Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
The Combination of Red and Blue Light, Radiofrequency and Intense Pulsed Light for the Treatment of Facial Postacne Erythema
Received 13 September 2022
Accepted for publication 26 October 2022
Published 7 November 2022 Volume 2022:15 Pages 2383—2389
DOI https://doi.org/10.2147/CCID.S389705
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Yanping Liang, Lili Li
Department of Dermatology, People’s Hospital of Guangxi Zhuang Autonomous Region, Nanning, People’s Republic of China
Correspondence: Lili Li, Department of Dermatology, People’s Hospital of Guangxi Zhuang Autonomous Region, 6 Taoyuan Road, Nanning, 530021, People’s Republic of China, Tel +8618777190925, Email [email protected]
Introduction: Postacne erythema, also referred to as postinflammatory erythema, is a common sequela in acne patients. At present, there is no specific treatment for postacne erythema, and some treatment drugs can even aggravate facial erythema.
Objective: Our research sought to evaluate the efficacy of a combination therapy of LED red and blue light, radiofrequency (RF) and intense pulsed light (IPL) for the treatment of postacne erythema.
Methods: Patients were treated with red and blue light for 2 weeks, followed by RF for 4 treatments over 8 weeks. Finally, patients were treated with intense pulsed light for 16 weeks. Therapeutic outcomes were evaluated by erythema index, postacne erythema severity grading and clinical photography.
Results: After 3 stages of treatment, the percentage of excellent subjects was 79.2%, the percentage of good subjects was 17.2%, and the total effective rate was 96.4%. The mean erythema index decreased from 496.17± 79.11 to 89.32± 81.58 (p< 0.01) after treatment. The postacne erythema lesions were rated clear in 22.4%, faint erythema in 74.4%, dull red in 2.8% and deep red only in 0.4% of subjects after three-stage treatments.
Conclusion: Our results show that the combination of red and blue light therapy, RF therapy and IPL therapy is more effective than other treatments reported for facial postacne erythema.
Keywords: postacne erythema, red and blue light, radio-frequency, intense pulsed light
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Zhang has been published for this article.
Introduction
Acne is a common skin disease characterized by pimples on the face, chest, and back.1 Several interrelated factors lead to the occurrence of acne, including genetic background, abnormal follicular keratinization, sebum secretion, colonization of Cutibacterium acnes (C.acnes) and inflammation. Recently, the study of acne pathogenesis has focused on inflammatory processes that occur in both early- and late-stage acne lesions.2 Therefore, acne treatments should focus on the suppression of inflammation.3,4 Postacne erythema, also referred to as postinflammatory erythema, is a common sequela in acne patients.5 It is defined as lesions consisting of telangiectatic and erythematous macules, which occur as a result of skin inflammation.5 Some postacne erythema lesions may improve with time, but persistent postacne erythema has a substantial impact on the patient’s appearance and psychology. At present, there is no specific treatment for postacne erythema, and some treatment drugs can even aggravate facial erythema.6 Although the usual drug treatments have a certain effect on acne, the onset is slow, and the increase in the antibiotic resistance of C.acnes to the adverse effects of systemic retinoids and antibiotics is becoming an obstacle to acne treatment; the effect for postacne erythema especially is poor.
The principle of acne therapy by red and blue lights is that C.acnes absorbs the photon energy of red/blue light and activates photosensitizer molecules, mainly coproporphyrin, and a chemical reaction occurs, producing singlet oxygen and rapidly killing C.acnes.7 Blue light has the strongest bactericidal effect. Red light can reduce inflammation, promote tissue regeneration and collagen synthesis, and reduce or even eliminate erythema, reducing the formation of postacne scars and restoring skin smoothness.8
Radiofrequency (RF) is a high-frequency electromagnetic wave alternating between the RF and the infrared spectrum.9 RF treatment can release a large amount of thermal energy, which selectively acts on the deep layers of the dermis and fibrous septum, causing collagen contraction and new collagen deposition while stimulating collagen regeneration.10 In addition, the thermal energy could prevent the growth and reproduction of C.acnes, eliminate inflammation in patients, and relieve clinical symptoms such as pimples and acne.11
Intense pulsed light (IPL) is broad-spectrum light with a wavelength of 400–1200 nm, including the absorption peak of C.acnes at 400–417 nm.12 The basic mechanism of action of IPL is porphyrin activation triggered by photodynamic reactions, release of cytotoxic singlet oxygen. Yet the singlet oxygen can selective targeting of the receptor on the cell membrane of C.acnes, causing cell membrane damage and killing.8 In addition, IPL can inhibit the secretion of sebum by the sebaceous glands through photothermal action, prevent clogging of pores to a certain extent, and promote the absorption and resolution of inflammation.13
In our research, we used a combination of LED red and blue light, radiofrequency and intense pulsed light therapy to achieve the desired effect.
Methods
Subjects
We performed this study from August 2017 to August 2020. Five hundred patients, 308 men and 192 women. Inclusion criteria: Their ages ranged from 18 and 37 (average, 21.1±4.81), with postacne erythema on both sides and skin types III–V were enrolled. Exclusion criteria: 1. Pregnant or lactating women; 2. Patients who took isotretinoin within 6 months before treatment, used antibiotics systematically within 1 month before treatment, used external acne medication within 2 weeks before treatment, used contraceptives or photosensitizing drugs systematically, or had a history of photosensitivity or scars; 3. Patients who underwent chemical ablation or any type of laser therapy within 3 months before treatment; 4. Patients with severe heart, liver, kidney and other visceral diseases, tumors or mental disorders; 5. Patients with other facial skin diseases, such as seborrheic dermatitis, eczema, actinic dermatitis, skin infections, etc., that may interfere with the judgment of curative effect; and 6. Patients who refused to sign the consent form.
Treatment
The treatment methods included LED red and blue light therapy, RF therapy and IPL therapy. The specific methods are as follows: 1. Red and blue light therapy: A 460 nm blue light and 635 nm red light (Lifotronic, 87C) were used. The patient wore goggles and lay in the supine position. The red and blue light therapy instrument treatment probe was placed vertically approximately 10 cm above the patient’s cheek acne area. The blue and red light irradiation power densities were 20 mW/cm2 and 40 mW/cm2, respectively. The irradiation time was 20 min/session. The radiation dose was adjusted according to the degree of facial acne. The treatment took place every other day, with alternating red and blue light treatments, over the course of 2 weeks. 2. RF therapy: A GP699A radiofrequency treatment instrument (Jinweiyuan Technology Co., Ltd.) was used; the RF was 1.15 ± 0.02 MHz, and the energy range was 10–500 J. Based on the patient’s condition, we observed the patient’s RF adaptability, gradually increased the parameters, and set the energy range where the patient could adapt and receive the best effect. The duration of each treatment was 20 to 30 minutes. After treatment, facial skin was cleaned in a timely manner. If there was slight redness and swelling in the treatment area, the area was cooled with ice packs. The treatment was performed once every 2 weeks, and all patients underwent treatment 4 times. 3. IPL therapy: The treatment device was a unique Queen-93 with a wavelength of 560 nm. Before the operation, the patient’s face was cleaned, cold gel was applied, and the patient put on an eye mask. An appropriate filter was selected, and the treatment head was placed close to the patient’s face. The number of treatment pulses was set to 2, the delay was set to 40 ms, and the energy density was maintained in the range of 16 to 22 J/cm2 (pulse delay time, pulse width, and energy density were adjusted appropriately according to the patient’s facial acne). The patient received IPL treatment once a month, and 4 treatments were set as the course of treatment.
Clinical Assessments
Therapeutic outcomes were evaluated by erythema index, postacne erythema severity grading and clinical photography after the end of LED red and blue light treatment (the second week), after the end of RF treatment (the tenth week), after the first 2 IPL treatments (the 18th week) and after the second 2 IPL treatments (the 26th week).
The primary objective of the study was to demonstrate improvement in facial postacne erythema as determined by the total effective rate of treatment of postacne erythema lesions. The following scale was used: excellent: improvement from baseline, >90%; good: improvement from baseline, 60%-89%; fair: improvement from baseline, 30%-59%; and poor: improvement from baseline, <30%. The total effective rate percentage was calculated as (number of excellent subjects + number of good subjects)/total subjects × 100%.
The erythema index was measured with a DSM II ColorMeter (Cortex Technology, Denmark) on three selected postacne erythema lesions per subject, averaging the results. The color of postacne erythema lesions was quantified into four severity grades by the primary investigator, described as follows: 0=clear, none; 1=faint erythema, light pink; 2=dull red, clearly distinguishable; and 3=deep red.
Clinical improvements in postacne erythema were determined using a five-point grading scale (1=0-10%; 2=11-25%; 3=26-50%; 4=51-75%; and 5≥75% improvement). Assessment was performed by a blinded evaluation panel consisting of three dermatologists using recorded clinical photographs.
Safety Assessment
Adverse events were recorded following each treatment and at all follow-up visits. Possible side-effects during and after treatment including erythema, edema, pruritus, burning sensation, burns and pain were recorded. Subjects were asked to report any complications during the treatment period.
Statistical Analysis
Data are expressed as the means ± standard deviations. Data were analyzed using SPSS software (version 16.0; SPSS Inc., Chicago, IL, USA). p<0.05 was considered statistically significant.
Results
All five hundred subjects completed the treatment and follow-up period.
Effective Rate of Treatment of Postacne Erythema Lesions
Five hundred patients received the combination therapy. Treatment effects were recorded at weeks 2, 10, 18, and 26. The results are shown in Table 1. After the 3 stages of treatment, excellent subjects accounted for 79.2% of the total patients, good subjects accounted for 17.2% of the total patients, and the total effective rate was 96.4%.
 |
Table 1 Effective Rate of Treatment of Post-Acne Erythema Lesions |
Erythema Index
Erythema indices decreased after the first stage of treatment. Mean erythema index decreased from a mean value of 496.17±79.11 to 419.56±80.78 after the first treatment. Moreover, the erythema indices indicated a significant decrease starting from the second stage of treatment until the third stage of treatment. The mean erythema indices were 325.44±81.21 (p<0.05) at the tenth week, 198.14±77.82 (p<0.01) at the 18th week and 89.32±81.58 (p<0.01) at the 26th week. This corresponded to a 15.44% reduction after the first treatment stage, 34.41% after the second treatment stage, 60.07% at the 18th week during the third treatment stage and 82.00% at the 26th week during the third treatment stage. The results are shown in Table 2.
 |
Table 2 Erythema Index at Different Stage |
Four-Point Postacne Erythema Severity Grading
Clear improvement in the mean postacne erythema severity scores was also noted after treatment. The intensity of postacne erythema significantly decreased with each successive session. The postacne erythema lesions were rated as clear in 22.4%, faint erythema in 74.4%, dull red in 2.8% and deep red only in 0.4% of subjects after third-stage treatments (Table 3 and Figure 1).
 |
Table 3 Changes in Degree of Acne Erythema Before and After Treatment |
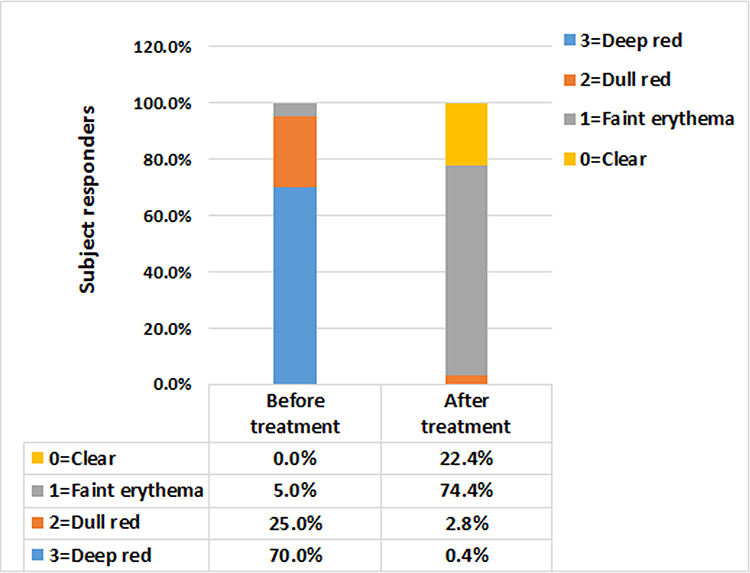 |
Figure 1 Changes in degree of acne erythema before and after treatment. Decrease in the intensity of post-acne erythema lesions is confirmed by the subsequent decrease in erythema indices after treatment. |
Patient Assessment
Figure 2 shows a 21-year-old female with facial postacne erythema, which decreased significantly after the combination therapy. The patient was asked to assess her treatment results while referring to the clinical photographs on a five-point scale (excellent, good, fair, some, little/no improvement). Figure 2 shows that her postacne erythema had excellent improvement (Grade 5) after 3 stages of treatment in terms of fading in color and reduction in the number of lesions.
 |
Figure 2 (A) Before treatment. (B) After the end of red and blue light treatment (at second week). (C) After RF treatment (at tenth week). (D) after 2 times of IPL treatments (the 18th week). (E) After 4 times of IPL treatments (the 26th week). |
Safety Assessment
Treatment-related pain was well-tolerated by all subjects. The side effects were limited to temporary erythema and edema at the treatment sites, which resolved within 1 day. No significant adverse effects such as burning or burning sensations, edema, erythema, pigmentation were observed in any of the subjects.
Discussion
Acne can be a challenging condition to treat because of the many potential consequences, including postacne erythema, postinflammatory hyperpigmentation (PIH), and scarring, which can cause huge psychological and social burdens in affected individuals even after the active disease has waned.14 Many therapies have been used to treat postacne erythema. Foreign scholars have proposed many methods, but there are still no standardized treatments.
At present, light-based technology has become a routine choice for the treatment of skin-related diseases.15,16 In acne treatment, despite various options of topical and oral drugs, there are still many patients who experience poor efficacy or adverse reactions that cannot be tolerated.17 Therefore, phototherapy technology is gradually becoming the best solution for the treatment of postacne erythema. There are many phototherapy techniques, among which visible light therapy (including red/blue light and IPL), laser therapy, and RF therapy have been widely used in the treatment of postacne erythema.
Blue light can rapidly kill C. acnes through a chemical reaction that produces singlet oxygen, which causes anti-inflammatory effects and reduces acne inflammation damage.18 Red light can reduce inflammation, promote tissue regeneration and collagen synthesis, and lessen or even eliminate erythema, reducing the formation of postacne scars and restoring skin smoothness.19 RF treatment releases a large amount of thermal energy, which selectively acts on the deep layers of the dermis and fibrous septum, inhibiting sebaceous gland secretion and causing collagen contraction and new collagen deposition while stimulating collagen regeneration. In addition, thermal energy can prevent the growth and reproduction of C. acnes, eliminate inflammation in patients, and relieve clinical symptoms such as pimples and acne.20,21 The principle of IPL in the treatment of acne erythema is selective photopyrolysis. The light energy penetrates the skin and is absorbed by hemoglobin, forming thrombosis in the blood vessel wall, stimulating the release of oxygen ions from cells and promoting the resolution of inflammation. IPL can also kill C. acnes, which removes inflammatory substances from hair follicles and reduces inflammation. In addition, IPL contains the absorption peak of hemoglobin, which can destroy hyperplastic and dilated capillaries and promote the elimination of erythema.22,23
Studies have shown that although red and blue light are effective in treating acne, due to poor penetration, this treatment is most effective at treating superficial acne, and it is difficult to treat deep acne and postacne erythema.24,25 IPL has a wide wavelength range and strong penetration, which allows it to treat deep acne. At the same time, it can inhibit inflammation, reduce inflammatory hyperplasia and dilated blood vessels, and reduce the production of postacne erythema. It has a relatively good therapeutic effect and accelerates the disappearance of erythema after acne. Therefore, the effect of combining red and blue light with intense pulsed photons is stronger.12 RF has strong penetrating power. The combination of RF energy and IPL treatment technology has also been studied at home and abroad. The absorption of RF energy by tissue depends on the water and electrolyte components in the tissue and is not affected by skin melanin content. Therefore, this treatment overcomes the epidermal barrier effect. When RF and IPL are used in combination, it is possible to activate bacterial porphyrin and inhibit sebaceous gland function due to thermal stimulation, so it is effective in the treatment of acne.8,10
Lee et al reported that 24 patients with mild to moderately severe facial acne were treated with alternating blue (415 nm) and red (633 nm) light twice a week; 11 patients (45.8%) expressed their satisfaction with the treatment as “good” or “excellent” at 2 weeks post treatment, and 18 patients (75%) rated their satisfaction as “good” or “excellent” at 8 weeks post treatment.26 Mathew et al reported 33 patients with acne-induced postinflammatory erythema who underwent treatment with the vascular mode of IPL using a 560 nm filter for three to six sessions; 78.78% of patients showed more than 50% improvement in their erythema scores, and the excellent improvement efficacy of IPL in the treatment of acne‑induced postinflammatory erythema was approximately 33.33%.12 Yu et al reported that there was an average reduction of 42% in active acne lesions after six RF treatments, and no significant adverse events were recorded during the study and follow-up periods.10 Although these individual and combined therapies have been reported, there are few reports about the combination therapy used in our study.7,12,27
In our study, we used a combination of red and blue light therapy, RF therapy and IPL therapy and achieved the desired effect. Our results show that as treatment progressed, the postacne erythema decreased significantly. The effective rate of treatment and the erythema index (325.44±81.21, p<0.05) showed a significant difference after the second stage of therapy, and there was a very significant difference in the third stage (89.32±81.58, p<0.01). After 3 stages of treatment, the total effective rate was 96.4% (482 subjects). The number of excellent subjects was 396 (79.2%), and the number of good subjects was 86 (17.2%). The facial postacne erythema of the patients significantly decreased after the combination therapy, as seen in the clinical photographs. Figure 2 shows that the patient’s postacne erythema had improved to “excellent” (Grade 5) after 3 stages of treatment in terms of fading in color and reduction in the number of lesions.
Although the previously reported therapies have achieved relatively good therapeutic effects, our combined therapy is more effective than other therapies at present. Moreover, our combined therapy did not result in obvious burning or burning sensations, edema, erythema, pigmentation or other adverse reactions at follow-up. These results show that the combination of red and blue light therapy, RF therapy and IPL therapy is superior to other reported treatments for facial postacne erythema.28 However, due to the limited time and sample size of this study, the evaluation of inflammatory acne and sequelae, such as pigmentation and scarring after acne, have not been analyzed and should be studied further.
In summary, the combination of three therapies for facial postacne erythema has a better therapeutic effect. The effect of combination therapy is worthy of clinical promotion.
Ethical Statement
The study was approved by the People’s Hospital of Guangxi Zhuang Autonomous Region and all subjects signed an informed consent form. The study was conducted in accordance with the Declaration of Helsinki Ethical Principles. The patient consent for publication of the clinical photographs.
Funding
This work was supported by funding from the GuangXi Natural Science Foundation (No. 2019GXNSFBA185018) and National Natural Science Foundation of China (No. 81960562).
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Williams HC, Dellavalle RP, Garner S. Acne vulgaris. Lancet. 2012;379(9813):361–372. doi:10.1016/S0140-6736(11)60321-8
2. Tanghetti EA. The role of inflammation in the pathology of acne. J Clin Aesthet Dermatol. 2013;6(9):27–35.
3. Chilicka K, Rogowska AM, Rusztowicz M, et al. The Effects of Green Tea (Camellia sinensis), Bamboo Extract (Bambusa vulgaris) and Lactic Acid on Sebum Production in Young Women with Acne Vulgaris Using Sonophoresis Treatment. Healthcare. 2022;10:4. doi:10.3390/healthcare10040684
4. Chilicka K, Rogowska AM, Szygula R, Rusztowicz M, Nowicka D. Efficacy of Oxybrasion in the Treatment of Acne Vulgaris: a Preliminary Report. J clin med. 2022;11:13.
5. Bae-Harboe YS, Graber EM. Easy as PIE (Postinflammatory Erythema). J Clin Aesthet Dermatol. 2013;6(9):46–47.
6. Habeshian KA, Cohen BA. Current Issues in the Treatment of Acne Vulgaris. Pediatrics. 2020;145(Suppl 2):S225–S230. doi:10.1542/peds.2019-2056L
7. Choi MS, Yun SJ, Beom HJ, Park HR, Lee JB. Comparative study of the bactericidal effects of 5-aminolevulinic acid with blue and red light on Propionibacterium acnes. J Dermatol. 2011;38(7):661–666. doi:10.1111/j.1346-8138.2010.01094.x
8. Omi T, Bjerring P, Sato S, Kawana S, Hankins RW, Honda M. 420 nm intense continuous light therapy for acne. J Cosmetic Laser Therapy. 2004;6(3):156–162. doi:10.1080/14764170410023785
9. Elsaie ML. Cutaneous remodeling and photorejuvenation using radiofrequency devices. Indian J Dermatol. 2009;54(3):201–205. doi:10.4103/0019-5154.55625
10. Yu JN, Huang P. Use of a TriPollar radio-frequency device for the treatment of acne vulgaris. J Cosmetic Laser Therapy. 2011;13(2):50–53. doi:10.3109/14764172.2011.564626
11. Min S, Park SY, Yoon JY, Kwon HH, Suh DH. Fractional Microneedling Radiofrequency Treatment for Acne-related Post-inflammatory Erythema. Acta Derm Venereol. 2016;96(1):87–91. doi:10.2340/00015555-2164
12. Mathew ML, Karthik R, Mallikarjun M, Bhute S, Varghese A. Intense Pulsed Light Therapy for Acne-induced Post-inflammatory Erythema. Indian Dermatol Online J. 2018;9(3):159–164. doi:10.4103/idoj.IDOJ_306_17
13. Bitter PH. Noninvasive rejuvenation of photodamaged skin using serial, full-face intense pulsed light treatments. Dermatol surgery. 2000;26(9):835–842. doi:10.1046/j.1524-4725.2000.00085.x
14. Zeichner JA. Optimizing topical combination therapy for the treatment of acne vulgaris. J Drugs Dermatol. 2012;11(3):313–317.
15. Racz E, Prens EP. Phototherapy of Psoriasis, a Chronic Inflammatory Skin Disease. Adv Exp Med Biol. 2017;996:287–294.
16. Singer S, Berneburg M. Phototherapy. J German Soc Dermatol. 2018;16(9):1120–1129.
17. Eichenfield DZ, Sprague J, Eichenfield LF. Management of Acne Vulgaris: a Review. JAMA. 2021;326(20):2055–2067. doi:10.1001/jama.2021.17633
18. Noborio R, Nishida E, Kurokawa M, Morita A. A new targeted blue light phototherapy for the treatment of acne. Photodermatol Photoimmunol Photomed. 2007;23(1):32–34. doi:10.1111/j.1600-0781.2007.00268.x
19. Pinto C, Schafer F, Orellana JJ, Gonzalez S, Hasson A. Efficacy of red light alone and methyl-aminolaevulinate-photodynamic therapy for the treatment of mild and moderate facial acne. Indian J Dermatol Venereol Leprol. 2013;79(1):77–82. doi:10.4103/0378-6323.104673
20. Simmons BJ, Griffith RD, Falto-Aizpurua LA, Nouri K. Use of radiofrequency in cosmetic dermatology: focus on nonablative treatment of acne scars. Clin Cosmet Investig Dermatol. 2014;7:335–339. doi:10.2147/CCID.S74411
21. Zeng R, Liu Y, Zhao W, et al. A split-face comparison of a fractional microneedle radiofrequency device and fractional radiofrequency therapy for moderate-to-severe acne vulgaris. J Cosmet Dermatol. 2020;19(10):2566–2571. doi:10.1111/jocd.13299
22. Babilas P, Schreml S, Szeimies RM, Landthaler M. Intense pulsed light (IPL): a review. Lasers Surg Med. 2010;42(2):93–104. doi:10.1002/lsm.20877
23. Piccolo D, Kostaki D, Dianzani C, Crisman G, Conforti C. Effective Intense Pulsed Light Protocol in the Treatment of Moderate to Severe Acne Vulgaris of the Chest and Back. J Clin Aesthet Dermatol. 2022;15(3):22–25.
24. Barbaric J, Abbott R, Posadzki P, et al. Light therapies for acne. Cochrane Database Sys Rev. 2016;9:CD007917. doi:10.1002/14651858.CD007917.pub2
25. Li J, Li J, Zhang L, et al. Comparison of red light and blue light therapies for mild-to-moderate acne vulgaris: a randomized controlled clinical study. Photodermatol Photoimmunol Photomed. 2022;38(5):459–464. doi:10.1111/phpp.12769
26. Lee SY, You CE, Park MY. Blue and red light combination LED phototherapy for acne vulgaris in patients with skin phototype IV. Lasers Surg Med. 2007;39(2):180–188. doi:10.1002/lsm.20412
27. Hirsch RJ, Shalita AR. Lasers, light, and acne. Cutis. 2003;71(5):353–354.
28. de Leeuw J, van der Beek N, Bjerring P, Neumann HA. Photodynamic therapy of acne vulgaris using 5-aminolevulinic acid 0.5% liposomal spray and intense pulsed light in combination with topical keratolytic agents. J Eur Acad Dermatol Venereol. 2010;24(4):460–469. doi:10.1111/j.1468-3083.2009.03447.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.