Back to Journals » OncoTargets and Therapy » Volume 12
The contribution of ABCG2 G34A and C421A polymorphisms to multiple myeloma susceptibility
Authors Niebudek K, Balcerczak E, Mirowski M ![]() , Pietrzak J
, Pietrzak J ![]() , Zawadzka I, Żebrowska-Nawrocka M
, Zawadzka I, Żebrowska-Nawrocka M ![]()
Received 19 November 2018
Accepted for publication 17 January 2019
Published 27 February 2019 Volume 2019:12 Pages 1655—1660
DOI https://doi.org/10.2147/OTT.S195245
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Leo Jen-Liang Su
Katarzyna Niebudek, Ewa Balcerczak, Marek Mirowski, Jacek Pietrzak, Izabela Zawadzka, Marta Żebrowska-Nawrocka
Laboratory of Molecular Diagnostics and Pharmacogenomics, Department of Pharmaceutical Biochemistry and Molecular Diagnostics, Interfaculty Cathedral of Laboratory and Molecular Diagnostics, Medical University of Lodz, Lodz 90-151, Poland
Background: Breast cancer resistance protein BCRP, belonging to superfamily G of the adenosine triphosphate-binding cassette (ABC) transporters, is an efflux pump and plays a critical role in protecting cells against xenobiotics and toxic compounds including (pro)carcinogens. BCRP is expressed in many tissues, including hematopoietic stem cells. Genetic variants such as single nucleotide polymorphisms (SNPs) can change the gene expression and/or reduce their products’ activity which may affect an individual’s susceptibility to xenobiotics and the development of carcinoma. These changes may affect the exposure of blood cells to toxic compounds, which increases the risk of multiple myeloma. The aim of this study was to determine polymorphisms at positions G34A and C421A of the ABCG2 gene in multiple myeloma in the Polish population for the first time.
Materials and methods: Material for the study included DNA isolated from nucleus of cells of peripheral blood of patients diagnosed with multiple myeloma (investigated group N=181) and from healthy people (control group N=97). Research into the polymorphisms was conducted using the polymerase chain reaction-restriction fragment length polymorphism technique.
Results: The present study showed a statistically significant association between SNP C421A of the ABCG2 gene and the risk of developing multiple myeloma (P=0.0218). No statistically significant relationship was found for the other parameters analyzed, such as age, gender, or type of secreted immunoglobulin.
Conclusion: Preliminary studies indicate that SNP C421A may become a potential predictor for the development of multiple myeloma.
Keywords: BCRP, polymorphism, ABCG2, multiple myeloma risk, plasma cell myeloma, single nucleotide polymorphism
Introduction
The ABCG2 gene located on chromosome 4q22 encodes the 655-amino-acid breast cancer resistance protein BCRP.1 Like other G-subfamily proteins of adenosine triphosphate-binding cassette (ABC) transporters, BCRP is a half transporter containing one nucleotide-binding domain and one transmembrane domain fused into a single polypeptide chain. BCRP has a functional form as a homodimer with a molecular mass of 144 kDa.2 In humans, BCRP functions as a protective pump. Physiologically, it occurs in many normal human tissues including the placenta, liver, brain, syncytiotrophoblast, small intestine, and breast tissue.3 This protein determines the existence of barriers: the brain, the testicles, and the placenta.4 BCRP is suggested to provide the fundamental physiological barrier function that can protect cells. High expression of BCRP affects tissues of organs responsible for detoxification processes.5 BCRP is one of the major proteins responsible for the active transport of a broad spectrum of chemical compounds across extracellular and intracellular membranes, for example: heme, porphyrin, riboflavin, hormones (estrogens), and chemotherapeutics (methotrexate, imatinib, doxorubicin, topotecan).6,7 Among the substrates for BCRP there are also carcinogenic xenobiotics. The BCRP transporter, by regulating the concentration of xenobiotics in the cell, fulfills the physiological protective role for the cell against toxicity of environmentally or clinically administered drugs.5 BCRP plays also an important protective role for hematopoietic stem cells against xenobiotics and hypoxia.3,8,9
The genetic background significantly determines the kinetic properties of BCRP, starting from the single nucleotide polymorphism (SNP) to large chromosome aberrations that change protein properties and functions leading to an increased risk of cancer.3,10
SNPs are the most frequent inherited sequence variations in a particular gene and occur every 100–300 bp.11 The ABCG2 gene protein was tested for SNPs in 90 different ethnic populations. Within the ABCG2 gene, more than 40 nonsynonymous and synonymous SNPs in promoter regions, exons, and intron sequences have been identified.12,13
The two most common SNPs are G34A and C421A. The G34A polymorphism in exon 2 (rs2231137) results in an amino acid change in position 12 from valine to methionine (Val12Met). This results in the formation of a protein with a significantly reduced ability to translocate the substance across the cell membrane. The C421A polymorphism in exon 5 (rs2231142) which leads to a glutamine-to-lysine amino acid substitution is associated with low levels of BCRP expression.2,10,14
Loss of the physiological function of BCRP resulting from SNPs G34A and C421A in ABCG2 gene variants may affect susceptibility to cancer development such as acute myeloid leukemia (AML), chronic myelogenous leukemia (CML), diffuse large B-cell lymphoma, breast cancer, prostate cancer, colorectal cancer, nonpapillary renal cell cancer, pancreatic cancer, and non-small-cell lung carcinoma. Therefore, several studies have tried to identify the role of SNPs with susceptibility, survival, and treatment outcomes of carcinoma.15,16
Multiple myeloma is a cancerous disease derived from a single clone of cancer cells from the bone marrow. Multiple myeloma belongs to the group of malignant monoclonal gammapathies.3 The incidence in Europe ranges between 4.5 and 5.8/100,000. In epidemiological studies in Poland carried out since the 1990s, there has been a steady increase in multiple myeloma incidence. Multiple myeloma represents 1% of all malignancies and up to 14% of hematological malignancies. The disease is slightly more common in men. The pathogenesis of multiple myeloma is not yet fully known. However, it is assumed to be a multifactorial disease where environmental, genetic, and long-term antigenic stimulation of the immune system in the course of bacterial and viral infections interact. The risk of first-degree multiple myeloma is 3–7 times higher in kinship relatives, which supports the concept of involvement of genetic factors in the development of the disease.
Therefore, it is reasonable to assume that the genetic variants of the ABCG2 gene can cause altered exposure of hematopoietic cells to xenobiotics and thereby reduce or increase the risk of multiple myeloma development.3
The aim of this study was to determine the potential significance of SNPs G34A and C421A of the ABCG2 gene in the development of multiple myeloma. To the best of our knowledge, the role of this polymorphism in multiple myeloma has not so far been studied in the Polish population.
Materials and methods
Materials
Blood samples (N=181) were collected from patients (85 females, 96 males; median age of group: 63 years) with multiple myeloma diagnosed at the Clinic of Hematology, Medical University of Lodz, Poland. The control group consisted of 97 blood samples obtained from healthy individuals (58 females, 39 males, median age of group: 33 years) from the local blood bank, and geographically and ethnically matched the group of patients with multiple myeloma. The investigation was performed in accordance with the principles of the Declaration of Helsinki and was approved by the Ethical Committee of the Medical University of Lodz (No RNN/88/16/KE and RNN/285/13/KE). All patients provided a written informed consent before their inclusion in the study.
DNA isolation
DNA was isolated from peripheral blood according to the “Blood Mini” protocol (A&A Biotechnology, Gdynia, Poland). DNA samples were stored at −20°C until analysis.
Genotyping of G34A and C421A
Polymerase chain reaction
Polymerase chain reaction (PCR) for both investigated polymorphisms was performed according to the 2×PCR Super Master Mix (Biotools, Jupiter, FL, USA) protocol. The mixture for PCR reaction consisted of: 5 μL of 2×PCR Super Master Mix (which included in its composition: buffer, MgCl2, dNTPs, Taq DNA polymerase); 0.5 mM of each primer, specific to the particular SNP; 50 ng of DNA template; and distilled water up to 20 μL. Negative control was included in every experiment. PCR products for both SNPs were evaluated during electrophoresis on 2% agarose gel. Products of PCR reaction for SNPs G34A and C421A had a size of 291 bp and 184 bp, respectively.
Restriction fragment length polymorphism
PCR products for both polymorphisms were digested by restriction enzyme specific to the studied polymorphism: BseMI for SNP G34A and MseI for SNP C421A. The digestion mixture consisted of 16 μL of PCR product, 2 μL of buffer, 0.1 μL of specified enzyme, and 1.9 μL of distilled water up to 20 μL for G34A; and 16 μL of PCR product, 2 μL of buffer, 0.5 μL of specified enzyme, and 1.5 μL of distilled water up to 20 μL. Digestion by restriction enzyme was performed for SNPs G34A and C421A, respectively, at 55°C for 16 h and at 30°C for 16 h. Genotypes for both studied polymorphisms were identified by electrophoresis (on 2% and 4% agarose gel for G34A and C421A, respectively) of amplified DNA fragments after digestion by restriction enzyme. The details of the band patterns are presented in Table 1.
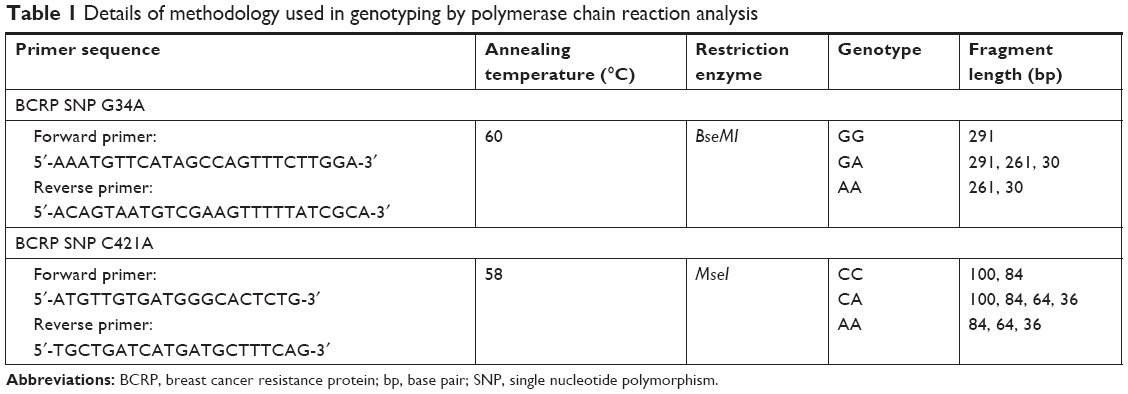 | Table 1 Details of methodology used in genotyping by polymerase chain reaction analysis |
Statistical analyses
All statistical analyses were performed using STATISTICA 10 (2011; StatSoft Inc., Tulsa, OK, USA). The Hardy–Weinberg equation was calculated in the experimental and control groups in the study only for SNP C421A. The χ2 Pearson test with the Yates correction was applied to evaluate conformity between the observed and expected genotype frequencies according to the Hardy–Weinberg rule. To determine the significance of differences in genotype frequencies between the group of multiple myeloma patients and the group of healthy individuals, the χ2 Pearson test with the Yates correction was used. In all conducted tests, P<0.05 was assumed significant.
Ethics statement
The investigation was in accordance with the Declaration of Helsinki and the Good Laboratory Practice rules, and was approved by the Ethical Committee of the Medical University of Lodz (Nos RNN/88/16/KE and RNN/285/13/KE). All patients provided a written informed consent before their inclusion in the study.
Results
This study recruited a total of 181 people diagnosed with multiple myeloma and 97 healthy people as a control group. All samples obtained from patients with multiple myeloma and from healthy individuals were included in the statistical analysis. The multiple myeloma and healthy control groups were analyzed using the Hardy–Weinberg equation model. Both groups were in Hardy–Weinberg equilibrium. Only SNP C421A of the ABCG2 gene was significantly associated with the increased risk of multiple myeloma development (P=0.0218). For SNP G34A in the ABCG2 gene (rs2231137), none of the patients or controls was carrying the minor (A) variant. For SNP C421A (rs2231142), our data showed that 10.5% and 1.1% of the patients with multiple myeloma had CA and AA genotypes respectively, while only 2.1% and 0% patients from the healthy control group had these genotypes (Table 2).
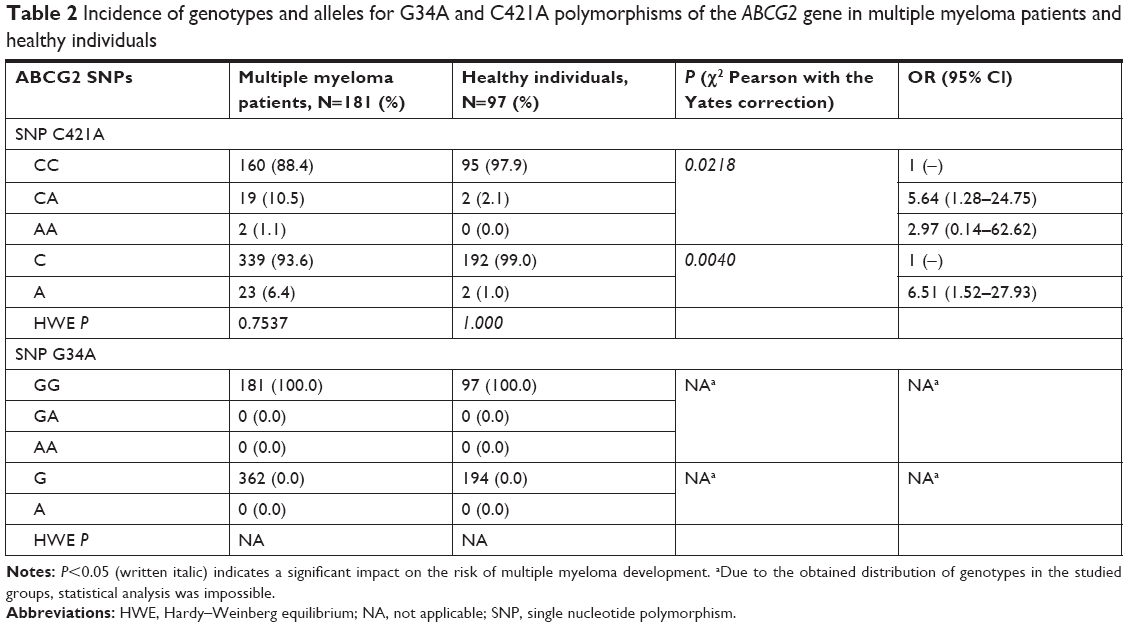 | Table 2 Incidence of genotypes and alleles for G34A and C421A polymorphisms of the ABCG2 gene in multiple myeloma patients and healthy individuals |
The group of patients with multiple myeloma was divided according to gender. Then, the correlation between gender and the incidence of individual genotypes and alleles for the C421A polymorphism in the ABCG2 gene was analyzed. No statistically significant relationship in the case of analysis for genotypes and also in case of the presence of the C allele or the A allele was found (P=0.1255, P=0.1307, and P=0.3865 respectively).
For 84 trials, clinical data were given about the type of immunoglobulin secreted by myeloma cells. In this case, no association was found between the different genotypes of SNP C421A of the ABCG2 gene and the type of immunoglobulin produced (Table 3).
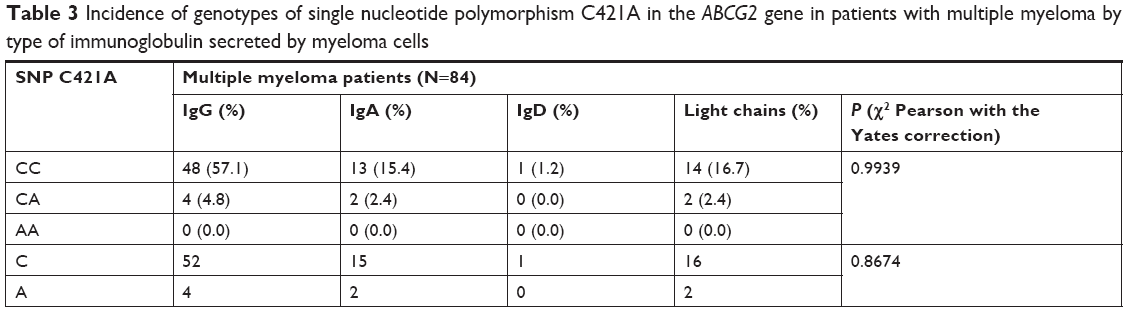 | Table 3 Incidence of genotypes of single nucleotide polymorphism C421A in the ABCG2 gene in patients with multiple myeloma by type of immunoglobulin secreted by myeloma cells |
Due to the lack of substantive association of the obtained results, they were not correlated with other available clinical data: disease advancement according to the Durie-Salmon classification, general condition of the patients according to the WHO, therapy regimen, or laboratory parameters such as C-reactive protein, lactate dehydrogenase, hemoglobin, albumin, and β2-microglobulin level (because data were not available from the whole group of patients with multiple myeloma).
Discussion
Multiple myeloma remains an incurable disease with an average survival of 4–6 years. Extensive epidemiological studies have shown that the processes of detoxification and elimination of xenobiotics from cells are associated with tumors.17 BCRP acts as a pump that actively removes toxic compounds, including carcinogens from cells. SNPs can alter the expression and activity of the relevant genes and their proteins, and predispose them to the development of tumors.9 Much research has been done to clarify the role of SNPs and the development of various cancers including hematologic and solid tumors.15
Thus far, there have been only a few epidemiological studies to investigate the association between G34A and C421A polymorphisms in the ABCG2 gene and the risk of various types of cancer. The exact association between cancer susceptibility and ABCG2 polymorphisms remains unclear. The results appear to depend on the ethnic origin and type of cancer. Previous studies have shown important differences in the frequencies of genotype of G34A and C421A. For G34A, the Han Chinese population appears to have the highest frequency (34%), while the variant allele is extremely rare in the sub-Saharan African population (<1%) and is relatively rare in the African-American (5%) and Caucasian populations in the United States (12%). Variant A of the G34A polymorphism in the European population, according to the dbSNP database, could account for about 5% of the population. However, it may occur at a lower level, such as in the Turkish or Dutch population. To the best of our knowledge, the G34A analysis of the ABCG2 gene presented in this publication is the first study of this type in the Polish population.18 The allelic frequencies in the Mexican-Indian, Mexican, and Latin populations were 90%, 10%, and 40%, respectively. Importantly, the A allele of C421A is widespread in the Japanese and Chinese populations (35%). For the Caucasian population it is below 10% and it is rarest for the sub-Sahara African and African-American populations, accounting for 5%.10
The present study focused on the role of the two most common polymorphisms of the ABCG2 gene in the development of multiple myeloma. G34A is not related to the risk of developing multiple myeloma, whereas C421A was significantly associated with multiple myeloma (P=0.0218).
In contrast to the obtained results, the GA and AA genotype variants of SNP G34A in the ABCG2 gene were associated with increased toxicity in AML. On the other hand, these genotypes were linked with improved survival in AML. In the same study, the ABCG2 C421A polymorphism was associated with decreased drug resistance and a higher risk of death when compared to the wild type.19
Kim et al20 demonstrated that SNP G34A variants may be relevant in response to imatinib therapy used in CML. They showed that the GA and AA genotypes were significantly associated with the lower rate of complete cytogenetic response to imatinib. In contrast, data available in another publication showed that there was no difference in the frequencies of SNP G34A between CML patients with good response and resistance to imatinib, but the AA genotype variant of SNP C421A was associated with the lower risk of resistance development to imatinib for patients with CML.1
Similar studies have been carried out on a group of children with acute lymphoblastic leukemia among SNPs G34A and C421A in BCRP. Only SNP G34A in the ABCG2 gene was related to a higher risk of acute lymphoblastic leukemia, which remains in contrast to the results of the research conducted by us on a group of patients with multiple myeloma.21 Hu et al9 obtained similar results. The researchers reported that the C421A A allele increased the risk of developing diffuse large B-cell lymphoma.
Regarding studies on the role of polymorphisms within the ABCG2 gene in solid tumors, Wu et al14 found an increased frequency of G34A GA and AA genotypes in patients with breast cancer. The G34A allele polymorphism was significantly different in these patients and was associated with an increased risk of cancer. Similarly, the homozygous variant of the C421A AA genotype was associated with a higher risk of developing breast carcinoma.14 Another study on the role of C421A polymorphism in a group of Kurdish breast cancer patients showed that the AA genotype is significantly associated with an increased risk of developing breast cancer.22
Similar results were obtained by Sari et al10 in a study into the role of SNPs in the BCRP transporter and susceptibility to colorectal cancer. In this study, ABCG2 C421A was statistically significantly associated with colorectal cancer risk. In particular, patients with A alleles were much more likely to have the disease than those with C alleles. In contrast, the ABCG2 G34A genotypes in the cases and controls did not differ significantly, and thus polymorphism was not associated with the risk of colorectal cancer.10
C421A in the ABCG2 gene plays contrasting roles in prostate cancer. First, enhanced tumor cell proliferation results from decreasing folate efflux and increased intracellular folate levels. On the other hand, in patients treated with docetaxel intratumoral, the level of docetaxel and tumor cell sensitivity increased and so did the patients’ survival time.23 Different results for C421A and prostatic cancer were obtained by Gardner et al24 as there were no significant differences in the prevalence of prostate cancer based on the genetic variability of ABCG2 in a non-Hispanic Caucasian cohort. Hahn et al25 demonstrated that hormone-refractory prostate cancer patients carrying the ABCG2 C421A genotype were more likely to survive beyond 15 months compared with those carrying the C421A CC genotype.
In contrast, another analysis of the role of SNP C421A in the ABCG2 gene performed by Korenaga et al26 proved that the CC genotype was associated with a higher risk of developing nonpapillary renal cell cancer.
Conclusion
Our study has shown that SNP C421A of the ABCG2 gene predisposed to an increased individual risk of developing multiple myeloma. These results encourage further research into SNP C421A in the BCRP encoding gene and the risk of developing multiple myeloma, despite the fact that the small number of examined individuals may have limited the possibility to detect the effects of SNPs on the risk of multiple myeloma. However, further studies on the relationship between polymorphism and the risk of multiple myeloma are required to confirm our findings prior to the use of polymorphism to identify subgroups with an increased risk of multiple myeloma.
Acknowledgment
This research was supported by statutory funds of the Department of Pharmaceutical Biochemistry and Molecular Diagnostics, Medical University of Lodz (503/3-015-02/503-31-001), research task of Medical University of Lodz (502-03/3-015-02/502-34-109) and by a grant from Medical University of Lodz (named: “grant UMED”) (564/3-000-00/564-20-013).
Disclosure
The authors report no conflicts of interest in this work.
References
Au A, Aziz Baba A, Goh AS, et al. Association of genotypes and haplotypes of multi-drug transporter genes ABCB1 and ABCG2 with clinical response to imatinib mesylate in chronic myeloid leukemia patients. Biomed Pharmacother. 2014;68(3):343–349. | ||
Taylor NMI, Manolaridis I, Jackson SM, et al. Structure of the human multidrug transporter ABCG2. Nature. 2017;3(7659):504–509. | ||
Martino A, Campa D, Buda G, et al. Polymorphisms in xenobiotic transporters ABCB1, ABCG2, ABCC2, ABCC1, abcc3 and multiple myeloma risk: a case-control study in the context of the International multiple myeloma rESEarch (IMMEnSE) Consortium. Leukemia. 2012;26(6):1419–1422. | ||
Ross DD. Modulation of drug resistance transporters as a strategy for treating myelodysplastic syndrome. Best Pract Res Clin Haematol. 2004;17(4):641–651. | ||
Sarkadi B, Özvegy-Laczka C, Német K, Váradi A. ABCG2 – a transporter for all seasons. FEBS Lett. 2004;567(1):116–120. | ||
Ni Z, Bikadi Z, Rosenberg MF, Mao Q. Structure and function of the human breast cancer resistance protein (BCRP/ABCG2). Curr Drug Metab. 2010;11(7):603–617. | ||
Lockhart AC, Tirona RG, Kim RB. Pharmacogenetics of ATP-binding cassette transporters in cancer and chemotherapy. Mol Cancer Ther. 2003;2(7):685–698. | ||
Tang L, Bergevoet SM, Gilissen C, et al. Hematopoietic stem cells exhibit a specific ABC transporter gene expression profile clearly distinct from other stem cells. BMC Pharmacol. 2010;10(1):12. | ||
Hu LL, Wang XX, Chen X, et al. BCRP gene polymorphisms are associated with susceptibility and survival of diffuse large B-cell lymphoma. Carcinogenesis. 2007;28(8):1740–1744. | ||
Sari FM, Yanar HT, Ozhan G. Investigation of the functional single-nucleotide polymorphisms in the BCRP transporter and susceptibility to colorectal cancer. Biomed Rep. 2015;3(1):105–109. | ||
Cheok MH, Pottier N, Kager L, Evans WE. Pharmacogenetics in acute lymphoblastic leukemia. Semin Hematol. 2009;46(1):39–51. | ||
Hardwick LJ, Velamakanni S, van Veen HW. The emerging pharmacotherapeutic significance of the breast cancer resistance protein (ABCG2). Br J Pharmacol. 2007;151(2):163–174. | ||
Noguchi K, Katayama K, Sugimoto Y. Human ABC transporter ABCG2/BCRP expression in chemoresistance: basic and clinical perspectives for molecular cancer therapeutics. Pharmgenomics Pers Med. 2014;7:53–64. | ||
Wu H, Liu Y, Kang H, et al. Genetic variations in ABCG2 gene predict breast carcinoma susceptibility and clinical outcomes after treatment with anthracycline-based chemotherapy. BioMed Res Int. 2015;2015(1):1–12. | ||
Natarajan K, Xie Y, Baer MR, Ross DD. Role of breast cancer resistance protein (BCRP/ABCG2) in cancer drug resistance. Biochem Pharmacol. 2012;83(8):1084–1103. | ||
Fehér Á, Juhász A, László A, et al. Association between the ABCG2 C421A polymorphism and Alzheimer’s disease. Neurosci Lett. 2013;550:51–54. | ||
Chen P, Zhao L, Zou P, et al. The contribution of the ABCG2 C421A polymorphism to cancer susceptibility: a meta-analysis of the current literature. BMC Canc. 2012;12(1):383. | ||
Bosch TM, Kjellberg LM, Bouwers A, et al. Detection of single nucleotide polymorphisms in the ABCG2 gene in a Dutch population. Am J Pharmacogenomics. 2005;5(2):123–131. | ||
Hampras SS, Sucheston L, Weiss J, et al. Genetic polymorphisms of ATP-binding cassette (ABC) proteins, overall survival and drug toxicity in patients with acute myeloid leukemia. Int J Mol Epidemiol Genet. 2010;1(3):201–207. | ||
Kim DH, Sriharsha L, Xu W, et al. Clinical relevance of a pharmacogenetic approach using multiple candidate genes to predict response and resistance to imatinib therapy in chronic myeloid leukemia. Clin Canc Res. 2009;15(14):4750–4758. | ||
Zhai X, Wang H, Zhu X, et al. Gene polymorphisms of ABC transporters are associated with clinical outcomes in children with acute lymphoblastic leukemia. Arch Med Sci. 2012;4(4):659–671. | ||
Ghafouri H, Ghaderi B, Amini S, et al. Association of ABCB1 and ABCG2 single nucleotide polymorphisms with clinical findings and response to chemotherapy treatments in Kurdish patients with breast cancer. Tumor Biol. 2016;37(6):7901–7906. | ||
Sobek KM, Cummings JL, Bacich DJ, O’Keefe DS. Contrasting roles of the ABCG2 Q141K variant in prostate cancer. Exp Cell Res. 2017;354(1):40–47. | ||
Gardner ER, Ahlers CM, Shukla S, et al. Association of the ABCG2 C421A polymorphism with prostate cancer risk and survival. BJU Int. 2008;102(11):1694–1699. | ||
Hahn NM, Marsh S, Fisher W, et al. Hoosier Oncology Group randomized phase II study of docetaxel, vinorelbine, and estramustine in combination in hormone-refractory prostate cancer with pharmacogenetic survival analysis. Clin Canc Res. 2006;12(20 Pt 1):6094–6099. | ||
Korenaga Y, Naito K, Okayama N, et al. Association of the BCRP C421A polymorphism with nonpapillary renal cell carcinoma. Int J Cancer. 2005;117(3):431–434. |
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.