")
Back to Journals » Therapeutics and Clinical Risk Management » Volume 18
The Course and Anatomical Characteristics of Sciatic and Femoral Nerves in Unilateral Crowe Type-IV Hip Dysplasia
Authors Song P, Kong X, Yang M, Ma M , Chai W
Received 28 January 2022
Accepted for publication 14 April 2022
Published 26 April 2022 Volume 2022:18 Pages 491—497
DOI https://doi.org/10.2147/TCRM.S360087
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Deyun Wang
Ping Song,1– 3,* Xiangpeng Kong,2,3,* Minzhi Yang,2,3 Mingyang Ma,1– 3 Wei Chai2,3
1Graduate School, Chinese PLA Medical School, Beijing, People’s Republic of China; 2Senior Department of Orthopedics, the Fourth Medical Center of PLA General Hospital, Beijing, People’s Republic of China; 3National Clinical Research Center for Orthopedics, Sports Medical and Rehabilitation, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Wei Chai, Tel +8610-66938304, Email [email protected]
Background: This study aims to investigate the course and anatomical characteristics of sciatic and femoral nerves in unilateral Crowe type-IV developmental dysplasia of the hip (DDH) patients.
Methods: We conducted a retrospective own-control study of patients with unilateral Crowe type-IV DDH. Bilateral hip computed tomography (CT) of 21 female patients was reviewed in our institute from February 2018 to February 2020. The distances between nerves and bony landmarks were measured in different CT sections (anterior superior iliac spine, acetabular inner wall, teardrop, and ischial tuberosity) to analyze the anatomical position and course of sciatic and femoral nerves between bilateral hips.
Results: In the section of the acetabular inner wall, the distance between the femoral nerve and the acetabular anterior wall in affected hip (13.20 ± 3.59 mm) was significantly smaller than that in the healthy hip (16.58 ± 5.12mm) (p < 0.001). In other sections, the distances between nerves and bony landmarks in affected hips were significantly larger than or equal to those in the healthy hips.
Conclusion: In female patients with unilateral Crowe type-IV DDH, the femoral nerve in the affected hip runs closer to the anterior acetabular wall than that in the healthy hip.
Keywords: developmental dysplasia of the hip, total hip arthroplasty, nerve injury, nerve course, sciatic nerve, femoral nerve
Introduction
Total hip arthroplasty (THA) is an effective and mature treatment for patients with Crowe type-IV developmental dysplasia of the hip (DDH). But the incidence of postoperative nerve injury in Crowe type-IV patients, ranging from 7.35% to 10%, was significantly higher than that in other patients with an incidence of 0.08%-3.7%.1–3 Nerve injury following THA is a disastrous adverse complication which severely affects postoperative functional training, recovery, and quality of life.4 Limb Lengthening and poor soft-tissue compliance were considered as important risk factors of nerve injury in hip replacement for Crowe type-IV DDH patients.5–7 However, Eggli8 and other researchers9,10 have found that nerve injury was most caused by direct or indirect mechanical trauma, not by limb lengthening on its own.
THA in adult patients with Crowe type-IV DDH is a technically challenging procedure. Due to the femoral upward dislocation and abnormal pelvic architecture, the course of sciatic and femoral nerves may change accordingly. Thus, the difficult surgery is associated with a higher risk of direct or indirect mechanical nerve trauma. A better understanding of the course and anatomical characteristics of sciatic and femoral nerves in patients with Crowe type-IV DDH may help minimize the risk of mechanical injury after THA.11–14 However, the characteristics of the peripheral nerve course of dysplastic hip have not been well studied.15 This study aims to investigate the course and anatomical characteristics of sciatic and femoral nerves in unilateral Crowe type-IV DDH patients in computed tomography (CT).
Patients and Methods
Patients with unilateral Crowe type-IV DDH were retrospectively enrolled in our institute from February 2018 to February 2020. Inclusion criteria:1. One hip is Crowe type-IV DDH and the other hip is normally developed, ie the central-edge angle is greater than 25°,16 2. Female, 3. Age:18–50 years old, 4. Height: 150–170cm, 5. BMI: 20–30kg/m2. Exclusion criteria: 1. History of infection/surgery/trauma in either hip, 2. Lower limb peripheral nerve diseases, such as poliomyelitis sequelae, 3. The angle between femoral longitudinal axis and pelvic median axis is greater than 15° in CT localization image, 4. The angle between inter-teardrop line and horizontal line is greater than 10° in CT localization image. Our study protocol was approved by the Ethics Committee of Chinese PLA General Hospital and informed consent obtained from the study participants prior to study commencement.
CT Scan Protocols and Parameters
CT scan (Brilliance ICT, Philips Healthcare, Netherlands) was completed in the supine position, covering the entire pelvis and proximal femur. The scanning parameters were described as follows, layer thickness: 0.625mm, pitch: 5mm, kVp: 120kVp, mA: 200mA, field of view (FOV): 500mm, image resolution: 512×512 matrix.
Measurements
We selected reference transverse sections through several key points (Figure 1, A: anterior inferior iliac spine, B: most medial part of acetabular inner wall, C: inferior margin of the teardrop, D: ischial tuberosity) in CT soft tissue window of the hip using picture archiving and communication system (PACS, Knowlesys Software Technology Co., Ltd., China) in our institute, and identified sciatic nerve and femoral nerve locations according to anatomical adjacency relationship and nerve CT values (40–60) (Figure 2).
 |
Figure 1 Transverse sections through selected key points (A: anterior inferior iliac spine, B: acetabular inner wall, C: inferior margin of the teardrop, D: ischial tuberosity). |
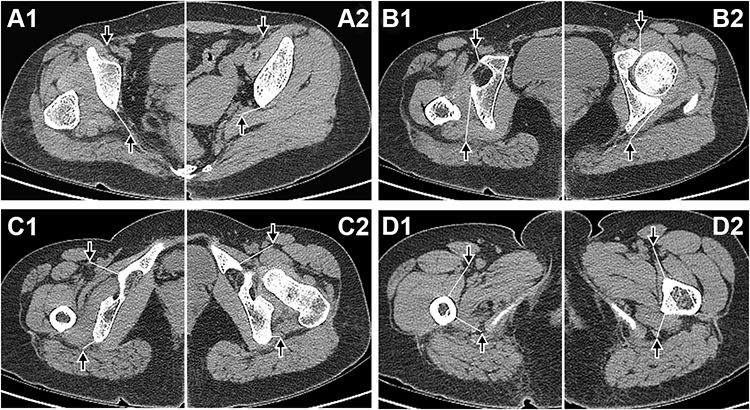 |
Figure 2 Axial CT scans demonstrating the sections used for evaluation of the femoral nerve (indicated by down arrow) and sciatic nerve (indicated by up arrow) in a cranio-caudal direction. A1, B1, C1, D1 were affected hip and A2, B2, C2, D2 were healthy hip. Linear distance (indicated by white line) between nerves and adjacent bony landmarks. (A): distance from sciatic nerve to posterior edge of iliac crest, section (B): distance from sciatic nerve to posterior acetabular wall and distance from femoral nerve to anterior acetabular wall, section (C): distance from sciatic nerve to ischium and distance from femoral nerve to pubis, section (D): distance from sciatic nerve and femoral nerve to femur. |
After confirming the nerves’ location, their linear distance to the adjacent pelvic or femoral bony landmarks were measured (Figure 2). All the measurements were carried out by two postgraduate students in orthopedics, then repeated two weeks later. Screenshots of CT images were saved at the time of measurement, and if the results differed significantly or nerve location was controversial, a senior orthopedic surgeon made the determination. The mean measurements were used for comparison.
Statistics
Statistical analysis was performed in SPSS22.0 (IBM Company, NY, USA) and power analysis was performed in PASS15.0 (NCSS, LLC. Kaysville, USA). All indices were subjected to normality test, and those conforming to normal distribution were expressed as mean ± standard deviation. All the distances in both sides were analyzed by paired-t test. Intra-class correlation coefficients (ICC) were adopted to assess consistency in measurements. ICC value ranged between 0 and 1, and consistency would be poor (κ=0-0.4), moderate (κ=0.4–0.6), substantial (κ=0.6–0.8) or almost perfect (κ=0.8–1) agreement. The criterion for a significant statistical difference was p<0.05.
Results
Bilateral hips’ CTs of 21 female patients with unilateral Crowe type-IV DDH were selected in our study (Figure 3). These patients’ basic information showed in Table 1. Consistency in the measurement results was almost perfect, with ICC>0.81. Although the power of comparison of distance from femoral nerve to pubis (0.58) and femur (0.74) was relatively low, the power of comparison of distance from femoral nerve to anterior acetabular wall (1.00) and distance from sciatic nerve to posterior acetabular wall (1.00) and femur (0.93) were convincing.
 |
Table 1 Demographic Data |
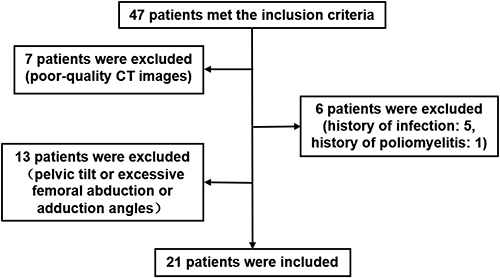 |
Figure 3 Patient flow diagram. |
In section A, the mean distance from sciatic nerve to posterior edge of iliac crest was 10.89±0.50mm in healthy hip and 11.03±0.65mm in affected hip, with no significant difference bilaterally (p=0.487). The femoral nerve was far from the operating area and no measurement was performed.
In section B, the distance from sciatic nerve to posterior acetabular wall in affected hip (30.70±6.68mm) was significantly larger (p<0.001) than that in healthy hip (20.07±2.08mm); the distance from femoral nerve to anterior acetabular wall in affected hip (13.20±3.59mm) was significantly smaller (p<0.001) than that in healthy hip (16.58±5.12mm).
In section C, the distance from sciatic nerve to ischium was 13.98±3.24mm in healthy hip and 13.30±2.90mm in affected hip, no significant difference was detected bilaterally (p=0.429); the distance from femoral nerve to pubis in affected hip (26.2±6.90mm) was significantly larger (p=0.036) than that in healthy hip (21.70±2.17mm).
In section D, the distance from sciatic nerve to femur in affected hip (15.62±1.11mm) was significantly larger (p=0.001) than that in healthy hip (14.52±0.86mm). The distance from femoral nerve to femur in affected hip (30.40±5.67mm) was significantly larger (p=0.013) than that in healthy hip (34.36±5.33mm). The detailed values are shown in Tables 2 and 3.
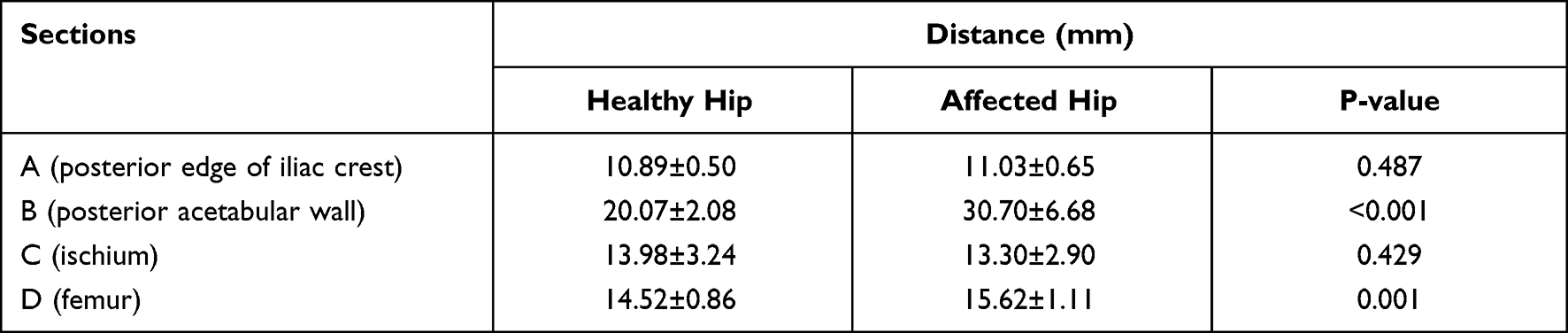 |
Table 2 Distance from Sciatic Nerve to Bony Landmarks on Each Section |
 |
Table 3 Distance from Femoral Nerve to Bony Landmarks on Each Section |
Discussion
Comparing to healthy hips, the femoral nerve in affected hips moved away from the femur while it got closer to anterior acetabular wall. The distances from the sciatic nerve to posterior acetabular wall and femur in affected hips were larger than those in healthy hips.
Understanding the anatomic adjacency of sciatic and femoral nerves in hip region could help reduce nerve injury during THA.17–19 Previous studies on peripheral nerve anatomy and course were mainly based on magnetic resonance imaging (MRI) or cadaveric specimens. However, CT might be a better choice of evaluating nerve course for DDH.20–25 On the one hand, MRI was not a routine examination for DDH patients and cannot clearly show bony landmarks; it would increase patients’ medical costs purely for the purpose of observing nerve course. On the other hand, it was very difficult to find cadaveric donors with DDH. Several researchers have confirmed that CT, as a routine preoperative examination for Crowe type-IV DDH patients, can accurately identify sciatic and femoral nerve.21,26,27
To date, there was only one study done in the subject of nerve course in patients with DDH. In 2015, Wang et al15 used CT to observe the nerve course in DDH patients and summarized the anatomical characteristics of sciatic nerve. They found that the sciatic nerve was located near the ischium and ilium but relatively far from the femur of the affected hip, compared to its location on the healthy hip for patients with unilateral DDH.15 Their finding was important to help surgeons improve their understanding of soft tissue developmental abnormalities around the hip joint in patients with DDH, thereby reducing the risk of nerve injury. However, there were still some flaws in their study. Firstly, the study did not include Crowe type-IV DDH, who was at the highest danger of nerve injury. Secondly, the reference section for all measurements were femur-based, and the femoral landmarks varied with the dislocation level, which reduced the comparability of bilateral nerves anatomical position. Thirdly, their measurement region excluded the area above acetabulum and the area below lesser trochanter, which were often the operating region for Crowe type-IV DDH patients. Fourthly, only the sciatic nerve, but not the femoral nerve was analyzed.
The femoral nerve injury accounted for 27.78% (5/18) of all nerve injuries after surgery in Crowe type-IV DDH.5 However, previous studies reported that femoral nerve was more resistant to distraction than sciatic nerve; limb lengthening may not be the main cause of femoral nerve injury.11,12 Our findings provided a new explanation for femoral nerve injury in Crowe type-IV DDH from the nerve course viewpoint. Firstly, the femoral nerve was only 1.3 cm on average away from the anterior acetabular wall, improperly positioned the retractor anterior to acetabulum, or prolonged traction may injure the femoral nerve. Secondly, overhanging acetabular cup was a common sacrifice for cup stability in Crowe type-IV DDH hip replacement. The femoral nerve, originating from lumbar plexus, arced around anterior aspect of acetabulum into femoral triangle. When femoral nerve was stretched and tensed with less arc, nerve injury happened with touching the anterior edge of overhanging acetabular cup and cause.
Some studies have also confirmed that the placement of retractor anterior to acetabulum was a high-risk step of femoral nerve injury. Shubert et al26 investigated the position of acetabular retractor in relation to adjacent neurovascular structures in CT scans and cadavers. They found that the anterior inferior iliac spine is the safest anterior acetabular retractor position, with inferior progression along the anterior wall, the distance to the femoral neurovascular bundle decreases.26 In our study, the distance between femoral nerve and anterior acetabular wall was smaller in Crowe type-IV DDH compared to normally developed hip, which might increase the risk of intraoperative femoral nerve injury.
The advantages of this study are reflected in the following aspects. Firstly, only unilateral Crowe type-IV DDH cases were included, eliminating the effect of factors such as body size on the data via an own-control design. Then, demographics such as gender, age, height, and weight were qualified, and previous history and neurological autoimmune diseases were excluded from interfering with the results. Finally, it’s the bony landmarks of the pelvis not of the femur that were chosen as references, which was not affected by the height of femoral dislocation.
This study, however, also has several limitations. First, these criteria were very restrictive and excluded nearly 70% of Crowe-IV DDH cases, making the sample size of this study relatively small. Second, the postoperative neurological complications of the cases were not studied, and it was not possible to correlate anatomical characteristic with clinical outcomes. So, we failed to evaluate the true impact of nerve coursing abnormalities on postoperative neurological function. Third, CT measurements in the supine position do not truly reflect the neurological status in the lateral position. Fourth, the morphological study of linear distances through different CT sections can be influenced by several factors, including height of patients, the scanning posture, the selected CT section etc. Although we have set the strict inclusion and exclusion criteria to minimize their influence, there may still have certain degree error in this method. Accordingly, a more comprehensive morphometric geometrical analysis via 3D reconstruction may receive more interesting results and benefit the clinical application better.
Conclusion
In female patients with unilateral Crowe type-IV DDH, the femoral nerve in affected hip runs closer to anterior acetabular wall than that in healthy hip.
Data Sharing Statement
The data used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgments
Our study protocol was approved by the Ethics Committee of Chinese PLA General Hospital and informed consent obtained from the study participants prior to study commencement. All procedures were conducted in compliance with the guidelines of the Declaration of Helsinki. We have obtained consent for publication. Ping Song and Xiangpeng Kong are co-first authors for this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by 1. Beijing Municipal Natural Science Foundation (M22016), 2. Clinical Application-oriented Medical Innovation Foundation from National Clinical Research Center for Orthopedics, Sports Medicine & Rehabilitation and Jiangsu China-Israel Industrial Technical Research Institute Foundation (2021-NCRC-CXJJ-ZH-01), 3. The National Natural Science Foundation of China (81772320).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Farrell CM, Springer BD, Haidukewych GJ, Morrey BF. Motor nerve palsy following primary total hip arthroplasty. J Bone Joint Surg Am. 2005;87:2619–2625.
2. Fleischman AN, Rothman RH, Parvizi J. Femoral Nerve Palsy Following Total Hip Arthroplasty: incidence and Course of Recovery. J Arthroplasty. 2018;33:1194–1199.
3. Wang D, Zeng W-N, Qin Y-Z, Pei F-X, Wang H-Y, Zhou Z-K. Long-Term Results of Cementless Total Hip Arthroplasty for Patients With High Hip Dislocation After Childhood Pyogenic Infection. J Arthroplasty. 2019;34:2420–2426.
4. de Bruijn IL, Geertzen JHB, Dijkstra PU. Functional outcome after peroneal nerve injury. Int J Rehabil Res. 2007;30:333–337.
5. Kong X, Chai W, Chen J, Yan C, Shi L, Wang Y. Intraoperative monitoring of the femoral and sciatic nerves in total hip arthroplasty with high-riding developmental dysplasia. Bone Joint J. 2019;101-B:1438–1446.
6. Nercessian OA, Piccoluga F, Eftekhar NS. Postoperative sciatic and femoral nerve palsy with reference to leg lengthening and medialization/lateralization of the hip joint following total hip arthroplasty. Clin Orthop Relat Res. 1994;1:165–171.
7. DeHart MM, Riley LH. Nerve injuries in total hip arthroplasty. J Am Acad Orthop Surg. 1999;7:101–111.
8. Eggli S, Hankemayer S, Müller ME. Nerve palsy after leg lengthening in total replacement arthroplasty for developmental dysplasia of the hip. J Bone Joint Surg Br. 1999;81:843–845.
9. Lai K-A, Shen W-J, Huang L-W, Chen M-Y. Cementless total hip arthroplasty and limb-length equalization in patients with unilateral Crowe type-IV hip dislocation. J Bone Joint Surg Am. 2005;87:339–345.
10. Weber ER, Daube JR, Coventry MB. Peripheral neuropathies associated with total hip arthroplasty. J Bone Joint Surg Am. 1976;58:66–69.
11. de Medinaceli L, Leblanc AL, Merle M. Functional consequences of isolated nerve stretch: experimental long-term static loading. J Reconstr Microsurg. 1997;13:185–192.
12. Lazansky MG. Complications revisited. The debit side of total hip replacement. Clin Orthop Relat Res. 1973;1:96–103.
13. Fei D, Ma L-P, Yuan H-P, Zhao D-X. Comparison of femoral nerve block and fascia iliaca block for pain management in total hip arthroplasty: a meta-analysis. Int J Surg. 2017;46:11–13.
14. Hasija R, Kelly JJ, Shah NV, et al. Nerve injuries associated with total hip arthroplasty. J Clin Orthop Trauma. 2018;9:81–86.
15. Liu R, Liang J, Wang K, Dang X, Bai C. Sciatic nerve course in adult patients with unilateral developmental dysplasia of the hip: implications for hip surgery. BMC Surg. 2015;15:14.
16. Jessel RH, Zurakowski D, Zilkens C, Burstein D, Gray ML, Kim Y-J. Radiographic and patient factors associated with pre-radiographic osteoarthritis in hip dysplasia. J Bone Joint Surg Am. 2009;91:1120–1129.
17. Rogers BA, Garbedian S, Kuchinad RA, Backstein D, Safir O, Gross AE. Total hip arthroplasty for adult hip dysplasia. J Bone Joint Surg Am. 2012;94:1809–1821.
18. Cameron HU, Eren OT, Solomon M. Nerve injury in the prosthetic management of the dysplastic hip. Orthopedics. 1998;21:980–981.
19. MacKenzie JR, Kelley SS, Johnston RC. Total hip replacement for coxarthrosis secondary to congenital dysplasia and dislocation of the hip. Long-term results. J Bone Joint Surg Am. 1996;78:55–61.
20. Tagliafico A, Podestà A, Assini A, et al. MR Imaging of total hip arthroplasty: comparison among sequences to study the sciatic nerve at 1.5 T. Magn Reson Imaging. 2010;28:1319–1326.
21. Ergun T, Lakadamyali H. CT and MRI in the evaluation of extraspinal sciatica. Br J Radiol. 2010;83:791–803.
22. Mehta CR, Constantinidis A, Farhat M, Suthersan M, Graham E, Kanawati A. The distance of the femoral neurovascular bundle from the hip joint: an intraoperative guide to reduce iatrogenic injury. J Orthop Surg Res. 2018;13:135.
23. Wang T-I, Chen H-Y, Tsai C-H, Hsu H-C, Lin T-L. Distances between bony landmarks and adjacent nerves: anatomical factors that may influence retractor placement in total hip replacement surgery. J Orthop Surg Res. 2016;11:31.
24. Güvençer M, Akyer P, Iyem C, Tetik S, Naderi S. Anatomic considerations and the relationship between the piriformis muscle and the sciatic nerve. Surg Radiol Anat. 2008;30:467–474.
25. Dikici F, Kale A, Ugras AA, Gayretli O, Gurses IA, Kaya I. Sciatic nerve localization relative to the position of the hip, an anatomical study. Hip Int. 2011;21:187–191.
26. Shubert D, Madoff S, Milillo R, Nandi S. Neurovascular structure proximity to acetabular retractors in total hip arthroplasty. J Arthroplasty. 2015;30:145–148.
27. Selkirk GD, Mclaughlin AC, Mirjalili SA. Revisiting the surface anatomy of the sciatic nerve in the gluteal region in children using computed tomography. Clin Anat. 2016;29:211–216.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.