Back to Journals » Open Access Emergency Medicine » Volume 15
The Clinical Predictive Score for Prehospital Large Vessel Occlusion Stroke: A Retrospective Cohort Study in the Asian Country
Authors Yuksen C ![]() , Tienpratarn W
, Tienpratarn W ![]() , Treerasoradaj T, Jenpanitpong C
, Treerasoradaj T, Jenpanitpong C ![]() , Termkijwanich P
, Termkijwanich P ![]()
Received 30 November 2022
Accepted for publication 27 January 2023
Published 9 February 2023 Volume 2023:15 Pages 53—60
DOI https://doi.org/10.2147/OAEM.S398061
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Hans-Christoph Pape
Chaiyaporn Yuksen, Welawat Tienpratarn, Thitibud Treerasoradaj, Chetsadakon Jenpanitpong, Phatcha Termkijwanich
Department of Emergency Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Welawat Tienpratarn, Department of Emergency Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand, Email [email protected]
Background: Large vessel occlusive (LVO) stroke causes severe disabilities and occurs in more than 37% of strokes. Reperfusion therapy is the gold standard of treatment. Studies proved that endovascular thrombectomy (EVT) is more beneficial and decreases mortality. This study aimed to evaluate the factor associated with LVO stroke in an Asian population and to develop the scores to predict LVO in a prehospital setting. The score will hugely contribute to the future of stroke care in prehospital settings in the aspect of transferal suspected LVO stroke patients to appropriate EVT-capable stroke centers.
Methods: This study was a retrospective cohort study using an exploratory model at the emergency department of Ramathibodi Hospital, Bangkok, Thailand, between January 2018 and December 2020. We included the stroke patients aged > 18 who visit ED and an available radiologic report representing LVO. Those whose stroke onset was > 24 hours and no radiologic report were excluded. Multivariable logistic regression analysis developed the prediction model and score for LVO stroke.
Results: A total of 252 patients met the inclusion criteria; 61 cases (24%) had LVO stroke. Six independent factors were significantly predictive: comorbidity with atrial fibrillation, clinical hemineglect, gaze deviation, facial palsy, aphasia, and cerebellar sign abnormality. The predicted score had an accuracy of 92.5%. The LVO risk score was categorized into three groups: low risk (LVO score < 3), moderate risk (LVO score 3– 6), and high risk (LVO score > 6). The positive likelihood ratio to predicting LVO stroke were 0.12 (95% CI 0.06– 0.26), 2.33 (95% CI 1.53– 3.53) and 45.40 (95% CI 11.16– 184.78), respectively.
Conclusion: The Large Vessel Occlusion (LVO) Risk Score provides a screening tool for predicting LVO stroke. A clinical predictive score of ≥ 3 appears to be associated with LVO stroke.
Keywords: acute stroke, thrombectomy, clinical decision rules, emergency medical services
Introduction
Acute stroke is a common emergency problem that causes devastated disabilities such as hemiparesis, paresthesia, facial drooping, slurred speech, and other symptoms that significantly affect the population’s well-being. In 2019, 355,671 inpatients were diagnosed with stroke in Thailand who suffered from the disease.1 The key to stroke management is time. The less time lost to diagnose stroke, the less time loss of opportunity to reperfusion brain circulation, which leads to better outcomes and prevents further disabilities from ongoing brain ischemia. Statistically, over 37.3% of stroke patients are pathologically from large vessel territories of brain circulation.2
Studies on predicting large vessel stroke have been published in recent years. Multiple tools or prediction scoring systems such as VAN,3 CPSS,4 d-CPSS,5 LAMS,6,7 FAST-ED,8 3ISS,9 RACE,10 and PAST11 were based on NIHSS and the relationship between clinical presentations and large vessel stroke.12 These studies show their sensitivity of 67–85% and specificity of 76–86%.3 VAN and FAST-ED have been validated in terms of comprehensibility in later studies.13,14 The result showed no difference in scoring or evaluation, representing the practicality of these prediction scores.
From the 2019 Emergency Medical Services (EMS) record in Bangkok, 1727 patients have reached EMS who were diagnosed with stroke. In general, after dispatching the EMS team and reaching patients, transferring to the appropriate healthcare center depends on various factors such as the type of their healthcare rights, distance from scene to destination, or needs of specific centers for indicated emergent conditions, which stroke is one of the conditions, especially for large vessel stroke.15 Endovascular treatment has been praised as a better treatment choice for some indicated strokes. Unfortunately, only a few stroke centers can provide endovascular treatment in Thailand. Ramathibodi Hospital is one of the endovascular-capable stroke centers.16
According to recent studies, endovascular treatment has reduced morbidity and mortality in indicated acute large vessel stroke. The verified extended onset time of 16–24 hours for endovascular treatment compared to the much shorter time of 4.5 hours from the onset for medical thrombolytic treatment has increased the chance of treatment for the number of the stroke patient.16,17 Therefore, it will be beneficial for suspected large vessel stroke patients who reach for EMS if the EMS team is well trained and able to predict from clinical syndrome whether the stroke is large vessel territory which resulted from inappropriate transfer to a suitable stroke center.
Ramathibodi Hospital, a university-affiliated super-tertiary-care hospital in Bangkok, Thailand, is an excellent endovascular-capable stroke center. Ramathibodi has a robust guideline for stroke fast track, and the guideline for endovascular treatment in indicated large vessel stroke patients has been implemented and updated for years. Prediction of large vessel stroke in prehospital care could be the next significant improvement in stroke care in Ramathibodi Hospital. This study aimed to evaluate the factor associated with LVO stroke in an Asian population and to develop the scores to predict LVO in a prehospital setting, which could be the initial step to improving prehospital stroke care.
Methods
Study Design and Setting
This study was a diagnostic, retrospective cohort study and exploratory model conducted at the Emergency Department (ED) of Ramathibodi Hospital Bangkok, Thailand. The Faculty of Medicine approved this study, Committee on Human Rights Related to Research Involving Human Subjects, of Mahidol University’s Ramathibodi Hospital. (MURA2021/430) Due to the retrospective design, the ethics committee waived the need for informed consent.
Participants
The study participant was required to be aged >18 years and visited the ED with the final stroke diagnosis. We excluded those with these criteria; no brain and vascular imaging reports, incomplete data record, and the onset of clinical stroke were >24 hours.
Study Protocol
The eligible patients were included with the final stroke diagnosis (not specified as hemorrhage or infarction) and cerebral infarction. This data was collected from the electronic Emergency Medical Record (EMR).
For sample size estimation, we collected data from stroke patients from 01 April 2020 and 30 June 2020 (3 months). Eleven large vessel stroke patients (23.4%) and 36 non-large vessel stroke patients (76.6%). The ratio of large vessel stroke per non-large vessel stroke was 0.31. STATA version 16.0 was used to analyze the sample size with a two-sample comparison of large vessel stroke and non-large vessel stroke. The assumptions of alpha = 0.05 (two-sided test), power was 0.8, and the sample size ratio was 1:3.2. The sample size was 60 in the large vessel stroke population, and the sample size was 192 in the non-large vessel stroke population.
Data Collection
The baseline characteristics and clinical variable factors associated with LVO stroke were recorded. The variables include gender, age, underlying disease (diabetes mellitus, hypertension, dyslipidemia, cerebrovascular disease, coronary artery disease, and atrial fibrillation), first glucose level at the ED, the onset of stroke, and first NIHSS. The clinical diagnostic for LVO stroke includes consciousness, hemineglect, gaze deviation, arm weakness, leg weakness, facial drooping, language disturbance, slurred speech, and abnormal cerebellar signs.
Cerebellar signs were basic neurological examinations that advanced EMS personnel, including emergency physicians and paramedics, could perform correctly. Cerebellar signs in our study were finger to nose, nystagmus, or ataxia. We excluded ataxia caused by any weakness.
Outcome Measures
The outcome of interest was an official report of LVO stroke from a radiologist of the brain or vascular imaging (CTA/MRA). LVO stroke in our study included intracranial internal carotid artery (ICA), middle cerebral artery (only M1 and M2) occlusion in anterior circulation and intracranial basilar artery (BA), vertebral artery (VA) and posterior cerebral artery occlusion in posterior circulation. The outcome of interest was an official report of large vessel occlusion stroke from a radiologist of the brain or vascular imaging (CTA/MRA) and an official report of large vessel occlusion from interventional radiologist of emergency cerebral angiogram with mechanical thrombectomy.
Patients were then categorized into either an LVO stroke group or a non-LVO group. Finally, we developed a prediction score for LVO stroke.
Statistical Analysis
We used STATA version 16.0 to analyze our data. Univariable logistic analysis was used to compare the variable between the LVO and non-LVO stroke groups. Fisher's exact test was used for categorical data with frequency and percentage, and the Student’s t-test for continuous data was presented with mean ± standard deviation (SD). The power of discrimination is presented with areas under the receiver operating characteristic (AuROC) curve, 95% confidence intervals (CIs), and P-value.
We selected the high discriminative performance variable, clinically relevant to use as a variable in a prehospital setting and statistically significant in the multivariable model. We used a multivariable logistic regression model with backward elimination and reported with odds ratios, 95% CIs, and p-values. The coefficients of each selected variable were divided by the smallest value, rounded to the nearest 0.5, and changed to LVO scores.
We classified LVO patients into three categories: high, moderate, and low probability of LVO stroke and reported with a positive likelihood ratio, 95% CIs, and p-values. Discrimination performance of the model is presented with AuROC curve and 95% CIs. The calibration performance is presented with a graph of observing and predicting risk.
Results
From January 2018 to December 2020. Of 880 patients diagnosed with a stroke, 252 met the criteria and were diagnosed with acute stroke within 24 hours of onset at Ramathibodi Hospital. Of 252 acute stroke patients included in this study, 61 had a radiological diagnosis of LVO stroke. Six factors (comorbidity with atrial fibrillation, clinical hemineglect, gaze deviation, facial palsy, aphasia, and cerebellar sign abnormality) had high discriminative performance variable, clinically relevant to use as a variable in a prehospital setting and statistically significantly affected by the radiological result of LVO stroke (Table 1).
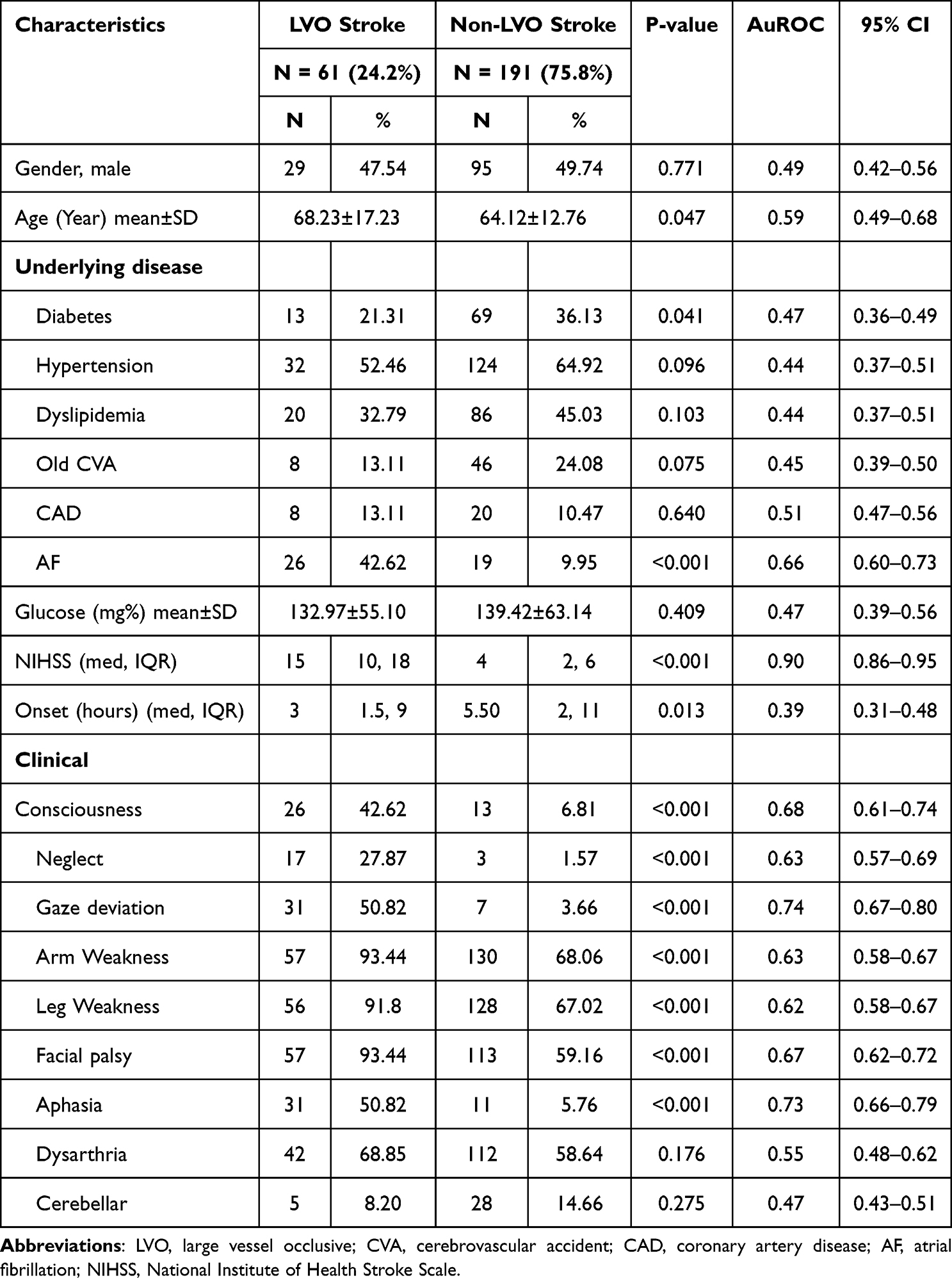 |
Table 1 Clinical Characteristics of participants Categorized by Imaging Reports of Stroke results as LVO or Non-LVO Stroke |
The multivariable logistic regression analysis of six factors was comorbidity with atrial fibrillation (OR 2.84, 95% CI 1.02–7.91, P-value 0.046), clinical hemineglect (OR 13.81, 95% CI 3.02–63.14, P-value 0.001), gaze deviation (OR 7.99, 95% CI 2.54–25.09, P-value <0.001), facial palsy (OR 10.31, 95% CI 2.31–46.04, P-value 0.002), aphasia (OR 19.33, 95% CI 6.91–54.03, P-value <0.001), and cerebellar sign abnormality (OR 2.65, 95% CI 0.68–10.34, P-value 0.159). The coefficients of each selected variable were divided by the smallest value, rounded to the nearest 0.5, and changed to LVO scores, with scores ranging from 0 to 3 (Table 2).
 |
Table 2 Predictors of LVO Stroke and the Assigned Item Score in Cases of Acute Stroke |
The discrimination performance of AuROC curve in multivariable logistic regression model was 92.5% (95% CI 88.7–96.3) (Figure 1), a good performance to predict LVO stroke. The calibration performance is presented with a graph of observing and predicting risk (Figure 2). The LVO risk score was categorized into three groups: low risk (LVO score <3), moderate risk (LVO score 3–6), and high risk (LVO score >6). The positive likelihood ratio to predicting LVO stroke were 0.12 (95% CI 0.06–0.26), 2.33 (95% CI 1.53–3.53) and 45.40 (95% CI 11.16–184.78), respectively.
 |
Figure 1 The AuROC and 95% Confidence Interval of the predictive power of the clinical risk score for LVO stroke in acute stroke patient. |
 |
Figure 2 Observed risk (circles) vs score-predicted risk (solid line) of LVO stroke in acute stroke patient. |
Discussion
This study demonstrated that the newly developed LVO stroke score is an exceptional predictive tool to distinguish the presence of LVO stroke in patients suspected of acute stroke in prehospital settings. LVO stroke score shows an impressive likelihood ratio of 2.33 and 45.40, in moderate risk, with an average score of 3–6 and a high score of >6, respectively (Table 3). The LVO stroke score is aggregated, and the total score is classified according to the probability of LVO: 0–2 points are mild risk, 3–6 points are moderate risk, and exceeding 6 points is a severe risk. In the mild risk group, the LR+ was found to reduce the odds of LVO. Emergency medical service personnel decided to transfer these patients to any stroke centers, but not necessarily a thrombectomy. If the LVO stroke score is moderate-to-severe risk, EMS personnel should be concerned that LVO is possible and decides to transfer patients to a thrombectomy-capable stroke center.
 |
Table 3 Probability Categories in the LVO Score |
Based on the data of this study, we compared the Cincinnati prehospital stroke scale (CPSSS), including gaze palsy (2 points), arm weakness (1 point) and abnormal level of consciousness (1 point), and LVO score. The cut-off points at LVO score of these more than 6 points have sensitivity, specificity, positive predictive value (PPV), and negative predictive value (NPV) 93.5%, 85.5%, 67.1%, and 97.7%, respectively. The cut-off points at CPSSS score of these more than 2 points have sensitivity, specificity 89.75%, and 71.95%.
From the seven highest statistically significantly different clinical presentations and comorbidities to suggest the presence of LVO stroke, six items were chosen to comply with the developed scoring tool (Table 2). Since the variability of interpretation in clinical consciousness was observed from the data-gathering process, we decided to exclude the factor. The comorbidity of AF was defined as pre-existing diagnosis or first-episode onset of atrial fibrillation or atrial flutter at the time of stroke diagnosis or during the period of in-hospital stroke admission. Either paroxysmal or persistent types of AF were included. Other types of arrhythmias were excluded. The included AF was confirmed by ECG 12-lead or noted in the medical record by medical personnel in case of paroxysmal type in which the abnormal rhythm had been presented briefly in continuous vital sign monitoring. We included AF in the final score because the EMS system in the Asian country, especially in Thailand, had 12-lead electrocardiograms in the ambulance. The atrial fibrillation interpretation can be made by EMS personnel and the medical director.
Since endovascular revascularization treatment for stroke is available in both anterior and posterior cerebral circulation,17 clinical cerebellar dysfunction was included in the LVO score despite the non-statistically significant power toward the presence of large vessel occlusion stroke (Table 1). The low number of large vessels of posterior circulation occlusion strokes, four cases from sixty-one LVO strokes, might have affected the characteristics statistic.
As previous reports or predicting LVO tools,3–11 the selected clinical presentations for analysis were based on NIHSS and suspected clinical presentations from affected large vessel lesion territories of the brain.12 From the latest clinical practice guidelines for ischemic stroke in the prehospital setting and ED from the Thai College of Emergency Physicians, 2020, FAST-ED is the screening tool for evaluating LVO stroke. Our cohort’s PPV and NPV of FAST-ED >4 are 72–80% and 82–100%, respectively.
The study of Alexandre AM evaluated the NIHSS score when the patient had a groin puncture. The study demonstrated that NIHSS ≤ 5 related to better outcomes for mechanical thrombectomy.18 This study did not analyze the data of NIHSS to predict LVO. Using the NIHSS score in the prehospital setting had limitations due to the variation level of EMS care and was more complicated than using the LVO score.
Unlike the previous scoring tools, the LVO score is the first tool to be based on all aspects of clinically suspected acute stroke: motor items, cortical sign items, and posterior circulation sign items. We believe the LVO score will be much beneficial and valuable scoring tool for screening suspected large vessel occlusion stroke in a prehospital setting.
In Thailand, not every stroke center can perform a thrombectomy to assess LVO from prehospital. Although the six predictors we chose to develop LVO score might affect slightly increased on-scene time, all six predictors can be assessed since out-of-hospital. Therefore, the LVO score is practical in a prehospital setting and an assistive tool for screening LVO stroke and guiding EMS personnel to decide to transfer patients to the appropriate destination hospital.
Limitation
Firstly, this study excluded stroke cases who came to ED later than 24 hours of onset, the possibility of data missing in case of the presence of large vessel occlusion stroke in those neither excluded group nor unmet criteria for endovascular treatment could have occurred. Secondly, most stroke patients in this study did not reach prehospital services, which could be implied by selection bias when implementing LVO in prehospital settings. The EMS personnel in the Asian country was paramedic and specialist doctor, and the interpretation of neurological exams with the same accuracy as physicians in the ED may be the next project. Thirdly, recorded clinical assessment in this study was done by a neurologist, which could be varied in real-life EMS personnel who are not specialized in neurological examination. However, the proposed LVO score could be a valuable tool for the early screening of prehospital acute stroke patients who should be transferred to a proper stroke center for endovascular treatment. Finally, this study excluded patients with hemorrhagic stroke, and this does not reproduce the actual usage of a prehospital LVO score at last as critically, including hemorrhagic stroke and stroke mimics.
Conclusion
In conclusion, the Large Vessel Occlusion (LVO) Risk Score provides a screening tool for predicting LVO stroke. A clinical predictive score of ≥3 appears to be associated with LVO stroke.
Data Sharing Statement
The datasets used and/or analysed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
This study was approved by the Faculty of Medicine, Committee on Human Rights Related to Research Involving Human Subjects, of Mahidol University’s Ramathibodi Hospital (MURA2021/430). The ethics committee did not require consent for this research because reviewing the medical record is the reason for the waiver and a statement covering patient data confidentiality and compliance with the Declaration of Helsinki.
Funding
No funding was obtained for this study.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Department of Disease Control. Mortality due to non-communicable diseases in the Thailand 2016–2019; 2020. Available from:https://ddc.moph.go.th/uploads/files/1492720200930084722.rar.
2. Chung JW, Park SH, Kim N, et al. Trial of ORG 10172 in Acute Stroke Treatment (TOAST) classification and vascular territory of ischemic stroke lesions diagnosed by diffusion-weighted imaging. J Am Heart Assoc. 2014;3(4). doi:10.1161/JAHA.114.001119
3. Teleb MS, Ver Hage A, Carter J, Jayaraman MV, McTaggart RA. Stroke vision, aphasia, neglect (VAN) assessment-a novel emergent large vessel occlusion screening tool: pilot study and comparison with current clinical severity indices. J Neurointerv Surg. 2017;9(2):122–126. doi:10.1136/neurintsurg-2015-012131
4. Crowe RP, Myers JB, Fernandez AR, Bourn S, McMullan JT. The Cincinnati prehospital stroke scale compared to stroke severity tools for large vessel occlusion stroke prediction. Prehosp Emerg Care. 2020;35:1–9.
5. Tarkanyi G, Csecsei P, Szegedi I, et al. Detailed severity assessment of Cincinnati Prehospital Stroke Scale to detect large vessel occlusion in acute ischemic stroke. BMC Emerg Med. 2020;20(1):64. doi:10.1186/s12873-020-00360-9
6. Llanes JN, Kidwell CS, Starkman S, Leary MC, Eckstein M, Saver JL. The Los Angeles Motor Scale (LAMS): a new measure to characterize stroke severity in the field. Prehosp Emerg Care. 2004;8(1):46–50. doi:10.1080/312703002806
7. Brandler ES, Thode H, Fiorella D. The Los Angeles Motor Scale as a predictor of angiographically determined large vessel occlusion. Intern Emerg Med. 2020;15(4):695–700. doi:10.1007/s11739-019-02272-4
8. Lima FO, Silva GS, Furie KL, et al. Field assessment stroke triage for emergency destination: a simple and accurate prehospital scale to detect large vessel occlusion strokes. Stroke. 2016;47(8):1997–2002. doi:10.1161/STROKEAHA.116.013301
9. Singer OC, Dvorak F, du Mesnil de Rochemont R, Lanfermann H, Sitzer M, Neumann-Haefelin T. A simple 3-item stroke scale: comparison with the National Institutes of Health Stroke Scale and prediction of middle cerebral artery occlusion. Stroke. 2005;36(4):773–776. doi:10.1161/01.STR.0000157591.61322.df
10. Perez de la Ossa N, Carrera D, Gorchs M, et al. Design and validation of a prehospital stroke scale to predict large arterial occlusion: the rapid arterial occlusion evaluation scale. Stroke. 2014;45(1):87–91. doi:10.1161/STROKEAHA.113.003071
11. Li S, Wang A, Zhang X, Wang Y. Design and validation of prehospital acute stroke triage (PAST) scale to predict large vessel occlusion. Atherosclerosis. 2020;306:1–5. doi:10.1016/j.atherosclerosis.2020.04.001
12. Fischer U, Arnold M, Nedeltchev K, et al. NIHSS score and arteriographic findings in acute ischemic stroke. Stroke. 2005;36(10):2121–2125. doi:10.1161/01.STR.0000182099.04994.fc
13. Birnbaum L, Wampler D, Shadman A, et al. Paramedic utilization of Vision, Aphasia, Neglect (VAN) stroke severity scale in the prehospital setting predicts emergent large vessel occlusion stroke. J Neurointerv Surg. 2020;13:505–508. doi:10.1136/neurintsurg-2020-016054
14. Guillory BC, Gupta AA, Cubeddu LX, Boge LA. Can prehospital personnel accurately triage patients for large vessel occlusion strokes? J Emerg Med. 2020;58(6):917–921. doi:10.1016/j.jemermed.2020.01.015
15. Vince Mosesso M, Michael Holtz M. PHTLS Prehospital Trauma Life Support.
16. Tanimoto S, Ikari Y, Tanabe K, et al.2019 Thai guidelines of endovascular treatment in patients with acute ischemic stroke. J Thai Stroke Soc. 2019;18(2):2094.
17. Mokin M, Ansari SA, McTaggart RA, et al. Indications for thrombectomy in acute ischemic stroke from emergent large vessel occlusion (ELVO): report of the SNIS Standards and Guidelines Committee. J Neurointerv Surg. 2019;11(3):215–220. doi:10.1136/neurintsurg-2018-014640
18. Alexandre AM, Valente I, Pedicelli A, et al. Mechanical thrombectomy in acute ischemic stroke due to large vessel occlusion in the anterior circulation and low baseline National Institute of Health Stroke Scale score: a multicenter retrospective matched analysis. Neurol Sci. 2022;43(5):3105–3112. doi:10.1007/s10072-021-05771-5
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.