Back to Journals » Journal of Multidisciplinary Healthcare » Volume 7
The community-based Health Extension Program significantly improved contraceptive utilization in West Gojjam Zone, Ethiopia
Authors Yitayal M ![]() , Berhane Y
, Berhane Y ![]() , Worku A, Kebede Y
, Worku A, Kebede Y ![]()
Received 12 February 2014
Accepted for publication 17 March 2014
Published 15 May 2014 Volume 2014:7 Pages 201—208
DOI https://doi.org/10.2147/JMDH.S62294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Mezgebu Yitayal,1 Yemane Berhane,2 Alemayehu Worku,3 Yigzaw Kebede1
1University of Gondar, Gondar, Ethiopia; 2Addis Continental Institute of Public Health, Addis Ababa, Ethiopia; 3Addis Ababa University, Addis Ababa, Ethiopia
Background: Ethiopia has implemented a nationwide primary health program at grassroots level (known as the Health Extension Program) since 2003 to increase public access to basic health services. This study was conducted to assess whether households that fully implemented the Health Extension Program have improved current contraceptive use.
Methods: A cross-sectional community-based survey was conducted to collect data from 1,320 mothers using a structured questionnaire. A multivariate logistic regression was used to identify the predictors of current contraceptive utilization. A propensity score analysis was used to determine the contribution of the Health Extension Program “model households” on current contraceptive utilization.
Result: Mothers from households which fully benefited from the Health Extension Program (“model households”) were 3.97 (adjusted odds ratio, 3.97; 95% confidence interval, 3.01–5.23) times more likely to use contraceptives compared with mothers from non-model households. Model household status contributed to 29.3% (t=7.08) of the increase in current contraceptive utilization.
Conclusion: The Health Extension Program when implemented fully could help to increase the utilization of contraceptives in the rural community and improve family planning.
Keywords: Health Extension Program, current contraceptive utilization
Background
The Government of Ethiopia has implemented the Health Extension Program (HEP) since 20031 to improve primary health coverage at the grassroots level. The center for the HEP activity is a health post (HP) located in each smallest administrative unit of the country and is staffed by two female Health Extension workers (HEWs) who receive 1 year’s training and a regular salary from the government.2,3
Community health workers (CHWs) improve access, and increase the utilization of primary health care by serving as a bridge between clients in need and needed health care and human services.4,5 The HEWs in the Ethiopian context are responsible for implementing the HEP packages. They spend 75% of their time on household visits to teach and demonstrate HEP packages to the community, and 25% in the HP to provide basic health services. The HEP has 16 packages under disease prevention and control, family health, hygiene and environmental sanitation, and health education and communication services. The three packages, HIV/AIDS (human immunodeficiency virus/acquired immunodeficiency syndrome) and tuberculosis, malaria prevention and control, and first aid emergency measures, are under disease prevention and control services. The five packages, maternal and child health, family planning, immunization, nutrition, and adolescent reproductive health, are under family health services. The seven packages, excreta disposal, solid and liquid waste disposal, water supply and safety measures, food hygiene and safety measures, healthy home environment, control of insects and rodents, and personal hygiene, are under hygiene and environmental sanitation services. Finally, the health education and communication package, which is a tool for implementing all the packages, deal with services related to health education and communication.1–3
The HEP is designed to increase the coverage of primary health care services in Ethiopia, mainly by producing model households using model-family training. The model-family training comprises a total of 96 hours of training on basic hygiene and environmental sanitation (30 hours), family health care (42 hours), and disease prevention and control (24 hours). Households which attend at least 75% of the training and implement at least 75% of the HEP packages receive certificates of completion at a graduation ceremony and graduate as model households (families). The program also addresses health service utilization through the establishment of an HP to serve 5,000 people, and the deployment of two HEWs who conduct home visits in the community and give basic health services in each HP.2
In many African countries, CHWs have fulfilled generalist health functions, and evidences suggest that they have increased the coverage of a range of services.6–8 Home visiting services by CHWs and other community-based health programs, such as community-based reproductive health communication interventions and community-based distribution programs to promote maternal and child health as well as family planning, have been implemented in different countries and have shown encouraging results.9–13
Previous studies on the effects of HEP in Ethiopia have indicated that the program has had a tangible effect on maternal and child health outcomes such as increased full immunization rates, BCG (Bacille de Calmette et Guérin) vaccination, DPT3 (diphtheria–pertussis–tetanus vaccines), and increased TT2 (tetanus–toxoid vaccine). The contribution of the HEP “model households” on current use of any contraceptive method among married women has also been reported in some studies related to HEP.14–19
Although there are signs of promising results of the HEP, evidences are very few. Therefore, this study was conducted with the aim of assessing whether or not HEP “model households” have better contraceptive utilization in Ethiopia.
Methods
A community-based cross-sectional study was conducted among mothers in 1,320 households drawn from 44 kebeles (lowest administrative units) over a period of 3 months (March–May, 2012). The kebeles were randomly selected from six districts (Yilmana Densa, Mecha, Semien Achefer, Bure, Jabi Tehnan, and Dega Damot) in West Gojjam Zone, the Amhara National Regional State, Ethiopia. The HEP was launched in 2003, and during the study period, there were 6,530 HEWs (6,401 rural and 129 urban HEWs) in the region, and 782 HEWs (772 rural and 10 urban HEWs) in the West Gojjam Zone who were responsible for implementing the packages of the HEP.
A multistage sampling procedure was used to select the study population. At the first stage, six districts were randomly selected from the 13 rural districts in the study administration zone. At the second stage, 44 kebeles out of 184 were selected randomly from the six districts. In the third stage, 30 households were selected randomly from each kebele to get 1,320 mothers required for the study. The study population for this work was women aged 15–49 years in the selected kebeles.
To collect information for the study, interviews were administered using a structured questionnaire consisting mainly of closed-ended questions. Twelve data collectors and six supervisors were recruited and trained to administer the questionnaire. The data collectors were nurses (diploma graduates), and the supervisors were health officers (BSc [Bachelor of Science] holders). The structured questionnaire was pre-tested in kebeles which were not included in the actual study in the same administrative zone. The pre-test was done on 5% of the study participants, and the questionnaire was assessed for its completeness, clarity, and length before starting the survey. A daily data quality-check was made during the study, and data were double-entered to minimize error during data processing.
For this study, model households were defined as households that attended at least 75% of the training given by HEWs and implemented at least 75% of the HEP packages. Current contraceptive utilization was confirmed by asking the study participants whether they were then using any family planning methods, checking what types of methods they were using and for how long, and by checking the availability of family planning methods, and then by finding out if they were using contraceptive pills.
Data analysis
Data were entered into Epi-Info™ 3.5.1 (Centers for Disease Control and Prevention, Atlanta, GA, USA) and transferred to SPSS 16 (SPSS Inc., Chicago, IL, USA) for binary logistic regression analysis and to STATA 12 (StataCorp LP, College Station, TX, USA) for propensity score analysis. Mean and standard deviation were used to describe the sociodemographic and economic characteristics of the study participants.
The binary logistic regression was used to see the association of current contraceptive utilization with sociodemographic and economic characteristics and HEP-related factors. Multivariate logistic regression was used to control confounding factors and to get less biased estimates of the association between explanatory and outcome variables. Explanatory variables which had significant association with current contraceptive utilization (P<0.2) in the bivariate binary logistic regression were entered in to multivariate logistic regression model to identify the predictors of current contraceptive utilization.
Propensity score analysis was conducted to determine the effects of the HEP model households on current contraceptive utilization in the community. A propensity score is the probability of being exposed to the intervention (in this case, being HEP model household) given a set of observed covariates, X, and it was estimated using the logistic regression model. Nearest neighborhood matching was used in the analysis, which matches a given treated subject to an untreated subject whose propensity score was closest to that of the treated subject or vice versa. The method was used to balance the intervention and control units so that a direct comparison would be possible for evaluating the effects of the HEP model households on current contraceptive utilization. The average treatment effect on treated model households was computed by averaging the difference between the outcome of the model households and the outcome of the non-model households.
Ethical issues
The University of Gondar Ethics Review Committee approved the research proposal. Written informed consent was obtained from each study participant. Confidentiality was assured by not taking personal identifiers. The respondents were also informed of their freedom to withdraw at any time while they were being interviewed.
Results
Socioeconomic and demographic characteristics of study participants
A total of 1,318 mothers, 1,006 (76.3%) of whom were from model households, and 312 (23.7%) from non-model households), participated in the study, with a response rate of 99.85%. The age of the respondents ranged from 18 to 48 years, with a mean age of 32.53±6.25 years. Out of the participants, 90.1% were married, 74.2% illiterate, 79.0% housewives, 100% Orthodox Christians, and 99.3% Amhara. The average family size was 5.53±1.79 individuals. The average monthly income of the households was 887.90±587.632 birr (Table 1).
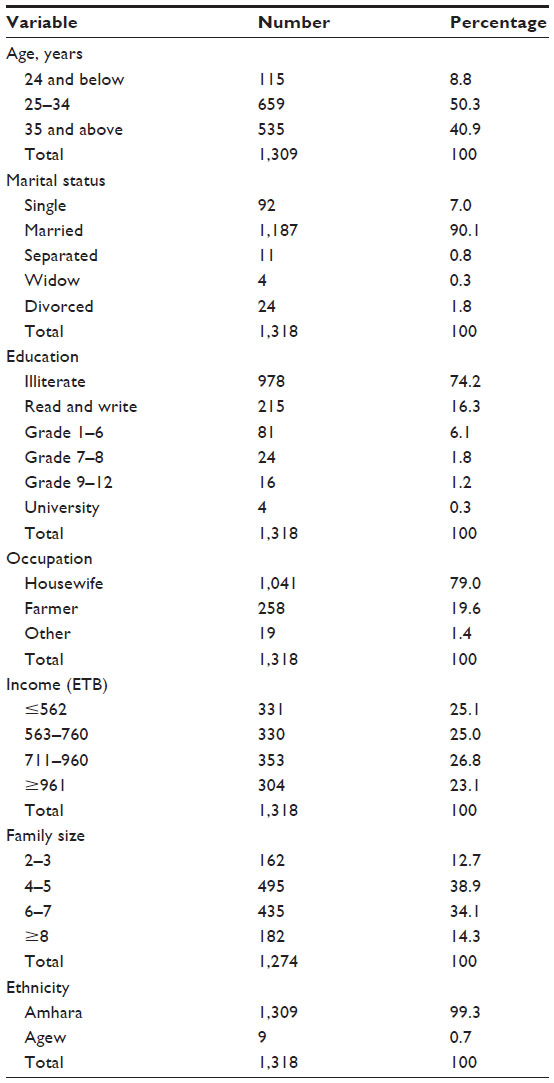 | Table 1 Socioeconomic and demographic characteristics of study participants, West Gojjam Zone, Amhara National Regional State, Ethiopia, 2012 |
A total of 1,211 study participants (91.9%) had heard about the HEP; and of these, HEWs were the source of information for 1,190 (98.3%). Of 1,211 of the study participants, 890 (73.5%) felt that they understood/comprehended what the HEP was, but only 373 (41.9%) out of 890 accurately mentioned the number of HEP packages. Most of the study participants (94.7%) viewed the conduct of HEWs as “good”, and 94.4% rated the health services provided at the HPs as of “good quality”. A total of 1,034 (78.5%) study participants visited HPs during the year. Model households numbered 1,006 (76.3%), and 68.3% graduated in 2009 and 2010. A total of 1,110 study participants (84.2%) had home visits by HEWs, and 52.7% had frequent visits (at least one visit every 4 weeks), as indicated in Table 2.
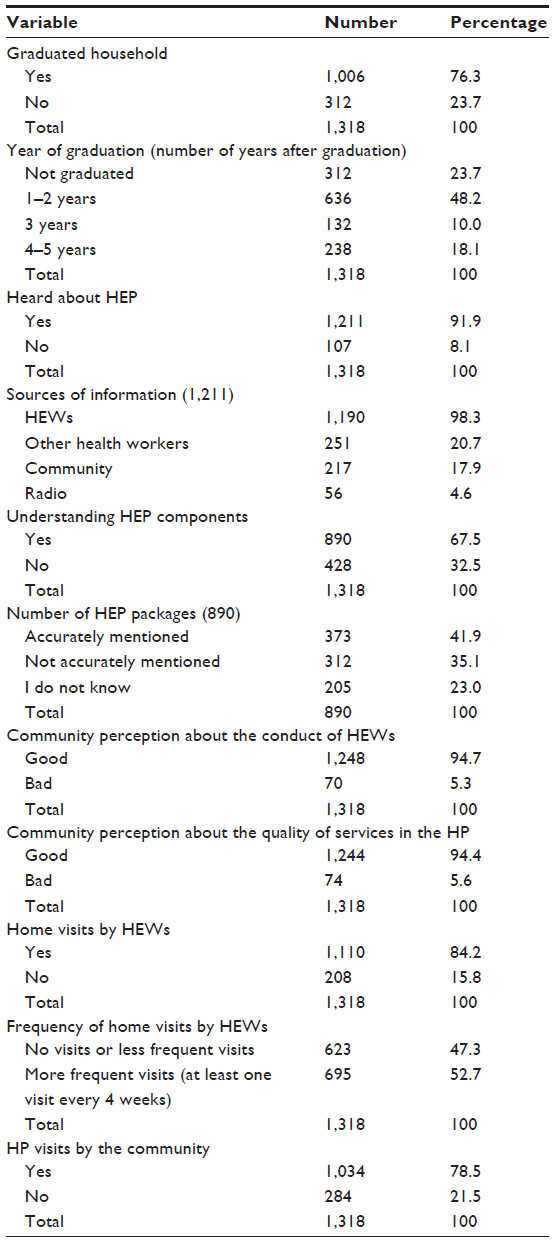 | Table 2 Study participants’ HEP-related status in West Gojjam Zone, Ethiopia, 2012 |
Contraceptive utilization
A total of 1,239 (94.0%) study participants had heard about family planning, and HEWs were the source of information for 1,149 (92.74%). Only 119 (9%) mothers were able to identify six or more family planning methods. A total of 1,045 (79.3%) mothers used contraceptives, and 873 (66.2%) were current users. Out of the current contraceptive users, 767 (87.9%) used injectables and 49 (5.6%) implants as family planning methods, and 591 (67.7%) of the current users were getting the contraceptive methods from the HPs (Table 3).
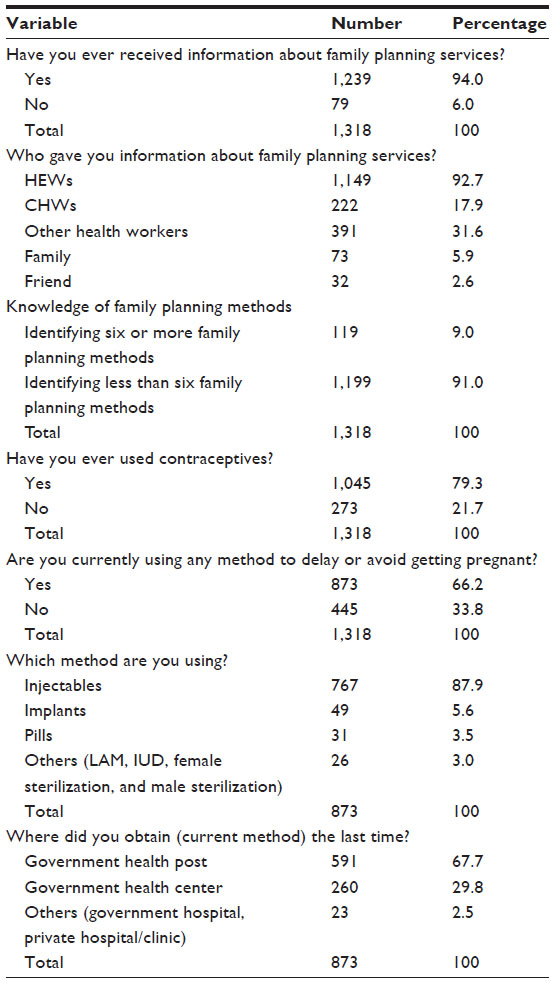 | Table 3 Study participants’ knowledge and utilization of contraceptives, West Gojjam Zone, Amhara National Regional State, Ethiopia, 2012 |
Multivariate logistic regression
Mothers from HEP model households were 3.966 times more likely to utilize contraceptives (adjusted odds ratio [AOR], 3.966; 95% confidence interval [CI], 3.007–5.230) compared with mothers from non-model households. Mothers who identified six or more types of family planning methods were 2.724 times more likely to use contraceptives (AOR, 2.724; 95% CI, 1.640–4.523) compared with mothers who identified less than six types of family planning methods. Mothers who could at least read and write were 1.418 times more likely to use contraceptives (AOR, 1.418; 95% CI, 1.058–1.899) compared with illiterate mothers (Table 4).
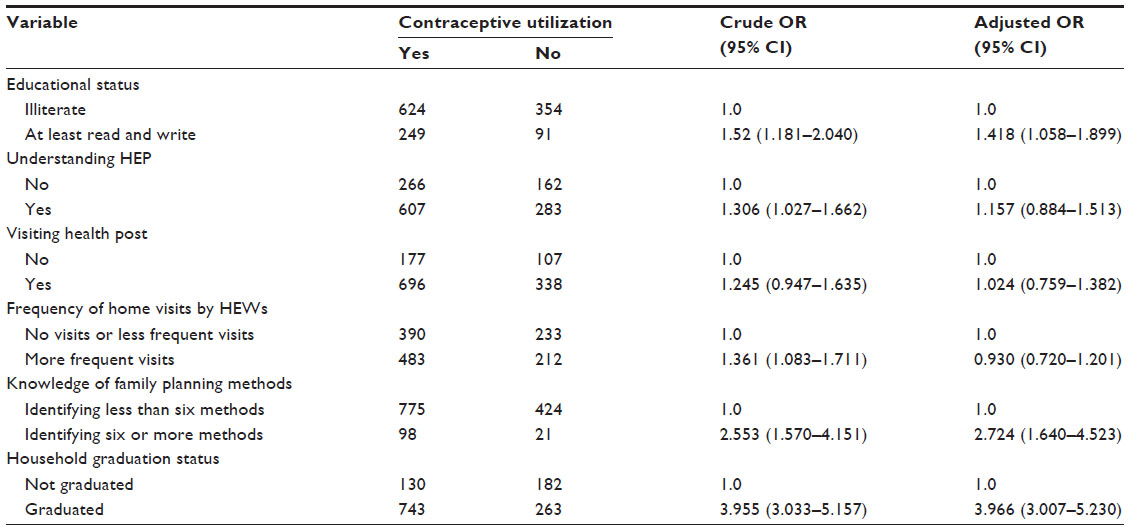 | Table 4 Factors associated with current contraceptive utilization by the community, West Gojjam Zone, Ethiopia, 2012 (n=1,318) |
Propensity score analysis
Descriptive results of the study indicated that mothers from 73.86% of the model households and 41.67% of the non-model households were using contraceptive methods. By statistically balancing 1,006 HEP model households (intervention group) and 312 HEP non-model households (matched control group) based on the propensity scores and all the variables used to construct it, the average treatment effect on treated model households was found to be 0.293 points (t=7.084) for contraceptive utilization. This indicated that HEP model households contributed a 29.30% increase to current contraceptive utilization compared with HEP non-model households (Table 5).
 | Table 5 ATT of HEP “model households” on current contraceptive utilization by the community, West Gojjam Zone, Ethiopia, 2012 |
Discussion
The study showed that participation in the HEP significantly increased mothers’ current contraceptive utilization in the community. Household graduation status (being model households) had a positive significant association with and significantly contributed to current contraceptive utilization in the community, which is in agreement with previous assessments of HEP in Ethiopia.14–16 The proportion of married women who were current contraceptive method users was higher in households that had graduated as a model-family than in households that had not yet graduated as a model-family.16 Another assessment in Ethiopia also indicated that the increase in contraceptive use was largely attributable to the HEP.17–19 Findings of studies on other community-based health programs in other countries also support this study. Studies on the effect of community-based reproductive health communication interventions on contraceptive use among young married couples in Bihar, India, and community-based distribution programs on contraceptive uptake in Ethiopia have indicated that demand for contraception increases in intervention areas.9,10
The present study also indicated that mothers who had more knowledge about contraceptive methods were more likely to use contraceptives than mothers who had less knowledge about contraceptive methods, which is in line with findings of studies in other countries.20–22 A study on contraceptive use among reproductive-age women in Kenya’s city slums has indicated that women’s knowledge of family planning is associated with use of family planning services.20 In India, a study on knowledge and use of contraception among married adolescent women has indicated that there is a huge difference in contraceptive use between women who know all modern methods of contraception and those who know only some of them.21 In Nigeria, a study on knowledge and practice of contraception among women of reproductive age has revealed that there is a significant relationship between respondents’ level of awareness to family planning and their use of contraceptives.22
Although the overall educational status of women in the study area was generally low, the present study indicated that literate mothers who could at least read and write were more likely to use contraceptives than illiterate mothers. This was consistent with a study done in Bangladesh which indicated that school attendance has significant effects on knowledge of family planning and on use of contraception.23 Studies on the relationship of female literacy with contraceptive use in urban slums of Punjab, and on women’s autonomy, education, and contraception use in Pakistan have concluded that contraceptive use is strongly associated with women’s education, indicating higher education level is associated with higher use of contraceptives.24,25 Contrary to these findings, studies in Taiwan and Nicaragua have indicated no association between health literacy and health care utilization, even after adjusting for other covariates.26,27
In this study, frequency of household visits by HEWs had no significant association with current contraceptive utilization, which is in contrast to a previous study.8 A meta-analysis of home visiting programs for at-risk families to examine differences in the effects of programs on maternal behavior has indicated that the effectiveness of home visiting programs is principally dependent upon the frequency of services, stating that programs with more frequent contact between home visitors and their clients are most successful.8 In contrast to these findings, some systematic reviews of home visiting programs have found no pattern of difference in the average intensity and duration of the program related to the outcomes measured.28,29
Conclusion
This study indicated that HEP model households contributed significantly to current contraceptive utilization compared with non-model households. It also indicated that mothers’ knowledge about contraceptive methods had a significant association with current contraceptive utilization in the community.
Households need to be encouraged to participate regularly in the HEP by implementing strategies that enhance their motivation by providing evidence of the positive changes that are occurring in the communities. In addition, following up the existing model households, and producing more model households by giving model-family training to non-model households are crucial in the implementation of the HEP to increase basic health service utilization.
This study gives insight that other zones and regions of Ethiopia, and other countries of similar conditions with Ethiopia, may benefit from the findings of this study in their effort to implement the HEP and similar health programs that reach the community at the grass-roots level. The HEP was also started in urban areas of the country and is expected to bring about better health service utilization; however, studies are needed to ascertain this.
Limitations of the study
This study was designed to assess the effects of HEP model households on contraceptive utilization using a cross-sectional study design so that causal relationships between determinants and current contraceptive utilization might not be ascertained. The application of propensity score analysis could give us an option, but it could not be as effective as randomized controlled trials to identify the effects of HEP model households. There was lack of baseline information about contraceptive utilization before the implementation of the HEP, and we could therefore not measure the actual contribution of the HEP to contraceptive utilization from the base line. Also, the two groups (model households and non-model households) were not formatted randomly.
Authors’ information
MY is a lecturer of Health Service Management and Health Economics at the Institute of Public Health, the University of Gondar. He is also a PhD student at the University of Gondar and Addis Continental Institute of Public Health Joint PhD Program doing his dissertation on the Implementation of the Health Extension Program in West Gojjam Zone, Amhara National Regional State, Ethiopia. YB is a Professor of Epidemiology and Public Health at the Addis Continental Institute of Public Health, Addis Ababa, Ethiopia. AW is Associate Professor of Biostatistics at the Addis Ababa University, Addis Ababa, Ethiopia. YK is a Professor of Public Health at the University of Gondar and Director of Dabat Rural Health Research Center of the University, Gondar, Ethiopia.
Acknowledgments
We would like to thank the Amhara National Regional Health Bureau, and West Gojjam Zone Health Department for facilitating the conduct of this study. Our special thanks also extend to all study participants who participated in this study, unreservedly committing their time. This study was funded by the University of Gondar and the African Health and Population Research Center (AHPRC), which is supported by the International Research Development Center (IRDC), Canada.
Author contributions
MY conceived the study, participated in the design, data collection, and analysis of the study, and drafted the manuscript. YB participated in the conceptualization and design of the study and helped to draft the manuscript. AW helped in the design of the study and analysis of the data, and contributed to the drafting of the manuscript. YK also participated in the design of the study and contributed to the drafting of the manuscript. All authors read and approved the final manuscript.
Disclosure
The authors declare that they have no competing interests.
References
Federal Ministry of Health. Health Sector Strategic Plan (HSDP-III), Planning and Programming Department. Addis Ababa, Ethiopia; 2005. | |
Federal Ministry of Health. Health Extension Program in Ethiopia Profile, Health Extension and Education Center. Addis Ababa, Ethiopia; Jun 2007. Available from: http://www.pathfinder.org/publications-tools/pdfs/Ethiopias-Health-Extension-Program-Pathfinder-Internationals-Support-2003–2007.pdf. Accessed April 17, 2014. | |
Federal Ministry of Health. Health Extension program implementations guide line. Addis Ababa, Ethiopia; Jul 2005. Available from: http://www.etharc.org/resources/download/finish/66/365. Accessed April 17, 2014. | |
Ro MJ, Treadwell HM, Northridge M. Community Health Workers and Community Voices: promoting Good Health. National Center for Primary Care at Morehouse School of Medicine. W.K. Kellogg Foundation, New York, NY. 2003. | |
Witmer A, Seifer SD, Finocchio L, Leslie J, O’Neil EH. Community health workers: integral members of the health care work force. Am J Public Health. 1995;85(8):1055–1058. | |
Perez F, Ba H, Dastagire SG, Altmann M. The role of community health workers in improving child health programmes in Mali. BMC Int Health Hum Rights. 2009;9:28. | |
Mushi D, Mpembeni R, Jahn A. Effectiveness of community based safe motherhood promoters in improving the utilization of obstetric care. The case of Mtwara Rural District in Tanzania. BMC Pregnancy Childbirth. 2010;10:14. | |
McDonald M, Moore T. Sustained Home Visiting for Vulnerable Families and Children: a Literature Review of Effective Programs Prepared for Australian Research Alliance for Children and Youth, Parkville, Victoria. The Royal Children’s Hospital’s Centre for Community Child Health and Murdoch Childrens Research Institute; 2012. Available from http://www.aracy.org.au/documents/item/61. Accessed April 17, 2014. | |
Daniel EE, Masilamani R, Rahman M. The effect of community-based reproductive health communication interventions on contraceptive use among young married couples in Bihar, India. Int Fam Plan Perspect. 2008;34(4):189–197. | |
Tawye Y, Jotie F, Shigu T, Ngom P, Maggwa N. The potential impact of community-based distribution programmes on contraceptive uptake in resource-poor settings: evidence from Ethiopia. Afr J Reprod Health. 2005;9(3):15–26. | |
Gryboski K, Yinger NV, Dios RH, Worley H, Fikree FF. Working With the Community for Improved Health. Health Bulletin Number 3. Washington, DC: Population Reference Bureau; 2006. Available from: http://www.prb.org/pdf06/WorkingWithTheCommunity.pdf. Accessed March 27, 2014. | |
Ugal DB. Household environment and maternal health among rural women of Northern Cross River State, Nigeria. Ea. 2010;2(2). | |
Grosso PD, Kleinman R, Esposito AM, Martin ES, Paulsell D. Assessing the Evidence of Effectiveness of Home Visiting Program Models Implemented in Tribal Communities. Washington, DC: Office of Planning, Research and Evaluation, Administration for Children and Families, US. Department of Health and Human Services; 2011. | |
Amare S. The Impact of Ethiopian Health Services Extension Program on Maternal and Child Health Outcomes: The Case of Tigray Region [master’s thesis]. Atlanta, GA: George State University; 2013. | |
Admassie A, Abebaw D, Woldemichael AD. Impact Evaluation of the Ethiopian Health Services Extension Program. New Delhi: Global Development Network; 2009. | |
Center for National Health Development in Ethiopia. Ethiopia Health Extension Program Evaluation Study: Rural Ethiopia, 2005–2010, Part-I. Household Health Survey, Addis Ababa, Ethiopia. Colombia University; 2011. | |
Medhanyie A, Spigt M, Kifle Y, et al. The role of health extension workers in improving utilization of maternal health services in rural areas in Ethiopia: a cross sectional study. BMC Health Serv Res. 2012;12:352. | |
The Last Ten Kilometers Project. Baseline Household Health Survey: Amhara, Oromiya, SNNP and Tigray. Addis Ababa, Ethiopia: JSI Research and Training, Inc.; 2009. | |
Gurmu E, Mturi AJ. Trend and correlates of contraceptive use in rural and urban Ethiopia: is there a link to the health extension programme? Etude Popul Afr. 2013;27(2):140–154. | |
Okech TC, Wawire NW, Mburu TK. Contraceptive use among women of reproductive age in Kenya’s city slums. Int J Bus Soc Sci. 2011;2(1):22–43. | |
Narzary PK. Knowledge and use of contraception among currently married adolescent women in India. Stud Home Comm Sci. 2009;3(1):43–49. | |
Adeyinka A, Asabi O, Adedotun O. Knowledge and practice of contraception among women of reproductive ages in South West, Nigeria. Int J Eng Sci. 2012;1(2):70–76. | |
Islam MR, Thorvaldsen G. Family planning knowledge and current use of contraception among the Mru indigenous women in Bangladesh: a multivariate analysis. Open Access J Contracept. 2012;3:9–16. | |
Sarmad R, Akhtar S, Manzoor S. Relationship of female literacy to contraceptive use in urban slums of Khushab (Punjab). Biomedica. 2007;23:21–23. | |
Saleem S, Bobak M. Women’s autonomy, education and contraception use in Pakistan: a national study. Reprod Health. 2005;2:8. | |
Lee SY, Tsai TI, Tsai YW, Kuo KN. Health literacy, health status, and healthcare utilization of Taiwanese adults: results from a national survey. BMC Public Health. 2010;10:614. | |
Lubbock LA, Stephenson RB. Utilization of maternal health care services in the department of Matagalpa, Nicaragua. Rev Panam Salud Publica. 2008;24(2):75–84. | |
Aslam H, Kemp L. Home Visiting in South Western Sydney: an Integrative Literature Review, Description and Development of a Generic Model. Sydney: Centre for Health Equity Training Research and Evaluation; 2005. | |
Kendrick D, Elkan R, Hewitt M, et al. Does home visiting improve parenting and the quality of the home environment? A systematic review and meta analysis. Arch Dis Child. 2000;82:443–451. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.