Back to Journals » International Journal of General Medicine » Volume 13
The Clinical Application of the Tracheostomy Decision-Making Program in Respiratory Care Center Prolonged Mechanical Ventilation Patients in Taiwan
Received 18 October 2020
Accepted for publication 27 November 2020
Published 10 December 2020 Volume 2020:13 Pages 1487—1494
DOI https://doi.org/10.2147/IJGM.S285795
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Chien Hsiu Huang, I-Hung Chen
Department of Internal Medicine, Division of Chest Medicine, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, Chiayi, Taiwan
Correspondence: Chien Hsiu Huang
Department of Internal Medicine, Division of Chest Medicine, Dalin Tzu Chi Hospital, Buddhist Tzu Chi Medical Foundation, No. 2, Min-Sheng Road, Dalin Town, Chiayi, Taiwan
Email [email protected]
Background: We applied the tracheostomy decision-making program for respiratory care center prolonged mechanical ventilation patients. Our objectives are to correct the misconception of patients about tracheostomy. We expect to understand whether the program is effective in educating patients and whether the patients are satisfied with the results of their decision-making. We compared the prognostic differences between patients receiving tracheostomy and those who continue to have an endotracheal tube, which serves as our basis to provide suggestions for patients in the shared decision-making program.
Patients and Methods: A retrospective study was conducted in Dalin Tzu Chi Hospital from January 2017 to December 2019. We set up a tracheostomy decision-making program. The medical team identified eligible patients. We tracked the survival of each patient and followed up on each patient to ask whether they thought they had made an optimal decision based on the results of their participation in the tracheostomy decision-making program in January 2020. Data of respiratory care center prolonged mechanical ventilation patients who participated in the tracheostomy decision-making program were collected and analyzed.
Results: Fifty-seven respiratory care center patients attended the tracheostomy decision-making program. At the end of the study, 37 patients underwent tracheostomy (64.9%), and 20 patients maintained endotracheal tube intubation (35.1%). The survival rate of patients undergoing tracheostomy was 86.5% and 32 participants (86.5%) believed that they made an optimal decision after participating in the tracheostomy decision-making program. The survival rate of patients who maintained endotracheal tube intubation was 40%, and twenty (100%) participants believed that they made an optimal decision after participating in the tracheostomy decision-making program.
Conclusion: The clinical application of the tracheostomy decision-making program ensures that patients have a clearer understanding of the methods of tracheostomy and endotracheal tube intubation. Overall, 91.2% of the participants believed that they made an optimal decision despite the end result.
Keywords: shared decision making, respiratory care center, tracheostomy, endotracheal tube intubation
Introduction
Shared decision-making (SDM) in medicine, involving medical staff and patients was proposed in the United States in 1982, which has been implemented for a long period of time.1 Advocating patients to participate in SMD not only helps patients to better understand their disease and various treatment options, but also increases patient satisfaction and safety, improves the quality of medical treatment received, and promotes exemplary medical care. In Taiwan, a nationwide SDM project was launched in 2016 to promote patient safety and evidence-based medicine. SDM allows patients to understand disease information more comprehensively, including the available treatment methods. Based on the evidence, the medical team conducts a disease analysis and allows both medical staff and patients to propose different treatments before reaching a therapeutic decision. This would occur after an in-depth discussion, patient feedback, and any concern regarding treatment modalities. The patient and physician would then decide on the best option, given all feasible treatments. The decision-making program “If my family has difficulty weaning from the ventilator, does he/she need to undergo tracheostomy?” was developed under the Ministry of Health and Welfare’s “Medical and Disease Sharing Decision Promotion Plan.” (https://sdm.patientsafety.mohw.gov.tw/AssistTool/AccessibilityForm?sn=24&tid=F7D1B4EE284BE40E).
The “Trial Plan for National Public Health Insurance Ventilator Dependent Patients Comprehensive Care System” began in Taiwan in July 2000.2 This program covers mechanical ventilator care in the following settings: intensive care unit (ICU), respiratory care center (RCC), respiratory care ward (RCW), and home care services. The RCC is a subacute stage for patients who undergo ventilator support for more than 21 days. The goal of RCC care is to wean prolonged mechanical ventilation (PMV) patients off the ventilator. Tracheostomy is recommended for RCC patients who cannot be weaned from the ventilator in the short term. However, most patients or family members do not want this procedure done. The most common reasons for refusal are that the operation will leave a wound on the patient’s neck, worry about the risks and complications of tracheostomy, and subjectively incorrect views of the family members. The following are some of the incorrect opinions regarding tracheostomy: 1) it will prolong the patient’s disease course and increase the burden on the family; 2) it will increase patient pain and shorten the individual’s life; and 3) after a tracheostomy, the tube cannot be removed permanently, and the patient will be bed-ridden for life. As such, family members may believe it would be better to let the patient suffer from side effects and discomfort after endotracheal tube intubation rather than permit tracheostomy. Thus, the proportion of patients undergoing tracheostomy in Taiwan is lower than that in the US. In Taiwan, the Clinical Performance Indicators data revealed that the tracheostomy rate of PMV patients in the RCC medical center was about 39%. The US literature discusses early tracheostomy or late tracheostomy for ICU patients, which provides a better course of treatment and better prognosis for patients on ventilators.3–6 In the study of Combes et al, ICU patients with early tracheostomy were reported to have better chances of survival than those who do not undergo a tracheostomy.7 In Taiwan, Weng et al reported that patients with early tracheostomy had fewer ventilator days, higher weaning rates, and lower in-hospital mortality.8 Wu et al showed that patients who undergo tracheostomy have a lower in-hospital mortality rate than those who do not.9 According to Huang et al, PMV patients who have undergone tracheostomy have a favorable one-year survival rate as well as a significantly lower rate of in-hospital mortality.10 Taiwan’s RCC PMV patients usually must decide whether they need a tracheostomy, not whether to have an early or late tracheostomy.
In 2017, Dalin Tzu Chi Hospital applied the program “If my family has difficulty weaning from the ventilator, does he/she need to undergo tracheostomy?”. Our objectives are to correct the misconception of patients and/or family members about tracheostomy. We expect to understand whether the program is effective in educating patients and whether the patients are satisfied with the results of their decision-making. We compared the prognostic differences between patients receiving tracheostomy and those who continue to have an endotracheal tube, which serves as our basis to provide suggestions for patients or family members in the shared decision-making program. This study also provides the preliminary results of tracheostomy by sharing the results of the decision-making program in the weaning center PMV patients with the medical community.
Patients and Methods
Study Design
A retrospective cross-sectional study was conducted. The study was performed in the respiratory care center of Dalin Tzu Chi Hospital from January 2017 to December 2019. Details related to the methods of the study, the decision-making program, and the measurement of program outcomes are provided below.
The study conformed to the Declaration of Helsinki 1975, revised Hong Kong 1989. The project was approved by the Buddhist Dalin Tzu Chi General Hospital Research Ethics Committee (Approved IRB No.: B10802009). All participants (patients or family members) provided written informed consent to participate. Because most patients could not talk and were in unclear states of consciousness and in this case, the participants were family members instead (patients’ legal representatives).
Program Steps
We set up a tracheostomy decision-making program (Appendix). The goals of this program were as follows:
1) Educate patients and family members so that they may understand the differences between advantages and disadvantages of the two treatment methods (tracheostomy and endotracheal tube intubation); 2) Inform patients and family members of the factors and degrees of concern related to the two methods of treatment; and 3) Help patients and family members decide on a method of treatment. We divided the tracheostomy decision-making program into four steps. In step one, patients and family members were invited to compare the alternatives and the advantages, risks, adverse effects, complications, and costs of each treatment option. Then, during the process of choosing a treatment, participants were asked about their concerns and the degrees to which they were concerned regarding the two methods of treatment (step two). In the third step, we tested the knowledge of patients or family members, related to the two treatment methods. Finally, we asked the patients or family members to evaluate their treatment decisions (step four).
Setting and Participants
Dalin Tzu Chi Hospital is a tertiary general hospital. Our RCC, which is a weaning unit within an acute-care hospital, caters to PMV patients. There are 10 beds in our RCC. In the past 3 years, an average of 127 PMV patients were hospitalized each year. All patients on PMV were invited to participate in the tracheostomy decision-making program.
Exclusion Criteria
- The patient was expected to die in the near future.
- The patient was expected to be weaned from the ventilator in the near future.
- The patient or family members did not accept the idea of a tracheostomy at all and were unwilling to understand the tracheostomy decision-making program.
- The surgeon determined that the patient had no indication for a tracheostomy or was at high risk for undergoing the procedure.
- The patient had received a tracheostomy before being admitted to RCC.
Procedures
Eligible study medical teams included RCC physicians and RCC nurses. The medical team identified eligible patients after family members agreed to participate. We did not perform a questionnaire survey and baseline data collection of the family’s concept of tracheostomy before the program. We allowed all participating families to watch educational videos on tracheotomy recorded by our hospital before the program. (http://ok.tzuchi.com.tw/okban/01_event_01/lessons/03_Tracheotomy/index_c.html)
Then, we chose to conduct semi-structured interviews with individual family members. Additionally, written informed consent was received from individual participants prior to each interview. After patients were discharged from the RCC, they could be classified into the following three situations: 1) patients died; 2) patients received long-term ventilator support in the RCW; and 3) patients were discharged to their homes. We tracked the survival of each patient and the satisfaction of the patient or family members with the tracheostomy decision-making program. Post-program interviews with patients or patients’ families were conducted over the phone by the head nurse in January 2020. We explored the end-of-life decisions (signing the do-not-resuscitate: DNR) for all 57 patients also.
Outcomes Measure
We explored whether the following aspects of the two groups of patients (patients undergoing tracheostomy versus patients preferring endotracheal tube intubation) were statistically different:
- The factors of concern regarding the two treatment methods
- The degrees of concern regarding the two treatment methods
- Results of the test on knowledge of the two treatment methods
- The rate of success in ventilator weaning
- Patient survival rate
- Signing the DNR order
- The rate of satisfaction with the tracheostomy decision-making program
Statistical Analysis
Continuous variables express as mean ± SD or median (range), and categorical variables express as frequency and percentage. Differences in baseline characteristics and causes of respiratory failure and step 2 were evaluated using the Student’s t-test for continuous variables and Pearson chi-square test or Fisher’s exact test for categorical variables. Step 3, patient survival rate, the rate of success in ventilator weaning, signing the DNR order, and the rate of satisfaction with the tracheostomy decision-making program were evaluated using logistic regression analysis. All statistical analyses were conducted using the statistical package SPSS for Windows (Version 17.0, SPSS Inc., Chicago, IL) and a P value<0.05 was considered to show statistical significance.
Results
Fifty-seven patients attended the tracheostomy decision-making program, which accounted for 15.0% of the RCC PMV patients during the 3-year period. The clinical data of the patients are listed in Table 1. The average age of the patients was 69.6 years; 68.4% were men and 31.6% were women. Pneumonia was the primary cause of respiratory failure in patients.
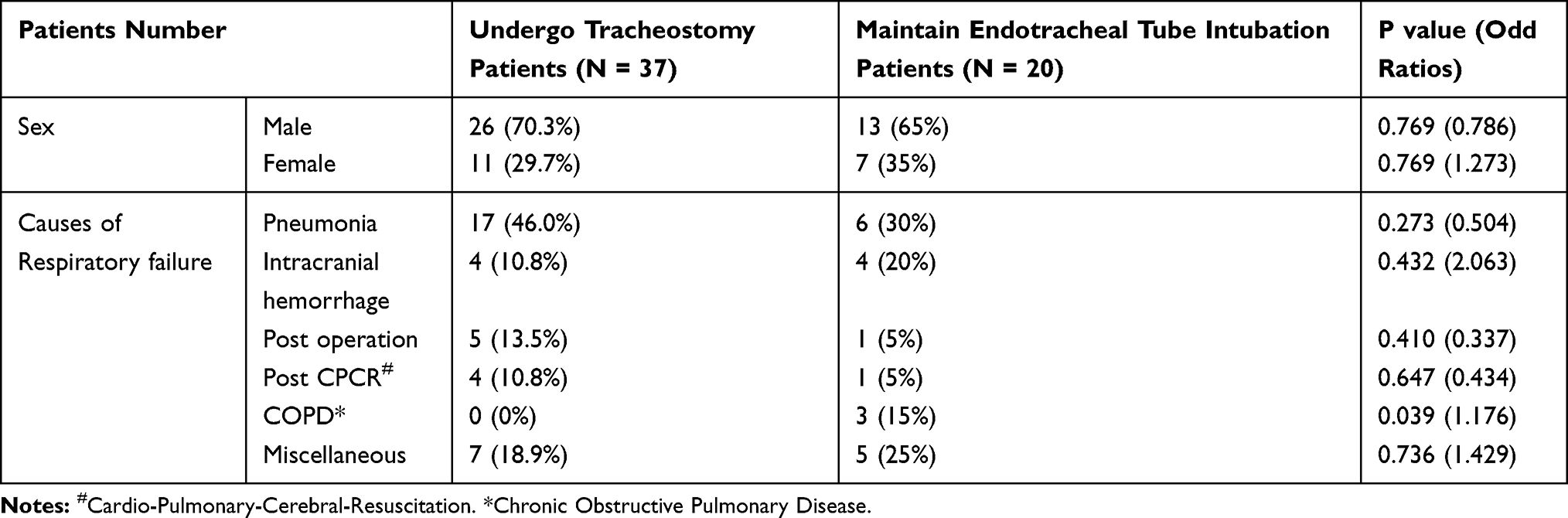 |
Table 1 Clinical Characteristics of Study Patients (n=57) |
The results of the factors and degrees of concern regarding the two treatment methods are provided in Table 2. Patients chose tracheostomy primarily for the following reasons, which are listed in the order of importance: 1) the patient’s comfort; 2) the patient can eat or speak; and 3) the patient can be discharged and return home. The primary reasons for choosing to maintain endotracheal tube intubation also listed in the order of importance, were: 1) the patient’s comfort; 2) the patient can eat or speak; and 3) possible complications of a tracheostomy. The differences in the responses between the two groups of patients were not statistically significant.
 |
Table 2 The Results of the Factors and Degrees of Concern Related to the Two Methods of Treatment |
The results of the test evaluating family member knowledge are shown in Table 3. The difference in the correct rate between the family members of patients who chose tracheostomy and those who maintained endotracheal tube intubation was not statistically significant. Three patients needed to discuss their options with other relatives and friends before making a decision. Of these, two patients later decided to undergo a tracheostomy, and one patient chose to maintain endotracheal tube intubation. At the end of the study, 37 patients (64.9%) underwent tracheostomy, and 20 patients (35.1%) maintained endotracheal tube intubation.
 |
Table 3 The Result of Step 3: How Much Does the Patient or Family Know About the Treatments? |
In January 2020, we telephonically followed-up with each patient to ask whether they thought they had made an optimal decision based on the results of their participation in the tracheostomy decision-making program. The results are listed in Table 4. Forty-one patients were successfully weaned from the ventilator, including 28 tracheostomy patients and 13 endotracheal tube intubation patients. The rate of successfully weaned patients who underwent tracheostomy was not significantly different from those who maintained endotracheal tube intubation (75.7% vs 65.0%, P=0.538).
 |
Table 4 The Discharged Status of RCC Prolonged Mechanical Ventilation Patients |
In terms of survival, 12 patients in the endotracheal tube intubation group died, but there were only five deaths in the tracheostomy group (p=0.001, OR=9.6, 95% confidence interval: 2.618–35.207) (Table 5). After participating in the tracheostomy decision-making program, 20 (100%) and 32 (86.5%) participants in the endotracheal tube intubation group and tracheostomy group, respectively, believed that they made an optimal decision. The reasons for participants in the tracheostomy group not being satisfied with their decision included: 1) it was inconvenient to move the tracheostomy tube when the patient’s hand flexed; 2) the patient was too old to undergo the operation; 3) no experience of benefit with tracheostomy; and 4) the perception that tracheostomy was no better than endotracheal tube intubation (opined by family members from two different patient cases). Overall, 91.2% of participants believed that they made an optimal decision after taking part in the tracheostomy decision-making program. We explored the end-of-life decisions for all 57 patients (Table 5). By far, a higher percentage of those who maintained endotracheal tube intubation (75%) signed the DNR orders than those who underwent tracheostomy (43.2%) (P=0.028. OR: 0.254, 95% confidence interval: 0.076–0.846).
 |
Table 5 The Results of Long-Term Outcome and Satisfaction with Their Decision Based on the Result of the Tracheostomy Decision-Making Program |
Discussion
We applied the “If my family has difficulty weaning from the ventilator, does he/she need to undergo tracheostomy?” question in the decision-making program for RCC PMV patients. This study is for PMV patients (mechanical ventilation>21 days), and the research focus is the tracheostomy decision-making clinical application report. Besides, this research reflects the culture of Taiwan. To our knowledge, we did not find any similar studies in the international literature related to the clinical application of tracheostomy decision-making in PMV patients. Thus far, only one similar case report has been reported in Taiwan.11 Therefore, we can only analyze our own research results and hope that this result can inspire a similar discussion.
The purpose of the first of the four steps in the tracheostomy decision-making program was to provide the patients’ families with a complete understanding of the differences between tracheostomy and endotracheal tube intubation. In step 2, we discovered that the patients and their family members considered the patient’s comfort level to be the most important factor in making their decision, placing less importance on the opinions of friends and relatives; there was no statistically significant difference between patients undergoing tracheostomy and those maintaining endotracheal tube intubation with respect to attitudes toward patient care. The influencing factors related to tracheostomy were maintaining the integrity of the patient’s neck surgery and possible complications of the tracheostomy. The group of patients who maintained an endotracheal tube had a higher degree of concern for these two influencing factors, thus reducing their family members’ willingness for the patient to undergo tracheostomy. In step 3, we tested the knowledge of the patients’ families about tracheostomy and endotracheal tube intubation. There was a high degree of knowledge about treatment methods, with a correct rate of 93.3%. The families scored <90% on the following three items: 1) tracheostomy will prolong the patient’s disease course and increase the burden on the family; 2) after a tracheostomy, the patient should be able to be weaned from the ventilator; and 3) after a tracheostomy, the incidence of pneumonia and mortality will decrease. When comparing the two treatment methods, doctors need to explain these three questions in more detail so that the family members can have a more accurate understanding of what is involved. Finally, in step 4, only three patients’ families (5.3%) had to discuss their options with other relatives and friends before making a final decision. Therefore, the tracheostomy decision-making program reached its goal of educating the patients and their family members.
The results of our follow-up telephone interviews showed that survival of the patients who underwent tracheostomy was excellent. Equally, the survival of patients who maintained their endotracheal tube intubation was poor, but all participants who chose to remain intubated believed that they made an optimal decision after participating in the tracheostomy decision-making program. Although 12 of the patients who maintained their endotracheal tube intubation died, their family members still believed that it was an appropriate treatment choice for the patient. It is very likely that the main factor for poor survival rate among the patients who maintained endotracheal tube intubation was a higher percentage of those who signed the DNR orders. Why did patients’ families sign the DNR orders for these patients? Patients experienced suffering in their critical care with PMV support. This experience is very shocking and painful for patients. Most patients are in poor health status or unconscious and cannot recover in the short term. Because patients’ families did not wish for their loved ones to undergo this experience again, they believed that palliative therapy was of greater benefit for their patients. From a prognostic point of view, the survival of patients undergoing tracheostomy is significantly better than that of patients who maintain endotracheal tube intubation. When PMV patients are expected to survive for a long time, they are strongly advised to choose tracheostomy.
Limitations of This Study
Our report is a small, retrospective study with few participants. There was no control group with which to compare the differences in patient and family mindset after exposure to the tracheostomy decision-making program intervention. It is impossible to make any firm conclusions based on this preliminary result. We hope to conduct a control study which will be shared in the future. Besides, this research reflects the culture of Taiwan, so it is not applicable to most countries. However, the culture of some countries is similar to Taiwan. This study will serve as a reference.
Conclusion
The clinical application of the tracheostomy decision-making program is that patients and family members have a clearer understanding of the methods of tracheostomy and endotracheal tube intubation after participating in the program. Overall, 91.2% of the participants believed that they made an optimal decision after their participation in the program.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval
The project was approved by Buddhist Dalin Tzu Chi General Hospital Research Ethics committee. (Approved IRB No.: B10802009).
Consent
All participants (patients and their family members) provided written informed consent to participate.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Funding
There was no funding for this study.
Disclosure
The authors declare that they have no competing interests.
References
1. United States: the ethical and legal implications of informed consent in the patient-practitioner relationship. United States. President’s commission for the study of ethical problems in medicine and biomedical and behavioral research; 1982. Available from: https://catalog.hathitrust.org/Record/001827278.
2. Bureau of National Health Insurance: prospective payment system of ventilator dependents managed care demonstration. Available from: https://www.nhi.gov.tw/Resource/webdata/13988_1_1050002331-1.pdf.
3. Wang F, Wu Y, Bo L, et al. The timing of tracheotomy in critically ill patients undergoing mechanical ventilation: a systematic review and meta–analysis of randomized controlled trials. Chest. 2011;140:1456–1465. doi:10.1378/chest.11-2024
4. Zheng Y, Sui F, Chen XK, et al. Early versus late percutaneous dilatational tracheostomy in critically ill patients anticipated requiring prolonged mechanical ventilation. Chin Med J. 2012;125:1925–1930.
5. Young D, Harrison DA, Cuthbertson BH, Rowan K. Effect of early vs. Late tracheostomy placement on survival in patients receiving mechanical ventilation. The TracMan randomized trial. JAMA. 2012;309(20):2121–2129.
6. Siempos II, Ntaidou TK, Filippidis FT, Choi AMK. Effect of early versus late or no tracheostomy on mortality and pneumonia of critically ill patients receiving mechanical ventilation: a systematic review and meta-analysis. Lancet Respir Med. 2015;3:150–158. doi:10.1016/S2213-2600(15)00007-7
7. Combes A, Luyt CE, Nieszkowska A, Trouillet JL, Gibert C, Chastr J. Tracheostomy associated with better outcomes for patients requiring long-term mechanical ventilation. Crit Care Med. 2007;35:802–807. doi:10.1097/01.CCM.0000256721.60517.B1
8. Weng MX, Li JY. Prognosis analysis of early tracheostomy or late tracheostomy. J Life Sci. 2008;12:195–205.
9. Wu YK, Tsai YH, Lan CC, et al. Prolonged mechanical ventilation in a respiratory-care setting: comparison of outcome between tracheostomized and translaryngeal intubated patients. Crit Care. 2010;14:R26. doi:10.1186/cc8890
10. Huang CT, Lin JW, Ruan SY, Chen CY, Yu CJ. Preadmission tracheostomy is associated with better outcomes in patients with prolonged mechanical ventilation in the postintensive care respiratory care setting. J Formosan Med Assoc. 2017;116:169–176. doi:10.1016/j.jfma.2016.05.005
11. Wu CY, Chen RQ. Application of shared decision making for tracheostomy in an ICU patient with decision conflict. Formosan J Med. 2018;22:593–598.
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.