Back to Journals » Clinical, Cosmetic and Investigational Dentistry » Volume 16
The Correlation Between Odontogenic Infection and Total Spectrum of Dental Caries with Oral Health Related Quality of Life in Children with Intellectual Disabilities
Authors Sabila A ![]() , Riyanti E
, Riyanti E ![]() , Indriyanti R, Tjahajawati S, Rikmasari R, Rakhmatia YD
, Indriyanti R, Tjahajawati S, Rikmasari R, Rakhmatia YD ![]()
Received 8 July 2024
Accepted for publication 23 October 2024
Published 30 October 2024 Volume 2024:16 Pages 431—439
DOI https://doi.org/10.2147/CCIDE.S486015
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Christopher E. Okunseri
Afina Sabila,1 Eriska Riyanti,1 Ratna Indriyanti,1 Sri Tjahajawati,2 Rasmi Rikmasari,3 Yunia Dwi Rakhmatia3
1Paediatric Dentistry Department, Faculty of Dentistry, Universitas Padjadjaran, Bandung, West Java, Indonesia; 2Oral Biology Department, Faculty of Dentistry, Universitas Padjadjaran, Bandung, West Java, Indonesia; 3Prosthodontic Department, Faculty of Dentistry, Universitas Padjadjaran, Bandung, West Java, Indonesia
Correspondence: Eriska Riyanti, Paediatric Dentistry Department, Faculty of Dentistry, Universitas Padjadjaran, Jl. Sekeloa Selatan No. 1, Lebakgede, Kecamatan Coblong, Bandung, West Java, 40132, Indonesia, Tel/Fax +62 22 2533031, Email [email protected]
Objective: : Children with Intellectual Disabilities (ID) have a higher rate of untreated caries and often progress to caries with pulpal involvement or odontogenic infections. This can be assessed using the Caries Assessment Spectrum and Treatment (CAST) index and the Pulp Ulcer Fistula Abscess (PUFA) index. Dental problems often have an impact on quality of life, so Oral Health-Related Quality of Life (OHRQoL) assessment is needed for ID children.
Purpose: To identify and analyze the correlation between odontogenic infection, the total spectrum of caries, and OHRQoL in ID children.
Methods: : The subjects of the research were 70 ID children who attended Special Needs Schools (SNS) Type D of the Foundation for the Development of Disabled Children (FDDC). This research uses an analytical survey using questionnaires and interviews to assess OHRQoL. The sampling technique, namely Total Sampling, obtained 43 ID child subjects who met the inclusion criteria. The data were tested statistically using the Spearman Correlation non-parametric test and the t-test.
Results: : The average value of odontogenic infection in the population was 1.79, including in the poor category, and the total spectrum of dental caries was 51.16%, including severe morbidity. Multivariate analysis showed a significant correlation between odontogenic infection, total spectrum of caries, and OHRQoL; odontogenic infection with total dental caries spectrum was significantly associated with each p-value = 0.0000, while the correlation between OHRQoL and both odontogenic infection and total caries spectrum had p-values > 0.05, respectively, so it is considered not significant.
Conclusion: : Odontogenic infection in ID children is a poor category. The total spectrum of dental caries in ID children mostly includes severe morbidity. There is a correlation between odontogenic infections, the total spectrum of dental caries, and OHRQoL, as well as between odontogenic infections and the total spectrum of dental caries.
Keywords: odontogenic infection, dental caries, oral health related quality of life, intellectual disabilities
Introduction
Children with intellectual disabilities (ID) have a significant impairment in an individual’s cognitive abilities, carrying out daily routines, and interacting with other people. These disorders can be seen during their developmental phase. An individual may have ID alone or may present with congenital malformations, neurological features, and/or differences in developmental behavior.1
Nearly 3% of the world’s population has some form of ID,2,3 including mild (85%), moderate (10%), severe (4%), and profound (2%), the mortality rate is higher in profound than other forms.2 The prevalence of ID in Indonesia is in the range of 1–3% in a population. The true incidence of ID is difficult to quantify because mild ID is sometimes not recognized until middle childhood. The highest incidence is in school-age children, with a peak age of 6–12 years.4
Children with ID are usually able to participate in education and be independent, but they cannot exercise full independence as adults, including maintaining oral hygiene.5 Children with ID tend to have a higher prevalence of poor oral hygiene, gingivitis, malocclusion, and untreated caries. This can occur due to a high carbohydrate intake and drugs that encourage the development of caries and periodontal disease.3,5–7
They also tend to have more missing teeth, untreated caries, and tooth extractions than restorations,1 so an index is needed that can measure various advanced stages of caries lesions, such as the Pulp Ulcer Fistula Abscess (PUFA) index,8 and the Caries Assessment Spectrum and Treatment (CAST) index.9 The PUFA index records the consequences of untreated carious lesions and focuses on the most severe stage of caries,9 which may represent an assessment of odontogenic infection.8
The CAST index is an index that measures early-stage caries lesions up to more severe stages.9 The CAST index is an instrument that was developed and can assess the total spectrum of dental caries, from healthy tooth surfaces to teeth with abscesses and even tooth loss. The instrument was validated for appearance, content, and concept. Its reproducibility in clinical studies has been tested in pediatric and adult populations.10–12
Oral health also has a significant impact on a person’s psychological health, resulting in reduced nutritional intake, impaired social interactions, difficulty carrying out daily activities, and anxiety related to these things.13–15 In a study by Davila et al3 dental problems are one of the ten main causes that can limit the activities of children with ID.3
In addition to assessing the status, clinical signs, and symptoms of oral health, a better idea emerged to obtain subjective points related to oral health. Quality of life indicators related to oral health, or Oral Health-Related Quality of Life (OHRQoL). The Oral Health Impact Profile-14 questionnaire (OHIP-14), composed of 7 dimensions with 2 questions each, has been widely used in several countries to assess an individual’s OHRQoL.15
Studies show that poor oral health status, such as advanced caries with pulp involvement and odontogenic infections in people with disabilities, can have a negative impact on their quality of life and that of their families.16 Assessment of oral health care needs, and in particular the impact of oral health on the quality of life of children with ID who have been neglected.15 Therefore, the authors expected, that we could understand the oral health condition of ID children and the associated risk factors involved can contribute in the future and can positively influence their life expectancy, and there is no research on how oral health with more advanced caries can impact the quality of life of ID children, which can affect their quality of life. This made the authors interested in investigate the correlation between odontogenic infections and the total spectrum of dental caries with OHRQoL in ID children.
Methods
Study Design and Participants
This type of research is analytical research with a survey method using questionnaires and interviews, which aims to determine the correlation between variables in a situation or group of subjects without treatment. The analytical research aims to determine the correlation between odontogenic infections and the total spectrum of dental caries with OHRQoL in ID children.
The subjects in this research were 70 ID children who attended Special Needs Schools (SNS) Type D of the Foundation for the Development of Disabled Children (FDDC). The sampling technique was carried out using Total Sampling. The inclusion criteria in this study were ID children who have or are currently experiencing caries and odontogenic infections, chronologically aged 6 to 18 years, and parents or caregivers of ID children who are willing to fill out informed consent to take part in the research. The exclusion criteria were ID children who were uncooperative in being examined, caregivers who did not completely answer the questionnaire, and children who did not attend school.
Data Collection and Measurements
At the implementation stage, research information sheets and informed consent forms were given to parents/caregivers. After that, dental health education was carried out for children and their caregivers, and then the researcher accompanied ID children to toothbrushing and continued with dental examinations using the PUFA index and CAST index. Researchers conducted interviews with closed questionnaires using OHIP-14 to assess the OHRQoL of ID children with their caregivers (proxy), which had been tested for validity and reliability by Suwargiani A, et al.17
Statistical Analysis
Odontogenic infection examination was assessed using the subject’s PUFA index. The PUFA/pufa score per individual is calculated cumulatively and represents the number of teeth that meet the PUFA/pufa diagnostic criteria. PUFA for permanent teeth and pufa for primary teeth are reported separately.8,18 The PUFA⁄pufa experience for a population is calculated as an average and thus has a decimal value. PUFA counting codes are tabulated in a frequency table: P: Pulp Involvement, U: Ulceration, F: Fistula, and A: Abscess. The results of calculating the PUFA index for both individual PUFA and population PUFA are categorized as follows: PUFA index 0 = good, and PUFA index >0 = bad.18
The prevalence of PUFA⁄pufa was calculated as the percentage of the population with a PUFA⁄pufa score of one or more. The “Untreated Caries, PUFA Ratio” was calculated as follows:19
The calculation of the PUFA/pufa index is by dividing the amount of PUFA/pufa by the number of teeth with active caries and multiplying the result obtained by 100.11,19 The final criteria for the PUFA index in this study were good, fair, and poor.
A more detailed caries detection instrument that assesses not only cavities in the dentin but also looks for restorations or cavities with pulp involvement or that have developed into an abscess or fistula was carried out by examining the total spectrum of dental caries by assessing the CAST index in each subject. The characteristics and codes of the CAST index assessment are as follows, Sound (0) : no visible evidence of distinct carious lesion is present; Sealant (1): Pits and/or fissures are at least partially covered with sealant material; Restoration (2): A cavity is restored with an direct or indirect restorative material; Enamel (3): Distinct visual change in enamel only, a clear caries related discolouration is visible, with or without localized enamel breakdown; Dentine (4): Internal caries-related discolouration in dentine is visible through the enamel; Pulp (5): Distinct cavitation into dentine and the pulp chamber is intact; Pulp (6): Involvement of the pulp chamber, cavitation reaching the pulp chamber or only root fragment are present; Abscess/Fistula (7): A pus containing swelling or a pus releasing sinus tract to a tooth with pulp involvement; Lost (8): The tooth has been removed because of dental caries; Other (9): Does not match with any of the other descriptions.12
The maximum CAST score per subject allows individuals to be grouped based on disease severity, so that subjects with maximum scores of 0, 1, and 2 are classified as healthy; those showing a maximum CAST score of 3 were classified as in the premorbidity stage; and individuals with maximum CAST scores of 4 and 5 were classified as in the morbidity stage. The severe morbidity classification contained subjects with a maximum CAST score of 6 or 7, and mortality was characterized by subjects with a maximum CAST score of 8.12
Research for OHRQoL was carried out using a survey analytical method in the form of data collection through a questionnaire form answered by caregivers who have ID children (proxy). The questionnaire used is a modified version of the OHIP-49 questionnaire, which has been validated for the population studied, called OHIP-14. The questionnaire is used to assess OHRQoL and consists of 14 questions with 7 dimensions (Functional limitations, Physical pain, Psychological discomfort, Physical disability, Psychological disability, Social disability, and Handicap). Each dimension has 2 questions. Each question is rated on a 5-point Likert scale. The total possible score ranges from 0 to 56, with higher scores indicating a poorer quality of life.15
Sociodemographic data was also collected, which included the gender and age of the child, place of residence, highest level of education, and parents income. The OHRQoL score criteria are classified into three categories: less impact, moderate impact, and very impact.20 Higher scores indicate greater oral health impact and lower or poor OHRQoL.21
The non-parametric Spearman Correlation Test is a statistical analysis to see the correlation between OHRQoL in ID children and the total spectrum of dental caries and odontogenic infections. It can be calculated using the Spearman rank correlation coefficient. The t-test was used to test the significance of the correlation by looking at the differences in the correlation between odontogenic infection and the total spectrum of dental caries with the OHRQoL of ID children.
Ethics Statement
This study underwent review and approval by The Research Ethics Committee, University of Padjadjaran, Indonesia (No. 583/UN6.KEP/EC/2023), and has complied with the Declaration of Helsinki.
Results
General Characteristics of Research Respondents
The research was conducted on ID children and caregivers at SNS Type D of FDDC Bandung in May 2023. The subjects obtained consisted of 43 ID children whose parents met the inclusion criteria of the 70 ID children registered at the school. Based on the age of the ID children studied, they were generally in the age range of 11–18 years (79.06%), consisting of 37.21% girls and 62.79% boys.
According to the descriptive data of caregiver respondents in this study based on gender, 72.09% were women and 27.91% were men, with an age range of 26 to 65 years, and the age of respondents was generally 41–50 years (41.86%). The highest level of education among parent respondents was among high school graduates (44.19%). The parents occupation shows that they are generally housewives (46.51%), comparable to working parents (46.51%), and the rest are retirees (6.98%). The highest level of monthly income for parents (62.79%) is in the range of IDR 2,500,000–IDR 5,000,000; while income above IDR 5,000,000/month is 30.23%.
Frequency Distribution of Odontogenic Infections and Total Spectrum of Dental Caries
The component values of the PUFA/pufa index from 43 research subjects found a total of 77 teeth, including odontogenic infections, as shown in Table 1. The most frequently found was pulp exponation (P) (90.91%), which consisted of 33.77% of adult teeth and 57.14% of primary teeth. As many as 9.09% were found to have abscesses (A), both in adult teeth (3.90%) and primary teeth (5.19%), and the average value of the population where infection occurred Odontogenicity in ID children in this study was 1.79, which is included in the poor category. This is likely because the age that is generally examined is 11–18 years old, and the possibility of visible teeth is the remaining roots of primary teeth that have not been removed, so that most are included in the criteria for pulp involvement in the PUFA index but do not cause ulceration and fistula. The examination also found an abscess, which as an infection looks swollen and contains pus in the gums, but no fistula was found. Figure 1 shows the number of individuals included in the odontogenic infection category based on the ratio of odontogenic infection to existing dental caries, generally included in the good category (60.47%), followed by the fair category (27.91%) and the poor category (11.63%).
 |
Table 1 Frequency Distribution of Odontogenic Infections Assessed by the PUFA Index |
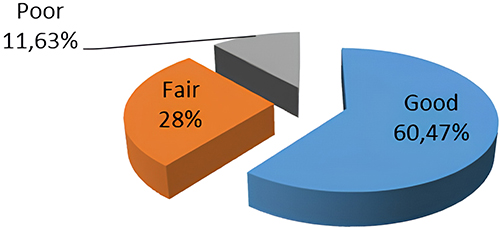 |
Figure 1 Description of Odontogenic Infection in Children with Intellectual Disabilities in SNS Part D FDDC Bandung, West Java, Indonesia. |
The characteristics of ID children based on the total spectrum of dental caries were assessed using the CAST index. Table 2 shows that 51.16% are in the severe morbidity category, followed by premorbidity (20.93%), the healthy category (13.95%), and finally morbidity (6.98%), mortality (4.65%), and others (2.33%).
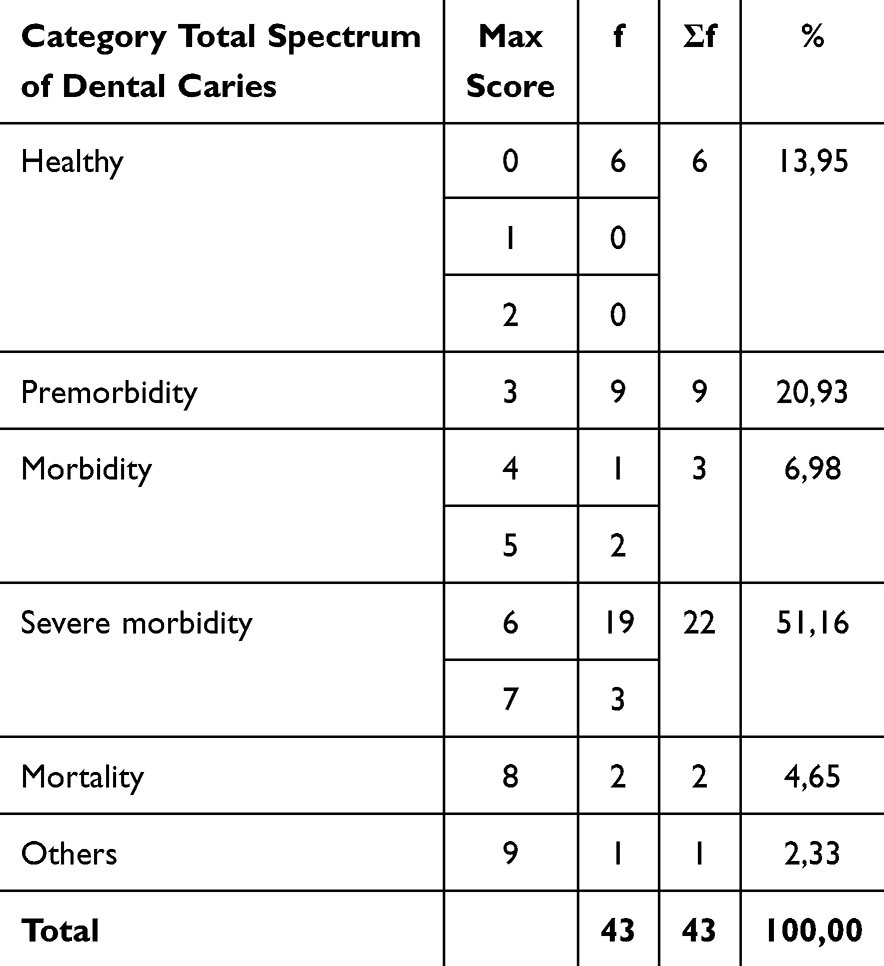 |
Table 2 Frequency Distribution of the Total Spectrum of Dental Caries in ID Children |
Assessment of OHRQoL in ID Children Using OHIP-14
The results of interviews with parents who have children with ID based on responses from the OHIP-14 questionnaire are shown in Table 3. The results of the dimension that most influences children’s quality of life related to oral health are the “Psychological Discomfort” dimension (35.47%), followed by the “Physical Pain” dimension (32.85%), but the dimension that was least affected was the “Psychological disability” dimension (20.93%). The overall percentage assessment of OHRQoL in ID children is 27.41%, which is in the low impact category.
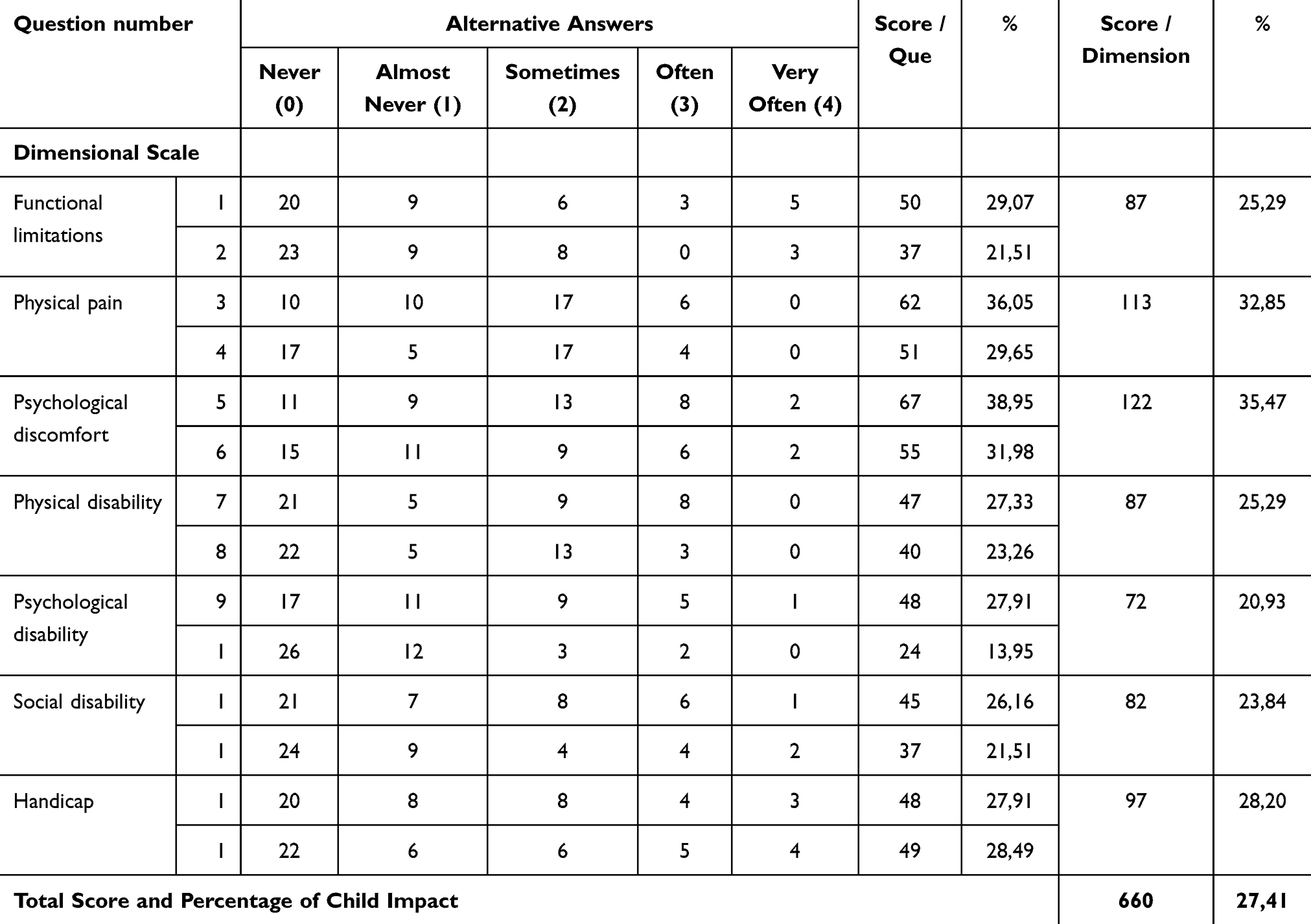 |
Table 3 Responses of Caregivers with ID Children to the OHIP-14 Survey |
Correlation Between Variables
The multivariate correlation between OHRQoL with odontogenic infections and the total spectrum of dental caries is shown in Table 4 using Kendall’s Concordal correlation, statistically showing a value of W = 0.603 which is statistically significant with a p-value = 0.0000 <0.05. This means that there is a correlation between these three variables.
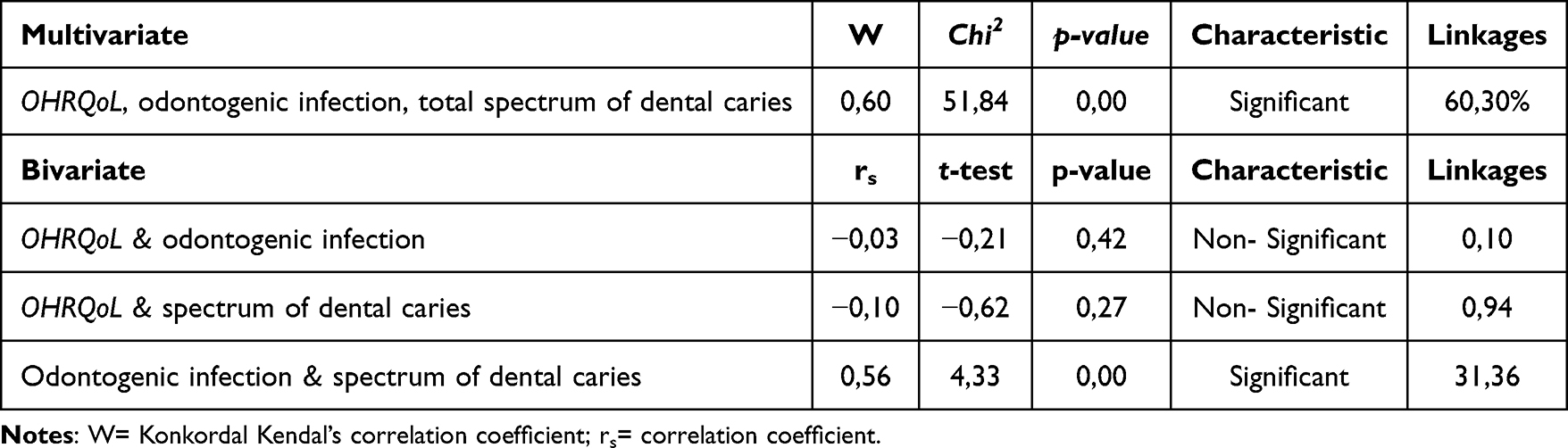 |
Table 4 Correlation Between OHRQoL with Odontogenic Infections and Total Spectrum of Dental Caries in ID Children |
The bivariate correlation between OHRQoL, odontogenic infection, and the total spectrum of dental caries was calculated using Spearman rank correlation analysis, which is shown in Table 4. The results of this test showed a strong correlation between odontogenic infection and the total spectrum of dental caries, which was statistically significant with a p-value < 0.05. The correlation between OHRQoL with odontogenic infections and the total spectrum of dental caries provides a weak correlation value and is not significant; statistically, the p-value for both is >0.05.
Discussion
Based on the characteristics of ID child respondents in this study, based on age, they were generally 11–18 years old (79.06%), while based on gender, it was generally more boys (62.79%) than girls (37.21%). This is almost similar to research by Ayoglu and Kiran,22 who found that the prevalence of individual with ID in Turkey is more common in men (61.9%) compared to women (38.2%).22
The average odontogenic infection in the population of ID children in this study was assessed as “bad”. However, the assessment of the number of individuals experiencing odontogenic infections was highest in the “good” category (60.47%), followed by the “fair” category (27.91%) and “not good” (11.63%). Research by Tefera, Girma, et al states that maternal education, frequency of consuming sweet foods, and type of disability are statistically significant factors related to oral hygiene status.23
The results of the assessment of the total spectrum of dental caries show that, generally, ID children suffer from severe morbidity (51.16%). This can occur due to a lack of information sources and self-awareness from caregivers with inadequate education to maintain dental and oral health in ID children, as stated by Nunes, 24 that those with lower education often pay less attention to the impact of oral cavity conditions on their children’s lives and lack access to dental care24 causing caries in their children to tend to go untreated and cause caries involving the pulp.
Table 3 shows the results of caregiver responses regarding the quality of life of ID children related to dental and oral health using the OHIP-14 questionnaire. The dimensions “psychological discomfort” (35.47%) and “physical pain” (32.85%) are the most affected in this study, followed by “handicap”, “functional limitations”, “physical disability”, “social disability”, and “psychological disability”, which are the least affected by the dental and oral health of children with ID. The results of interviews with most of the parents in this study stated that although their children often or sometimes complained of pain in their teeth and mouth, psychologically and socially, most of the children did not feel affected by the pain, so they continued to socialize or play with their friends. Almost similar to the results of this study, research by Couto et al15 and Nuttall et al25 shows that the two dimensions that are greatly affected by dental and oral health are “physical pain”, followed by “psychological discomfort”.15,25
In study by Pani et al,26 he found that parental age and education level were associated with greater negative perceptions of the impact of oral health on children’s quality of life [24, 26]. Research by Aggarwal et al,27 stated that the perception of children’s dental and oral health can also be influenced by the family’s socio-economic status.24,27
The conclusions of the OHRQoL categories in ID children are shown in Table 3, which generally includes the less impact category (67.44%) followed by the moderate impact category (32.56%). Study by Tefera et al,23 states that children with special needs do not have significant differences in OHRQoL as assessed by gender, age group, and dental caries.23
Table 4 shows the multivariate analysis regarding the correlation between OHRQoL with odontogenic infections and the total spectrum of dental caries in ID children, showing the Kendall Concordal correlation value; W = 0.603, with a p-value <0.05 indicates that there is a significant correlation between these three variables.
In research by Praveen in India,8 in the general population in the city of Rangareddy, he stated that there was a positive correlation between OHRQoL as assessed by OHIP and untreated caries as assessed by the PUFA index among the study population. As untreated caries increases, it has a detrimental effect on an individual.8
Bivariate correlation test was carried out as shown in Table 4, between odontogenic infections assessed by the PUFA index and OHRQoL in ID children, showing the results of the non-parametric Spearman correlation test with a weak correlation value and not statistically significant. This is similar to the correlation between OHRQoL and the total spectrum of dental caries, with a p-value of >0.05, while the correlation between odontogenic infection and the total spectrum of dental caries has a strong correlation, with a p-value <0.05, which is significant.
The results of the study by Carrada, et al28 highlight the importance of preventing and treating oral cavity conditions. Dental caries can cause pain, discomfort, and decreased well-being for ID children, which can affect the emotions and activities of their family members. As treatment improves the oral and dental health of ID children, can improve their quality of life and have a positive impact on their families.28
This study has several limitations, such as not carrying out further analysis of the impact of socio-demographic variables on the OHRQoL of ID children. This research relies on parents’ perceptions to assess their children’s OHRQoL. However, parent’s knowledge about their children’s activities and feelings is limited, so they cannot assess the OHRQoL of ID children with one hundred percent accuracy.
Conclusion
Odontogenic infection in ID children is a poor category. The total spectrum of dental caries in ID children mostly includes severe morbidity and the average total spectrum of caries in ID children is included in the diseased population because most subjects had at least one tooth in the stage of severe morbidity. There is a correlation between odontogenic infections, total caries spectrum, and OHRQoL in ID children, as well as odontogenic infections and total caries spectrum. Meanwhile, the correlation between OHRQoL and odontogenic infections, as well as OHRQoL and the total caries spectrum in ID children, is considered less significant.
Acknowledgments
We would like to acknowledge Universitas Padjadjaran for financial and technical support during the study. In addition, thank to Special Needs Schools (SNS) Type D of the Foundation for the Development of Disabled Children (FDDC), Bandung City, West Java, Indonesia for their organizational and logistical support from the first day of this study until the end.
Funding
This study was supported by Academic Leadership Grant (ALG) 2023, grant number (2203/UN.6.3.1/PT.00/2022), Universitas Padjadjaran, Bandung, West Java, Indonesia.
Disclosure
The authors have no conflicts of interest associated with the material presented in this paper.
References
1. Abdullah MAH, Sa’idah IN, Knights J, Dhaliwal SKS, Ming LC, Dhaliwal JS. Oral hygiene practices among adults with intellectual disabilities—a pilot study. Dent J. 2022;10(8):1–9. doi:10.3390/dj10080155
2. Nirmala S, Saikrishna D, Nuvvula S. Dental concerns of children with intellectual disability - A narrative review. Dent Oral Craniofacial Res. 2018;4(5):1–5. doi:10.15761/DOCR.1000266
3. Chavez MCM. Alternatives of management of patients with intellectual disability in the dental consultation dental management of intellectual disability. South Asian Res J Oral Dent Sci. 2020;2(4):32–37.
4. Maidartati SH, Aliyah R. Description of self-esteem for mothers who have mentally retarded children aged 7-12 years. J Keperawatan BSI. 2018;2018(6):151–157.
5. Dean JA. McDonald and Avery’s Dentistry for the Child and Adolescent.
6. Morais I, Rodrigues JT, Peixoto C, Sousa I, Mesquita E, Morais A. Ambulatory dental procedures in children with intellectual disability: a ten-year review. Ambul Surg. 2019;25(4):110–113.
7. Anders PL, Davis EL. Oral health of patients with intellectual disabilities: a systematic review. Spec Care Dent. 2010;30(3):110–117. doi:10.1111/j.1754-4505.2010.00136.x
8. Praveen BH, Prathibha B, Parthasarthi Reddy P, Monica M, Samba A, Rajesh R. Co relation between PUFA index and oral health related quality of life of a rural population in India: a cross-sectional study. J Clin Diagn Res. 2015;9(1):39–42.
9. Young DA, Nový BB, Zeller GG, et al. The American Dental Association caries classification system for clinical practice: a report of the American Dental Association council on scientific affairs. J Am Dent Assoc. 2014;146(2):79–86. doi:10.1016/j.adaj.2014.11.018
10. De Souza AL, Bronkhorst EM, Creugers NHJ, Leal SC, Frencken JE. The caries assessment spectrum and treatment (cast) instrument: its reproducibility in clinical studies. Int Dent J. 2014;64(4):187–194. doi:10.1111/idj.12104
11. Bagińska J. Evaluation of the status of primary dentition in 6–7-year-old children from Bialystok District using the mean dmf and the index of clinical consequences of untreated caries (pufa). TDent Med probl. 2013;50(2):160–165.
12. Leal SC, Ribeiro APD, Frencken JE. Caries assessment spectrum and treatment (CAST): a novel epidemiological instrument. Caries Res. 2017;51(5):500–506. doi:10.1159/000479042
13. Alamri H. Oral care for children with special healthcare needs in dentistry: a literature review. J Clin Med. 2022;11(19):5557. doi:10.3390/jcm11195557
14. AlJameel AH. Oral health-related quality of life outcomes for individuals with disabilities: a review. J Clin Diagn Res. 2020;2020(11):1–5.
15. Couto P, Pereira A, Nunes M, Mendes RA. Oral health-related quality of life of Portuguese adults with mild intellectual disabilities. PLoS One. 2018;13(3):1–14. doi:10.1371/journal.pone.0193953
16. de Almeida JS, Fernandes RF, Andrade ÁCB, et al. Impact of dental treatment on the oral health-related quality of life of children and adolescents with autism spectrum disorder. Spec Care Dent. 2021;41(6):658–669. doi:10.1111/scd.12618
17. Suwargiani AA, Pribadi IMS, Hidayat W, Yasrin TA. Validation and reliability of Oral Health Impact Profile-14 questionnaire among pregnant woman. Padjadjaran J Dent. 2016;28(2):126–129. doi:10.24198/pjd.vol28no2.13725
18. Raynuary N, Suwargiani AA, Suryanti N. PUFA index of pregnant women who came to the puter community health centre, Bandung, Indonesia. J Kedokt Gigi Univ Padjadjaran. 2017;29(2):99–105.
19. Monse B, Heinrich-Weltzien R, Benzian H, Holmgren C, Van Palenstein Helderman W. PUFA - An index of clinical consequences of untreated dental caries. Oral Epidemiol. 2010;38(1):77–82. doi:10.1111/j.1600-0528.2009.00514.x
20. Elfarisi RN, Susilawati S, Suwargiani AA. Dental and oral health research report regarding the quality of life of children aged 4-5 years in Cilayung Village. J Ked Gi Unpad. 2018;30(2):85–94. doi:10.24198/jkg.v30i3.18509
21. Du King RY, Yiu CKY, King NM. Health ‑ and oral health ‑ related quality of life among preschool children with autism spectrum disorders. Eur Arch Paediatr Dent. 2019;2019:1–7.
22. Ayoglu FN, Cabuk F, Kiran S, Ocakci A, Sahin Z, Dursun A. The prevalence of mental retardation by gender, age of diagnosis and location in Zonguldak province, Turkey. Neurosciences. 2008;13(1):57–60.
23. Tefera AT, Girma B, Adane A, Muche A, Ayele TA. Oral health-related quality of life and oral hygiene status among special need school students in amhara region, Ethiopia. BMC Heal Qual Life Outcomes. 2023;4(21):1–11.
24. de S. Nunes F, Fernandez MDS, Viana VDS, et al.. Factors associated with the oral health-related quality of life in children with intellectual disabilities. Odovtos - Int J Dent Sci. 2020;(8):432–446. doi:10.15517/ijds.2020.43309
25. Nuttall NM, Steele JG, Pine CM, White D, Pitts NB. The impact of oral health on people in the UK in 1998. Br Dent J. 2001;190(3):121–126 . doi:10.1038/sj.bdj.4800901a
26. Pani SC, Mubaraki SA, Ahmed YT, Alturki RY, Almahfouz SF. Parental perceptions of the oral health-related quality of life of autistic children in Saudi Arabia. Spec Care Dent. 2013;33(1):8–12. doi:10.1111/j.1754-4505.2012.00294.x
27. Aggarwal VP, L. DC, Batra M. Impact of sociodemographic attributes and dental caries on quality of life of intellectual disabled children using ECOHIS. Int J Health Sci. 2016;10(4):463–472.
28. Carrada CF, Scalioni FAR, Abreu LG, Ribeiro RA, Paiva SM. Impact of oral conditions of children/adolescents with down syndrome on their families’ quality of life. Spec Care Dent. 2020;40(2):175–183. doi:10.1111/scd.12444
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.