")
Back to Journals » Patient Preference and Adherence » Volume 18
The Clinical Impact and Good Practices of Remote Patient Monitoring for Chronic Heart Failure: A French Case Report
Authors Creton S, Saadi M, Monfort H, Yaghobian S, Pages N, Nisse-Durgeat S, Diebold B
Received 4 November 2023
Accepted for publication 6 January 2024
Published 16 January 2024 Volume 2024:18 Pages 131—135
DOI https://doi.org/10.2147/PPA.S445638
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Sonia Creton,1 Malika Saadi,1 Hélène Monfort,1 Sarina Yaghobian,2 Nicolas Pages,3 Sophie Nisse-Durgeat,3 Benoit Diebold1
1Cardiology Department, AP-HP Cochin Hospital, Paris, 75014, France; 2Télémédicine 360, TLM360 SAS, Paris, 75116, France; 3NP Medical, Bordeaux, 33000, France
Correspondence: Sonia Creton, Cardiology Service, AP-HP Cochin Hospital, 27 Rue du Faubourg Saint-Jacques, Paris, 75014, France, Tel +33 0158413279, Email [email protected]
Purpose: Remote patient monitoring (RPM) can improve the management of chronic diseases. Since 2019, RPM in chronic heart failure (CHF) management has been internationally supported. However, evidence on the clinical impact and good practices of RPM is scarce. We present a case of a patient with CHF that used RPM in France.
Patients and Methods: A 74-year-old male was diagnosed with CHF (NYHA I) at the AP-HP Cochin Hospital in January 2020. He faced repetitive hospitalizations for acute heart failure and acute kidney injury. The causes of these acute episodes were unknown. Three therapeutic interventions were implemented (diuretic treatment, RPM and therapeutic education sessions). The patient answered questionnaires regularly and directly through the RPM web application named Satelia®Cardio. Therapeutic education was provided to instruct the patient about his symptoms and treatment management.
Results: Since November 11, 2020, the patient had seven hospitalizations representing a total length of stay of 76 days over a period of 15 months and 2 weeks. Pericarditis was diagnosed as a potential cause and a pre-operative checkup was performed. No tangible benefits were found with diuretic treatment and therapeutic education since they had no effect on stopping the acute episodes leading to hospitalization. RPM did not trigger any clinical alerts until his last hospitalization. During this stay, a clinical telehealth nurse reviewed the patient’s clinical setup and found that his initial baseline weight was incorrectly inputted. Since amending this, there were no new episodes. A high-risk, complex and costly heart surgery for pericardial decortication was avoided, and patient satisfaction has increased.
Conclusion: To respect good practices, inclusion not only involves adding or registering a patient to a telehealth activity and database but involves redesigning the management and pathway of patients in order to conduct periodic and personalized clinical care via integrated technology into routine care.
Keywords: chronic heart failure, CHF, remote patient monitoring, telehealth, case report
Introduction
Chronic heart failure (CHF) is a progressive cardiac syndrome that affects up to 2% of the global adult population in developed countries.1 The incidence of CHF has significantly declined in the last decade, mostly due to advances in primary prevention and treatment strategies, however, mortality rates have remained relatively unchanged.2 Some challenges faced in CHF management include providing patients access to care systems, reaching target doses, as well as monitoring drug-dose changes, and reducing hospitalization rates.3
Remote patient monitoring (RPM) is a telehealth activity that has previously been shown to improve the management of chronic diseases.4–6 Such practices enable healthcare professionals to remotely monitor and deliver care to patients as well as allow patient engagement and access to relevant health-related educational and support systems. In 2019, RPM was recommended for CHF.7 However, evidence on the clinical impact and good practices of RPM, particularly for CHF, is scarce.8 We present a case of a patient with CHF that used RPM for follow-ups in France.
Case Presentation
A 74-year-old male was diagnosed with CHF (NYHA I) at the APHP Cochin Hospital in France in January 2020. He is a retired general practitioner living with his wife who is a physician specializing in nephrology. The patient has been independent for his daily life activities and reportedly walking approximately one hour every day. He has had no major events in his medical history except for superficial venous insufficiency. Since 2020, he has been treated for CHF and had not undertaken any other treatment. This report complied with MR-004 methodology declared by the French data protection authority (CNIL) and ethical approval by an institutional review board was not required according to French legislation to publish the case details. Written informed consent was obtained from the patient for publication.
Since November 11, 2020, the patient had seven hospitalizations representing a total length of stay of 76 days over a period of 15 months and 2 weeks (Table 1). His first hospitalization was due to atrial fibrillation (AF); however, the following causes were primarily due to episodes of acute heart failure (AHF) (n = 3) and acute kidney injury (AKI) (n = 3). The patients’ weight was 88kg at first hospitalization entry and 70kg at the seventh hospitalization entry (Table 1). The causes of his AHF episodes were unknown.
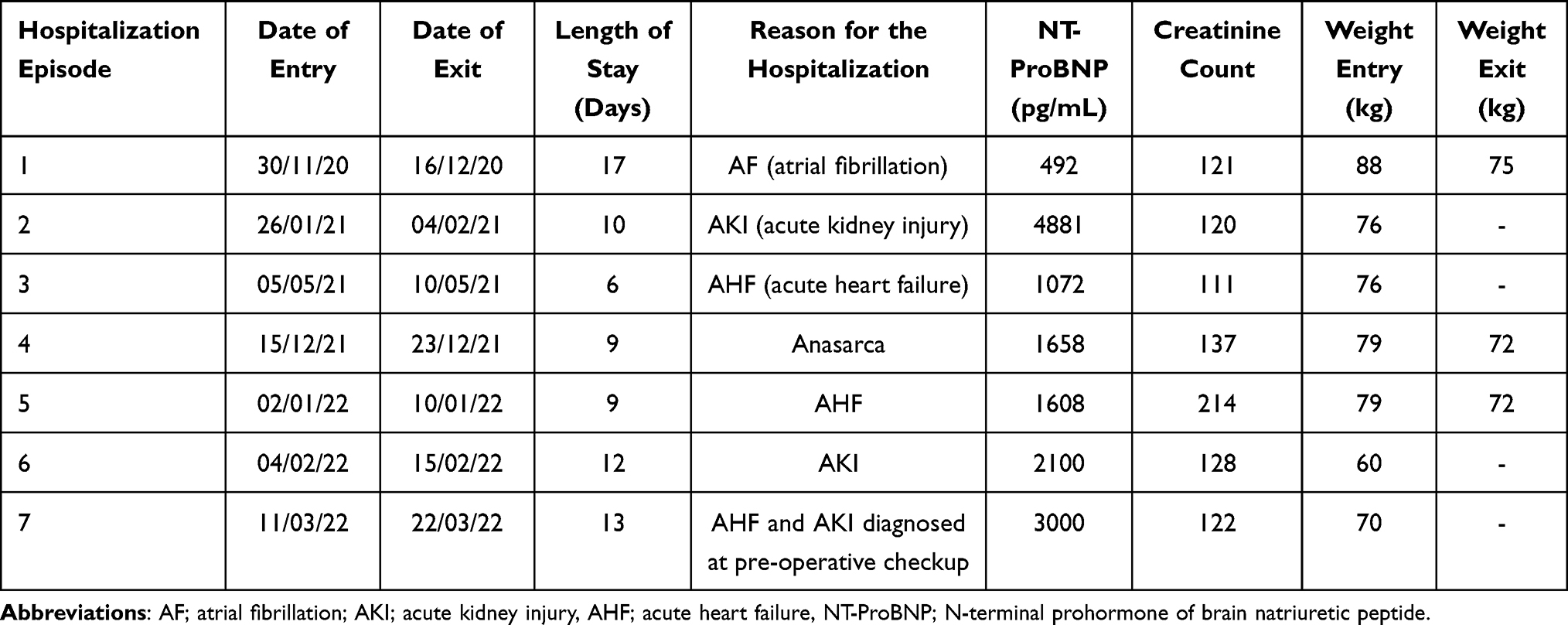 |
Table 1 Characteristics of the Hospitalization Episodes of a Patient with Chronic Heart Failure (CHF) Using a Remote Patient Monitoring (RPM) Web Application in France |
Diagnostic tests, including cardiac MRI, CT scans and ultrasound imagery, were performed during his hospital stays. At first hospitalization, using a CT scan, constrictive pericarditis was suspected as the potential cause of his clinical condition (Table 2) A diagnosis of chronic non-constrictive pericardial dysfunction was made using a cardiac MRI in February 2021. No targeted therapy was prescribed to the patient due to his suspected pericarditis. Discussion about a surgical intervention to avoid pericardial decortication took place during his sixth hospitalization (Table 2).
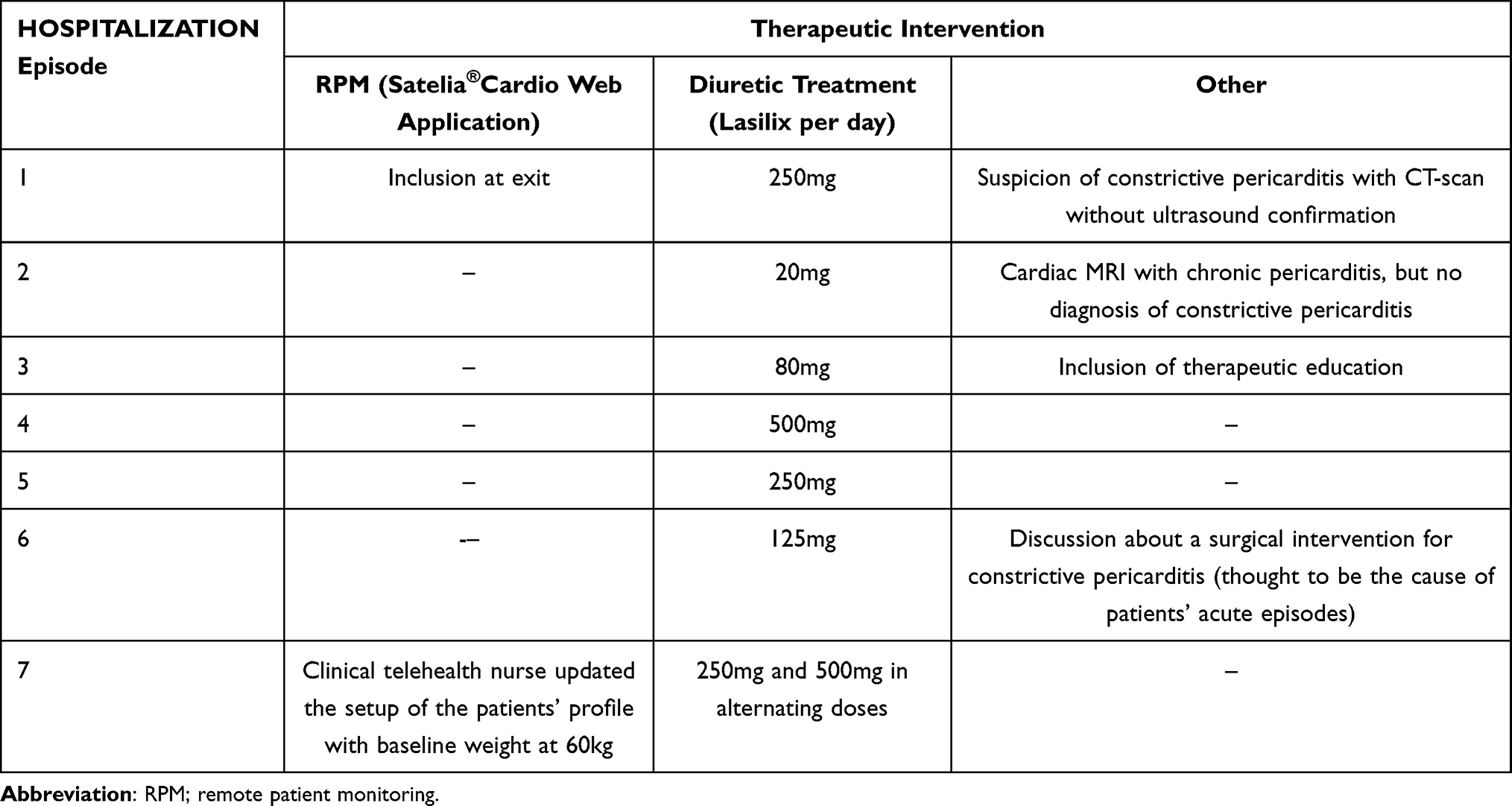 |
Table 2 Description of the Hospitalization Episodes of a Patient with Chronic Heart Failure (CHF) Using a Remote Patient Monitoring (RPM) Web Application in France |
NT-ProBNP was over 400pg/mL during all hospitalizations (Min: 492, Max: 4881) (Table 2). Creatinine count started at 121 and peaked at 214. At first entry, the left ventricular ejection fraction (LVEF) of the patient was 30% representing moderate dysfunction. This figure rose to 55% representing normal function at his seventh hospitalization in 2022.
Three types of therapeutic interventions were implemented during the course of the patients’ hospitalizations. Diuretic treatment was initiated during and after each hospitalization with various doses of Lasilix ranging from 20mg to 250mg to 500mg in alternating doses. On December 16, 2020, the patient was included in an RPM program for follow-ups. The RPM solution was a web application based on patient reported outcomes (PROs) named Satelia®Cardio.9 The patient answered questionnaires regularly and directly through the web application. The hospital unit in which the patient was treated had enrolled a total of 80 patients to RPM. Patients registered to the RPM program had a mean age of 71.9 years. Finally, in May 2021, therapeutic education sessions were provided to the patient to instruct him about his symptoms and treatment management.
In terms of patient stabilization, no tangible benefits were found when diuretic treatment and therapeutic education were provided. These interventions had no effect on stopping the acute episodes leading to hospitalization. The RPM also did not trigger any clinical alerts until his last hospitalization. During this stay, a new coming clinical nurse who was trained in telehealth reviewed the patient’s clinical setup and found that his initial baseline weight was incorrectly inputted. It was discovered that instead of his weight being measured at the end of his last hospital stay, it was taken during the length of stay resulting in a consistently higher reported weight. Because of this, no alerts were triggered by the RPM algorithm that had analyzed weight as one of the key parameters. The nurse has continued to evaluate his responses to the questionnaires even in the absence of any alerts and records the patient’s weight as well as any symptoms discussed at each clinical follow-up.
Since the last hospitalization, there have been no new episodes for the patient between April and December 2022. A high-risk, complex and costly heart surgery for pericardial decortication was avoided, and patient satisfaction has increased. The patient has been able to carry out more physical activities and provided the following statement on his experience with RPM:
After having multiple hospitalizations either for cardiac decompensation or for my difficulties in adapting to the treatment, I was well, and on the way back to normal. I have absolute confidence in medicine. I had been asked to have surgery but given the risk-improvement ratio, I decided to take the advice of my relatives and postpone it. Since my last hospitalization I have seen a marked improvement in my quality of life with a return to almost normal. I can climb stairs, walk without shortness of breath, and I can dress and tie my laces without problem. Only downside is the muscle loss I have faced after my hospitalization and strict diet without salt which deprives me of eating cold cuts and seafood which are my biggest indulgence.
Discussion
CHF carries a substantial burden to the healthcare system both at a national and international scale.10 Many studies have shown that RPM can reduce the number of hospitalizations and improve effectiveness in CHF management.11 Jourdain et al detailed that such digital tools can identify low-risk patients which can support physicians to better prioritize and customize consultations for optimal care.12 In terms of adherence, a real-world use study reported that RPM could allow better adherence to CHF treatment regimens.13 Sabatier et al also stated that RPM adherence was associated with better outcomes.14
In this case report, we show that if well managed by a trained team, PROs-based RPM for CHF can help improve the clinical conditions of patients and potentially reduce hospitalization rates. More generally, measurements such as that of the baseline weight should be carefully inputted and periodically updated. Dedicated and available human resources should also be considered to the follow-up of patients. Before the last hospitalization, it was reported that the RPM was not as well managed due to limited trained CHF nurses. The main limitations of this study were potential biases that are common in case report findings and the impossibility to specifically indicate the causative inference between the change of the RPM setup, the increase of diuretic dosage and the improvement of the clinical conditions of the patient.
Conclusion
In conclusion, to respect good practices, patient inclusion to RPM consists not only of adding or registering a patient to the platform and database but also redesigning the management and pathway of patients in order to conduct periodic and personalized clinical care via integrated technologies into routine care.
Consent
Written informed consent was obtained from the patient for publication.
Acknowledgments
The authors would like to thank Chloé Bedel from NP Medical for her contribution as well as Marty Brucato from AcaciaTools for his proofreading and reviewing services.
Disclosure
The authors report that NP Medical funded the production of this article. Dr Malika Saadi reports Creation Support Presentation from BAYER, Orateur (Symposium) from ASTRA ZENECA, Cas Cliniques/Plateforme Enseignement from BAYER, outside the submitted work. Dr Nicolas Pages and Dr Sophie Nisse-Durgeat are employees of NP MEDICAL. The authors have no other competing interests to disclose.
References
1. McDonagh TA, Metra M, Adamo M, et al. 2021 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: developed by the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC). With the special contribution of the Heart Failure Association (HFA) of the ESC. European J of Heart Fail. 2022;24:4–131. doi:10.1002/ejhf.2333
2. Tsutsui H, Tsuchihashi-Makaya M, Kinugawa S. Clinical characteristics and outcomes of heart failure with preserved ejection fraction: lessons from epidemiological studies. J Cardiol. 2010;55:13–22. doi:10.1016/j.jjcc.2009.09.003
3. Wagner JA. Top ten challenges in heart failure management. J Nurse Pract. 2006;2:528–532. doi:10.1016/j.nurpra.2006.07.011
4. Gokalp H, de Folter J, Verma V, Fursse J, Jones R, Clarke M. Integrated Telehealth and Telecare for Monitoring Frail Elderly with Chronic Disease. Telemed E-Health. 2018;24:940–957. doi:10.1089/tmj.2017.0322
5. Isaranuwatchai W, Redwood O, Schauer A, Van Meer T, Vallée J, Clifford P. A remote patient monitoring intervention for patients with chronic obstructive pulmonary disease and chronic heart failure: pre-post economic analysis of the smart program. JMIR Cardio. 2018;2:e10319. doi:10.2196/10319
6. Jenneve A, Lorenzo-Villalba N, Courdier G, et al. Benefit of ambulatory management of patients with chronic heart failure by protocolized follow-up therapeutic education and remote monitoring solution: an original study in 159 patients. JCM. 2020;9:3106. doi:10.3390/jcm9103106
7. Seferovic PM, Ponikowski P, Anker SD, et al. Clinical practice update on heart failure 2019: pharmacotherapy, procedures, devices and patient management. An expert consensus meeting report of the heart failure association of the European society of cardiology. Eur J Heart Fail. 2019;21:1169–1186. doi:10.1002/ejhf.1531
8. Nakamura N, Koga T, Iseki H. A meta-analysis of remote patient monitoring for chronic heart failure patients. J Telemed Telecare. 2014;20:11–17. doi:10.1177/1357633X13517352
9. Pages N, Picard F, Barritault F, et al. Remote patient monitoring for chronic heart failure in France: when an innovative funding program (ETAPES) meets an innovative solution (Satelia® Cardio). Dig Health. 2022;8:205520762211167. doi:10.1177/20552076221116774
10. Bui AL, Horwich TB, Fonarow GC. Epidemiology and risk profile of heart failure. Nat Rev Cardiol. 2011;8:30–41. doi:10.1038/nrcardio.2010.165
11. Bashi N, Karunanithi M, Fatehi F, Ding H, Walters D. Remote Monitoring of Patients With Heart Failure: an Overview of Systematic Reviews. J Med Inter Res. 2017;19(10.2196/jmir.6571):e6571.
12. Jourdain P, Pages N, Amara W, et al. Perceptions and satisfaction of patients with chronic heart failure when using a remote monitoring web application named Satelia® Cardio. Ann Cardiol Angéiologie. 2023;72:101606. doi:10.1016/j.ancard.2023.101606
13. Patrick J, Picard F, Girerd N, et al. Security and performance of remote patient monitoring for chronic heart failure with Satelia® Cardio: first results from real-world use. J Cardiol Cardiovasc Med. 2023;8:042–50. doi:10.29328/journal.jccm.1001152
14. Sabatier R, Legallois D, Jodar M, et al. Impact of patient engagement in a French telemonitoring programme for heart failure on hospitalization and mortality. ESC Heart Fail. 2022;9(5):2886–2898. PMID: 35715956; PMCID: PMC9715861. doi:10.1002/ehf2.13978
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.