreds of thousands of data points across the entire cornea and an emphasis on the ability to determine the root cause(s) of prediction error and prediction of postoperative IOL tilt and effective lens position.
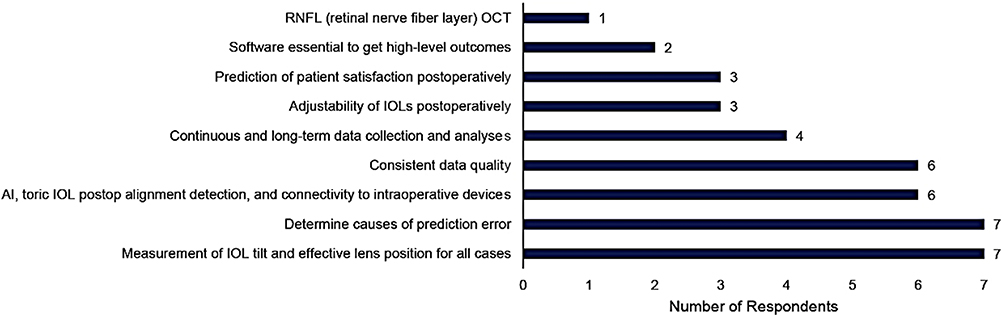 |
Figure 3 Future innovation needs related to preoperative cataract-refractive diagnostic technologies and IOL calculation methods. |
IOL Power Prediction Formulas
Current Limitations: Statements 6 to 8
Panelists estimated 5% to 15% of patients possess some type of atypical eye which may be difficult to model (statement 6; median: 4; range: 4–5) (Table 3). Existing IOL power prediction is unable to account for every patient-specific variable, especially for atypical eyes (statement 7; median: 5; range: 4–5). Limitations remain in the ability of preoperative diagnostic device and associated IOL formula to predict the final position of the IOL (statement 8; median: 4; range: 4–5).
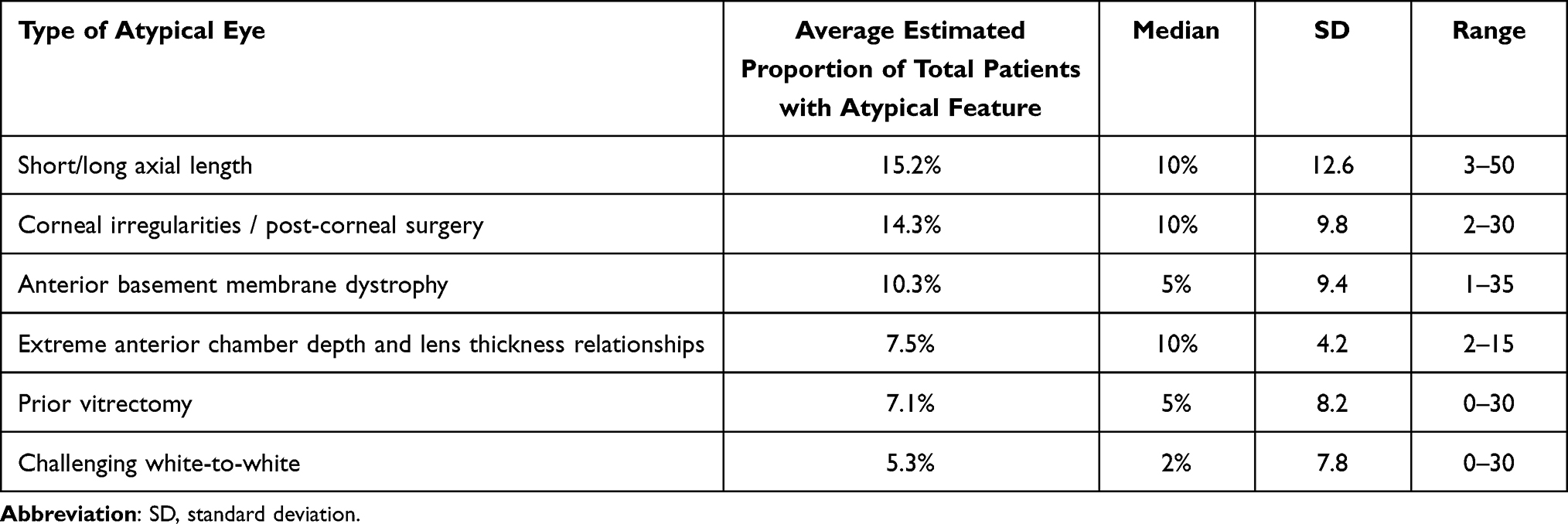 |
Table 3 Proportion of Patients Reported by Panel with Each Type of Atypical Eye That are Difficult to Accurately Model Using Existing IOL Power Prediction Formulas and Therefore More Likely to Lead to Unpredictable Refractive Outcomes |
Potential Solutions: Statements E to J
Improving the accuracy of preoperative measurement of crystalline lens morphology and final postoperative IOL position will help optimize effective lens position (statement E; mean: 4; range: 4–5) and IOL tilt (statement G; mean: 4; range: 2–5), which would subsequently improve refractive outcomes (statement F; median: 5; range: 3–5). Panelists estimated an average of 20% (median: 20%; range: 5%–60%) and 11% (median: 10%; range: 2%–35%) increase in patients achieving target refraction would be expected if a diagnostic device could account for effective lens position and postoperative lens tilt, respectively. If technology could compile, synthesize, and validate multiple data outputs to generate an accurate 3D model of the eye (statement H; mean: 4; range: 4–5), then utilizing software with ray tracing algorithms would be an ideal approach for IOL power calculations, particularly in atypical eyes (statement I; median: 4; range: 4–5). Inclusion of exact IOL physical properties such as lens type and power into the ray tracing formula may provide improvement in prediction compared with generic IOL values (statement J; median: 4; range: 4–5).
Clinic Workflow and Efficiency
Current Limitations: Statements 9 to 10
Current need for multiple diagnostic devices to support decision-making for premium IOL selection may further contribute to workflow inefficiency (statement 9; median: 5; range: 4–5). Panelists identified addressing patient’s expectations, suboptimal eye measurements, premium IOL recipients, and ocular surface disease as factors that may lengthen discussion time with patients. The average time to complete the diagnostic component of a preoperative evaluation (excluding patient exam and discussion of results) was an estimated 58 minutes (median: 60 minutes; range: 30–90 minutes), and average time allocated for discussion of evaluation results was estimated at 19 minutes (median: 10 minutes; range: 3–60 minutes). Additional resource use may be associated with patients with unexpected refractive or visual outcomes including longer chair-time and more follow-up visits (statement 10; median: 5; range: 4–5).
Potential Solutions: Statements K to P
To enhance workflow efficiency, the panel reached consensus that an ideal device would collect all preoperative measurements, perform cross-validation, simplify IOL planning using one set of software, and provide patient-centric features to enhance patient-surgeon communication. These features would help reduce preoperative evaluation time by approximately 45% (statement K; median: 4; range: 4–5) and reduce time allocated to discussing results with patients by an average of 34% (median: 30%; range: 20%–75%). The panel highlighted the need for an integrated device that combines patient psychometric questionnaires, patient biometric validation, and patient communication tools as this would significantly reduce the time required to communicate evaluation results with patients (statement L median: 4; range: 4–5). As well, incorporation of a dry eye testing tool in a future diagnostic device would help standardize the preoperative process (statement M; median: 5; range: 4–5) as it relates to identifying candidates for premium IOLs (statement N; median: 5; range: 4–5). From a practice efficiency perspective, a comprehensive, whole eye diagnostic device may substantially reduce operational costs and administrative burdens such as maintenance and contract management, respectively (statement O; median: 5; range: 4–5). Innovation should allow a shift from using multiple biometers, topographers, and other supplementary technologies for premium IOL implantation to a single whole eye analyzer in the future (statement P; median: 5; range: 3–5).
Technician Skill and Training
Current Limitations: Statements 11 to 13
On average, panelists estimated a ratio of 3.8 technicians: 1 surgeon per practice (median: 4, range: 1–6). Approximately 25 hours of initial training (statement 11; median: 4; range: 3–4) and 5 hours of ongoing training (statement 12; median: 4; range: 4–5) per year are required for technicians to achieve proficiency in using devices to perform a preoperative evaluation and to maintain competency, respectively. On average, 48% (median: 40%; range: 0–100%) of technicians can effectively identify measurement inconsistencies between devices. Competency in subjective refraction may be difficult to achieve for all technicians given the quantity of training and motivation needed. As a result, practices that rely on technicians to measure subjective refraction may be collecting inaccurate postoperative refraction outcomes and associated outcomes reporting (statement 13; median: 4; range: 3–5).
Potential Solutions: Statements Q to R
Panelists agreed that a diagnostic device with built-in training features available and the ability to provide specific, real-time feedback (eg, the need for troubleshooting or re-measurement) is expected to reduce training time up to 50% (statement Q; median: 4; range: 3–5) and reduce associated training costs. A device that automates critical steps in the measurement collection and validation process may reduce training needs and dependence on technician skill (statement R; median: 5; range: 4–5).
Surgical Planning
Current Limitations: Statements 14 to 15
For a toric or presbyopia-correcting IOL preoperative evaluation, the panel reported importance of including biometry, tomography, high resolution macular imaging, posterior corneal astigmatism, tear film assessment, and refraction. However, existing devices are unable to accurately predict surgical outcomes through the integration of both objective and subjective measurements, which hinders surgeons’ ability to set expectations with patients and decide if premium IOLs should be implanted (statement 14; median: 4; range: 3–5). Furthermore, accurately predicting the likelihood of dysphotopsia remains an ongoing challenge (statement 15; median: 5; range: 4–5).
Potential Solutions: Statements S to W
Multiple strategies were identified to help improve the surgical planning process and surgeon confidence in IOL selection. A device or supporting software that compiles, synthesizes, and validates multiple data outputs to alert user of potential outliers would improve surgeon confidence in IOL selection and reduce refractive surprises (statement S; median: 5; range: 4–5). By collecting all necessary measurements in a single device, including validation topography, surgeons could make informed decisions and achieve optimal outcomes for patients (statement T; median: 5; range: 4–5). Device capability to predict postoperative lens position, anterior chamber depth, pupil size, angle kappa, and iris position may help identify the likelihood of dysphotopsias (statement U; median: 4; range: 1–5). Tools to assess suitability of IOL choice and facilitate communication of expected surgical outcomes with patients, such as patient and IOL specific retinal point spread functions, would support recommendations for premium IOLs and help manage patient expectations (statement V; median: 4; range: 4–5). Future IOL decision-making could be improved by incorporating machine learning to analyze postoperative parameters including objective refraction, A-constant, surgically induced astigmatism, and patient satisfaction to generate new algorithms for objective predictions of patient-reported outcomes (statement W; median: 4; range: 4–5).
Potential Challenges to Consider with an All-in-One Device
Statements 16 to 17
While an all-in-one device may bring efficiencies and improve patient outcomes, panelists identified potential limitations including device downtime, cost, and adjustment for staff (statement 16; median: 4; range: 4–5). Other considerations included dependency on a single device and measurement quality and accuracy (statement 17; median: 4; range: 4–5). Device downtime as a result of service or maintenance without backup units readily available at the site may delay diagnostic procedures and downstream workflow. As such, a comprehensive next-generation device should include the ability to perform real-time machine health analysis to predict and prevent device failure. Staff and surgeons may also be accustomed to using multiple diagnostic devices; therefore, it may require adjustment to feel confident working with one device. When evaluating a new diagnostic technology for purchase, it is important to weigh its upfront cost and potential long-term cost savings. Additionally, a transition period with multiple devices is a common approach to satisfy concerns about quality and accuracy of measurements.
Discussion
This is the first study to utilize a modified Delphi method to achieve expert consensus on the burden associated with current diagnostic devices and the potential solutions to these burdens. The utilization of the Delphi method was necessary to understand the limitations of the current devices in order to create the next generation of devices to address those deficits. The panelists agreed that there is room to improve the accuracy and validation of preoperative measurements used in IOL power prediction calculations. Disagreement between devices in magnitude or axis of astigmatism can reduce surgeon confidence in recommending toric IOLs. This aligns with literature suggesting current swept-source optical coherence tomography (OCT) and Scheimpflug technologies may face challenges in defining the posterior corneal surface,26,27 and predicting refractive outcomes with accuracy and reproducibility.2,3 Measurement inaccuracy and validation challenges associated with existing diagnostic devices can impact downstream workflow efficiency, which may lead to patient dissatisfaction, and impact future patient interactions with the clinic.28 The risk of measurement failure may be increased in atypical eyes such as those with abnormal anterior to posterior corneal ratio, short or long eyes, and dense cataract.2,29–32 The experts agreed specific technological innovations could help to improve accuracy and confidence of measurements, including instantaneous collection of data points across the entire cornea and natural lens, eliminating motion artifact, and having one device use multiple technologies to collect and review measurements to help standardize the process and identify inconsistencies between measurement relationships. Although these advancements have yet to be tested in a clinical study, there is potential to transform IOL power prediction.
The panel identified factors that may contribute to suboptimal refractive outcomes, particularly in patients with atypical eyes (eg, long or short axial length, post-refractive surgery eyes). These findings helped identify the key challenges faced in achieving target refraction for atypical eyes with existing IOL prediction formulas, providing clarity on the subject matter.5,10,11,13,33 On average, literature reports that surgeons achieve within ±0.5D of target 76% of the time, with a range from 70% to 90%, and reduced prediction accuracy for atypical eyes.5,10–12,34 IOL formulas utilizing the theoretical derivation method still have room for improvement as they provide a simplified eye model that does not account for abnormal relationships between parameters in atypical eyes.5,10,11 The panel estimated between 5% and 15% of their patients are difficult to model with existing formulas, which highlights the need for devices and IOL power formulas to account for additional ocular characteristics such as preoperative natural lens tilt and postoperative IOL tilt. The panel agreed that innovative technology that can generate an accurate 3D eye model will help to calculate optimal IOL power, even for atypical eyes. Additionally, the panel reached consensus that ray tracing incorporating specific lens and IOL morphology data may help to overcome the limitations of existing formulas in accounting for outliers. Although their utility and effectiveness for atypical eyes require further exploration, ray tracing IOL formulas have demonstrated suitability for corneal irregularities and post-refractive eyes.13 By avoiding errors associated with standard formulas due to dependencies on assumptions such as keratometric index, anterior to posterior corneal curvature ratio, and effective lens position, ray tracing methods may offer a promising opportunity to enhance IOL power calculation accuracy and predictability.35,36
Patients receiving premium IOLs (eg, toric IOL, presbyopia-correcting IOL) often pay out of pocket and may therefore have high expectations of their postoperative vision.37 Greater than 90% patient satisfaction can be achieved with premium IOLs;38 however, these IOLs are sensitive to misalignment and incorrect power calculations, which can make it challenging to achieve target refraction.39 Consequently, physician confidence in their ability to achieve target outcomes and meet expectations can impact toric and presbyopia-correcting IOL adoption.40 The panel agreed that there is a need for a next-generation, whole eye analyzer to enable comprehensive screening, help surgeons to communicate expectations with patients, and enhance physician confidence in achieving target outcomes. In this study, surgeons identified multiple features a next-generation, whole eye analyzer would need to facilitate comprehensive screening for premium IOL suitability. Importantly, helping patients to achieve their vision goals with premium IOLs may also help to support practice reputation, performance, and growth.28,37,41 Empirical research examining the impact of a whole eye analyzer on premium IOL adoption may provide further validation of these Delphi study findings.
With an aging population, increasing patient expectations, and the demand for preventative eye care, there is a need for skilled technicians.17,18 Technician expertise can impact quality measures such as biometry, image acquisition, and procedural efficiency.42–44 In this study, panelists estimated that approximately half of technicians can competently identify inconsistencies in inter-device measurements and perform remeasurement. This aligns with existing literature that there is room for improvement in ophthalmic technicians’ competency in identifying outliers.45 In general, the learning curve for ophthalmic technicians varies, but may be considerable for some6,14,18 and 6 to 12 months may be needed to achieve competency.17 Panelists agreed that in-built training and automation of critical measurement steps will help to reduce training burden, dependency on technician expertise, and preoperative evaluation time. Additionally, standardizing staff training may help to improve clinic workflow and increase efficiency.16 Future research may prioritize evaluating the effectiveness of in-built training modules and automated measurement steps in diagnostic devices to improve measurement accuracy and patient outcomes.
The potential benefits of a whole eye analyzer for a preoperative refractive cataract evaluation for improving patient outcomes and providing efficiency in time, space and technician training were rated highly by the panel. Interventions to reduce time between measurements and optimize technician training have helped to improve efficiency and patient throughput in a retina practice setting.46 While cost, reliance on a single device, and adapting to a new workflow may be of concern to some practices, the value of improving patient outcomes and increasing efficiency may offset hesitations regarding conversion to a comprehensive whole eye analyzer for a preoperative refractive cataract evaluation. Innovations in surgical planning software that integrate postoperative data and synthesize preoperative measurements from multiple devices may also be a solution for surgeons hesitant to transition to a whole eye analyzer;47 however, combining planning software with a whole eye analyzer may be the best solution to address inter-device measurement issues highlighted by the panel in this study.
Perspectives of surgeons from multiple regions were captured by the study. Using the input of the expert panelists, statements were formulated and/or reformulated to accurately reflect the unmet needs and potential solutions in the refractive cataract surgery space. Although consensus was specified a priori as ≥70%, the consensus among the study participants was much closer (average 94%) for all the questions and statements. Of note, 6 of the 40 statements were revised according to the suggestions provided by the SC and panel experts during the virtual meeting to achieve consensus, which contributed to the 94% average. Quantitative estimates of burden and proposed solutions were reviewed and refined if deemed necessary during Round 2, and a range of results were reported for transparency of the breadth of panelist responses. After refinement of quantitative queries, the remaining variation reflected in the range of results may reflect different practice patterns, expectations from surgeons, and experience levels of clinic staff or technicians. A future prospective study should assess measurement accuracy and validation, IOL power prediction accuracy, workflow, surgical planning, and training associated with a whole eye analyzer for preoperative cataract-refractive evaluation to help understand its benefits for surgeons, technicians, and patients.
Conclusion
In conclusion, this modified Delphi study achieved consensus for current burden and future solutions for preoperative refractive cataract evaluation diagnostic devices. Innovation in preoperative diagnostic devices and their associated analytics software is highly anticipated to improve patient outcomes, surgeon confidence, and provide long-term efficiencies.
Disclosure
BH, JA, RV, AA, JB, KGG, SG, PG, SM, DR, GS, HJS, and LW are consultants for Alcon Laboratories, Inc. JA reports personal fees from Johnson and Johnson and Staar Surgical, outside the submitted work. AA reports use of equipment by his department from Haag Streit, Oculus, and Zeiss, outside the submitted work. JB reports consultant and/or lecture fees from AbbVie, Aerpio, Alcon, Aldeyra, Aurea Medical, Aurion Biotech/CorneaGen (with ownership), Bausch and Lomb, Dakota Lions Eye Bank, Elios Vision INC, Equinox (with ownership and patents), Expert Opinion (with ownership), Glaukos, Gore, Imprimis (with patents/royalty), Interfeen (with ownership), iRenix, Iacta Pharmaceuticals, JNJ, Kala, Kedalion, MELT Pharmaceuticals, MicroOptx, New World Medical, Ocular Surgical Data (with ownership), Ocular Therapeutix, Omega Ophthalmic (with ownership), Orasis, Oyster Point, RxSight, Santen, Sight Sciences, Surface Inc, Tarsus, Tear Clear, Vertex Ventures, ViaLase, Vittamed, Vance Thompson Vision (with ownership), Verana Health, Versea Biologics, Visionary Ventures, Visus, and Zeiss (with ownership), outside the submitted work. PG reports personal fees from Bausch + Lomb, Carl Zeiss, and Novartis. SM reports personal fees from EyeDx. GS reports grants from Fondazione Roma, Italian Ministry of Health, during the conduct of the study; personal fees from Alcon, Staar, Zeiss, and Johnson & Johnson, outside the submitted work. LW reports personal fees from AcuFocus, Carl Zeiss Meditec, and Cassini Technologies, outside the submitted work. MAG, NF, EP, and WZW are employees of EVERSANA Life Science Services and consult for Alcon Laboratories, Inc. The authors report no other conflicts of interest in this work.
References
1. Schiano-Lomoriello D, Hoffer KJ, Abicca I, Savini G. Repeatability of automated measurements by a new anterior segment optical coherence tomographer and biometer and agreement with standard devices. Sci Rep. 2021;11(1):983. doi:10.1038/s41598-020-79674-4
2. Cummings AB, Naughton S, Coen AM, Brennan E, Kelly GE. Comparative Analysis of Swept-Source Optical Coherence Tomography and Partial Coherence Interferometry Biometers in the Prediction of Cataract Surgery Refractive Outcomes. Clin Ophthalmol. 2020;14:4209–4220. doi:10.2147/opth.S278589
3. Abulafia A, Barrett GD, Kleinmann G, et al. Prediction of refractive outcomes with toric intraocular lens implantation. J Cataract Refract Surg. 2015;41(5):936–944. doi:10.1016/j.jcrs.2014.08.036
4. Siddiqui AA, Devgan U. Intraocular lens calculations in atypical eyes. Indian J Ophthalmol. 2017;65(12):1289–1293. doi:10.4103/ijo.IJO_834_17
5. Aristodemou P, Knox Cartwright NE, Sparrow JM, Johnston RL. Formula choice: Hoffer Q, Holladay 1, or SRK/T and refractive outcomes in 8108 eyes after cataract surgery with biometry by partial coherence interferometry. J Cataract Refract Surg. 2011;37(1):63–71. doi:10.1016/j.jcrs.2010.07.032
6. Jackson MA. The learning curve: is it really worth it? Healio News. Available from: https://www.healio.com/news/ophthalmology/20150313/j241_3305_23_news_print_3.
7. Chang DF. Adjustable IOLs—Disrupting the Refractive IOL Industry. US Ophthalmic Rev. 2017;10(2):95–98.
8. Thompson V. The future of the premium IOL; 2018:52–54. Available from: https://crstoday.com/articles/2018-may/the-premium-iol-channel-pitfalls-prospects.
9. Carones F. Reviewing key presbyopia-correcting IOL trends from the ESCRS clinical survey. Eurotimes. Available from: https://www.eurotimes.org/reviewing-key-presbyopia-correcting-iol-trends-from-The-escrs-clinical-survey/.
10. Melles RB, Holladay JT, Chang WJ. Accuracy of Intraocular Lens Calculation Formulas. Ophthalmology. 2018;125(2):169–178. doi:10.1016/j.ophtha.2017.08.027
11. Hipólito-Fernandes D, Elisa Luís M, Gil P, et al. VRF-G, a New Intraocular Lens Power Calculation Formula: a 13-Formulas Comparison Study. Clin Ophthalmol. 2020;14:4395–4402. doi:10.2147/opth.S290125
12. Savini G, Hoffer KJ, Balducci N, Barboni P, Schiano-Lomoriello D. Comparison of formula accuracy for intraocular lens power calculation based on measurements by a swept-source optical coherence tomography optical biometer. J Cataract Refract Surg. 2020;46(1):27–33. doi:10.1016/j.jcrs.2019.08.044
13. Martinez-Enriquez E, Pérez-Merino P, Durán-Poveda S, Jiménez-Alfaro I, Marcos S. Estimation of intraocular lens position from full crystalline lens geometry: towards a new generation of intraocular lens power calculation formulas. Sci Rep. 2018;8(1):9829. doi:10.1038/s41598-018-28272-6
14. Dubey S, Jain K, Fredrick TN. Quality assurance in ophthalmic imaging. Indian J Ophthalmol. 2019;67(8):1279–1287. doi:10.4103/ijo.IJO_1959_18
15. Juhas C. 15 tips to optimize capital equipment purchasing. Healthcare Purchasing News. Available from: https://www.hpnonline.com/sourcing-logistics/article/13000918/15-tips-to-optimize-capital-equipment-purchasing.
16. Hansen MS, Hardten DR. Financially efficient cataract surgery in today’s healthcare environment. Curr Opin Ophthalmol. 2015;26(1):61–65. doi:10.1097/icu.0000000000000120
17. Leonard C. The Ophthalmic Staffing Shortage. Available from: https://www.reviewofophthalmology.com/article/the-ophthalmic-staffing-shortage.
18. Tello MC. The onboard formula for new techs. 2020:10–15. Available from: https://www.ophthalmicprofessional.com/issues/2020/january-2020/the-onboard-formula-for-new-techs.
19. Dalkey NC. The Delphi Method: an Experimental Study of Group Opinion. Int J Med. 1969;87.
20. Hsu -C-C, Sandford BA. The Delphi Technique: making Sense of Consensus. Practical Assessment Res Evaluation. 2007;12(1):1–8.
21. Varndell W, Fry M, Lutze M, Elliott D. Use of the Delphi method to generate guidance in emergency nursing practice: a systematic review. Int Emerg Nurs. 2021;56:100867.
22. Hsu -C-C, Sandford BA. The Delphi technique: making sense of consensus. Practical Assessment Res Evaluation. 2007;12(1):10.
23. Belton I, MacDonald A, Wright G, Hamlin I. Improving the practical application of the Delphi method in group-based judgment: a six-step prescription for a well-founded and defensible process. Technol Forecast Soc Change. 2019;147:72–82. doi:10.1016/j.techfore.2019.07.002
24. Thomsen ASS, la Cour M, Paltved C, et al. Consensus on procedures to include in a simulation-based curriculum in ophthalmology: a national Delphi study. Acta Ophthalmol. 2018;96(5):519–527. doi:10.1111/aos.13700
25. Diamond IR, Grant RC, Feldman BM, et al. Defining consensus: a systematic review recommends methodologic criteria for reporting of Delphi studies. J Clin Epidemiol. 2014;67(4):401–409. doi:10.1016/j.jclinepi.2013.12.002
26. Sideroudi H, Labiris G, Giarmoulakis A, Bougatsou N, Mikropoulos D, Kozobolis V. Repeatability, reliability and reproducibility of posterior curvature and wavefront aberrations in keratoconic and cross-linked corneas. Clin Exp Optom. 2013;96(6):547–556. doi:10.1111/cxo.12044
27. Piñero DP, Alió JL, Alesón A, Escaf M, Miranda M. Pentacam posterior and anterior corneal aberrations in normal and keratoconic eyes. Clin Exp Optom. 2009;92(3):297–303. doi:10.1111/j.1444-0938.2009.00357.x
28. Hobbs L. Premium Practice Promotion. Available from: https://theophthalmologist.com/business-profession/premium-practice-promotion.
29. Oh R, Oh JY, Choi HJ, Kim MK, Yoon CH. Comparison of ocular biometric measurements in patients with cataract using three swept-source optical coherence tomography devices. BMC Ophthalmol. 2021;21(1):62. doi:10.1186/s12886-021-01826-5
30. Wang Z, Yang W, Li D, et al. Evaluation and comparison of a novel Scheimpflug-based optical biometer with standard partial coherence interferometry for biometry and intraocular lens power calculation. Exp Ther Med. 2021;21(4):326. doi:10.3892/etm.2021.9757
31. Fişuş AD, Hirnschall ND, Findl O. Comparison of 2 swept-source optical coherence tomography-based biometry devices. J Cataract Refract Surg. 2021;47(1):87–92. doi:10.1097/j.jcrs.0000000000000373
32. Yang CM, Lim DH, Kim HJ, Chung TY. Comparison of two swept-source optical coherence tomography biometers and a partial coherence interferometer. PLoS One. 2019;14(10):e0223114. doi:10.1371/journal.pone.0223114
33. Savini G, Hoffer KJ. Intraocular lens power calculation in eyes with previous corneal refractive surgery. Eye Vis. 2018;5:18. doi:10.1186/s40662-018-0110-5
34. Solomon R, Tamilarasi S, Sachdev G, Dandapani R. Accuracy of Barrett versus third-generation intraocular lens formula across all axial lengths. Oman J Ophthalmol. 2022;15(3):290–294. doi:10.4103/ojo.ojo_188_21
35. Savini G, Bedei A, Barboni P, Ducoli P, Hoffer KJ. Intraocular lens power calculation by ray-tracing after myopic excimer laser surgery. Am J Ophthalmol. 2014;157(1):150–153.e1. doi:10.1016/j.ajo.2013.08.006
36. Ghaffari R, Abdi P, Moghaddasi A, Heidarzadeh S, Ghahvhechian H, Kasiri M. Ray Tracing versus Thin-Lens Formulas for IOL Power Calculation Using Swept-Source Optical Coherence Tomography Biometry. J Ophthalmic Vis Res. 2022;17(2):176–185. doi:10.18502/jovr.v17i2.10788
37. Cionni RJ. Physician: refractive cataract surgery should have outcomes as accurate as LASIK. Available from: https://www.healio.com/news/ophthalmology/20140210/10_3928_1081_597x_20140101_02_1332062.
38. Modi S, Lehmann R, Maxwell A, et al. Visual and Patient-Reported Outcomes of a Diffractive Trifocal Intraocular Lens Compared with Those of a Monofocal Intraocular Lens. Ophthalmology. 2021;128(2):197–207. doi:10.1016/j.ophtha.2020.07.015
39. Núñez MX, Henriquez MA, Escaf LJ, et al. Consensus on the management of astigmatism in cataract surgery. Clin Ophthalmol. 2019;13:311–324. doi:10.2147/opth.S178277
40. Freeman W. 2021 IOL Market Report: Global Analysis for 2020 to 2026 . (Market Scope). 2021.
41. Woodward MA, Randleman JB, Stulting RD. Dissatisfaction after multifocal intraocular lens implantation. J Cataract Refract Surg. 2009;35(6):992–997. doi:10.1016/j.jcrs.2009.01.031
42. Martín-Serrano MJ, Roman-Ortiz C, Villa-Sáez ML, et al. Concordance and interchangeability of biometric measurements of ocular axial length in patients awaiting cataract surgery. Eur J Ophthalmol. 2014;24(1):29–34. doi:10.5301/ejo.5000318
43. de Araujo AL, Rados DRV, Szortyka AD, et al. Ophthalmic image acquired by ophthalmologists and by allied health personnel as part of a telemedicine strategy: a comparative study of image quality. Eye. 2021;35(5):1398–1404. doi:10.1038/s41433-020-1035-5
44. Poyales F, Poyales B, Medel D, López-Brea I, López-Artero E, Garzón N. The influence of surgeons and technicians on the learning curve of femtosecond-laser cataract surgery. J Optom. 2020;13(4):242–248. doi:10.1016/j.optom.2020.01.001
45. Laurent C, Bachir Y, Viana M, et al. Capacité discriminative de la normalité de l’examen ophtalmologique par les orthoptistes [Ability of ophthalmic technicians to identify a normal ophthalmological examination]. J Fr Ophtalmol. 2021;44(9):1381–1386. doi:10.1016/j.jfo.2021.03.006. French
46. Lin CC, Li AS, Ma H, et al. Successful interventions to improve efficiency and reduce patient visit duration in a retina practice. Retina. 2021;41(10):2157–2162. doi:10.1097/iae.0000000000003169
47. Wortz G. In Your Head: what’s New in Surgical Planning? Available from: https://millennialeye.com/articles/nov-dec-21/in-your-head-whats-new-in-surgical-planning/.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.