")
Back to Journals » Patient Preference and Adherence » Volume 18
The Burden of Suboptimal Insulin Dosing in People with Diabetes in Spain: Barriers and Solutions from the Physician Perspective
Authors Bellido V, Duque N , Newson RS, Artime E , Spaepen E, Rubio de Santos M, Redondo-Antón J , Díaz-Cerezo S, Navarro J
Received 12 September 2023
Accepted for publication 9 January 2024
Published 16 January 2024 Volume 2024:18 Pages 151—164
DOI https://doi.org/10.2147/PPA.S439814
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Virginia Bellido,1 Natalia Duque,2 Rachel S Newson,3 Esther Artime,2 Erik Spaepen,4 Miriam Rubio de Santos,2 Jennifer Redondo-Antón,2 Silvia Díaz-Cerezo,2 Jorge Navarro5
1Unidad de Gestión Clínica de Endocrinología y Nutrición, Hospital Universitario Virgen del Rocío, Sevilla, Spain; 2Medical Department, Medical Affairs, Eli Lilly and Company, Madrid, Spain; 3NAPAC Real World Evidence, Medical Affairs, Eli Lilly and Company, Sydney, NSW, Australia; 4Statistics, HaaPACS GmbH, Schriesheim, Germany; 5Department of Medicine, University of Valencia, Valencia, Spain
Correspondence: Natalia Duque, Eli Lilly and Company, Alcobendas, Madrid, Spain, Email [email protected]
Background: This study aimed to determine physicians’ perceptions of the extent of suboptimal insulin dosing and the barriers and solutions to optimal dosing in people with diabetes (PwD) treated with insulin.
Methods: A cross-sectional online survey was conducted in four countries with primary care physicians and endocrinologists treating PwD using insulin pens, which included 53 questions on physicians’ characteristics and their perceptions of the behaviors of PwD in relation to insulin dosing routines, unmet needs and potential solutions. Analyses were descriptive.
Results: Of the 160 physicians (80 primary care physicians, 80 specialists) surveyed in Spain, 58.1% were male and 88.8% had been qualified to practice for more than five years. Most physicians (> 65%) indicated that 0– 30% of PwD missed or skipped, mistimed, or miscalculated an insulin dose in the last 30 days. Common reasons for these actions were that PwD forgot, were out of their normal routine, were too busy or distracted, or were unsure of how much insulin to take. To optimize insulin dosing, over 75% of physicians considered it very helpful for PwD to have real-time insulin dosing calculation guidance, mobile app reminders, a device automatically recording glucose measurements and/or insulin, having insulin and glucose data in one place, and having the time for more meaningful conversations about insulin dosing routines.
Conclusion: According to physicians’ perspectives, suboptimal insulin dosing remains common among PwD. This survey highlights the need for integrated and automated insulin dosing support to manage the complexity of insulin treatment, improve communications between PwD and physicians, and ultimately improve outcomes for PwD.
Plain Language Summary: In Spain, more than 50% of people with diabetes (PwD) do not reach glycemic targets (glycated hemoglobin [HbA1C] under 7%). While there are many innovations in insulin therapy and device technology, treatment adherence is often poor.
This study presents results from an online survey of physicians’ perceptions of insulin dosing and the barriers and solutions to optimal insulin dosing in Spain. Most physicians indicated that PwD missed or skipped, mistimed, or miscalculated an insulin dose. Common reasons included PwD being out of their normal routine, being too busy or distracted, or being unsure of how much insulin to take. To improve insulin dosing, physicians suggested real-time insulin dosing calculation guidance, mobile app reminders, and a device that automatically records glucose measurements and insulin. Furthermore, having time for more meaningful conversations about insulin dosing routines was found as a solution to improve insulin dosing.There is a need for integrated and automated insulin dosing support to manage insulin treatment, improve communications between PwD and physicians, and improve outcomes for PwD.
Keywords: diabetes mellitus, type 1 diabetes mellitus, type 2 diabetes mellitus, insulin dosing, physicians, Spain, barriers, solutions
Introduction
Diabetes is a severe chronic condition and is becoming a leading cause of blindness, renal failure, lower limb amputation, and cardiovascular disease.1 In 2021, the worldwide prevalence of diabetes was approximately 10.5% among adults aged 20 to 79 years, and this is estimated to increase to 12.2% by 2045.2 In Spain, prevalence rates are estimated to range between 10% and 15%.3
For type 1 diabetes mellitus (T1DM) the current approach for keeping blood glucose levels in a near-normal range is imitating normal insulin secretion with either continuous subcutaneous insulin infusions or multiple doses of insulin.4 Although early treatment in most individuals with type 2 diabetes mellitus (T2DM) is an oral hypoglycemic agent, the progression to insulin is common.5
The achievement and maintenance of glycemic control is important to reduce the risk of diabetes-related complications such as cardiovascular disease and microvascular complications.6 Successful disease management is highly challenging for insulin-treated individuals (who must engage in multiple time-consuming and complex behaviors while trying to live as normal a life as possible) and for their physicians.7 Unsurprisingly, evidence suggests failure to achieve glycemic control at a population level.8 In Spain, 72% of adult individuals with T1DM4 and 54.9% to 55.9% of adult individuals with T2DM do not reach glycemic targets (glycated hemoglobin [HbA1C] under 7%).9 As adequate glycemic control reduces the risk of diabetes-related complications, it is advised that PwD must not miss doses, must take insulin at appropriate times, and take doses accounting for glucose measurements, carbohydrate intake, and physical activity.8
Despite many innovations in insulin therapy and device technology,7 suboptimal dosing continues to be a barrier to the achievement of glycemic control.10,11 Moreover, among those receiving insulin therapy, regimen adherence and intensity may be poor,5,12 resulting in worse glucose control and increased hospital admissions for diabetes-related complications.13,14 In addition, suboptimal glycemic control contributes to excess morbidity and mortality, negatively influences patients’ quality of life, and adds to the societal costs of diabetes.15
For PwD, non-adherence to diabetes management and self-care regimens is common due to patients being busy, traveling, skipping meals, and stress or emotional problems.13 There are many known factors influencing why a patient might deliberately skip or miss treatments, including younger age, lower income, higher education, T2DM, unhealthy diet, increased daily injections, the impact of injections on daily activities, injection pain, and embarrassment.16 Other factors influencing suboptimal glycemic control include poor adherence to self-monitoring of blood glucose regimens, poor adherence to prescribed insulin regimens, diabetes distress, and fear of hypoglycemia.12,15 This is a considerable challenge for insulin treated PwD and the physicians trying to support them.7,8
While the achievement of glycemic control is important to reduce the risk of diabetes-related complications,17 many insulin-treated PwD are still failing to reach glycemic targets.8 With physicians playing a vital role in supporting PwD to navigate the complexities of diabetes treatment, this study aimed to determine physicians’ perceptions of the extent of suboptimal insulin dosing in PwD, and the barriers and solutions to optimal insulin dosing. An understanding of these factors is key to developing coordinated management approaches that integrate the benefits of monitoring, education, and clinical support to facilitate self-care among PwD.8
Materials and Methods
Study Design
A multi-national, cross-sectional, online survey was conducted in the United Kingdom, the United States of America (USA), Germany, and Spain to examine insulin dosing, barriers, and potential solutions for PwD from the perspective of both PwD and physicians. No PwD data was collected in Spain. Findings from the Spanish physician sample are presented here. Details of the multi-national study are reported elsewhere.18 This study was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki and are consistent with Good Pharmacoepidemiology Practices and applicable laws and regulations of the country or countries where the study was conducted, as appropriate. The STROBE checklist was used to inform reporting of the findings.
Participants
Physicians, including general practitioners (GPs) or specialists (diabetologists/ endocrinologists), treating adults with T1DM and/or T2DM were invited to participate. Physicians were required to provide insulin for adult PwD using insulin pens, have at least two years of post-graduate experience, and actively see at least five PwD who use insulin pens per week.
Survey Development
The online questionnaire was informed by a systematic literature review conducted to understand the issues and barriers to suboptimal dosing,8 in discussion with PwD advocates and key opinion leaders in diabetes on issues, behaviors, and barriers to optimal dosing. The questionnaire consisted of 53 questions covering current treatment routines, insulin dosing routines of PwD, insulin dosing issues, and solutions, and took approximately 45 minutes to complete (see Supplementary File 1 for Questionnaire). All sections in the online survey were programmed to prevent the participant from moving on to the next question before completing the previous item. The questionnaire was pilot tested in the USA via virtual web-assisted telephone interviews. After refinement the questionnaire was subsequently translated into Spanish using forward translation with a check of the final version for natural language flow and correctness of medical language.
Recruitment
Physicians were recruited through a company specializing in health outcomes market research. Physicians joined via an online registration tool, where they were informed about study participation, and completed a series of online screening questions to confirm eligibility and an electronic informed consent form before data collection commenced. Additional participants were obtained using peer referral from a list acquisition and custom recruitment methods. The prevalence of diabetes in Spain was considered, and a soft recruitment quota per country of 160 physicians (GPs: n=80; specialists: n=80) was applied to maximize the generalizability of the study findings. All participants were recruited from September 2021 to January 2022. Participants were remunerated for their participation.
Survey Measures
In brief, this analysis included sociodemographic characteristics, missed or skipped, mistimed, and miscalculated bolus/basal insulin dosing factors, and barriers and solutions for optimizing insulin dosing.
Analysis
All analyses were performed using SAS Version 9.4. Descriptive statistics (eg, total number of participants [N], mean, median, standard deviation [SD], range for continuous variables, and frequency and percentages with number of subjects with missing category data for categorical variables) were used to summarize participants’ survey responses. Results are provided overall and by GP/specialist and, where available, results are provided for people with T1DM and T2DM separately. Free-text fields for “other” responses were reviewed with similar responses grouped. Responses were grouped when reported by more than 10% of participants. The answers were then included as an additional category.
Results
Sociodemographic Characteristics, Physician Practice, and Current Treatment Routines
Of the total 640 physicians participating in the global survey, 160 (GPs: n=80; specialists: n=80) were recruited in Spain. In the Spanish sample, 58.1% of physicians were male, 82.5% identified as White race and ethnicity, 88.8% had been qualified to practice for more than five years, and 81.9% provided care for more than ten PwD using an insulin pen regimen in a week. Furthermore, 47.5% and 60.6% of physicians identified that over 91% or more of their PwDs treated with insulin were using insulin pens for T1DM and T2DM, respectively (Table 1). 31.9% and 26.9% of physicians perceived that no more than 30% of their patients with T1DM and T2DM had adequate control of their glucose levels, respectively.
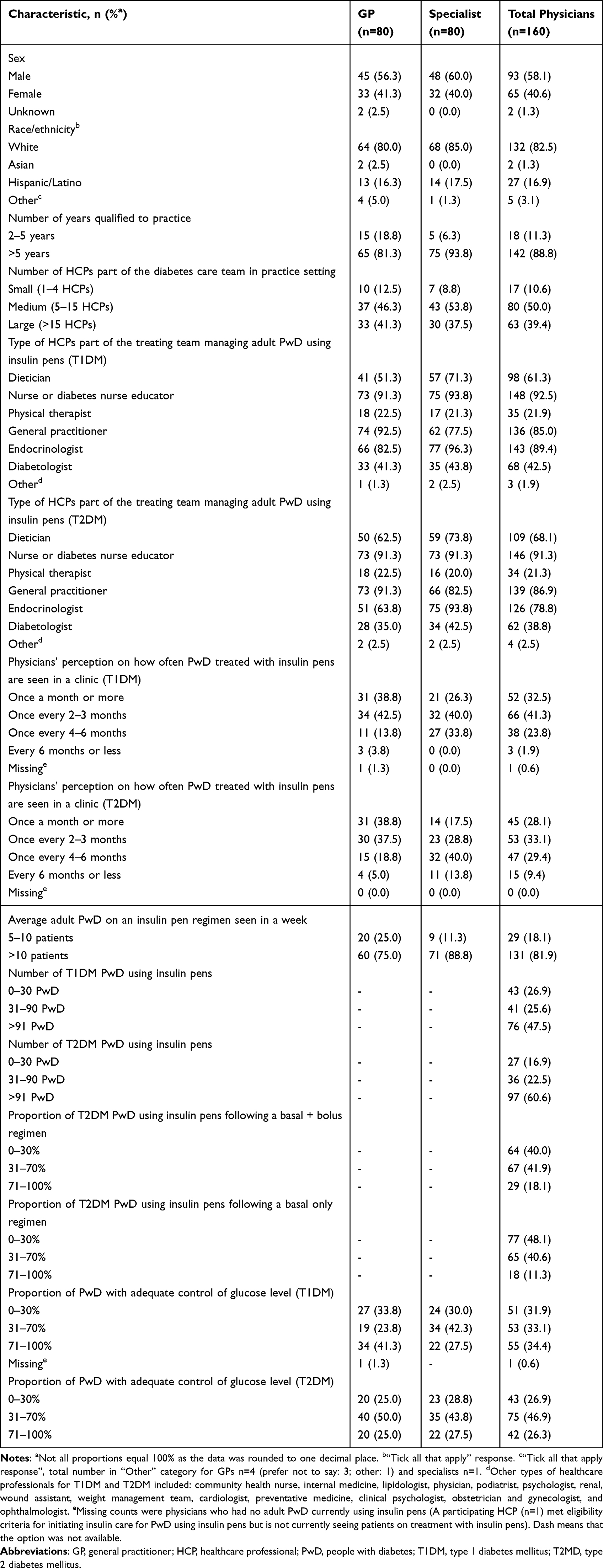 |
Table 1 General Practitioner and Specialist Sociodemographic Characteristics |
Missed, Forgot, or Skipped, Mistimed, Miscalculated Bolus/Basal Insulin Dose
Most physicians (>65%) indicated that 0% to 30% of PwD missed or skipped, mistimed, or miscalculated bolus and basal insulin doses in the last 30 days (Figure 1). More specifically, over 75% indicated that 0% to 30% of PwD missed or skipped bolus and basal insulin doses with similar findings between T1DM or T2DM. Furthermore, over 65% of physicians indicated that 0% to 30% of PwD miscalculated bolus and basal insulin doses with a slightly lower percentage in T2DM patients versus T1DM patients (bolus: 66.3% vs 79.4%, respectively; basal: 81.3% vs 88.8%, respectively).
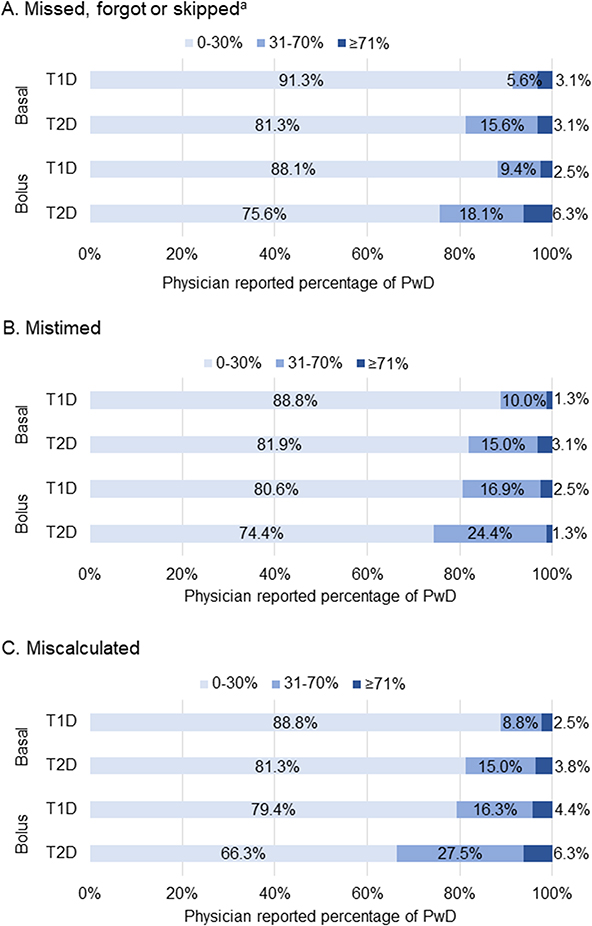 |
Figure 1 Physicians’ perceptions of the percentage of PwD (T1DM and T2DM) who missed, forgot, or skipped, mistimed, and miscalculated bolus/basal insulin dose in the last 30 days. aNot due to skipping a meal. Abbreviations: PwD, people with diabetes; T1D, type 1 diabetes; T2D, type 2 diabetes. |
Physicians’ Perceptions of Reasons for Suboptimal Insulin Dosing by PwD
Physicians perceived similar factors contributed to PwD missing, mistiming, or miscalculating basal/bolus insulin doses. Differences were seen between GPs and specialists for basal insulin for PwD that wanted to avoid their bloods sugar getting too low (missed: 23.8% vs 36.3% and mistimed: 16.3% vs 25.0%, respectively). Furthermore, differences between GPs and specialists were also seen for bolus insulin doses when PwD were not sure how much insulin to take so they did not take any (missed: 15.0% vs 28.8%; mistimed: 23.8% vs 36.3%, respectively). (Table 2 and Table 3).
 |
Table 2 General Practitioner and Specialist Perception of Factors That Cause PwD (T1DM and T2DM) to Miss or Skip, Mistime, or Miscalculate Basal Insulin Dose |
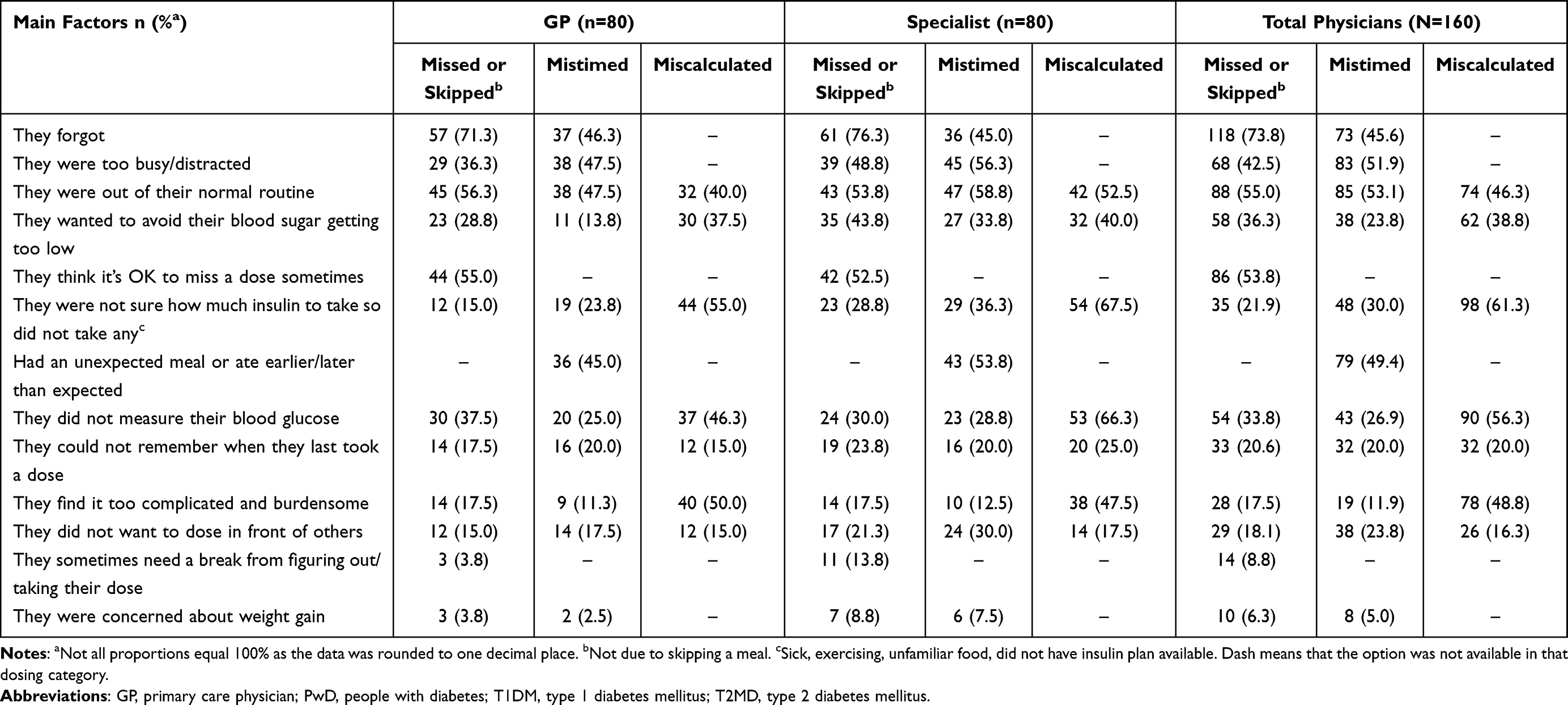 |
Table 3 General Practitioner and Specialist Perception of Factors That Cause PwD (T1DM and T2DM) to Miss or Skip, Mistime, or Miscalculate Bolus Insulin Doses |
Factors identified by physicians for PwD to miss or skip a basal/bolus insulin included they forgot (basal: 67.5%; bolus: 73.8%), they were out of their normal routine (basal: 46.9%; bolus: 55.0%), they were too busy or distracted (basal: 44.4%; bolus: 42.5%), or they thought it was OK to miss a dose sometimes (basal: 38.8%; bolus: 53.8%). Similarly, for mistimed basal/bolus insulin, physicians felt that PwD forgot (basal: 52.2%; bolus: 45.6%), were too busy or distracted (basal: 56.9%; bolus: 51.9%) or were out of their normal routine (basal: 49.4%; bolus: 53.1%). For miscalculated basal/bolus insulin dose, factors included PwD were out of their normal routine (basal: 55.6%; bolus: 46.3%), were not sure how much insulin to take (basal: 49.4%; bolus: 61.3%), or found it too complicated or burdensome (basal: 38.1%; bolus: 48.8%).
Barriers Initiating and Titrating Insulin Dosing
For initiating and titrating insulin, 36.3% and 38.1% of physicians found it slightly difficult having a lack of objective blood glucose data on which to base their decisions (Table 4). For initiating insulin, 41.9% of physicians found taking their PwD’s lifestyle into consideration slightly difficult. Additionally, physicians found it slightly difficult to get their PwD to understand the impact of missing, mistiming, or calculating doses for initiating (33.8%) and titrating (35.6%) insulin. Furthermore, some physicians found the time it takes to convince and educate their PwDs on their insulin regimen or follow their progress moderately difficult for initiating (31.3%) and titrating (25.6%) insulin doses.
 |
Table 4 Physician’s Issues Initiating and Titrating Insulin Dosing (n=160) |
Solutions for Optimizing Insulin Dosing
Overall, physicians felt having more time with PwD to discuss their insulin dosing routines (50.0%), a device that automatically records glucose measurements (50.0%), dosing reminders in a mobile application (43.8%), a device that automatically records insulin doses and timing (43.1%), having a PwD’s insulin and glucose data combined in one place (41.9%), and having real-time insulin dosing calculation guidance (37.5%) would be very helpful for PwD to optimize their insulin dosing (Table 5).
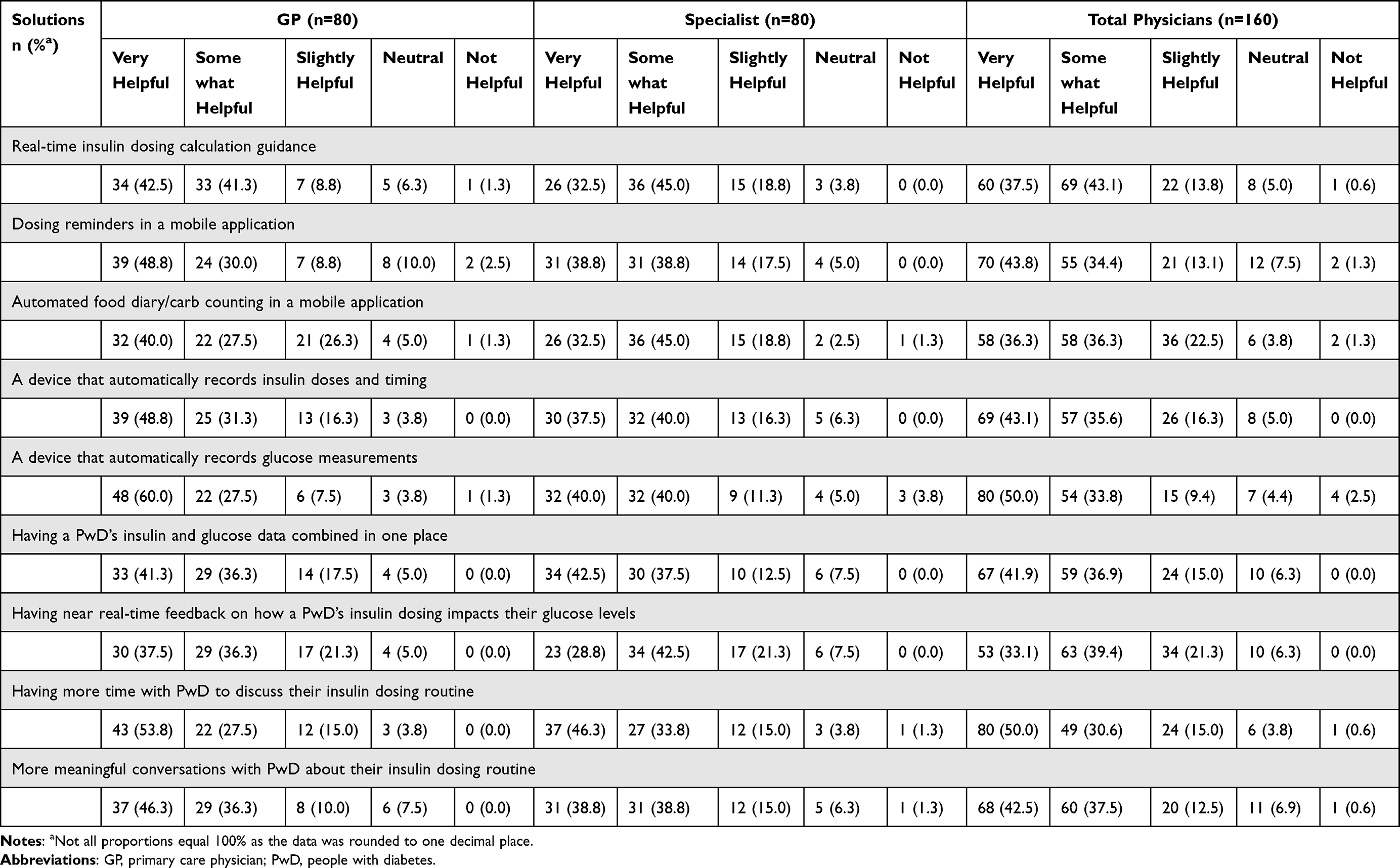 |
Table 5 General Practitioner and Specialist Solutions to Help PwD Optimize Their Insulin Dosing |
Discussion
This study examined physicians’ perspectives on the extent of suboptimal insulin dosing in PwD treated with insulin, as well as barriers and solutions to optimal dosing, indicating that suboptimal insulin dosing behaviors are still frequent despite advances in insulin therapy and technology. Most of the physicians included in this analysis indicated that 30% of PwD missed or skipped, mistimed, or miscalculated a basal and bolus insulin dose in the last 30 days. Common reasons identified by physicians for PwD to miss or skip, mistime, or miscalculate basal/bolus insulin doses included: PwD forgot, were out of their normal routine, were too busy or distracted, or were unsure of how much insulin to take. To optimize insulin dosing, most physicians considered it somewhat or very helpful to have more time with PwD to discuss their insulin dosing routines, a device that automatically records glucose measurements or dosing reminders in a mobile application. Furthermore, having a device that automatically records insulin doses and timing, insulin and glucose data combined in one place or having real-time insulin dosing calculation guidance would help optimize dosing.
Both GPs and specialists in this study perceived that PwD struggled with the complexities of insulin self-management largely for unintentional reasons, such as being out of their normal routine, being too busy or distracted, or being unsure how much insulin to take, resulting in a skipped/missed, mistimed, or miscalculated dose. Similarly, previous research identified factors associated with missed or mistimed insulin doses which were both unintentional (forgetting for various reasons) and intentional (deliberately not taking insulin as directed).8 Forgetfulness can be caused by a disruption in daily routines and interference by social situations.13,19 Furthermore, it has been noted that challenging self-care regimens can lead PwD to experience frustrations and emotional struggles that interfere with glycemic control and increase the risk for diabetes-related complications.20,21 Despite the perceptions of physicians’ participating in this study, previous research indicates that Spanish patients with T2DM report significantly fewer dosing irregularities (missed, mistimed, reduced) compared with patients from other European countries.22
In this study, physicians felt that insulin dosing was complicated and burdensome for PwD and contributed to skipped/missed, mistimed, or miscalculated doses. There is evidence showing that, given the relentlessness of diabetes self-management and the associated burden of insulin regimens, many PwD experience diabetes-related distress and diabetes burnout, wherein they may disengage from self-care tasks.23 Hessler et al found that diabetes-related distress was significantly associated with the frequency of missed bolus insulin doses.24 In a separate review of patients with T2DM in the UK, PwD found self-management challenging and reported feeling defeated and anxious, particularly if they failed to complete their self-care regimens.25
Physicians in this study found it slightly difficult to initiate and titrate insulin, due to a lack of objective blood glucose data, a lack of time to figure out the best approach for an individual PwD, and a lack of time to educate the PwD on their insulin regimen. This is comparable to another extensive study where physicians indicated a lack of time to support or fully understand the concerns of their PwDs and to take an individually tailored approach to treatment.26 Physicians surveyed identified a lack of objective blood glucose data to make decisions on, indicating that perhaps patients were not providing accurate data measurements. A previous study has identified that some PwDs are often reluctant to discuss self-care with their physician and sometimes misrepresent or withhold important information on diet, exercise, blood glucose monitoring, and medication.21 Possible reasons include fear of being judged, not wanting to disappoint their physician, or not understanding the medical recommendations.21 By ensuring GPs and specialists have the time, confidence, knowledge, and opportunity to discuss diabetes and optimal insulin dosing, PwD may, in turn, provide more accurate information and initiate or maintain improved self-care regimens.
Physicians want real-time insulin dosing calculation guidance and a device that automatically records insulin doses and timing for their patients. While there is a lack of evidence about the use and impact of connected insulin devices and diabetes management applications in Spain,27 recent work on the use of Insulclock has shown favorable improvements in glycemic control, as well as a reduction in missed and mistimed insulin doses.28,29 Furthermore, Spain has made a move toward digital health tools with the development of the National Health System’s Digital Health Strategy which aims to empower and involve patients in their disease through the transforming capacity of digital technologies.30 This strategy will enable the development of a National Health Data Space for sharing scientific knowledge and evaluating services, and targeting the 5P (Preventive, Personalized Predictive, Participatory, and Psycho-cognitive) medicine.31 Digital health tools for diabetes, such as continuous glucose monitoring, mobile applications, smart insulin pens, and connection-enabled pen caps/clips and their connection to integrated platforms, have tremendous potential to help people with diabetes to optimize disease management.7
Strengths and Limitations
This study reached its soft recruitment quota of 160 physicians which was based on the prevalence of diabetes in Spain. The survey also ensured equal representation of both GPs and specialists. However, as participation was voluntary, the sample may not fully represent the medical population treating PwD in Spain. Furthermore, the results present physicians’ perceptions of their PwDs so may be missing individual patient nuances. Using a self-report questionnaire meant no qualitative insights from physicians were acquired and the data is subject to recall bias. However, before initiation of the survey, the survey was piloted to examine its validity with revisions made to limit bias and ensure all required information was captured.
Research has often shown discrepancies between the observations of physicians and that of their PwD, with higher rates of missed or mistimed doses being reported by physicians based on the behavior of a typical patient.13 Therefore, to acquire an accurate understanding of the extent and burden of suboptimal insulin dosing, the perspectives of PwD are essential to further validate responses.
Conclusions
Based on physicians’ perceptions, suboptimal insulin dosing remains common for many PwD. This survey highlights the need for having both insulin and glucose data combined in one place and automated insulin dosing support to manage the complexity of insulin treatment, improve communications between PwD and physicians, and ultimately improve outcomes for PwD. Approaches that facilitate better PwD management are needed, particularly those that empower physicians and PwD and improve the meaningfulness of the PwD–healthcare professional relationship and communication. While healthcare professionals recognize that current management is suboptimal, improvements can be achieved by initiating frequent discussions on these issues with patients and providing appropriate education and training.
Abbreviations
GP, general practitioner; HCP, healthcare professional; PwD, people with diabetes; T1DM, type 1 diabetes mellitus; T2DM, type 2 diabetes mellitus.
Data Sharing Statement
The datasets generated during and/or analyzed during the current study are not publicly available as on-going country specific analyses are not yet complete and/or published.
Ethical Approval and Consent to Participate
This study was conducted in accordance with the ethical principles that have their origin in the Declaration of Helsinki and that are consistent with Good Pharmacoepidemiology Practices and applicable laws and regulations of the country or countries where the study was conducted, as appropriate. In Spain the study was submitted to the ethics committee of 12 de Octubre Hospital (Madrid, Spain), which judged that it did not need their approval. A centralized Ethical & Independent (E&I) review service reviewed the conduct of the multi-country study (E&I Study Number 21052-01A, approved on 16-Nov-2021). Informed consent was obtained by the researchers from all individual participants included in the study.
Acknowledgments
The authors would like to acknowledge Caragh Flannery, PhD, for project management support and strategic communication expertise. The authors would also like to acknowledge the Evidera team (Amy Clarke, Monica Hadi, Nicola Barnes, Nashmel Sargano) for the development of the tools, data collection, and reporting.
These data were previously presented in part at the 63 Congreso Nacional de la Sociedad Española de Endocrinología y Nutrición (SEEN) congress: Physicians’ perspectives on the burden of suboptimal insulin dosing in patients with diabetes in Spain. (SEEN, 26-28 Oct, Las Palmas de Gran Canaria, 2022).
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Eli Lilly and Company (Indianapolis, IN, USA).
Disclosure
ND, RSN, EA MRS, JRA and SDC are employees and minor shareholders of Eli Lilly and Company; ES is a contractor at Eli Lilly and Company via HaaPACS, Schriesheim, Germany. VB has received unrestricted research support from Abbott, Novo Nordisk, and Sanofi, and has received speaker/advisory honoraria from Abbott, AstraZeneca, Boehringer Ingelheim, Eli Lilly, Esteve, Janssen, Merck, Mundi- pharma, Novartis, Novo Nordisk, Roche, and Sanofi. JN declares no conflicts of interest.
References
1. Rojo-Martínez G, Valdés S, Soriguer F, et al. Incidence of diabetes mellitus in Spain as results of the nation-wide cohort di@ bet. es study. Sci Rep. 2020;10(1):1–9. doi:10.1038/s41598-020-59643-7
2. Sun H, Saeedi P, Karuranga S, et al. IDF diabetes atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022;183:109119. doi:10.1016/j.diabres.2021.109119
3. Valdes S, Rojo-Martínez G, Soriguer F. Evolution of prevalence of type 2 diabetes in adult Spanish population. Med Clin. 2007;129(9):352–355. doi:10.1157/13109554
4. Gómez-Peralta FME, Conde S, Conget I, Novials A, Novials A. Clinical characteristics and management of type 1 diabetes in Spain. The SED1 study. Endocrinología, Diabetes y Nutrición. 2021;68(9):642–653. doi:10.1016/j.endien.2021.11.020
5. Cramer JA, Pugh MJ. The influence of insulin use on glycemic control: how well do adults follow prescriptions for insulin? Diabetes Care. 2005;28(1):78–83. doi:10.2337/diacare.28.1.78
6. Jude EB, Nixon M, O’Leary C, et al. Evaluating glycemic control in patients with type 2 diabetes suboptimally controlled on basal insulin: UK ATTAIN Real-World Study. Diab Ther. 2019;10(5):1847–1858. doi:10.1007/s13300-019-0667-6
7. Bailey TS, Stone JY, Stone JY. Emerging Technologies for Diabetes Care. Diabetes Technol Ther. 2018;20(S2):
8. Robinson S, Newson RS, Liao B, Kennedy-Martin T, Battelino T. Missed and mistimed insulin doses in people with diabetes: a systematic literature review. Diabetes Technol Ther. 2021;23(12):844–856. doi:10.1089/dia.2021.0164
9. Mata-Cases M, Vlacho B, Real J, et al. Trends in the degree of control and treatment of cardiovascular risk factors in people with type 2 diabetes in a primary care setting in Catalonia during 2007–2018. Front Endocrinol. 2022;12:1884. doi:10.3389/fendo.2021.810757
10. Foster NC, Miller KM, Clements MA, et al. State of Type 1 diabetes management and outcomes from the T1D Exchange in 2016–2018. Diabetes Technol Ther. 2019;21(2):66–72. doi:10.1089/dia.2018.0384
11. Morris AD, Boyle DI, McMahon AD, Greene SA, MacDonald TM, Newton RW. Adherence to insulin treatment, glycaemic control, and ketoacidosis in insulin-dependent diabetes mellitus. The DARTS/MEMO Collaboration. Diabetes audit and research in Tayside Scotland. Medicines monitoring unit. Lancet. 1997;350(9090):1505–1510. doi:10.1016/s0140-6736(97)06234-x
12. C JA. A systematic review of adherence with medications for diabetes. Diabetes Care. 2004;27(5):1218–1224. doi:10.1111/dme.12651
13. Peyrot M, Barnett AH, Meneghini LF, Schumm-Draeger P-M. Insulin adherence behaviours and barriers in the multinational global attitudes of patients and physicians in insulin therapy study. Diab Med. 2012;29(5):682–689. doi:10.1111/j.1464-5491.2012.03605.x
14. Gregg EW, Hora I, Benoit SR. Resurgence in Diabetes-Related Complications. JAMA. 2019;321(19):1867–1868. doi:10.1001/jama.2019.3471
15. Gilbert TR, Blalock O, Polonsky WH, Polonsky WH. Change in hemoglobin A1c and quality of life with real-time continuous glucose monitoring use by people with insulin-treated diabetes in the landmark study. Diabetes Technol Ther. 2021;23(S1):
16. Peyrot M, Rubin RR, Kruger DF, Travis LB. Correlates of insulin injection omission. Diabetes Care. 2010;33(2):240–245. doi:10.2337/dc09-1348
17. Skyler JS. Effects of glycemic control on diabetes complications and on the prevention of diabetes. Clin Diabetes. 2004;22(4):162–166. doi:10.2337/diaclin.22.4.162
18. ISPOR Europe. Patient and health care professional experiences of suboptimal insulin dosing. Value in Health. Vienna, Austria; 2022.
19. Brod MPB, Kongsø JH, Kongsø JH. Insulin administration and the impacts of forgetting a dose. Patient. 2014;7(1):63–71. doi:10.1007/s40271-013-0029-9
20. Rubin RR, Peyrot M. Psychological issues and treatments for people with diabetes. J Clin Psychol. 2001;57(4):457–478. doi:10.1002/jclp.1041
21. Beverly EA, Ritholz MD, Lee Y, et al. Look who’s (not) talking: diabetic patients’ willingness to discuss self-care with physicians. Diabetes Care. 2012;35(7):1466–1472. doi:10.2337/dc11-2422
22. Ampudia-Blasco FJ, Brod M, Brod M. A cross-sectional survey among patients and prescribers on insulin dosing irregularities and impact of mild (self-treated) hypoglycemia episodes in Spanish patients with type 2 diabetes as compared to other European patients. Endocrinología y Nutrición. 2014;61(8):426–433. doi:10.1016/j.endonu.2014.03.008
23. Fisher LPW, Hessler DM, Masharani U, et al. Understanding the sources of diabetes distress in adults with type 1 diabetes. J Diabet Compl. 2015;29(4):572–577. doi:10.1016/j.jdiacomp.2015.01.012
24. Hessler DM, Fisher L, Polonsky WH, et al. Diabetes distress is linked with worsening diabetes management over time in adults with Type 1 diabetes. Diab Med. 2017;34(9):1228–1234. doi:10.1111/dme.13381
25. Psarou A, Cooper H, Wilding JPH. Patients’ Perspectives of oral and injectable type 2 diabetes medicines, their body weight and medicine-taking behavior in the UK: a systematic review and meta-ethnography. Diab Ther. 2018;9(5):1791–1810. doi:10.1007/s13300-018-0490-5
26. Stuckey HL, Vallis M, Kovacs Burns K, et al. “I do my best to listen to patients”: qualitative insights into DAWN2 (diabetes psychosocial care from the perspective of health care professionals in the second diabetes attitudes, wishes and needs study). Clin Ther. 2015;37(9):1986–98.e12. doi:10.1016/j.clinthera.2015.06.010
27. Conget IAE, Duque N, Díaz-Cerezo S, Rubio-de Santos M. Connected insulin systems in diabetes patients in Spain: present and future perspectives. Endocrinología, Diabetes y Nutrición. 2023;70(2):155–157. doi:10.1016/j.endinu.2022.10.006
28. Gomez-Peralta F, Abreu C. O035 Evaluation of the hypoglycaemia predictive algorithm in the insulclock insulin pen cap digital platform in type 1 diabetes treated with insulin multidose. Advan Technol Treat Diab. 2021;2021:1.
29. Gomez-Peralta FAC, Gomez-Rodriguez S, Cruz-Bravo M, María-Sanchez C, Poza G, Ruiz-Valdepeñas L. Efficacy of insulclock in patients with poorly controlled type 1 diabetes mellitus: a pilot. Random Clin Trial. 2020;22(9):686–690. doi:10.1089/dia.2019.0427
30. Secretaría General de Salud Digital. Estrategia de Salud Digital. Sistema Nacional de Salud; 2021:57–58.
31. Pravettoni G, Triberti S. A “P5” approach to healthcare and health technology. P5 eHealth. 2020;2020:3–17.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.