Back to Journals » Patient Preference and Adherence » Volume 16
The Co-Utilization of Oral Rehydration Solution and Zinc for Treating Diarrhea and Its Associated Factors Among Under-Five Children in Ethiopia: Further Analysis of EDHS 2016
Authors Kassa SF ![]() , Alemu TG, Techane MA
, Alemu TG, Techane MA ![]() , Wubneh CA
, Wubneh CA ![]() , Assimamaw NT
, Assimamaw NT ![]() , Belay GM, Tamir TT
, Belay GM, Tamir TT ![]() , Muhye AB, Kassie DG
, Muhye AB, Kassie DG ![]() , Wondim A, Terefe B
, Wondim A, Terefe B ![]() , Tarekegn BT
, Tarekegn BT ![]() , Ali MS
, Ali MS ![]() , Fentie B, Gonete AT
, Fentie B, Gonete AT ![]() , Tekeba B
, Tekeba B ![]() , Desta BK, Ayele AD
, Desta BK, Ayele AD ![]() , Dessie MT
, Dessie MT ![]() , Atalell KA
, Atalell KA
Received 12 February 2022
Accepted for publication 15 July 2022
Published 21 July 2022 Volume 2022:16 Pages 1713—1721
DOI https://doi.org/10.2147/PPA.S356557
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Selam Fisiha Kassa,1 Tewodros Getaneh Alemu,1 Masresha Asmare Techane,1 Chalachew Adugna Wubneh,1 Nega Tezera Assimamaw,1 Getaneh Mulualem Belay,1 Tadesse Tarik Tamir,1 Addis Bilal Muhye,1 Destaye Guadie Kassie,1 Amare Wondim,1 Bewuketu Terefe,2 Bethelihem Tigabu Tarekegn,1 Mohammed Seid Ali,1 Beletech Fentie,1 Almaz Tefera Gonete,1 Berhan Tekeba,1 Bogale Kassahun Desta,1 Amare Demsie Ayele,1 Melkamu Tilahun Dessie,1 Kendalem Asmare Atalell1
1Department of Pediatrics and Child Health Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Community Health Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Selam Fisiha Kassa, Email [email protected]
Introduction: Diarrhea causes a loss of body water and salt, which can lead to dehydration and death. The use of oral rehydration salts and zinc together is regarded as an effective treatment for diarrhea in resource-poor settings like Ethiopia. However, studies that examine the co-utilization of oral rehydration solution and zinc in the treatment of diarrhea are limited Ethiopia.
Objective: To assess the prevalence and associated factors of oral rehydration solution and zinc co-utilization to treat diarrhea in children under the age of five in Ethiopia, EDHS 2016.
Methods: Secondary data from the 2016 Ethiopia Demographic and Health Survey (EDHS) was used to investigate the prevalence and factors associated with the co-utilization of ORS and zinc to treat diarrhea in under-five children. A multilevel binary logistic regression model was fitted to identify factors associated with the co-utilization of ORS and zinc. Adjusted odds ratios (AOR) with 95% CI were calculated and used as a measure of associations, and variables having a p-value of less than 0.05 were declared as statistically significant.
Results: The national prevalence of ORS and zinc co-utilization was 16.65% (14.66%, 18.84%). Maternal educational status (AOR = 1.45; 95% CI; (1.01, 2.09)), household size (AOR = 1.53; 95% CI; 1.09, 2.16) and distance to health facilities at the community level (AOR = 1.60, 95% CI = 1.02, 2.58) were variables significantly associated with the co-use of ORS and zinc.
Conclusion: The co-utilization of ORS and zinc for the management of diarrhea was low in Ethiopia. Education, household size, and distance to health facilities at the community level were significantly associated with the co-utilization of ORS and zinc in Ethiopia.
Keywords: associated factor, children, diarrhea, Ethiopia, ORS, zinc
Introduction
Diarrhea is defined as the passage of three or more loose or watery stools within 24 hours, which might be manifested with the change in a person’s daily stool fluidity, frequency, or volume from what is considered normal.1,2 Diarrhea is the leading cause of morbidity and mortality in children under the age of five worldwide, killing an estimated 533,768 children under the age of five in 2017.3,4 According to the Ethiopian demographic and health survey report 2016, 13% of under-five children had diarrhea within two weeks preceding the survey,5 and the third killer of under-five children in Ethiopia.6 The major complications of diarrheal diseases are, dehydration, infection and malnutrition.7 Children with diarrhea is mostly dead due to dehydration, which can be treated easily with an oral rehydration solution (ORS).8
Although, the co-utilization of ORS and zinc to treat diarrhea is low in Ethiopia, previous studies showed that the co-utilization of ORS and zinc can help to reduce morbidity and mortality of children.7 According to the United Nations Children’s Fund (UNICEF) and the World Health Organization (WHO), childhood diarrhea is treated with prolonged feeding, oral rehydration solutions, and zinc supplementations,9 but less than 40% of children with diarrhea received the recommended treatment in developing countries.10 The co-use of ORS and zinc is low in Africa, ranging from 17% in Cote d’Ivoire to 38% in Niger.11 In Ethiopia, the utilization of ORS and zinc for treating diarrhea were 46% and 33% respectively.5 However, the co-utilization of ORS and zinc was not yet studied. Hence, understanding the co-utilizations of ORS and zinc as per the recommendation of WHO is important to reduce morbidity and mortality caused by diarrhea. Educational status of the mother, distance from the health facility, and occupation of the mother are some of the factors associated with the co-utilization of ORS and zinc for treating children with diarrhea.12
From 2012 to 2016, the Clinton Health Access Initiative (CHAI) worked with governments, health care providers, and communities in India and a few African nations to enhance diarrhea treatment. In certain target locations, the initiative was able to increase the combined usage of ORS and zinc.13 In the treatment of acute diarrhea, the Integrated Management of Neonatal and Childhood Illness (IMNCI) recommends these two medications. Under the leadership of the federal ministry of health’s maternal and child health directorate and nutrition section, Drivers Knowledge Test Ethiopia (DKT/E) and the Micronutrient Initiative (MI) launched a combined ORS and Zinc product to treat childhood diarrhea, which is one of Ethiopia’s leading causes of illness and child mortality.14 Health-care providers treating children with diarrhea should give their caregivers two 1-liter packets of the new ORS to use at home until the diarrhea stops, as well as enough zinc tablets to continue home treatment for 10–14 days.15 Zinc, when combined with ORS, reduces the duration and intensity of diarrhea, as well as the frequency of diarrhea over the next 2–3 months.16
Despite the fact that utilizing ORS in conjunction with zinc has numerous benefits, as demonstrated above, it is rarely used to treat diarrhea in Ethiopian children under the age of five years.17 Thus, we aimed to assess the co-utilization of oral rehydration solution and zinc for treating diarrhea and its associated factors among under-five children in Ethiopia.
Method
Study Design and Setting
A secondary analysis of nationally representative population-based cross-sectional survey was conducted to assess the co-utilization and factors associated with ORS and zinc for treating diarrhea among children with diarrhea in Ethiopia. Ethiopia is the second and the 12th most populous country in Africa and worldwide respectively, which is located in East Africa. The country has an estimated total surface area of 1.1 million square kilometers, with altitudes ranging from 125 meters below sea level in the Afar depression to 4550 meters above sea level in the Semien Mountains Ras Dejen. The study was done by using the EDHS 2016, which is the fourth national survey. The survey addresses all the 11 administrative geographical regions in Ethiopia; which are further subdivided into zones, districts, and Kebeles, the smallest administrative units. A Household Survey of EDHS was conducted by dividing each smallest administrative unit (Kebele) into enumeration areas. Then the enumeration areas was used as a sampling frame. The 2016 EDHS sample was created to offer estimates of key indicators for the entire country, as well as for urban and rural areas individually.
Study Population and Sampling Procedures
The source population of this study was all under-five children with diarrhea in Ethiopia. The study population was all under-five children with diarrhea within the last two weeks preceding the survey in Ethiopia. The study participants were selected using a two-stage stratified cluster sampling technique. In the first stage, 645 enumeration areas/clusters were selected randomly. In the second stage, a total of 28 households per cluster were selected by using a newly produced household list with an equal likelihood of systematic selection. From a total of 10,641 total deliveries, died children and those who have no diarrhea in the last two weeks were excluded. Finally, a weighted sample of 1228 women with children under the age of five who had experienced diarrhea in the last two weeks before the survey were included in the study.
Study Variables
Dependent Variables
The outcome variable of this study was the co-utilization of ORS and zinc for the management of childhood diarrhea, which was dichotomized into “yes=1” if the child uses both ORS and zinc for the management of childhood diarrhea and “no=0” if the child did not use both ORS and zinc for the management of childhood diarrhea.
Independent Variables
Socio-demographic characteristics (maternal age, child age, sex, residence, education status, marital status, and wealth quintile) and factors like health insurance coverage, distance from the health facility, household size, and media exposure were included as independent variables.14,18 In this study, media exposure was categorized as yes and no by using the variables (frequency of watching TV, reading a newspaper, and listening to the radio) from the dataset. Accordingly having media exposure was defined as if an individual was exposed to all or either of the three and having no exposure if an individual was not used at least one of those the above mentioned.
Data Management and Statistical Analysis
The data was accessed in the measure DHS at the DHSprogram.com website, through an online request after registration. The data was extracted from the Kids Record (KR) datasets. Data cleaning, weighting, recording, and analysis were done by using STATA version 14. To adjust for disproportionate samples and non-responses, sample weighting was done for each variable. Descriptive statistics such as weighted frequencies and percentages were used to summarize the data. The multilevel binary logistic regression model was fitted to identify the individual-level and community-level factors associated with the co-utilization of ORS and zinc. The intra-class correlation coefficient (ICC) was calculated to show whether there was a difference in co-utilization of ORS and zinc between clusters, and model comparison was done using deviance (−2log likelihood), the model with the lowest deviance value was the best-fitted model. Adjusted Odds Ratio (AOR) with 95% CI was calculated and used as a measure of associations. Variables with a p-value less than 0.25 in the multilevel bivariable logistic regression model were fitted into the multilevel multivariable logistic regression model. Variables with a p-value < 0.05, in the final model, were declared as significantly associated with the co-utilization of ORS and zinc for the management of childhood diarrhea. A multicollinearity test was done to rule out a significant correlation between variables. The mean variance inflation factor (VIF) was found to be 1.5 and all variables had VIF values less than 10.
Results
Socio-Demographic Characteristics of Study Participants
The total weighted sample of 1228 under-five children with diarrhea was included in this study. The majority, 1102 (89.73%) of the children were from rural. More than half, 649 (52.87%) of the children were males. More than two-thirds of children were from households with ≥5 household size. The majority, 801 (65.27%) of their family had no media exposure. About half of the participants were from high community media exposure (52.54%) and high maternal community education (50.84%). Six hundred thirty-seven (51.90%) of them were from the community with high poverty levels (Table 1).
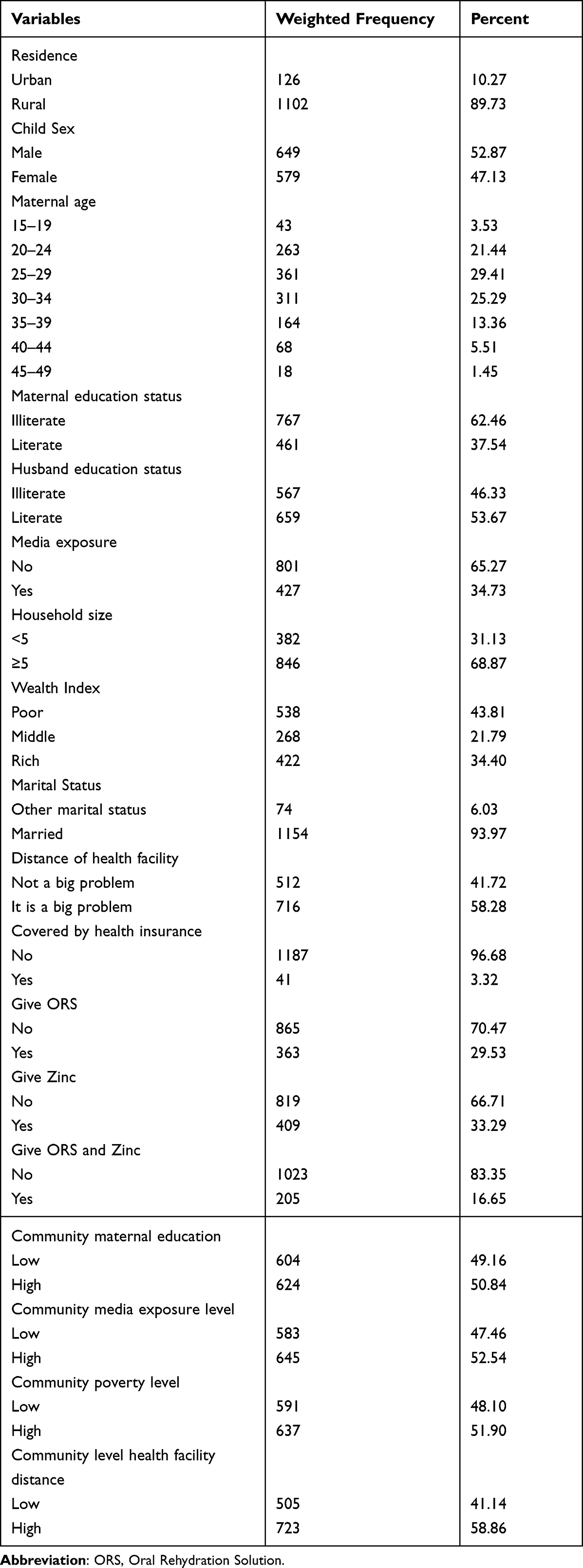 |
Table 1 Socio-Demographic Characteristics of Respondents in Ethiopia, EDHS 2016 |
Co-Utilization of ORS and Zinc
The overall co-utilization of ORS and zinc for the treatment of diarrhea among children in Ethiopia was 16.65% with a 95% CI (14.66%, 18.84%).
Random Effect Analysis
Cluster variability accounted for 17.5%of overall ORS and zinc co-utilization in the null model. In the null model, the MOR for the co-utilization of ORS and zinc was 2.21, indicating that there was a difference in the co-utilization between clusters. Children in the cluster with higher zinc utilization had a 2.21 times higher prevalence of ORS and zinc usage than those in the cluster with lower ORS and zinc utilization, which may explain if children drowned at random from various clusters. Model fitness was assessed using deviation, and the model with the lowest deviance (Model III) was chosen since it had the lowest deviance while also having the best fitness (Table 2).
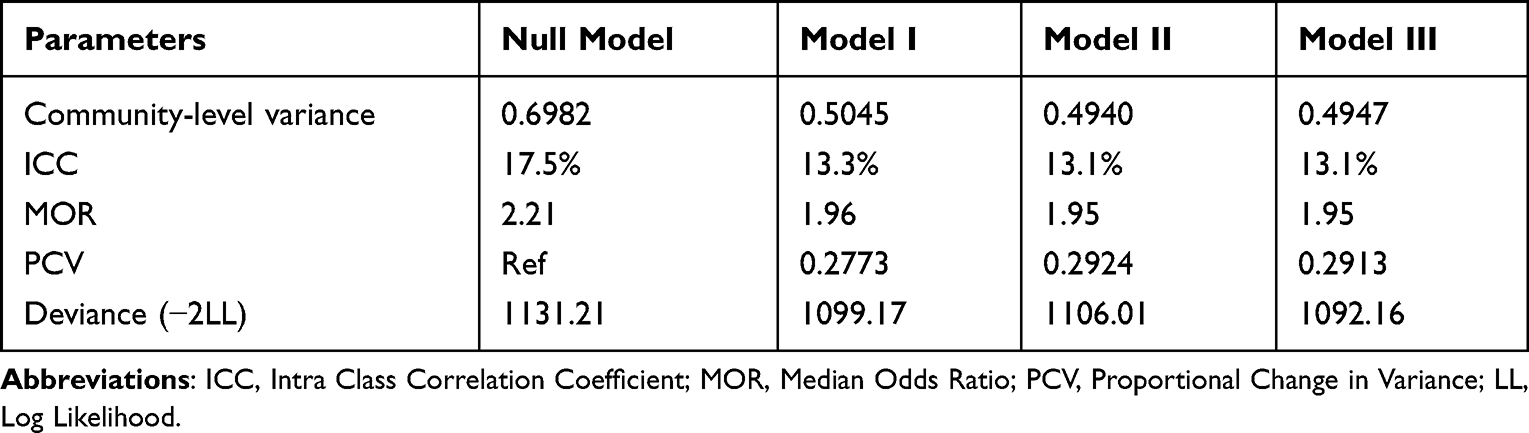 |
Table 2 Model Comparison and Random Effect Analysis results |
Determinants of Co-Utilization of ORS and Zinc Among Under-Five Children with Diarrhea
The multilevel binary logistic regression model was fitted to identify factors associated with the co-utilization of ORS and zinc for treating diarrhea among under-five children in Ethiopia. First, the crude association of independent variables (Residence, Distance to health facility, Maternal educational status, Media exposure, Wealth Index, Household size, Community health facility distance, Community level media exposure, Community level poverty status) with ORS and zinc co-utilization was assessed. Accordingly, all variables with a p-value <0.25 in the bivariable analysis were entered into the multivariable multilevel regression model (final model). Finally, maternal educational status, household size, and community health facility distance were significantly associated with the combined use of ORS and zinc (p<0.05).
When comparing mothers with formal education to mothers without formal education, the odds of using ORS and zinc during diarrheal sickness were 1.45 (AOR = 1.45; 95% CI; 1.01, 2.09) times higher.
Mothers who were from a household size of less than five were 1.53 (AOR = 1.53; 95% CI; 1.09, 2.16) times higher odds of ORS and zinc utilization for diarrhea management as compared to those mothers who were from household members greater than and equal to five. Furthermore, the odds of ORS and zinc utilization among children with short community health facility distances were 60% higher as compared to their counterparts (AOR = 1.60, 95% CI = 1.02, 2.58) (Table 3).
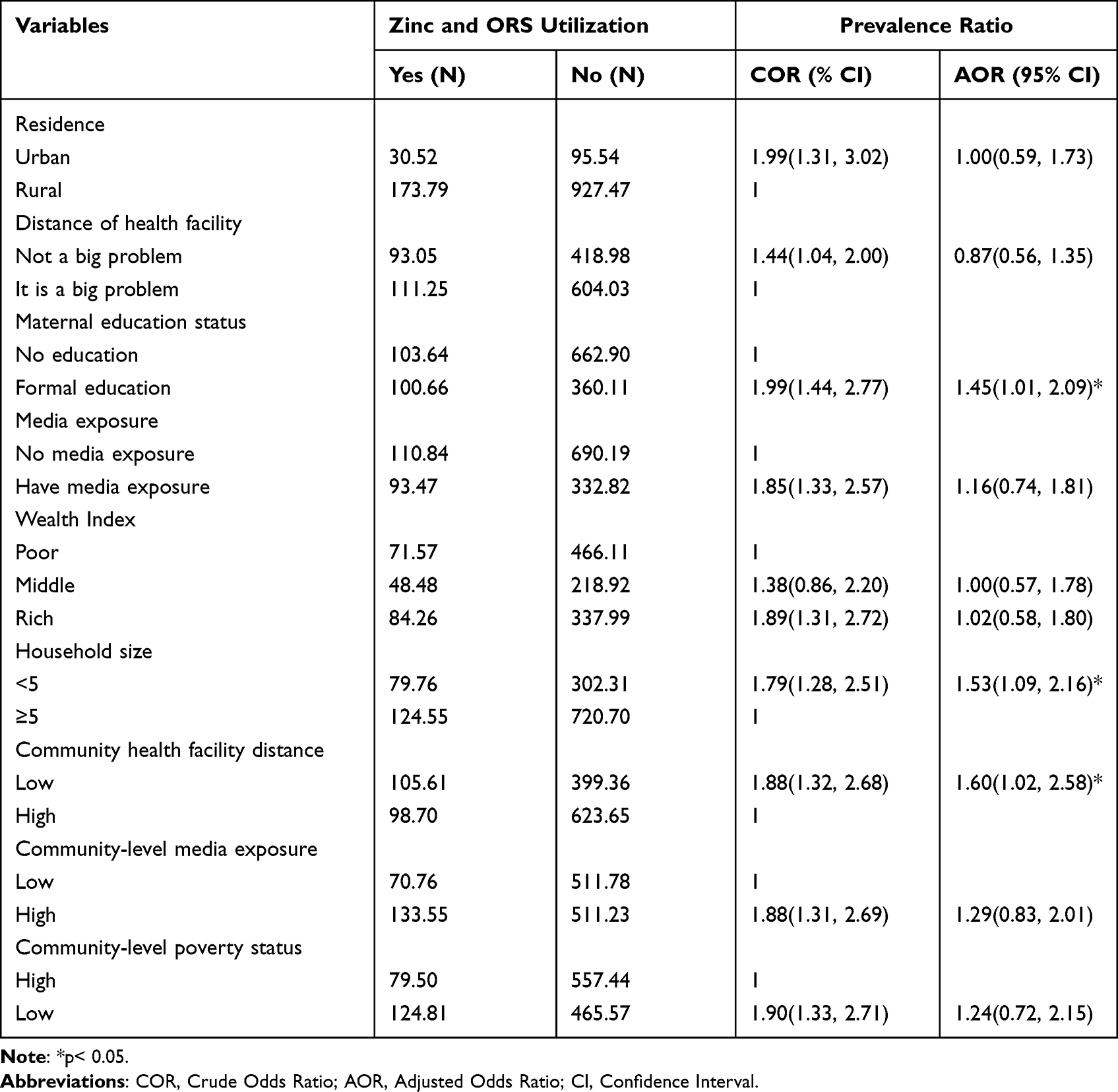 |
Table 3 Multilevel Regression Analysis of ORS and Zinc Utilization Among Under-Five Children with Diarrhea in Ethiopia |
Discussion
The World Health Organization and United Nations Children’s Fund recommend the supplementation of both ORS and zinc as primary management of diarrheal diseases in children as they can reduce the most common complication which is dehydration and also the duration, severity, and recurrence of diarrheal diseases in children.19,20 This study assessed the prevalence and associated factors of combined use of ORS and zinc for diarrhea management in under-five children using a multi-level logistic regression model. Thus, the study finding revealed that maternal education, household size, and community level distance to health facilities were found to be statistically significant factors.
The utilization of both ORS and zinc in Ethiopia was found to be 16.65% with a 95% CI of (14.66%, and 18.84%). ORS plus zinc use for acute diarrheal management was used relatively uncommonly the Ethiopian population.21 The poor adoption of ORS plus zinc in this study might be attributable to a lack of advocacy on the part of government health offices, health extension workers, non-governmental organizations, and civic groups engaged in promoting ORS plus zinc supplementation. This magnitude of combined ORS and zinc use estimate is lower than the finding done in Gujarat and Uttar Pradesh India.22 This might be because our study is national however, the studies in India were in two states and the survey was conducted after the community-based intervention.
When compared to mothers with more than or equal to five household members, mothers with a smaller household size (ie less than five) had a higher likelihood of administering ORS and zinc to their children with diarrhea. The finding is supported by a study done in Ethiopia.18 This could be because women with fewer family members have more time and are better able to care for their sick children. Furthermore, mothers in smaller households are less likely to experience parenting stress, which might affect recommended child-feeding practices and health-seeking behavior if their kid becomes ill.
The odds of giving ORS and zinc to their under-five children with diarrheal disease were higher among mothers who had formal education as compared to those who have no formal education. The finding of this study is in line with a study conducted in Nigeria,23 Ethiopia,18 and India Gujarat.22 This could be because educated women are more conscious of their children’s health and are more likely to take their sick children to the nearest health institution. Besides, the possible justification might be an educated mother is more likely than an uneducated mother to take her sick child to the doctor for treatment and follow-up, as well as to take the prescribed medication.
Community-level distance of health facilities was also found to be associated with ORS and zinc use. Those mothers who reside in the community where health facility accessibility is a big problem were less likely to seek treatment for their sick children than those who are near health institutions. This is in line with studies conducted elsewhere.24–26 This can be justified by the reason that health care availability affects the health-seeking behavior of mothers. Those who cannot access health facilities around their residence find it difficult to afford the cost of transportation for seeking health services at a distance.27,28
However, unlike a study conducted in India Uttar Pradesh,22 in which media exposure increases the utilization of combined ORS and zinc, there is no significant effect of individual and community level media exposure on combined ORS and zinc uptake in this study. This might be the difference in study population, period, and study design.
This study had both limitations and strengths. The study’s strength is that it is based on nationally representative data and uses appropriate analysis methodologies. Furthermore, this is the first study in Ethiopia to evaluate the combined use of ORS and zinc in under-five children during diarrhea therapy. As a result, we are unable to compare our findings to those of other studies due to a lack of relevant literature. However, because the study was done in a cross-sectional design, a clear cause and effect link between the combined ORS and zinc utilization and independent variables remained unknown.
Conclusion
The study found that both the individual and community level factors were associated with the outcome variable. In this study, factors like having a formal education, household size of less than five, and a short-distance community health facility were significantly associated with the use of both ORS and zinc.
Abbreviations
AOR, Adjusted Odds Ratio; CI, Confidence Interval; DHS, Demographic and Health Survey; EDHS, Ethiopian Demographic and Health Survey; ICC, Intra Class Correlation; LL, Log-likelihood; ORS, Oral Rehydration Solution; UNICEF, United Nations Children’s Fund; WHO, World Health Organization.
Ethical Consideration
The study was conducted following the guidelines outlined in the Declaration of Helsinki. Ethical clearance was obtained from the Ethical Review Board (IRB) of College of Medicine and Health Sciences, University of Gondar. Informed written consent was obtained before the interview where informed consent for children was obtained from their parents/guardians. Data access was approved after it was requested from the demographic and health survey by registering online from http://www.dhsprogram.com. All data used in this study were publicly available, and aggregated secondary data with no personal identity.
Acknowledgments
We would like to express our deepest appreciation to measure DHS for providing the data for the analysis. Above all, we are grateful to thank the Almighty God.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
There was no funding received.
Disclosure
The authors declared no conflicts of interest in relation to this work.
References
1. Olopha OO, Egbewale B. Awareness and knowledge of diarrhoeal home management among mothers of under-five in Ibadan, Nigeria. Univ J Public Health. 2017;5(1):40–45. doi:10.13189/ujph.2017.050106
2. Mosisa D, Aboma M, Girma T, Shibru A. determinants of diarrheal diseases among under five children in Jimma Geneti District, Oromia Region, Ethiopia, 2020: a case-control study. BMC Pediatr. 2021;21(1). doi:10.1186/s12887-021-03022-2
3. UNICEF D. Monitoring the situation of children and women. 2014. Available from: monitoring the situation of children and women; 2014.
4. Troeger CE, Khalil IA, Blacker BF, et al. Quantifying risks and interventions that have affected the burden of diarrhoea among children younger than 5 years: an analysis of the Global Burden of Disease Study 2017. Lancet Infect Dis. 2020;20(1):37–59. doi:10.1016/S1473-3099(19)30401-3
5. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia demographic and health survey 2016: key indicators report. Addis Ababa E, and Rockville, Maryland, USA: CSA and ICF; 2016.
6. Tesfaye TS, Magarsa AU, Zeleke TM. Moderate to severe diarrhea and associated factors among under-five children in Wonago District, South Ethiopia: a cross-sectional study. Pediatric Health Med Ther. 2020;11:437. doi:10.2147/PHMT.S266828
7. Bajait C, Thawani V. Role of zinc in pediatric diarrhea. Indian J Pharmacol. 2011;43(3):232. doi:10.4103/0253-7613.81495
8. Walker CLF, Black RE. Zinc for the treatment of diarrhoea: effect on diarrhoea morbidity, mortality and incidence of future episodes. Int J Epidemiol. 2010;39(suppl_1):i63–i69. doi:10.1093/ije/dyq023
9. Olatona F, Obrutu O, Adeniyi O. Home management of childhood diarrhea including zinc supplementation among mothers attending primary health centers in an urban community in Lagos. Trop J Health Sci. 2016;23(2):23–29.
10. Jain H, Bamnawat S. Knowledge and attitude towards oral rehydration therapy among mothers of under-five children of South Rajasthan, India. Int J Contemp Pediatr. 2016;3(2):394–397. doi:10.18203/2349-3291.ijcp20161021
11. Carvajal-Vélez L, Amouzou A, Perin J, et al. Diarrhea management in children under five in sub-Saharan Africa: does the source of care matter? A Countdown analysis. BMC Public Health. 2016;16(1):1–14. doi:10.1186/s12889-016-3475-1
12. El-Khoury M, Banke K, Sloane P. Improved childhood diarrhea treatment practices in Ghana: a pre-post evaluation of a comprehensive private-sector program. Global Health. 2016;4(2):264–275.
13. Black RE. Progress in the use of ORS and zinc for the treatment of childhood diarrhea. J Glob Health. 2019;9(1). doi:10.7189/jogh.09.010101
14. Ayele E, Tasew H, Mariye T, Teklay G, Alemayhu T, Mesfin F. Zinc utilization and associated factors among under-five children having acute diarrhea in Kebri-dehar Town, Somali Region, Ethiopia-2017. Medicine. 2020;4(1):15–19.
15. WHO/UNICEF JOINT STATEMENT. Clinical management of acute diarrhoea; 2014.
16. Omuemu VO, Ofuani IJ, Kubeyinje IC. Knowledge and use of zinc supplementation in the management of childhood diarrhoea among health care workers in public primary health facilities in Benin-City, Nigeria. Glob J Health Sci. 2012;4(2):68. doi:10.5539/gjhs.v4n2p68
17. Walker CLF, Fontaine O, Young MW, Black RE. Zinc and low osmolarity oral rehydration salts for diarrhoea: a renewed call to action. Bull World Health Organ. 2009;87:780–786. doi:10.2471/BLT.08.058990
18. Teshale AB, Liyew AM, Tesema GA. Factors associated with zinc utilization for the management of diarrhea in under-five children in Ethiopia. BMC Public Health. 2020;20(1):1–7. doi:10.1186/s12889-020-09541-4
19. World Health Organization. Clinical Management of Acute Diarrhoea: WHO. World Health Organization; 2004.
20. Yimenu DK, Kasahun AE, Chane M, Getachew Y, Manaye B, Kifle ZD. Assessment of knowledge, attitude, and practice of child caregivers towards oral rehydration salt and zinc for the treatment of diarrhea in under 5 children in Gondar town. Clin Epidemiol Global Health. 2022;14:100998. doi:10.1016/j.cegh.2022.100998
21. Hassen S, Haidar J, Bogale AL. Occurrence of diarrhea and utilization of zinc bundled with ORS among caregivers of children less than five-years in Addis Ababa, Ethiopia. J Public Health Epidemiol. 2018;10(9):348–355. doi:10.5897/JPHE2018.1029
22. Lam F, Pro G, Agrawal S, et al. Effect of enhanced detailing and mass media on community use of oral rehydration salts and zinc during a scale-up program in Gujarat and Uttar Pradesh. J Global Health. 2019;9(1). doi:10.7189/jogh.09.010501
23. Gwarzo G. Mothers’ awareness and use of zinc in under-five children with diarrhoea in North-Western Nigeria. Niger J Paediatr. 2018;45(2):81–85.
24. Adane M, Mengistie B, Mulat W, Kloos H, Medhin G. Utilization of health facilities and predictors of health-seeking behavior for under-five children with acute diarrhea in slums of Addis Ababa, Ethiopia: a community-based cross-sectional study. J Health Popul Nutr. 2017;36(1):1–12.
25. Noorali R, Luby S, Hossein Rahbar M. Does use of a government service depend on distance from the health facility? Health Policy Plan. 1999;14(2):191–197. doi:10.1093/heapol/14.2.191
26. Okwaraji YB, Cousens S, Berhane Y, Mulholland K, Edmond K, Noor AM. Effect of geographical access to health facilities on child mortality in rural Ethiopia: a community based cross sectional study. PLoS One. 2012;7(3):e33564. doi:10.1371/journal.pone.0033564
27. Musoke D, Boynton P, Butler C, Musoke MB. Health seeking behaviour and challenges in utilising health facilities in Wakiso district, Uganda. Afr Health Sci. 2014;14(4):1046–1055. doi:10.4314/ahs.v14i4.36
28. Luo L, He X, Zhang X, Shi Y. Effects of distance on health seeking behaviors of outpatients in China’s large hospitals: case of West China hospital of Sichuan University. Int J Clin Exp Med. 2016;9(6):11923–11933.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.