Back to Journals » Journal of Inflammation Research » Volume 18
The Correlation Study of Bone Metabolism and Inflammatory Markers with Major Adverse Cardiovascular Events in Patients with Obstructive Sleep Apnea Syndrome
Authors Guo G, Xiao J, Chen J, Zhu C, Zhang Q, Li F
Received 26 May 2025
Accepted for publication 27 October 2025
Published 11 November 2025 Volume 2025:18 Pages 15817—15831
DOI https://doi.org/10.2147/JIR.S538725
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Qing Lin
Guohua Guo,1,2 Jianhong Xiao,1,2 Junhua Chen,1,2 Chuanqi Zhu,1,2 Qinghua Zhang,1,2 Feng Li1,2
1Department of Respiratory and Critical Care Medicine, Mindong Hospital Affiliated to Fujian Medical University, Fu’an, Fujian Province, 355000, People’s Republic of China; 2Department of Infectious Diseases, Mindong Hospital Affiliated to Fujian Medical University, Fu’an, Fujian Province, 355000, People’s Republic of China
Correspondence: Feng Li, Department of Respiratory and Critical Care Medicine, Mindong Hospital Affiliated to Fujian Medical University, No. 89 Heshan Road, Chengnan Street, Fu’an, Fujian Province, 355000, People’s Republic of China, Email [email protected]
Background: Obstructive sleep apnea syndrome (OSAS) elevates the risk of major adverse cardiovascular events (MACEs), though the underlying mechanisms are not fully elucidated. This study investigated the correlations between bone metabolism markers, inflammatory cytokines, and MACEs in OSAS patients.
Methods: A retrospective study was conducted on patients diagnosed with OSAS between March 2019 and March 2022, alongside baseline characteristics - matched controls without OSAS. The cohort comprised 496 OSAS patients and 545 controls. Based on the occurrence of major adverse cardiovascular events (MACEs), the entire cohort (n=1041) was segregated into a MACE group (n=120) and a non-MACE group (n=921). Clinical data collected included demographic information, polysomnography results, bone metabolism markers (β-CrossLaps [β-CTX], total procollagen type I N-terminal propeptide [TPINP]), and inflammatory cytokines (interleukin-1 beta [IL-1β], interleukin-6 [IL-6], C-reactive protein [CRP], tumor necrosis factor-alpha [TNF-α], interleukin-10 [IL-10], interferon-gamma [IFN-γ]). Statistical analyses included independent t tests, Pearson correlation coefficients, logistic regression, and structural equation modeling.
Results: OSAS patients showed significantly higher β-CTX (0.49± 0.15 vs 0.43± 0.14 ng/mL; P< 0.001) and lower TPINP (103.81± 37.57 vs 118.19± 41.20 ng/mL; P< 0.001) than controls. Levels of IL-6, TNF-α, and IL-1β were also elevated in the OSAS group (all P< 0.01). MACEs were more frequent in OSAS patients (P=0.002). Multivariate analysis identified severe OSAS (OR=2.771, P< 0.001), elevated IL-6 (OR=1.114, P=0.013), elevated IL-1β (OR=1.598, P=0.033), and increased β-CTX (OR=3.386, P< 0.001) as independent MACE predictors. SEM revealed OSAS directly associated with MACEs (β=0.18) and indirectly via inflammatory and bone metabolism pathways.
Conclusion: Altered bone metabolism markers and elevated pro-inflammatory cytokines are associated with an increased risk of MACEs in OSAS patients, suggesting their role in the pathophysiology of OSAS-related cardiovascular morbidity. Monitoring these markers could aid in risk stratification.
Keywords: obstructive sleep apnea syndrome, bone metabolism, inflammatory markers, major adverse cardiovascular events
Introduction
Obstructive sleep apnea syndrome (OSAS) is a prevalent sleep disorder marked by recurrent instances of upper airway blockage during sleep, resulting in intermittent hypoxia and fragmented sleep patterns.1,2 It impacts roughly 9–38% of the overall adult population, with higher prevalence in males and individuals with elevated body mass index (BMI).3 The pathophysiological implications of OSAS extend beyond disrupted sleep architecture, spanning a wide range of systemic effects that contribute to morbidity and mortality.4
One of the significant clinical concerns associated with OSAS is its strong linkage to cardiovascular diseases (CVDs). Multiple studies have demonstrated that OSAS is an independent predictor for hypertension, coronary artery disease, stroke, and heart failure.5,6 This risk is often compounded by common comorbidities like obesity, with anthropometric measures such as BMI being closely linked to both OSAS severity and cardiovascular risk.7,8 The pathophysiological links involve intermittent hypoxia triggering oxidative stress, sympathetic activation, endothelial dysfunction, and systemic inflammation.9–11
Despite the well-established association between OSAS and adverse cardiovascular outcomes, the underlying mechanisms remain incompletely understood. Inflammation has been identified as a key mediator, with pro-inflammatory cytokines such as interleukin-6 (IL-6), tumor necrosis factor-alpha (TNF-α), and interleukin-1 beta (IL-1β) playing pivotal roles in vascular endothelial injury and atherogenesis.11,12 Increased concentrations of these cytokines were noted in patients affected by OSAS, correlating with disease severity and cardiovascular risk.13
Bone metabolism, traditionally studied within the context of skeletal health, has emerged as a potential contributor to cardiovascular pathology.14 Markers of bone turnover, such as beta-cross-linked C-telopeptide of type I collagen (β-CTX) and total procollagen type I N-terminal propeptide (TPINP), reflect the dynamic processes of bone resorption and formation, respectively. Dysregulation of bone metabolism has been associated with vascular calcification and stiffness, promoting atherosclerotic changes and increasing the risk of cardiovascular events.15 In the context of OSAS, intermittent hypoxia and systemic inflammation may disrupt the bone remodeling balance. Pro-inflammatory cytokines like IL-6 and TNF-α, elevated in OSAS, can stimulate osteoclast activity and bone resorption.16 Concurrently, hypoxia-inducible factors may influence the expression of mediators linking bone and vascular calcification.17 This dysregulated bone metabolism, particularly increased resorption, might contribute to vascular calcification and stiffness, thereby promoting atherosclerosis and elevating cardiovascular risk.18
The interplay between bone metabolism and systemic inflammation offers a compelling avenue for exploration in OSAS. Inflammatory cytokines not only influence vascular function but also modulate bone remodeling.19 For instance, IL-6 and TNF-α stimulate osteoclast differentiation and activity, enhancing bone resorption, while IL-1β can inhibit osteoblast function. Conversely, bone-derived factors may impact vascular health, suggesting a bidirectional relationship.20
Given these considerations, it is plausible that alterations in bone metabolism markers and inflammatory cytokines among individuals with OSAS may play a role in the heightened incidence of major adverse cardiovascular events (MACEs) observed in this population. However, the correlation between bone metabolism, inflammation, and cardiovascular risk in OSAS has not been fully elucidated.21,22
The objective of this study is to examine the associations among bone metabolism markers, inflammatory cytokines, and the occurrence of MACEs in patients with OSAS. By comparing these parameters between OSAS patients and matched controls without OSAS, and further stratifying OSAS patients based on the presence of MACEs, we seek to identify potential biomarkers and mechanisms underlying the increased cardiovascular risk.
Research Methods and Materials
Study Framework and Participants
This retrospective study analyzed patients diagnosed with OSAS at our hospital between March 2019 and March 2022. The OSAS group comprised 496 patients identified from electronic medical records (EMR). The control group (Non-OSAS Group, n = 545) consisted of baseline characteristics -matched individuals from a health screening database who underwent polysomnography (PSG) confirming absence of OSAS (Apnea-Hypopnea Index, AHI < 5). Baseline characteristics (age, gender, BMI, smoking/alcohol history, comorbidities) were extracted at the time of OSAS diagnosis (“time 0”). Propensity score matching (PSM) was applied using these baseline variables to minimize confounding and create balanced groups for comparison, resulting in 408 matched pairs.
Based on the occurrence of MACEs, 1041 patients were further segregated into two groups: 120 patients who experienced MACE were categorized as the MACE group (n = 120), and 921 patients who did not experience MACE were designated as the non-MACE group (n = 921).
The study was approved by the Institutional Review Board and Research Ethics Committee of the Mindong Hospital Affiliated to Fujian Medical University, and was conducted in accordance with the tenets of the Declaration of Helsinki. As clinical data of patients, including basic demographic information and PSG parameters, were extracted from the hospital’s electronic medical record system, the requirement for informed consent from patients was waived. All patient data were anonymized and maintained with strict confidentiality to protect patient privacy throughout the research process.
Eligibility and Disqualification Criteria
Eligibility Criteria: All participants were aged between 18 and 65 years. Patients in the OSAS group met the diagnostic criteria for OSAS.23 Complete baseline data records were available for all participants, including but not limited to age, gender, BMI, smoking history, alcohol consumption history, and comorbidities (such as hypertension, diabetes, etc). Sufficient follow-up data were available for analysis.
Disqualification Criteria: Participants were excluded if they were currently taking medications that could significantly affect bone metabolism or inflammatory responses (such as glucocorticoids, bisphosphonates, etc), had undergone major surgery recently or were in the recovery phase of an acute illness, had severe cognitive impairment that prevented them from understanding or complying with study requirements, or were pregnant or breastfeeding. For the OSAS group, patients with other types of sleep disorders (such as central sleep apnea, rapid eye movement sleep behavior disorder, etc.) or those who did not provide sufficient follow-up data were also excluded. For the Non-OSAS group, patients with a history of major adverse cardiovascular events such as myocardial infarction, stroke, heart failure, or other chronic conditions that could lead to abnormal bone metabolism or inflammatory responses (such as chronic kidney disease, liver cirrhosis, etc.) were excluded.
Polysomnography Protocol
PSG was conducted using Compumedics E-series equipment (Australia), and data analysis was performed using Profusion PSG 5.1 software. Respiratory events were defined according to the AASM 2020 criteria24 as follows:
Apnea: A reduction in airflow by ≥90% lasting at least 10 seconds.
Hypopnea: A reduction in airflow by ≥50%, along with either a decline in oxygen saturation (SaO2) by ≥3% or the occurrence of arousal.
Key oxygenation indices included:
Oxygen Desaturation Index (ODI): The number of SaO2 drops by ≥3% per hour.
Lowest Oxygen Saturation (LSpO2): The lowest recorded SaO2 level during the study period.
CT90: The percentage of time spent with oxygen saturation below 90%.
The severity of OSAS was stratified based on the AHI as follows:
Mild: 5 ≤ AHI < 15
Moderate: 15 ≤ AHI < 30
Severe: AHI ≥ 30
Additionally, clinical symptoms such as daytime sleepiness, nighttime snoring, witnessed apneas, or choking events were also considered critical for the diagnosis of OSAS.
Data Collection
Data Sources: Clinical data of patients, including basic demographic information (age, gender, BMI, smoking history, alcohol consumption history, comorbidities, etc), PSG parameters, were extracted from the hospital’s electronic medical record system. Biochemical marker raw data were retrieved from the laboratory database. All PSG studies, biomarker measurements (bone metabolism and inflammatory markers), and baseline clinical data were collected at the time of OSAS diagnosis (baseline).
Bone Metabolism Markers Measurement: Fasting morning venous blood samples were collected between 7:00 and 9:00 AM. Serum levels of calcium (Ca), phosphorus (P), and alkaline phosphatase (ALP) were measured using an automated biochemical analyzer (Roche Cobas c702, Roche Diagnostics Ltd., Switzerland). Serum TPINP and β-CTX levels were quantified using an electrochemiluminescence immunoassay on a Roche Elecsys 2010 analyzer (Roche Diagnostics Ltd., Switzerland). All bone metabolism marker assays were performed in duplicate. The lower limits of detection (LLOD) and inter-assay coefficients of variation (CV) were as follows: TPINP (LLOD: 5 ng/mL, CV: <4.5%); β-CTX (LLOD: 0.01 ng/mL, CV: <5.8%).
Inflammatory Markers Measurement: Inflammatory markers (IL-1β, IL-6, TNF-α, interleukin-10 [IL-10], interferon gamma [IFN-γ]) were measured from the same fasting morning serum samples using a Luminex 200 suspension array system (Luminex Corporation, USA) with commercially available multiplex assay kits (R&D Systems, USA). High-sensitivity CRP (hs-CRP) was measured by immunoturbidimetry on the Roche Cobas c702 analyzer. All inflammatory marker analyses were performed in duplicate. The LLOD and inter-assay CVs for the Luminex assays were: IL-1β (0.1 pg/mL, CV<8%); IL-6 (0.2 pg/mL, CV<7%); TNF-α (0.5 pg/mL, CV<9%); IL-10 (0.5 pg/mL, CV<8%); IFN-γ (1.0 pg/mL, CV<10%). For hs-CRP, the LLOD was 0.1 mg/L and the inter-assay CV was <5%.
Documentation of complications: Complication information was extracted from the hospital’s electronic medical record (EMR) system. MACEs were defined as myocardial infarction, ischemic or hemorrhagic stroke, heart failure, and coronary revascularization (PCI or CABG).25 Initial identification was performed by two trained research assistants. All potential MACEs cases were independently verified by a cardiologist with 10 years of experience in cardiovascular disease. The verification process included review of medical records, imaging reports, and laboratory data to confirm the diagnosis.
Analytical Methods
Data were analyzed using SPSS 29.0 statistical software (SPSS Inc., Chicago, IL, USA). To address potential covariate bias, PSM was used to include all available baseline variables, including age, gender, BMI, smoking history, drinking history, and comorbidities (eg, hypertension, diabetes). Logistic regression analysis was employed to calculate the propensity scores, and a 1:1 nearest neighbor matching method without replacement was applied, with a caliper set at 20% of the standard deviation of the PSM scores between the two groups. Categorical data were presented as frequencies and percentages [n(%)] and compared using Chi-square tests or Fisher’s exact test as appropriate. Continuous, normally distributed data were expressed as means ± standard deviations and compared using independent samples t-tests. These tests were used for the between-group comparisons presented in the tables. Correlation analyses were performed using Pearson correlation coefficients. Multivariate analyses were performed using logistic regression. A P value <0.05 was considered statistically significant. Structural equation modeling (SEM) was employed to explore the potential pathways between OSAS severity, bone metabolism markers (TPINP, β-CTX), inflammatory markers (IL-1β, IL-6, TNF-α), and MACEs The model was constructed using AMOS 26.0 software, with parameters estimated via maximum likelihood estimation.
Results
Basic Data of Patients
In this study, we examined the baseline characteristics of patients. Prior to matching, statistically significant discrepancies existed between the non-OSAS and OSAS groups with respect to BMI, with the OSAS group exhibiting a higher BMI (26.32 ± 6.81 kg/m2 vs 25.21 ± 6.52 kg/m2; P=0.007), and gender distribution, with a higher prevalence of males in the OSAS group (75.60% vs 69.36%; P=0.024) (Table 1). However, age, smoking and drinking history, diabetes, hypertension, educational level, and marital status did not show significant differences, suggesting a general demographic similarity apart from BMI and gender (Table 2). After propensity score matching, these differences were mitigated, resulting in balanced groups across all measured parameters.
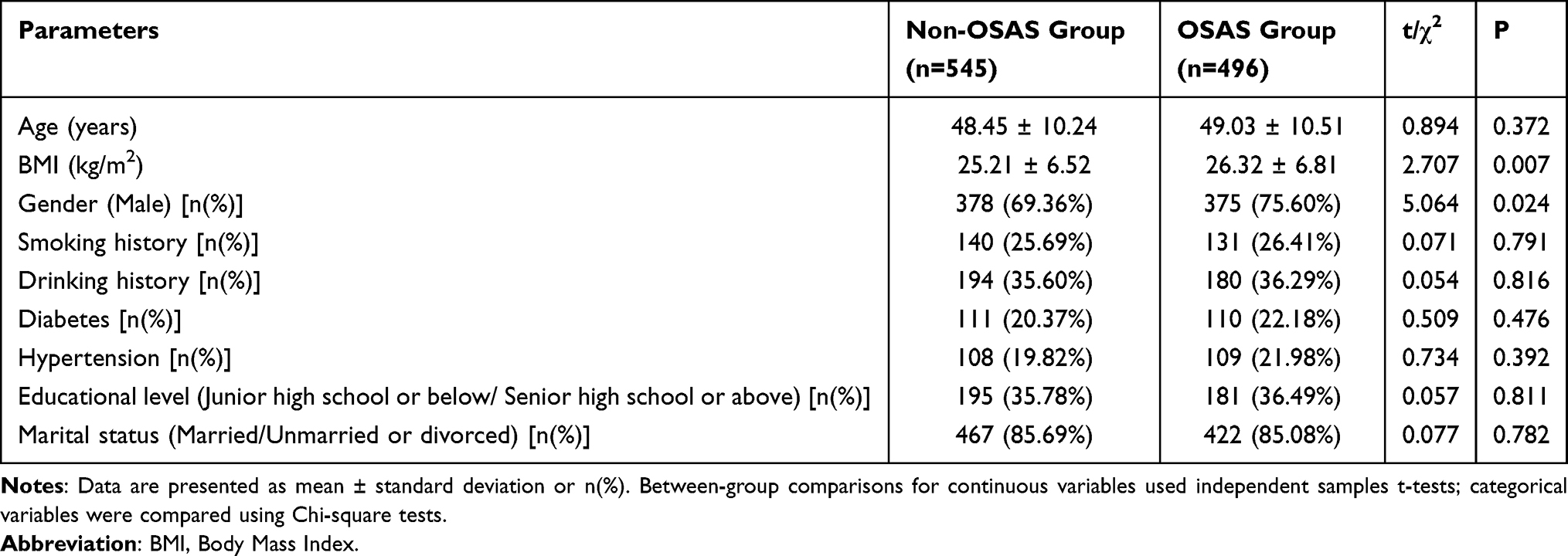 |
Table 1 Baseline Characteristics Before Propensity Score Matching |
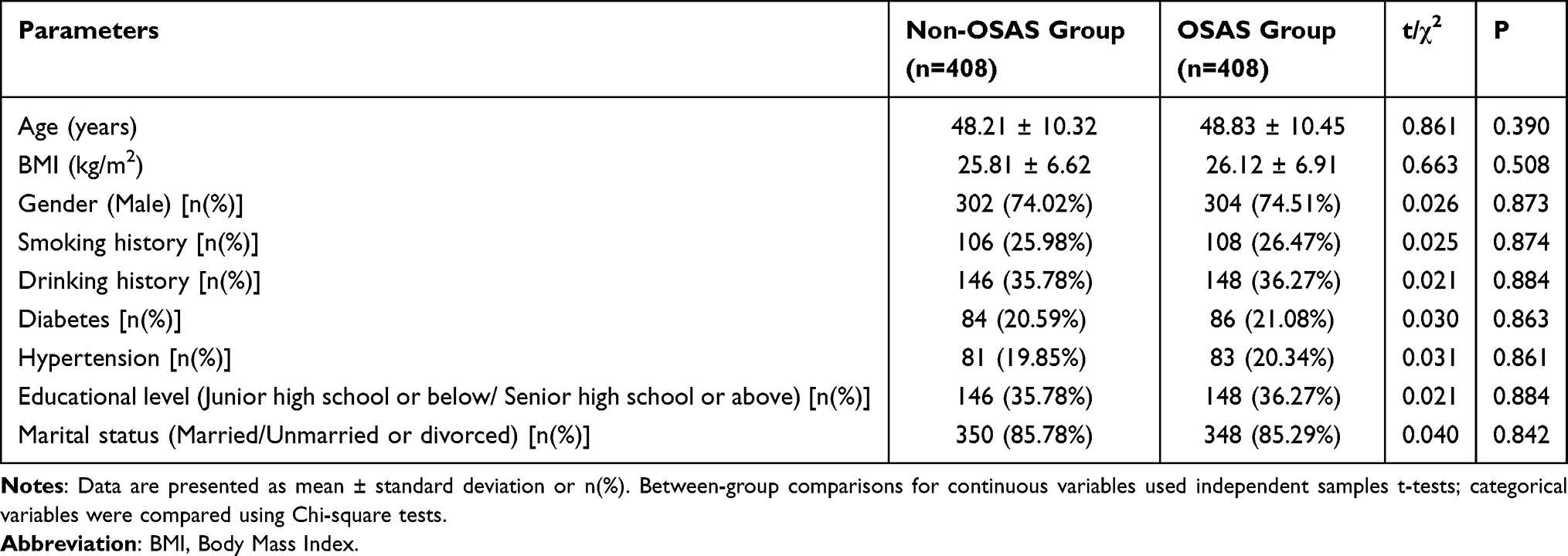 |
Table 2 Baseline Characteristics After Propensity Score Matching |
Manifestations and Indicators of Obstructive Sleep Apnea Syndrome (OSAS)
In the comparative analysis of clinical symptoms and polysomnography results between the OSAS and non-OSAS groups, significant differences were observed across all measured parameters. The prevalence of clinical symptoms such as daytime sleepiness, nocturnal arousals, snoring at night, witnessed apnea, and choking events were markedly more pronounced in the OSAS group than in the non-OSAS group (all P<0.001) (Table 3). Specifically, daytime sleepiness was reported by 51.47% of individuals in the OSAS group versus 13.72% in the non-OSAS group. Additionally, nocturnal arousals and snoring at night were considerably more prevalent in the OSAS group (46.32% and 76.47%, respectively) compared to their non-OSAS counterparts (11.03% and 19.12%, respectively). Regarding polysomnographic findings, the AHI was markedly elevated in the OSAS group, with a mean of 23.52±8.25 events/hour, contrasting sharply with 2.30±1.12 events/hour in the non-OSAS group (P<0.001) (Table 4). Furthermore, the OSAS group had markedly lower mean oxygen saturations (SaO2: 89.71±4.69% vs 96.15±1.20%), lower minimum oxygen saturation levels (LSpO2: 78.33±5.16% vs 85.20±1.51%), and higher indices reflecting compromised oxygenation (CT90: 11.12±5.08% vs 0.51±0.05%; ODI: 15.71±6.63 events/hour vs 1.29±0.62 events/hour; all P<0.001). These findings demonstrate substantial physiological and clinical disparities between the groups, underscoring the profound impact of OSAS on respiratory and sleep parameters.
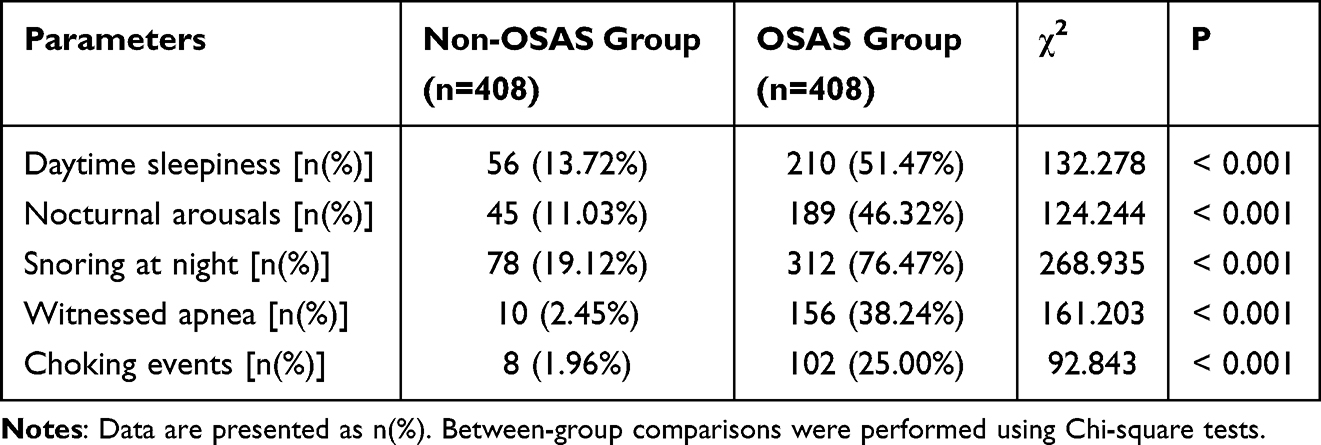 |
Table 3 Comparison of Clinical Symptoms Between Two Groups |
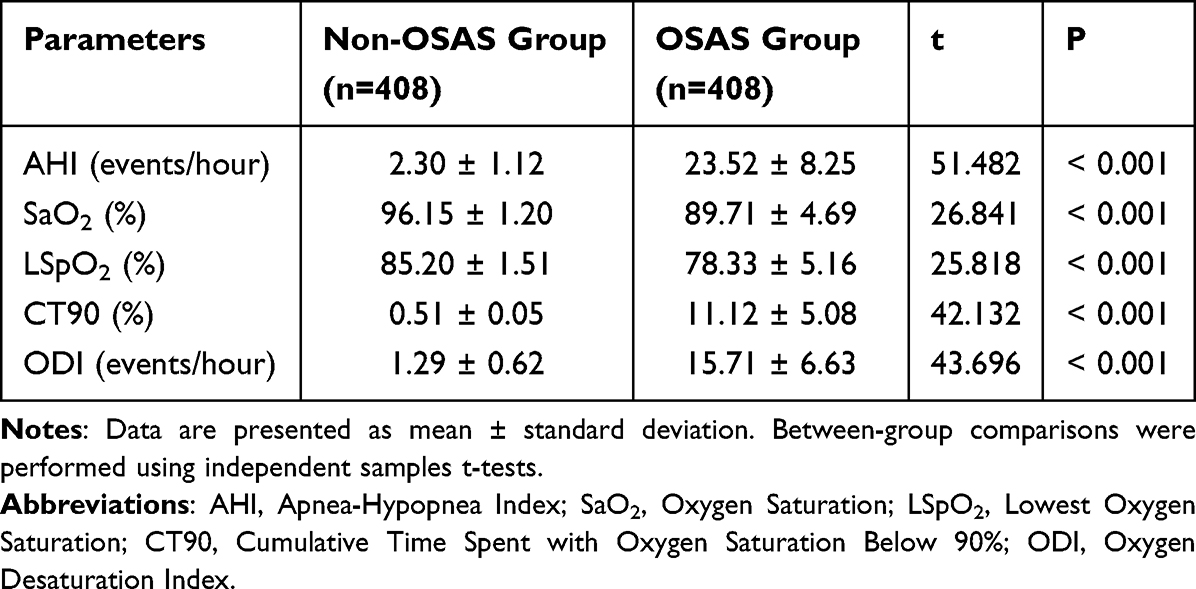 |
Table 4 Comparison of Polysomnography Results Between Two Groups |
Bone Metabolism and Inflammatory Markers
In the analysis of bone metabolism markers between the OSAS and non-OSAS groups, the levels of β-CTX exhibited a considerable increase in the OSAS group (0.49 ± 0.15 ng/mL) compared to the non-OSAS group (0.43 ± 0.14 ng/mL), with this difference reaching statistical significance (P<0.001) (Figure 1). Additionally, the levels of TPINP were markedly lower in the OSAS group (48.85 ± 19.87 ng/mL) than in the non-OSAS group (53.20 ± 20.49 ng/mL; P=0.002). However, other bone metabolism markers such as serum calcium (Ca), phosphorus (P), and alkaline phosphatase (ALP) did not exhibit significant differences between the two groups. Regarding inflammatory markers, the OSAS group exhibited significantly higher levels of IL-6 (2.90 ± 1.08 pg/mL vs 2.69 ± 0.85 pg/mL; P=0.003), TNF-α (6.10 ± 2.50 pg/mL vs 5.57 ± 2.31 pg/mL; P=0.002), and IL-1β (1.04 ± 0.39 pg/mL vs 0.97 ± 0.32 pg/mL; P=0.005) compared to the non-OSAS group (Figure 2). The levels of other inflammatory markers, including C-reactive protein (CRP), IL-10, and IFN-γ, did not differ significantly between the groups. These findings indicate a pronounced alteration in specific bone metabolism and inflammatory markers in patients with OSAS, which could be linked to the risk of major adverse cardiovascular events.
 |
Figure 1 Comparison of bone metabolism markers between two groups. **P<0.01; ***P<0.001. Data are presented as mean ± standard deviation. Between-group comparisons were performed using independent samples t-tests. Abbreviations: Ca, Serum calcium; P, Phosphorus; ALP, Alkaline Phosphatase; TPINP, Total Procollagen I N-Terminal Propeptide; β-CTX, Beta -collagen cross-linked. |
 |
Figure 2 Comparison of inflammatory markers between two groups. **P<0.01. Data are presented as mean ± standard deviation. Between-group comparisons were performed using independent samples t-tests. Abbreviations: IL-6, Interleukin-6; TNF-α, Tumor Necrosis Factor Alpha; CRP, C-Reactive Protein; IL-1β, Interleukin-1 Beta; IL-10, Interleukin-10; IFN-γ, Interferon Gamma. |
Complications
The analysis of complication incidences between the OSAS and non-OSAS groups revealed a markedly higher occurrence of Major Adverse Cardiovascular Events (MACEs) in the OSAS group (P=0.002) (Table 5). Specifically, the OSAS group demonstrated a greater incidence of myocardial infarction (4.41% vs 1.72%), ischemic or hemorrhagic stroke (6.13% vs 2.45%), heart failure (2.94% vs 1.47%), and coronary revascularization (3.68% vs 1.96%) than the non-OSAS group. In contrast, the prevalence of complications such as gastroesophageal reflux disease (GERD), depression, and nocturia showed no significant difference between the two groups, with P-values of 0.816, 0.770, and 0.704, respectively. These results underscore a strong correlation between OSAS and an elevated likelihood of experiencing major cardiovascular events, highlighting the importance of monitoring and managing cardiovascular risk in these patients.
 |
Table 5 Comparison of Complications Incidence Between Two Groups |
Clinical Data of the Non-MACE Group and the MACE Group
The comparison of clinical data between the non-MACE and MACE groups revealed several significant differences (Table 6). The MACE group showed a markedly greater BMI versus the non-MACE group (26.93 ± 6.11 kg/m2 vs 25.61 ± 5.72 kg/m2; P=0.018), suggesting a potential connection between increased BMI and major adverse cardiovascular events (MACE). Additionally, the occurrence of severe OSAS was markedly greater in the MACE group (40.00% vs 8.79%; P<0.001), highlighting a strong correlation between severe OSAS and cardiovascular risk. Biochemical markers also showed significant differences. Specifically, levels of TPINP were lower in the MACE group (49.78 ± 19.80 ng/mL vs 54.20 ± 20.49 ng/mL; P=0.026), while β-CTX levels were higher (0.64 ± 0.25 ng/mL vs 0.58 ± 0.24 ng/mL; P=0.011). These findings suggest alterations in bone metabolism associated with MACE. Furthermore, inflammatory markers such as IL-6 (2.84 ± 1.09 pg/mL vs 2.55 ± 0.86 pg/mL; P=0.005), TNF-α (6.05 ± 2.50 pg/mL vs 5.50 ± 2.31 pg/mL; P=0.015), and IL-1β (1.19 ± 0.50 pg/mL vs 1.09 ± 0.44 pg/mL; P=0.039) were elevated in the MACE group, indicating an increased inflammatory state among these patients. Overall, these results suggest that higher BMI, severe OSAS, altered bone metabolism markers (TPINP and β-CTX), and raised levels of inflammatory markers (IL-6, TNF-α, and IL-1β) are related to an increased chance of major adverse cardiovascular events. These data underscore the critical role of monitoring and managing these indicators in patients at risk for MACE.
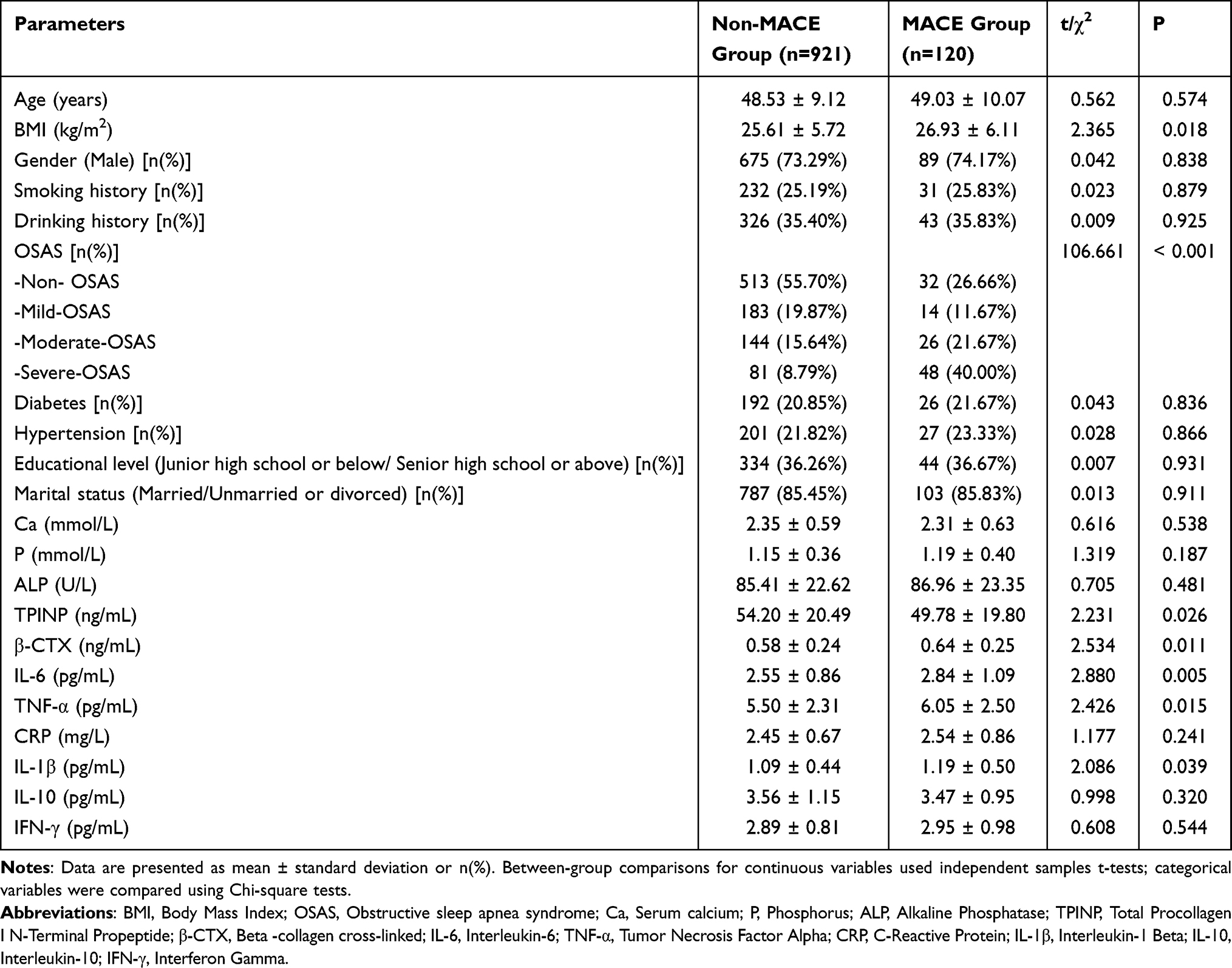 |
Table 6 Comparison of Clinical Data Between Two Groups |
Univariate and Multivariate Regression Analysis
The single-factor and multi-factor regression assessments identified several elements significantly related to the risk for MACEs in individuals with OSAS (Table 7). Both analyses demonstrated that higher BMI was a important predictor of MACEs, with an odds ratio (OR) per unit increase of 1.041 [95% CI, 1.007–1.076] in univariate analysis (P=0.019) and 1.044 [95% CI, 1.009–1.081] in multivariate analysis (P=0.014). OSAS presence strongly correlated with increased MACE risk, with ORs of 2.767 [95% CI, 1.257–6.136] (P<0.001) and 2.771 [95% CI, 1.195–6.426] (P<0.001) in univariate and multivariate analyses, respectively. Bone metabolism markers also influenced MACE risk: TPINP showed a protective effect, exhibiting multivariate OR of 0.987 [95% CI, 0.976–0.997] (P=0.012), whereas β-CTX was related to elevated risk (multivariate OR of 2.178 [95% CI, 1.820–2.607]; P=0.018). Moreover, inflammatory markers IL-6 and TNF-α were significant predictors, with IL-6 showing multivariate OR of 1.483 [95% CI, 1.174–1.875] (P<0.001), and TNF-α exhibiting an OR of 1.114 [95% CI, 1.023–1.214] (P=0.013). IL-1β also emerged as a predictor in both analyses, with a multivariate OR of 1.598 [95% CI, 1.021–2.504] (P=0.040). These findings highlight the significance of recognizing OSAS, BMI, specific bone metabolism, and inflammatory markers as critical factors in assessing cardiovascular risk in these patients.
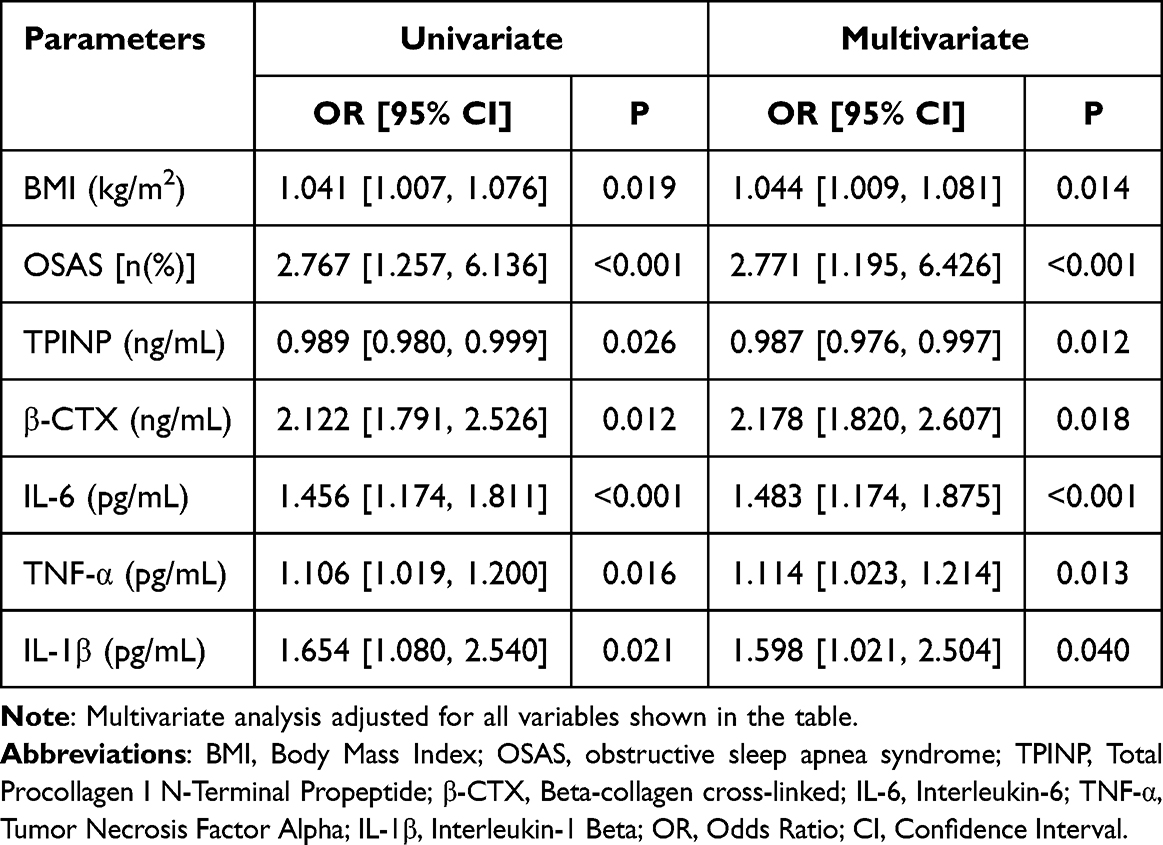 |
Table 7 Univariate and Multivariate Regression Analysis of Factors Influencing Major Adverse Cardiovascular Events |
Correlation Analysis
The correlation analysis identified notable connections between different severities of OSAS and various bone metabolism and inflammatory markers (Table 8). A negative relationship was detected between OSAS severity and TPINP, signified by rho = −0.122 (P=0.014), indicating reduced TPINP levels with increased OSAS severity. Conversely, positive correlations were found with β-CTX (rho = 0.190, P<0.001), IL-6 (rho = 0.260, P<0.001), TNF-α (rho = 0.143, P=0.004), and IL-1β (rho = 0.382, P<0.001), suggesting elevated levels of these markers with worsening OSAS. Additionally, a significant correlation was identified between the severity of OSAS and the incidence of Major Adverse Cardiovascular Events (MACEs), with rho = 0.258 (P<0.001). These findings underscore the intricate relationship between OSAS severity and alterations in bone metabolism and inflammation, as well as an increased cardiovascular risk, emphasizing the importance of monitoring these parameters in patients with OSAS.
 |
Table 8 Correlation Analysis of Different OSAS Severities with Bone Metabolism, Inflammatory Markers, and MACEs |
Structural Equation Modeling
The structural equation model depicted in Figure 3 elucidates the complex interplay between OSAS, bone metabolism, inflammatory markers, and major adverse cardiovascular events (MACEs). Obstructive sleep apnea syndrome was directly associated with MACEs (β=0.18), revealing its critical role as a predictor of cardiovascular risk. The model demonstrates that bone metabolism markers, indicated by β-CTX (β=0.32) and TPINP (β=0.11), mediated the impact of OSAS on cardiovascular outcomes, emphasizing their significant effects on MACEs (β=0.23). Similarly, inflammatory markers, such as TNF-α (β=0.21) and IL-6 (β=0.13), contributed to MACEs (β=0.26), underscoring their involvement in inflammation-linked cardiovascular pathology. Although BMI also contributed to the model, its direct influence on MACEs was less pronounced (β=0.12). This integrated model highlights the importance of bone metabolism and inflammation in the pathophysiology of OSAS-related cardiovascular complications.
 |
Figure 3 Structural Equation Modeling of Factors Influencing Major Adverse Cardiovascular Events in Patients with Obstructive Sleep Apnea Syndrome. Path coefficients (β) are standardized estimates. The model was constructed using AMOS 26.0 software with maximum likelihood estimation. Abbreviations: OSAS, Obstructive Sleep Apnea Syndrome; BMI, Body Mass Index; TPINP, Total Procollagen I N-Terminal Propeptide; β-CTX, Beta-collagen cross-linked; TNF-α, Tumor Necrosis Factor Alpha; IL-6, Interleukin-6; MACEs, Major Adverse Cardiovascular Events. |
Discussion
This study analyzed the associations among bone metabolism markers, inflammatory cytokines, and the occurrence of MACEs in patients diagnosed with OSAS. Our findings indicate that patients with OSAS exhibit significant alterations in bone metabolism and elevated levels of specific pro-inflammatory cytokines, which are related to a raised risk for MACE.26,27 These findings imply that OSAS might contribute to cardiovascular morbidity through mechanisms involving bone metabolism dysregulation and systemic inflammation.
The link between OSAS and cardiovascular diseases is well-documented, with OSAS acknowledged as an independent risk factor for hypertension, coronary artery disease, heart failure, and stroke.6,9 The intermittent hypoxia and fragmented sleep patterns of OSAS lead to physiological stress responses that can promote atherogenesis and cardiovascular dysfunction. In our study, patients with OSAS exhibited a markedly greater incidence of MACE relative to non-OSAS controls, reinforcing the notion that OSAS is intrinsically linked to adverse cardiovascular outcomes.28,29
One of the novel aspects of our study is the exploration of bone metabolism markers in OSAS patients and their potential role in cardiovascular risk. We observed that OSAS patients had elevated levels of β-CrossLaps (β-CTX), a marker of bone resorption, and decreased levels of TPINP, a marker of bone formation.30 This imbalance suggests a shift towards increased bone resorption and decreased bone formation in OSAS patients. Such alterations in bone metabolism may not only contribute to skeletal complications but may also have systemic effects influencing cardiovascular health.31
Bone metabolism is intricately linked to vascular health through shared signaling pathways and mediators. Osteocalcin, a hormone produced by osteoblasts, has been shown to influence insulin sensitivity and energy metabolism. Moreover, vascular calcification, a hallmark of atherosclerosis, comprises osteogenic differentiation of vascular smooth muscle cells, a process resembling bone formation. In the context of OSAS, intermittent hypoxia may induce oxidative stress and inflammatory responses that could disrupt the balance of bone remodeling. The increased β-CTX levels observed in our study might reflect heightened osteoclastic activity driven by systemic inflammation and hypoxia-induced stress. Conversely, the reduced TPINP levels may indicate suppressed osteoblastic activity, possibly due to disrupted anabolic signaling or hormonal imbalances.32
The elevated pro-inflammatory cytokines—IL-6, TNF-α, and IL-1β—in OSAS patients highlight the role of systemic inflammation as a mediator between OSAS and cardiovascular risk.33 These cytokines have been shown to contribute to atherogenesis by enhancing endothelial dysfunction, promoting leukocyte adhesion, and driving the expansion of vascular smooth muscle cells. IL-6, in particular, has been implicated in the progression of atherosclerotic plaques and their destabilization, leading to acute cardiovascular events. The positive correlations between OSAS severity and levels of these cytokines suggest that the burden of intermittent hypoxia may proportionally increase systemic inflammation.34
Intermittent hypoxia in OSAS activates hypoxia-inducible factors (HIFs), leading to the transcription of various genes involved in inflammatory responses, angiogenesis, and metabolic regulation. HIF activation can upregulate the expression of IL-6 and TNF-α, perpetuating a cycle of inflammation and endothelial dysfunction. Additionally, intermittent hypoxia may stimulate sympathetic nervous system activity and oxidative stress, further contributing to vascular injury and inflammation.35 Our structural equation modeling supports the intermediary function of inflammatory markers on the relation between OSAS and MACE, underscoring the importance of addressing systemic inflammation in OSAS management.
The interplay between bone metabolism and inflammation presents another layer of complexity. Pro-inflammatory cytokines such as IL-6 and TNF-α can influence bone remodeling by stimulating osteoclast differentiation and activity, leading to increased bone resorption. IL-1β has been shown to promote osteoclastogenesis and inhibit osteoblast function, contributing to bone loss. Therefore, the elevated levels of these cytokines in OSAS patients may not only impact vascular health but also exacerbate bone metabolism disorders. This bidirectional relationship suggests that interventions targeting inflammation in OSAS may have beneficial effects on both bone health and cardiovascular risk.36,37
Our findings have clinical implications for the management of OSAS patients. The identification of altered bone metabolism markers and elevated inflammatory cytokines as predictors of MACE suggests that these parameters could be used for risk stratification. Monitoring β-CTX, TPINP, IL-6, TNF-α, and IL-1β levels in OSAS patients may help identify those at higher risk for cardiovascular events. Moreover, therapeutic strategies aimed at modulating bone metabolism and reducing inflammation could potentially mitigate cardiovascular risk in this population.
Continuous positive airway pressure (CPAP) therapy, the gold standard treatment for OSAS, has been shown to improve endothelial function, reduce sympathetic activity, and decrease systemic inflammation. Studies have reported that CPAP therapy can lower levels of IL-6 and TNF-α, although responses may vary among individuals. Addressing bone metabolism alterations in OSAS patients may require additional interventions, such as optimizing vitamin D levels, ensuring adequate calcium intake, and potentially using pharmacological agents that modulate bone remodeling. Further investigations are required to examine the efficacy of such interventions in reducing MACE risk.38
Our research also underscores the significance of considering BMI as a factor in cardiovascular risk assessment among OSAS patients. Higher BMI was an independent predictor of MACE in our multivariate analysis, consistent with the well-established link between obesity, OSAS, and cardiovascular disease.7,8 Obesity is a major risk factor for OSAS and can exacerbate its severity. Furthermore, adipose tissue, particularly visceral fat, is a source of pro-inflammatory cytokines, creating a state of chronic low-grade inflammation that contributes to endothelial dysfunction and atherogenesis.11 This synergistic relationship suggests that OSAS and obesity interact to amplify cardiovascular risk through shared pathways including inflammation, oxidative stress, and metabolic dysregulation.7,11 Therefore, comprehensive management of OSAS patients must include aggressive weight management strategies to mitigate overall cardiovascular risk.
Despite the strengths of our study, including a sizable sample and comprehensive analysis of bone metabolism and inflammatory markers, there are limitations that need to be noted. The study’s retrospective design might lead to selection bias, and causality cannot be established. The reliance on electronic medical records for data extraction may result in incomplete information or misclassification. Despite efforts to standardize blood collection in the morning, we cannot rule out residual circadian influence on inflammatory marker levels due to the retrospective design. Future prospective studies should incorporate strict time-controlled sampling. Additionally, we did not assess the impact of CPAP therapy or other treatments on the observed parameters, which could influence bone metabolism and inflammatory markers.
Furthermore, while we measured specific markers of bone metabolism and inflammation, the complex interactions within these systems mean that other unmeasured factors may contribute to cardiovascular risk. For instance, we did not evaluate oxidative stress markers, adipokines, or other cytokines that could provide additional insights. Future prospective research is necessary to validate our conclusions and explore the effects of therapeutic interventions on bone metabolism and inflammation in OSAS patients.
In conclusion, our study demonstrates that patients with obstructive sleep apnea syndrome exhibit significant alterations in bone metabolism markers and elevated levels of specific pro-inflammatory cytokines, which are associated with an increased risk of major adverse cardiovascular events. These findings indicate that bone metabolism dysregulation and systemic inflammation may be key mechanisms linking OSAS to cardiovascular morbidity. Incorporating assessments of bone health and inflammatory status in OSAS management may enhance risk stratification and guide targeted interventions to reduce cardiovascular risk. Future prospective studies with stricter BMI matching or longitudinal designs assessing weight change are warranted to further elucidate the complex interplay between obesity, OSAS, bone metabolism, and cardiovascular outcomes.
Data Sharing Statement
The datasets used during the present study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board and Research Ethics Committee of the Mindong Hospital Affiliated to Fujian Medical University, and was conducted in accordance to the tenets of the Declaration of Helsinki. As clinical data of patients, including basic demographic information, PSG parameters, were extracted from the hospital’s electronic medical record system, the requirement for the informed consent from patients was waived.
Funding
This work was supported by grants from the Natural Science Foundation of Fujian Province (2021J011451).
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Partinen M, Telakivi TJS. Epidemiology of obstructive sleep apnea syndrome. Sleep. 1992;15:S1–S4. doi:10.1093/sleep/15.suppl_6.s1
2. Mannarino MR, Di Filippo F, Pirro MJE. Obstructive Sleep Apnea Syndrome. 2012;23:586–593.
3. Gabbay IE, Lavie P. Age-and gender-related characteristics of obstructive sleep apnea. Sleep Breathing. 2012;16:453–460. doi:10.1007/s11325-011-0523-z
4. Lv R, Liu X, Zhang Y, et al. Pathophysiological mechanisms and therapeutic approaches in obstructive sleep apnea syndrome. Signal Transduct Target Ther. 2023;8:218. doi:10.1038/s41392-023-01496-3
5. Javaheri S, Javaheri S, Somers VK, et al. Interactions of obstructive sleep apnea with the pathophysiology of cardiovascular disease, part 1: JACC state-of-the-art review. J Am Coll Cardiol. 2024;84:1208–1223. doi:10.1016/j.jacc.2024.02.059
6. Yao X, Li N, Heizhati M, et al. Obstructive sleep apnea remains a risk factor for major adverse cardiovascular and cerebrovascular events even in hypertensive patients under treatment: the Urumqi Research on Sleep Apnea and Hypertension (UROSAH) data. Cardiovasc Diagn Ther. 2023;13:968–978. doi:10.21037/cdt-23-284
7. Sutanto A, Wungu CDK, Susilo H, Sutanto H. Reduction of Major Adverse Cardiovascular Events (MACE) after bariatric surgery in patients with obesity and cardiovascular diseases: a systematic review and meta-analysis. Nutrients. 2021;13:3568. doi:10.3390/nu13103568
8. Yeşildağ M, Şentürk Z, Bekci TT, Guney İ. The usefulness of new body indices in determining the risk of cardiovascular disease in cases with obstructive sleep apnea syndrome. Int J Gen Med. 2024;17:5523–5534. doi:10.2147/IJGM.S489904
9. Zhang Y, Hao W, Fan J, et al. Association between obstructive sleep apnea and cardiovascular events in acute coronary syndrome patients with or without revascularization - A prospective cohort study. Circ J. 2023;87:1369–1379. doi:10.1253/circj.CJ-23-0164
10. Yeghiazarians Y, Jneid H, Tietjens JR, et al. Obstructive sleep apnea and cardiovascular disease: a scientific statement from the American heart association. Circulation. 2021;144:e56–e67. doi:10.1161/CIR.0000000000000988
11. Lavalle S, Masiello E, Iannella G, et al. Unraveling the complexities of oxidative stress and inflammation biomarkers in obstructive sleep apnea syndrome: a comprehensive review. Life. 2024;14(4):425. doi:10.3390/life14040425
12. Yang C, Zhou Y, Liu H, Xu P. The role of inflammation in cognitive impairment of obstructive sleep apnea syndrome. Brain Sci. 2022;12(10):1303. doi:10.3390/brainsci12101303
13. Meliante PG, Zoccali F, Cascone F, et al. Molecular pathology, oxidative stress, and biomarkers in obstructive sleep apnea. Int J Mol Sci. 2023;24(6):5478. doi:10.3390/ijms24065478
14. Danilevicius C, Lopes J, RMRJBJoM P, Research B. Bone metabolism and vascular calcification. Braz J Med Biol Res. 2007;40(4):435–442. doi:10.1590/s0100-879x2007000400001
15. SIJJotCS M. Bone metabolism and the cardiometabolic syndrome: pathophysiologic insights. J Cardiometab Syndrome. 2006;1:53–57.
16. Xu J, Yu L, Liu F, Wan L, Deng Z. The effect of cytokines on osteoblasts and osteoclasts in bone remodeling in osteoporosis: a review. Front Immunol. 2023;14:1222129. doi:10.3389/fimmu.2023.1222129
17. Zhang Z, Wang D, Xu R, Li X, Wang Z, Zhang Y. The physiological functions and therapeutic potential of hypoxia-inducible factor-1α in vascular calcification. Biomolecules. 2024;14(12):1592. doi:10.3390/biom14121592
18. Chen Y, Zhao X, Wu H. Arterial stiffness: a focus on vascular calcification and its link to bone mineralization. Arterioscler Thromb Vasc Biol. 2020;40(5):1078–1093. doi:10.1161/ATVBAHA.120.313131
19. Teramoto S, Yamamoto H, Yamaguchi Y, Namba R, Ouchi YJC. Obstructive sleep apnea causes systemic inflammation and metabolic syndrome. Chest. 2005;127:1074–1075. doi:10.1378/chest.127.3.1074
20. Demer LL, Tintut YJA; thrombosis, and biology v. Inflammatory, metabolic, and genetic mechanisms of vascular calcification. Arteriosclerosis Thrombosis Vasc Biol. 2014;34:715–723. doi:10.1161/ATVBAHA.113.302070
21. Wang X, Fan J, Guo R, et al. Association of obstructive sleep apnoea with cardiovascular events in women and men with acute coronary syndrome. Eur Respir J. 2023;61(1):2201110. doi:10.1183/13993003.01110-2022
22. Wen W, Cai X, Zhu Q, et al. Linear relationship between hepatic steatosis index and major adverse cardiovascular events in hypertensive patients with obstructive sleep apnea: a real-world cohort study from China. Rev Cardiovasc Med. 2023;24:280. doi:10.31083/j.rcm2410280
23. Kapur VK, Auckley DH, Chowdhuri S, et al. Clinical practice guideline for diagnostic testing for adult obstructive sleep apnea: an American academy of sleep medicine clinical practice guideline. J Clin Sleep Med. 2017;13:479–504. doi:10.5664/jcsm.6506
24. He B, Al-Sherif M, Wu Y, et al. Apnoea-hypopnoea-index comparing the 2007 and 2012 American Academy of Sleep Medicine criteria in chronic obstructive pulmonary disease/obstructive sleep apnoea overlap syndrome. J Thorac Dis. 2020;12:S112–s119. doi:10.21037/jtd-cus-2020-008
25. Javaid SS, Obaid MA, Noor T, et al. Impact of continuous positive airway pressure on cardiovascular health in patients with obstructive sleep apnea: a systematic review and meta-analysis. Cardiol Rev. 2025. doi:10.1097/CRD.0000000000001004
26. Deng L, Jia R, Yang G, et al. Association of obstructive sleep apnea with bone metabolism in older adults: a hospital-based study. BMC Musculoskelet Disord. 2024;25:939. doi:10.1186/s12891-024-08070-0
27. Ali M, Ramadan A, Surani S. Obstructive sleep apnea-hypopnea syndrome immunological relationship. World J Clin Cases. 2024;12:6011–6014. doi:10.12998/wjcc.v12.i27.6011
28. Chen X, Zhen L, Ai H, et al. Prognostic implications of obstructive sleep apnea in patients with acute coronary syndrome stratified by homocysteine level: a prospective cohort study. Respir Res. 2023;24:313. doi:10.1186/s12931-023-02627-8
29. Gottlieb DJ. Sleep apnea and cardiovascular disease. Curr Diab Rep. 2021;21:64. doi:10.1007/s11892-021-01426-z
30. Zhao JM, Wang BY, Huang JF, Xie HS, Chen ML, Chen GP. Assessment of bone mineral density and bone metabolism in young men with obstructive sleep apnea: a cross-sectional study. BMC Musculoskelet Disord. 2022;23:682. doi:10.1186/s12891-022-05644-8
31. Xu F, Zhang X, Zhang Y, Chen W, Liao Z. Causal relationship of obstructive sleep apnea with bone mineral density and the role of BMI. Nat Sci Sleep. 2024;16:325–333. doi:10.2147/NSS.S443557
32. Bi H, He J, He X, et al. Bone marrow stem cells therapy alleviates vascular injury in a chronic obstructive pulmonary disease‑obstructive sleep apnea overlap syndrome rat model. Mol Med Rep. 2021;23:1.
33. Arnaud C, Bochaton T, Pépin JL, Belaidi E. Obstructive sleep apnoea and cardiovascular consequences: pathophysiological mechanisms. Arch Cardiovasc Dis. 2020;113:350–358. doi:10.1016/j.acvd.2020.01.003
34. Popadic V, Brajkovic M, Klasnja S, et al. Correlation of dyslipidemia and inflammation with obstructive sleep apnea severity. Front Pharmacol. 2022;13:897279. doi:10.3389/fphar.2022.897279
35. Locke BW, Lee JJ, Sundar KM. OSA and chronic respiratory disease: mechanisms and epidemiology. Int J Environ Res Public Health. 2022;19(9):5473. doi:10.3390/ijerph19095473
36. Sadaf S, Shameem M, Siddiqi SS, Anwar S, Mohd S. Effect of obstructive sleep apnea on bone mineral density. Turk Thorac J. 2021;22:301–310. doi:10.5152/TurkThoracJ.2021.20051
37. Liu X, Ma Y, Ouyang R, et al. The relationship between inflammation and neurocognitive dysfunction in obstructive sleep apnea syndrome. J Neuroinflamm. 2020;17:229. doi:10.1186/s12974-020-01905-2
38. Sánchez-de-la-Torre M, Gracia-Lavedan E, Benitez ID, et al. Adherence to CPAP treatment and the risk of recurrent cardiovascular events: a meta-analysis. JAMA. 2023;330:1255–1265. doi:10.1001/jama.2023.17465
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.