Back to Journals » Cancer Management and Research » Volume 17

The Communication-Based Intervention Program Based on Narrative Medicine Theory Effectively Improves the Quality of Nursing Care for Nasopharyngeal Cancer Patients Undergoing Radiotherapy and Chemotherapy
Authors Liu XL, Chen BZ, Lin YY, Chen ZX, Zhu QH
Received 12 February 2025
Accepted for publication 16 August 2025
Published 10 September 2025 Volume 2025:17 Pages 1925—1934
DOI https://doi.org/10.2147/CMAR.S521105
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Yong Teng
Xing-Li Liu,1 Bao-Zhu Chen,1 Yun-Ying Lin,2 Zhi-Xian Chen,3 Qiao-Hua Zhu1
1Department 1 of Oncology, The Eighth Affiliated Hospital of Southern Medical University (The First People’s Hospital of Shunde Foshan), Foshan, 528308, People’s Republic of China; 2Youth League Committee, The Eighth Affiliated Hospital of Southern Medical University (The First People’s Hospital of Shunde Foshan), Foshan, 528308, People’s Republic of China; 3Department 2 of Oncology, The Eighth Affiliated Hospital of Southern Medical University (The First People’s Hospital of Shunde Foshan), Foshan, 528308, People’s Republic of China
Correspondence: Qiao-Hua Zhu, Email [email protected]
Objective: To evaluate the impact of a communication-based intervention program rooted in narrative medicine theory on the quality of nursing care and patient outcomes in nasopharyngeal carcinoma patients undergoing radiotherapy and chemotherapy.
Methods: This retrospective cohort study included 98 nasopharyngeal carcinoma patients treated at our hospital between September 2022 and August 2024. Patients were divided into two groups based on historical nursing records: the control group (n=49) received routine standard nursing care, while the observation group (n=49) received routine care supplemented with a narrative medicine-based communication intervention. The intervention was conducted 1– 2 times per week over four consecutive weeks. Outcomes were assessed using the Fear of Progression Questionnaire-Short Form (FoP-Q-SF), Pittsburgh Sleep Quality Index (PSQI), Cancer Fatigue Scale (CFS), Herth Hope Index (HHI), Nursing Quality Evaluation Scale, and Communication Satisfaction Questionnaire, measured at baseline and post-intervention.
Results: Compared to controls, the observation group showed significantly reduced fear of progression (FoP-Q-SF: 33.53 vs 43.11), improved sleep (PSQI: 11.25 vs 15.41), lower cancer-related fatigue (CFS total: 28.23 vs 35.94), and higher hope levels (HHI: 33.45 vs 25.56) (all p < 0.001). Nursing quality and communication satisfaction also improved significantly across all domains (p < 0.001).
Conclusion: The communication-based intervention program based on narrative medicine significantly improves psychological well-being, sleep quality, cancer-related fatigue, hope level, and overall nursing quality in nasopharyngeal carcinoma patients undergoing radiotherapy and chemotherapy. This approach offers a feasible and effective model for enhancing holistic cancer care.
Keywords: narrative medicine, patient-nurse communication, nasopharyngeal cancer, psychological state
Introduction
Nasopharyngeal carcinoma is a malignant tumor with a relatively low incidence globally but significantly higher in regions such as southern China and Southeast Asia, demonstrating a marked regional characteristic.1 It originates in the epithelial tissue of the nasopharynx and has a high risk of metastasis, often invading surrounding tissue structures. It can spread through the lymphatic system to the neck and via the bloodstream to vital organs such as the lungs and liver.2 Among all head and neck malignancies, nasopharyngeal carcinoma has the highest incidence.3,4 Radiotherapy and chemotherapy are the primary treatments for nasopharyngeal carcinoma, particularly for patients in intermediate and advanced stages who often require combined treatment modalities. Recent advances in radiation oncology highlight persistent clinical challenges, including precision targeting and toxicity management in complex anatomical sites like the nasopharynx.5,6 However, the side effects associated with radiotherapy and chemotherapy, such as dry mouth, mucositis, decreased appetite, and nausea, not only affect the patient’s physical condition but also have a substantial negative impact on their psychological state.7,8 Many patients experience varying degrees of anxiety and depression during treatment, further affecting their adherence to treatment and prognosis. Therefore, improving nursing quality, helping patients alleviate psychological stress, and enhancing their confidence in treatment have become critical issues in clinical nursing.
Numerous scholars have indicated that in the nursing care of nasopharyngeal carcinoma patients undergoing radiotherapy and chemotherapy, the emotional and psychological needs of patients are often overlooked. Traditional nursing models tend to focus more on disease treatment itself rather than effective management of patients’ psychological states and emotions. Previous studies in oncology nursing have demonstrated that narrative-based interventions significantly reduce distress in breast cancer patients9 and improve coping mechanisms among leukemia survivors,10 underscoring the cross-applicability of this approach. Narrative Medicine, an emerging medical model, emphasizes listening to patients’ stories and narratives, focusing on their subjective experiences and emotional expressions to create a more humane and individualized healthcare relationship. Narrative Medicine posits that healthcare providers should be not only treaters of diseases but also listeners and supporters of patients’ emotions.11,12 Through effective communication between nurses and patients, healthcare providers can gain a deeper understanding of patients’ psychological needs and emotional experiences, thereby offering more comprehensive and personalized care during the treatment process.
This study aims to explore the application effects of a communication-based intervention program grounded in narrative medicine theory in the nursing care of nasopharyngeal carcinoma during radiotherapy and chemotherapy. It evaluates the program’s impact on patient satisfaction with nursing care, nursing quality, and psychological state, and seeks to provide new intervention approaches and methods for the care of nasopharyngeal carcinoma patients.
Materials and Methods
General Information
This retrospective cohort study analyzed nasopharyngeal carcinoma patients undergoing radiotherapy and chemotherapy at our hospital between September 2022 and August 2024. After applying inclusion/exclusion criteria, 98 eligible patients were identified through electronic medical record review. Groups were defined by historical nursing approaches: Control group (n=49): Received routine standard nursing care during their treatment period; Intervention group (n=49): Received routine care plus the narrative medicine-based communication program as documented in nursing records
All data were anonymized and extracted retrospectively. The study complied with the Declaration of Helsinki and was approved by the Ethics Committee of The Eighth Affiliated Hospital of Southern Medical University (No. 2021-086) with waiver of informed consent due to the retrospective nature. A post-hoc power analysis (G*Power 3.1) confirmed 83% power to detect medium effects (d=0.63, α=0.05) in this cohort.
Inclusion and Exclusion Criteria
Inclusion Criteria
Patients diagnosed with nasopharyngeal carcinoma13 and undergoing radiotherapy and chemotherapy, able to complete the entire treatment course; no gender restrictions, all patients were adults with complete clinical records; patients were mentally stable, capable of simple communication, and had basic reading abilities; expected survival time exceeded 6 months.
Exclusion Criteria
Patients with treatment contraindications; those with severe intellectual or hearing impairments; patients with major organ diseases, tumors in other locations, or severe complications; individuals with congenital immune disorders; patients unwilling to cooperate or refusing treatment.
Methods
The control group received routine nursing care, which included nutritional support, monitoring, symptomatic treatments such as pain relief and immune enhancement, as well as standard psychological counseling.
In the observation group, a communication-based intervention program incorporating narrative medicine was implemented alongside routine care. The specific procedure was as follows. A nursing team was formed, composed of senior medical staff with over six years of clinical experience and holding at least a bachelor’s degree. The team members underwent a three-week training on the theory and implementation of a communication-based intervention program rooted in narrative medicine. This training included in-depth reading of narrative medicine materials and reflective writing exercises. Physicians were responsible for selecting and enrolling participants, as well as informing patients about their conditions and conducting pre-notification assessments. Nurses took charge of creating and implementing the narrative plans. All team members were capable of independently conducting narrative work. After thorough preparation, appropriate times and locations were chosen for one-on-one, face-to-face communication with the patients, ideally in a private room. Before the conversation, the researchers expressed empathy, respect, and support, encouraging patients to open up. The content of the communication included externalization, deconstruction, rewriting, external witnesses, and therapeutic documentation. Externalization: Naming the problem and separating it from the patient’s identity to help them view the issue more objectively, thereby enhancing their courage and sense of control over the illness. Deconstruction: Exploring the root causes of the problem, placing it within a broader social context, and understanding its impact on the individual, family, and society. This helps expand the patient’s narrative space. Rewriting: Replacing the “illness story” with “exceptional events” or side stories. During this process, questions such as
What was your previous profession? What are your skills or hobbies? How is your family situation? Who do you have the best relationship with in your family? How are your children?
Are used to guide patients to discover and utilize the positive forces in these exceptional events, which can then be applied to real-life issues, leading to behavioral changes. External witnesses: Accompanying and witnessing the patient’s story through “expression, intention, resonance, empathy, and curiosity”, enhancing the sense of ritual. For example, patients who successfully complete chemotherapy or a phase of radiotherapy can participate in a ritual to reinforce their progress, helping them feel a sense of existence and self-worth. Therapeutic documentation: Depending on the patient’s emotional needs, letters, certificates, awards, photos, videos, or crafts are used to document their emotional journey, helping patients actively shape a positive health perspective and identity.14 The intervention was conducted 1–2 times per week, each session lasting 30–40 minutes, for four consecutive weeks. After each session, the conversation content, effects, and any changes in the patient were recorded.
Observation Indicators
Data collection for all six scales was conducted at two time points: baseline (prior to the initiation of the intervention) and after the completion of the four-week nursing care intervention. Each participant required approximately 15–20 minutes to complete the full set of questionnaires. To minimize potential measurement bias associated with simultaneous administration of multiple scales, several standardized procedures were implemented. First, all scales were administered in a fixed order: Fear of Progression Questionnaire-Short Form (FoP-Q-SF), Pittsburgh Sleep Quality Index (PSQI), Cancer Fatigue Scale (CFS), Herth Hope Index (HHI), Nursing Quality Evaluation Scale, and Communication Satisfaction Questionnaire. Second, structured 5-minute breaks were provided between every two scales to reduce participant fatigue and improve data quality. Finally, all assessments were conducted in quiet, distraction-free environments during non-treatment hours to ensure optimal concentration and response accuracy.
Fear of Disease Progression
Patients were assessed using the Fear of Progression Questionnaire-Short Form (FoP-Q-SF). The questionnaire consists of 12 items divided into two dimensions: social-family and physical health. It uses a 5-point Likert scale, with total scores ranging from 12 to 60. Scores of 12–23, 24–36, and 37–60 indicate mild, moderate, and severe fear, respectively. A score above 34 suggests clinically significant fear, indicating that the fear level exceeds the normal range.
Sleep Quality
The Pittsburgh Sleep Quality Index (PSQI) was used to assess patients’ sleep quality. The scale contains 18 self-reported items divided into 7 components, with each component scored from 0 to 3. The total score ranges from 0 to 21, with higher scores indicating poorer sleep quality.
Cancer Fatigue
The Cancer Fatigue Scale (CFS), specifically designed to assess fatigue symptoms in cancer patients, was used. The scale consists of three dimensions: physical fatigue, emotional fatigue, and cognitive fatigue. All items are rated using a 5-point Likert scale. Physical fatigue scores range from 0 to 28, while emotional and cognitive fatigue scores range from 0 to 16. The total score ranges from 0 to 60, with higher scores indicating more severe fatigue symptoms.
Patient Hope
The Herth Hope Index (HHI) was used to assess patients’ mindset. The scale includes three dimensions: a positive attitude toward reality and the future (T), taking positive actions (P), and maintaining close relationships with others (I), with a total of 12 items. Each item is scored using a 4-point Likert scale, and the total score ranges from 12 to 48, with higher scores indicating a higher level of hope.
Nursing Quality
Nursing quality was evaluated across four dimensions: ward management, basic nursing care, nutritional management, and the assessment results of medical staff. The first three dimensions have a total score of 50 points each, with higher scores indicating better nursing quality in that dimension. The medical staff assessment results include theoretical knowledge (ward management standards, methods of complication prevention and treatment, and key aspects of quality control) and practical skills (intubation, disinfection, and puncture site care). The total score from both theory and practice is 100 points.
Communication Satisfaction
Communication satisfaction was assessed using the Cancer Clinical Patient-Provider Communication Satisfaction Questionnaire (Nurse Version). The questionnaire covers three dimensions: information exchange, communication methods, and communication performance, along with an overall satisfaction rating. The total score ranges from 14 to 56 points, with higher scores indicating higher satisfaction.
Data Analysis
Image processing was conducted using GraphPad Prism 8 software. Data from the study were organized and analyzed using SPSS 26.0. Measurement data were expressed as ( ), and intergroup comparisons were made using the t-test. Count data were expressed as [n(%)], and comparisons between groups were made using the X² test. A P-value of <0.05 was considered statistically significant.
), and intergroup comparisons were made using the t-test. Count data were expressed as [n(%)], and comparisons between groups were made using the X² test. A P-value of <0.05 was considered statistically significant.
Results
Baseline Data
In the observation group, there were 49 participants, including 27 males and 22 females. Their ages ranged from 25 to 70 years, with an average age of 44.71±6.82 years. Regarding educational background, 8 participants had a junior high school education or below, 22 had graduated from high school, and 19 had an associate degree or higher. In the control group, there were also 49 participants, including 25 males and 24 females. Their ages ranged from 25 to 70 years, with an average age of 45.19±7.18 years. As for educational background, 5 participants had a junior high school education or below, 23 had graduated from high school, and 21 had an associate degree or higher. There were no significant differences in baseline data between the two groups, making them comparable (P>0.05). See Table 1.
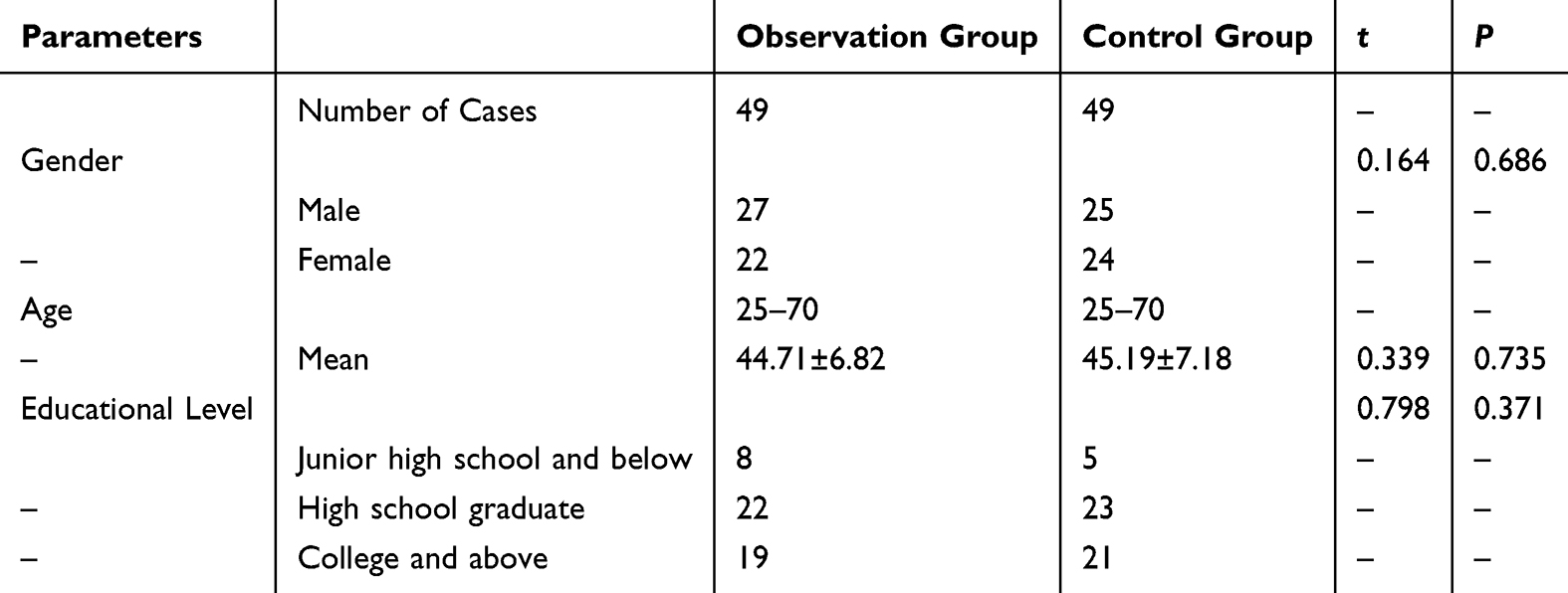 |
Table 1 Comparison of Baseline Data Between the Two Groups |
Fear of Disease Progression (FoP-Q-SF)
After the intervention, patients in the observation group reported significantly lower total FoP-Q-SF scores (33.53 ± 5.11) compared to the control group (43.11 ± 4.56), indicating reduced fear related to disease progression (P < 0.001).
In subscale analysis, the physical health dimension score was significantly lower in the observation group (19.22 ± 2.18) versus the control group (23.18 ± 2.07; P < 0.001). Similarly, the social and family dimension score was lower in the observation group (14.81 ± 2.13) compared to the control group (20.09 ± 2.12; P < 0.001). See Figure 1.
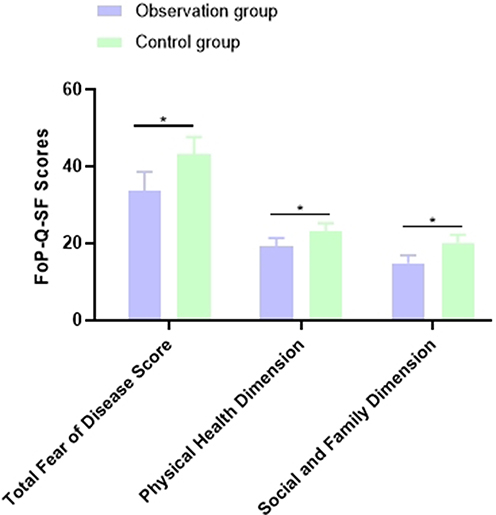 |
Figure 1 Comparison of FoP-Q-SF Scores Between the Two Groups. Note: *Indicates a significant difference, P<0.05. |
Sleep Quality (PSQI)
At baseline, PSQI scores were similar between groups (Observation: 18.36 ± 2.48; Control: 18.69 ± 2.11; P = 0.470). After the intervention, the observation group demonstrated significantly improved sleep quality, with a PSQI score of 11.25 ± 1.00 compared to 15.41 ± 1.96 in the control group (P < 0.001). See Figure 2.
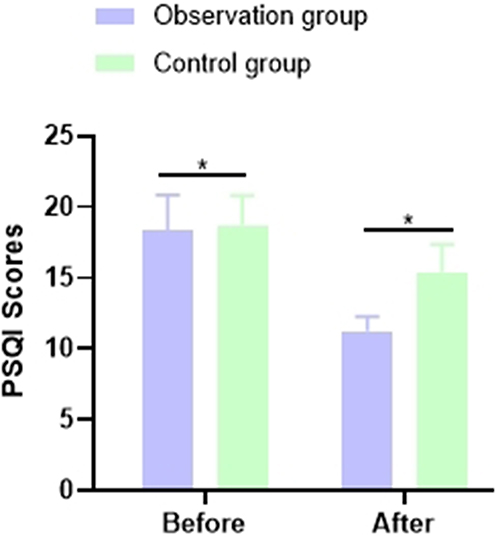 |
Figure 2 Comparison of PSQI Scores Before and After the Intervention Between the Two Groups. Note: *indicates a significant difference, P<0.05. |
Cancer Fatigue Scale (CFS)
After the intervention, patients in the observation group demonstrated significantly lower fatigue levels compared to those in the control group across all dimensions of the Cancer Fatigue Scale (CFS). Specifically, the mean physical fatigue score in the observation group was 13.18 ± 1.56, notably lower than the control group’s 17.02 ± 1.74 (P < 0.001). Similarly, scores for cognitive fatigue (5.62 ± 1.33 vs 8.35 ± 2.03, P < 0.001) and emotional fatigue (9.68 ± 1.24 vs 10.81 ± 1.62, P = 0.001) were significantly reduced in the observation group. The total fatigue score also showed a marked improvement, with the observation group averaging 28.23 ± 2.11 compared to 35.94 ± 2.76 in the control group (P < 0.001). See Figure 3.
 |
Figure 3 Comparison of CFS Scores Between the Two Groups. Note: *Indicates a significant difference, P<0.05. |
Patient Mindset
There were no significant differences in baseline HHI scores (Observation: 24.03 ± 4.25; Control: 24.11 ± 4.12; P = 0.91).
However, after the intervention, the observation group exhibited a significant increase in hope level, with a mean HHI score of 33.45 ± 4.21, compared to 25.56 ± 4.56 in the control group (P < 0.001). See Figure 4.
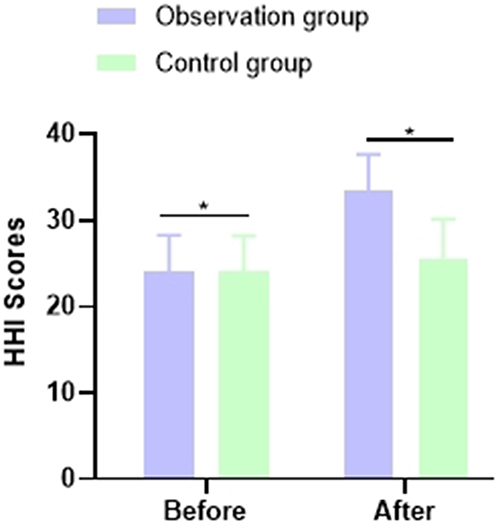 |
Figure 4 Comparison of HHI Scores Before and After the Intervention Between the Two Groups. Note: *Indicates a significant difference, P<0.05. |
Nursing Quality
The observation group demonstrated significantly higher scores in nursing quality across all evaluated domains compared to the control group (P < 0.001). Specifically, the mean score for ward management was 45.11 ± 3.41 in the observation group versus 40.92 ± 3.66 in the control group. In the domain of basic nursing, scores were 46.24 ± 2.69 and 41.87 ± 2.75, respectively. For nutrition management, the observation group scored 46.83 ± 1.96, notably higher than the control group’s 42.16 ± 2.01. Staff assessment scores also reflected a similar trend, with the observation group scoring 93.84 ± 2.47, while the control group scored 86.39 ± 3.12. Additionally, communication satisfaction was markedly better in the observation group, with a score of 51.56 ± 1.82 compared to 45.63 ± 2.09 in the control group (t = 15.58, P < 0.001). See Table 2.
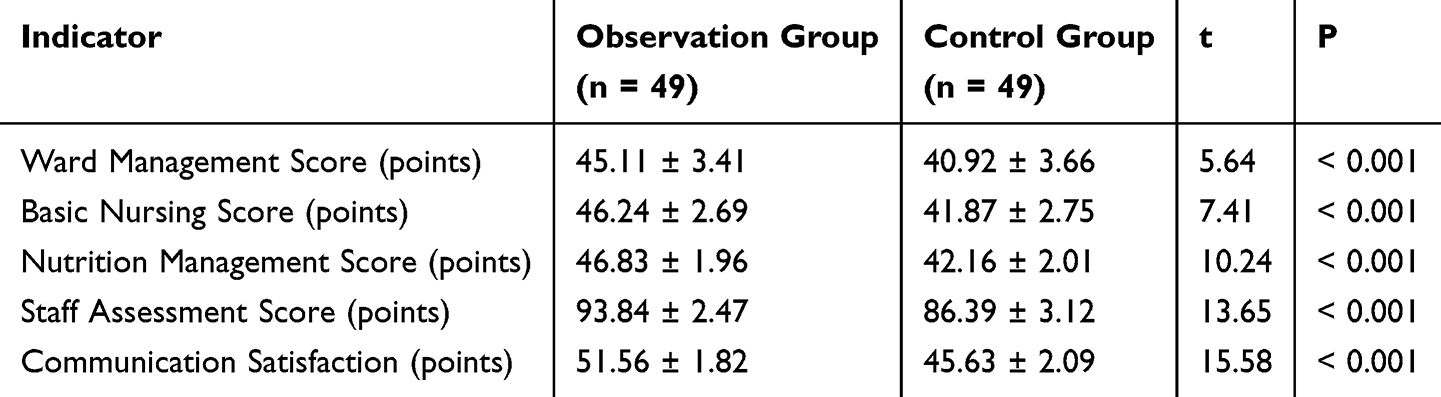 |
Table 2 Comparison of Nursing Quality and Communication Satisfaction Scores |
Discussion
This study evaluated the impact of a nurse-patient communication intervention program based on narrative medicine theory on the nursing quality of nasopharyngeal cancer patients undergoing radiotherapy and chemotherapy. The results showed that the intervention group significantly outperformed the control group in various aspects, supporting the effectiveness of narrative medicine interventions in improving nursing quality and enhancing patients’ psychological well-being.
Firstly, after the intervention, the Fear of Progression Questionnaire-Short Form (FoP-Q-SF) scores in all dimensions were significantly lower in the observation group, while the Hope Index (HHI) scores were significantly higher than those in the control group. This suggests that nurse-patient communication guided by narrative medicine theory can effectively reduce patients’ fear of disease progression while enhancing their sense of hope and positive emotions. The nurse-patient communication intervention program based on narrative medicine theory is rooted in the concept of humanized care services. By deeply understanding the patient’s personal stories and emotional experiences through dialogue and observation, nurses are able to care for the patient’s emotions and understand their personalities and true desires. Compared to conventional nursing care, this approach not only allows patients to feel warmth and establish a trusting nurse-patient relationship but also enables nurses to fully understand the patient and their family, which helps nurses think about how to inform the patient of their diagnosis and to prepare well for that process.15,16 When cancer patients learn about their diagnosis, they often experience negative emotions such as fear or denial. The nurse-patient communication intervention program based on narrative medicine theory helps patients express their emotions and reflect through storytelling, which is beneficial for their treatment. When patients narrate the details of their illness and traumatic events, they often reveal not only physical suffering but also psychological distress, such as feelings of helplessness, fear, confusion, and difficulty in self-acceptance. During the narrative process, the nurse’s listening, attention, and positive responses help the patient feel cared for and inspired to think about their story from different perspectives, discover their own potential, and try new approaches. This not only helps patients heal from trauma, establish positive psychological defenses, and better cope with the stress of illness, thereby reducing their fear of disease recurrence, but also promotes self-acceptance and restores the courage to live. Enhancing psychological support and emotional recognition also helps patients increase hope for the future and adopt a more positive attitude towards treatment.17,18
Moreover, recent studies focusing specifically on nasopharyngeal carcinoma (NPC) have demonstrated that patients often suffer high levels of psychological distress following chemoradiotherapy. Shafqat et al19 reported that anxiety and fear of recurrence were particularly elevated in the first six months post-treatment. McDowell et al20 also highlighted the persistent impact of treatment-related toxicities on mental health in NPC patients. These findings underscore the need for targeted psychosocial interventions, such as narrative-based communication, to improve mental well-being during and after treatment.
In recent years, the concept of hope has become a focal point in psychological research on cancer patients. Hope has a powerful motivating effect, helping patients tap into their inner potential, overcome difficulties, and eliminate negative emotions. Through narrative, patients can release their illness stories, which not only alleviates physical suffering but also soothes psychological anxiety and fear, generating sustained positive energy.
Secondly, the Pittsburgh Sleep Quality Index (PSQI) and the Cancer Fatigue Scale (CFS) scores in all dimensions were significantly lower in the observation group than in the control group. This indicates that the intervention effectively improved patients’ sleep quality and alleviated their physical, cognitive, and emotional fatigue. Good nurse-patient communication and emotional support help relieve sleep problems caused by the illness and treatment, improving overall sleep quality. Through regular individualized communication and emotional support, patients feel more understood and supported in managing fatigue symptoms, thereby improving their fatigue experience. The nurse-patient communication intervention program based on narrative medicine theory is an innovative psychological intervention model that applies postmodern psychological therapy concepts and methods to clinical nursing. It not only focuses on the illness itself but also on the psychological suffering caused by the illness.21,22
In cancer care, healthcare professionals’ responsibilities go beyond basic care and symptom control; they also need to engage sincerely with the patient’s inner world, helping them discover overlooked aspects of their life story, providing spiritual encouragement and comfort. Ultimately, the nurse-patient communication intervention program based on narrative medicine theory helps patients face their illness with greater courage and optimism.23,24 This approach organically combines psychological support, nursing care, and humanistic concern, allowing healthcare providers to see not just the disease but the vibrant life behind it. In terms of quality of life, previous studies have found that NPC patients experience significant impairments in physical functioning, emotional role limitations, and social well-being during radiotherapy.25–27 The narrative medicine-based approach, by improving sleep and reducing fatigue, directly contributes to enhancing these quality-of-life domains.
Finally, the nursing quality scores of patients in the intervention group were significantly higher than those in the control group. Through regular individualized communication and emotional support, patients in the intervention group received more attention and support during the nursing process, as reflected in the nursing quality evaluation. Studies have shown that a good nurse-patient relationship and effective communication can significantly improve nursing quality and enhance the overall care experience of patients. The results demonstrated that the nursing satisfaction of patients in the intervention group was significantly higher than that of the control group. This indicates that nurse-patient communication guided by narrative medicine theory enables healthcare professionals to better understand and respond to patients’ emotional needs, thereby increasing patient satisfaction with nursing services. Narrative medicine emphasizes interaction between healthcare professionals and patients, helping patients express their emotions and experiences through deep communication, making them feel more cared for in the nursing service.28,29 The improvement in nursing satisfaction not only reflects patients’ recognition of the nursing service but also helps boost their confidence and adherence to treatment.30,31
The results of this study are consistent with previous research, supporting the application value of narrative medicine in clinical nursing. Narrative medicine not only focuses on the disease itself but also on patients’ life stories and emotional experiences. By listening to and responding to patients’ stories, it is possible to more comprehensively meet their nursing needs.
However, this study also has several limitations. First, the sample size was relatively small, which may limit the generalizability of the findings to the broader nasopharyngeal cancer population. Second, the study used a retrospective cohort design without randomization or blinding, which may introduce selection and observer bias. Third, the follow-up period was limited to four weeks, so long-term effects of the intervention could not be evaluated. Future studies should adopt randomized controlled trial designs with larger sample sizes and extended follow-up periods to validate and expand on these findings.
Conclusion
In conclusion, nurse-patient communication interventions based on narrative medicine theory, by strengthening communication between healthcare professionals and patients, can help patients better understand the treatment process, reduce their fear of the disease, alleviate anxiety during treatment, enhance their confidence and adherence to treatment, alleviate cancer-related fatigue, improve sleep quality and psychological well-being, and thus improve nursing quality and patients’ overall quality of life. Patient satisfaction with nurse-patient communication also increases, demonstrating high clinical application value. It is recommended to promote this intervention model in clinical practice to further optimize patient care experiences and treatment outcomes.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Funding
Fund Project: 2023 Foshan Self-funded Science and Technology Innovation Project (2320001007478).
Disclosure
The authors declare that they have no competing interests.
References
1. Chen YP, Ismaila N, Chua MLK, et al. Chemotherapy in combination with radiotherapy for definitive-intent treatment of stage II-IVA nasopharyngeal carcinoma: CSCO and ASCO Guideline. J clin oncol. 2021;39(7):840–859. doi:10.1200/JCO.20.03237
2. Tang LL, Chen YP, Chen CB, et al. The Chinese Society of Clinical Oncology (CSCO) clinical guidelines for the diagnosis and treatment of nasopharyngeal carcinoma. Cancer Commun. 2021;41(11):1195–1227. doi:10.1002/cac2.12218
3. Guan S, Wei J, Huang L, Wu L. Chemotherapy and chemo-resistance in nasopharyngeal carcinoma. Eur J Med Chem. 2020;207:112758. doi:10.1016/j.ejmech.2020.112758
4. Lee HM, Okuda KS, González FE, Patel V. Current perspectives on nasopharyngeal carcinoma. Adv Exp Med Biol. 2019;1164:11–34. doi:10.1007/978-3-030-22254-3_2
5. Van Khac P, Doanh VT, Thao MT, et al. Optimizing intensity-modulated radiation therapy for stage II nasopharyngeal cancer: a comparative study of 7-field and 9-field treatment plans. Radiat Phys Chem. 2025;236:112700. doi:10.1016/j.radphyschem.2025.112700
6. Phat LT, Thao MT, Kien TT, et al. Dosimetric analysis of beam number variations in IMRT for head-and-neck, breast, and pelvic cancers using Halcyon. Radiat Phys Chem. 2025;236:112755. doi:10.1016/j.radphyschem.2025.112755
7. Zmijewski P, Lynch KA, Lindeman B, Vetter TR. Narrative medicine: perioperative opportunities and applicable health services research methods. Anesthesia Analg. 2022;134(3):564–572. doi:10.1213/ANE.0000000000005867
8. Su ZY, Siak PY, Lwin YY, Cheah SC. Epidemiology of nasopharyngeal carcinoma: current insights and future outlook. Cancer Metastasis Rev. 2024;43(3):919–939. doi:10.1007/s10555-024-10176-9
9. Wise M, Marchand LR, Roberts LJ, Chih MY. Suffering in advanced cancer: a randomized control trial of a narrative intervention. J Palliat Med. 2018;21(2):200–207. doi:10.1089/jpm.2017.0007
10. Crawford R, Sikirica S, Morrison R, et al. Correction: the patient experience of acute lymphoblastic leukemia and its treatment: social media review. JMIR Cancer. 2023;9:e54665. doi:10.2196/54665
11. Mnejja W, Nouri O, Fourati N, et al. État des lieux et perspectives thérapeutiques pour les carcinomes nasopharyngés localement évolués [Current management and perspectives for locally advanced nasopharyngeal carcinoma]. Cancer Radiotherapie. 2022;26(5):730–735. doi:10.1016/j.canrad.2021.11.0269
12. Scott-Conner CEH, Agarwal D. Applications of narrative medicine to surgical education. Am Surg. 2022;88(12):2851–2856. doi:10.1177/0003134821102985110
13. Fenstermacher E, Longley RM, Amonoo HL. Finding the story in medicine: the use of narrative techniques in psychiatry. Psychiatr Clin North Am. 2021;44(2):263–281. doi:10.1016/j.psc.2021.03.006
14. Paul TK, Reddy Y, Gnanakumar A, et al. Narrative medicine interventions for oncology clinicians: a systematic review. Support Care Cancer. 2024;32(4):241. doi:10.1007/s00520-024-08434-1
15. Lanphier E. Narrative and medicine: premises, practices, pragmatism. Perspect Biol Med. 2021;64(2):211–234. doi:10.1353/pbm.2021.001314
16. Launer J, Wohlmann A. Narrative medicine, narrative practice, and the creation of meaning. Lancet. 2023;401(10371):98–99. doi:10.1016/S0140-6736(23)00017-X
17. Cuestas E. Medicina narrativa [Narrative medicine]. Revista de la Facultad de Ciencias Medicas. 2012;69(2):75–76. doi:10.31053/1853.0605.v69.n2.21336
18. Nowaczyk MJ. Narrative medicine in clinical genetics practice. Am J Med Genet A. 2012;158A(8):1941–1947. doi:10.1002/ajmg.a.35482
19. Shafqat S, Munshi MS, Alam MS, et al. Assessment of core and bridge symptoms in psychiatric disorders and depression in patients with nasopharyngeal carcinoma. Assessment. 2024;55(12):1.
20. McDowell L, Corry J, Ringash J, et al. Quality of life, toxicity and unmet needs in nasopharyngeal cancer survivors. Front Oncol. 2020;10:930. doi:10.3389/fonc.2020.00930
21. Barber S, Moreno-Leguizamon CJ. Can narrative medicine education contribute to the delivery of compassionate care? A review of the literature. Med Humanit. 2017;43(3):199–203. doi:10.1136/medhum-2017-011242
22. Wallace CL, Trees A, Ohs J, Hinyard L. Narrative medicine for healthcare providers: improving practices of advance care planning. Omega. 2023;87(1):87–102. doi:10.1177/00302228211015596
23. Zhan Z-J, Huang H-Y, Xiao Y-H, et al. Anxiety and depression in nasopharyngeal carcinoma patients and network analysis to identify central symptoms: a cross-sectional study from a high-incidence area. Radiother Oncol. 2024;197:110324. doi:10.1016/j.radonc.2024.110324
24. Wang M. Analysis of the current status and influencing factors of oral health-related quality of life in nasopharyngeal carcinoma patients undergoing chemoradiotherapy. J Nurs. 2024;3(2):1–12.
25. Manne SL, Hudson SV, Preacher KJ, et al. Prevalence and correlates of fear of recurrence among oral and oropharyngeal cancer survivors. J Cancer Survivorship. 2025;19(1):66–77.
26. Luo M, Lin S, Li Z, et al. The mediating role of loneliness between psychological resilience and health-related quality of life among patients with nasopharyngeal carcinoma: a cross-sectional study using structural equation modeling. BMC Psychiatry. 2024;24(1):668. doi:10.1186/s12888-024-06036-z
27. Zhang H, Liu F. Predictive nursing versus routine nursing on health status, cancer-related fatigue and psychological state of patients with pancreatic cancer undergoing chemotherapy. J Mod Nurs Pract Res. 2023;3(1):3. doi:10.53964/jmnpr.2023003
28. Jiang J, Yan M-H, Fan -Y-Y, et al. Psychosocial adjustment experiences among nasopharyngeal carcinoma survivors: a qualitative study. Cancer Nurs. 2025;48(4):E230–E237. doi:10.1097/NCC.0000000000001312
29. Alghamdi NS, Rammal A, Alzahrani RM, et al. Health-related quality of life and psychological distress status in survivors of nasopharyngeal carcinoma: a retrospective study. Cureus. 2024;16(10):1.
30. Charon R. The patient-physician relationship. Narrative medicine: a model for empathy, reflection, profession, and trust. JAMA. 2001;286(15):1897–1902. doi:10.1001/jama.286.15.1897
31. Guthrie E, Charon R. Disability and narrative medicine: challenges and opportunities. Dev Med Child Neurol. 2024;66(2):149–154. doi:10.1111/dmcn.15685
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.