")
Back to Journals » Open Access Emergency Medicine » Volume 15
The Burden and Contributing Factors of Cardiogenic Pulmonary Edema Among Acute Heart Failure Patients Admitted to Tertiary Hospital, Eastern Ethiopia
Authors Degefu N , Jambo A , Nigusse S , Dechasa M , Gashaw T , Getachew M
Received 24 August 2023
Accepted for publication 1 November 2023
Published 9 November 2023 Volume 2023:15 Pages 405—414
DOI https://doi.org/10.2147/OAEM.S436352
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Hans-Christoph Pape
Natanim Degefu,1 Abera Jambo,2 Shambel Nigusse,2 Mesay Dechasa,2 Tigist Gashaw,3 Melaku Getachew4
1Department of Pharmaceutics, School of Pharmacy, Haramaya University, Harar, Ethiopia; 2Department of Clinical Pharmacy, School of Pharmacy, Haramaya University, Harar, Ethiopia; 3Department of Pharmacology, School of Pharmacy, Haramaya University, Harar, Ethiopia; 4Department of Emergency and Critical Care Medicine, School of Medicine, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Melaku Getachew, Department of Emergency and critical care medicine, School of Medicine, College of Health and Medical Sciences, Haramaya University, P.O. Box: 138, Harar, Ethiopia, Tel +251953137119, Email [email protected]
Background: Despite cardiogenic pulmonary edema is the most common phenotype of acute heart failure (AHF), studies on its burden and associated factors are limited. This study aimed to assess the burden and contributing factors of cardiogenic pulmonary edema in patients with acute heart failure admitted to a tertiary hospital in eastern Ethiopia.
Patients and Methods: An institution-based cross-sectional study was conducted on the medical records (n = 276) of patients with AHF between February 01, 2018, and January 31, 2023. A simple random sampling technique was used to select participants from the study population. Bivariable and multivariable logistic regression analyses were used to assess factors associated with the development of cardiogenic pulmonary edema. A P-value ≤ 0.05 was considered as statistically significant.
Results: The prevalence of cardiogenic pulmonary edema was 47.8% in AHF patients. Rural residence (adjusted odds ratio (AOR),9.54), smoking (AOR,3.17), comorbidity (AOR,2.1), and underlying cardiovascular disease (ischemic heart disease, chronic rheumatic valvular heart disease, and hypertensive heart disease with AOR: 6.71, 8.47, and 12.07, respectively) were significantly associated with the development of cardiogenic pulmonary edema in patients with AHF.
Conclusion: Nearly half of the patients with AHF had cardiogenic pulmonary edema. Being a rural dweller, cigarette smoking, comorbidities, and underlying cardiac illness were significantly associated with the development of cardiogenic pulmonary edema in patients with AHF.
Keywords: acute heart failure, cardiogenic pulmonary edema, Ethiopia, tertiary hospital
Background
Acute heart failure (AHF) is a clinical syndrome characterized by a new onset or progression of signs and symptoms of heart failure, which is the leading cause of hospital admission and mortality.1 Cardiogenic pulmonary edema is most often phenotype of AHF.2
Pulmonary edema can be either cardiogenic pulmonary edema or noncardiogenic pulmonary edema.3 Cardiogenic pulmonary edema is mainly caused by left ventricular failure.4 It is a major cause of emergency department (ED) visits in patients with AHF. The major triggering factors for cardiogenic pulmonary edema are acute ischemia or myocardial infarction, hypertension, arrhythmias (particularly atrial fibrillation), and acute regurgitant valvular heart diseases.5 The major treatment option for the management of cardiogenic pulmonary edema includes oxygen and diuretic.6
Cardiogenic pulmonary edema is a life-threatening condition. It is a major health problem, particularly in developing countries. The prevalence of cardiogenic pulmonary edema in patients with AHF is 80%.7 Worldwide, more than 1 million patients are admitted each year with a diagnosis of pulmonary edema secondary to cardiac causes.8 The prevalence of cardiogenic pulmonary edema in AHF with reduced ejection fraction (REF) trials ranged from 75% to 83% and in combined AHF-REF and AHF-PEF (preserved ejection fraction) trials from 51% to 100%.9 In a study done in Addis Ababa, Ethiopia, the prevalence of pulmonary edema among AHF patients was 64.3%.10
To the best of our knowledge, no study has been conducted on cardiogenic pulmonary edema among patients with AHF in Harar, Eastern Ethiopia, which describes the burden and contributing factors of cardiogenic pulmonary edema among patients with AHF. Therefore, the present study provides valuable information on the burden and contributing factors of cardiogenic pulmonary edema among patients with AHF admitted to a tertiary hospital in eastern Ethiopia.
Methods
Study Design, Setting, and Period
An institutional-based cross-sectional study was conducted in a tertiary hospital in Harar, Eastern Ethiopia, from April 1 to April 30, 2023. Harar is the capital of the East Hararghe Zone and the capital city of the Harari regional state of Ethiopia. It is located 526 km from the national capital, Addis Ababa. It has a total population of 246,000, of which 124,000 are males.11 Hiwot Fana Comprehensive Specialized Hospital is the only tertiary hospital in Harar City. Hiwot Fana Comprehensive Specialized Hospital serves as a teaching and referral hospital for eastern Ethiopia, including Eastern Oromia, the Dire Dawa City Administration, the Somali Regional State, and the Harari Regional State. It has a catchment population of 5.8 million.12
Study Participants and Sample Size
The medical records of all adult patients with an admission diagnosis of AHF from February 01, 2018, to January 31, 2023, were reviewed and included in this study. Patients with incomplete information regarding the signs and symptoms of AHF were excluded from this study. The sample size was calculated by using single population proportion considering the following assumptions: where n is the required sample size, Zα/2 = 1.96 at 95% confidence interval (CI), p is the proportion of patients with pulmonary edema among AHF patients, P=64.3%,10 and d is the assumed marginal error (5%), and the sample size was 353. Because the total population was below 10,000, the finite population correction formula was used (n=353 and N=1180), and the sample size was 272. Taking into a 10% contingency, a final sample size of 299 was selected for the present study. A simple random sampling technique was used to select samples from the study population.
Data Collection Methods and Procedures
The collection checklist has been adapted from a previous study.10 The checklist included sociodemographic characteristics (age, sex and residence), smoking status, comorbidities, clinical characterstics (sign & symptoms, and working diagnosis), laboratory and imaging. . Data were collected by two well-trained BSc nurses and a clinical pharmacist.
Operational Definitions
Cardiogenic pulmonary edema: The final diagnosis of acute cardiogenic pulmonary edema was made based on a physician’s diagnosis established according to different parameters: clinical examination, medical history, electrocardiogram, chest X-ray, echocardiographic examination, brain natriuretic peptide results, and response to therapy.13
Comorbidity: is defined as the co-existence of chronic diseases.
Acute heart failure: Signs and symptoms of new onset of heart failure or decompensation or worsening of chronic stable HF.14,15
Data Quality Control
Training was provided to the data collectors regarding the contents of the data collection checklist, data collection procedures, and ethical considerations during data collection. The principal investigator supervised the study. A pre-test was performed at Jugal General Hospital on 5% of patients’ medical records to ensure clarity, avoidance of ambiguity, comprehensiveness, and content uniformity. Adjustments were made to the tool for final data collection. The supervisors checked all the collected data for the completeness of the checklist, and incomplete checklists were discarded before data entry.
Data Processing and Analysis
The collected data were entered into Epi-Data 3.1 and exported to SPSS 27.0. Data were also screened for normality using the Shapiro–Wilk test. Continuous variables are reported as medians (interquartile range (IQR)). Categorical variables were reported as percentages and frequency tables. Bivariable and multivariable logistic regression analyses were used to identify factors associated with the development of pulmonary edema. Variables with p<0.25 in the bivariable stage, were considered for multivariable analysis to control for potential confounders. The variable with a p-value less than 0.05 with the 95% CI in the multivariable analysis was considered significantly associated with the development of cardiogenic pulmonary edema. The goodness of fit of the model was tested using the Hosmer–Lemeshow statistic test. The model was considered a good fit because it was found to be insignificant for the Hosmer–Lemeshow statistic (P = 0.445). A multicollinearity test was performed to determine the correlation between independent variables using correlation coefficients. No variables were observed with a value >0.7, indicating the absence of multicollinearity among the variables in this study.
Results
Socio-Demographic and Clinical Characteristics of the Study Participants
From the 299 patient medical records, 276 (93.3%) medical records of AHF patients were employed for analysis, and 23 (6.7%) were excluded due to incomplete information regarding the admission records. Of the total participants, more than half (147, 53.3%) of them were males. The median (IQR) age was 45 (35–60) years. Majority (167, 60.5%) of the patients were rural dwellers. Nearly one third (94, 34.1%) of the patients were smoking cigarette. More than one third of the patients (107, 38.8%) had comorbidity and around sixteen percent of the patients (44, 15.9%) were taking medication for heart failure. Chronic rheumatic valvular heart disease (CRVHD) (105, 38.0%) was the commonest underlying cardiovascular disease followed by hypertensive heart disease (HHD) (84, 30.4%). Shortness of breath (175, 63.4%) was the commonest chief compliant with the presentation of the patient to the hospital. Majority of the patients had orthopnea (256, 92.8%), postural nocturnal dyspnea (241, 87.3%), hypoxia (229, 83.0%), peripheral edema (208, 75.4%), and S3 gallop (182, 65.9%) (Table 1).
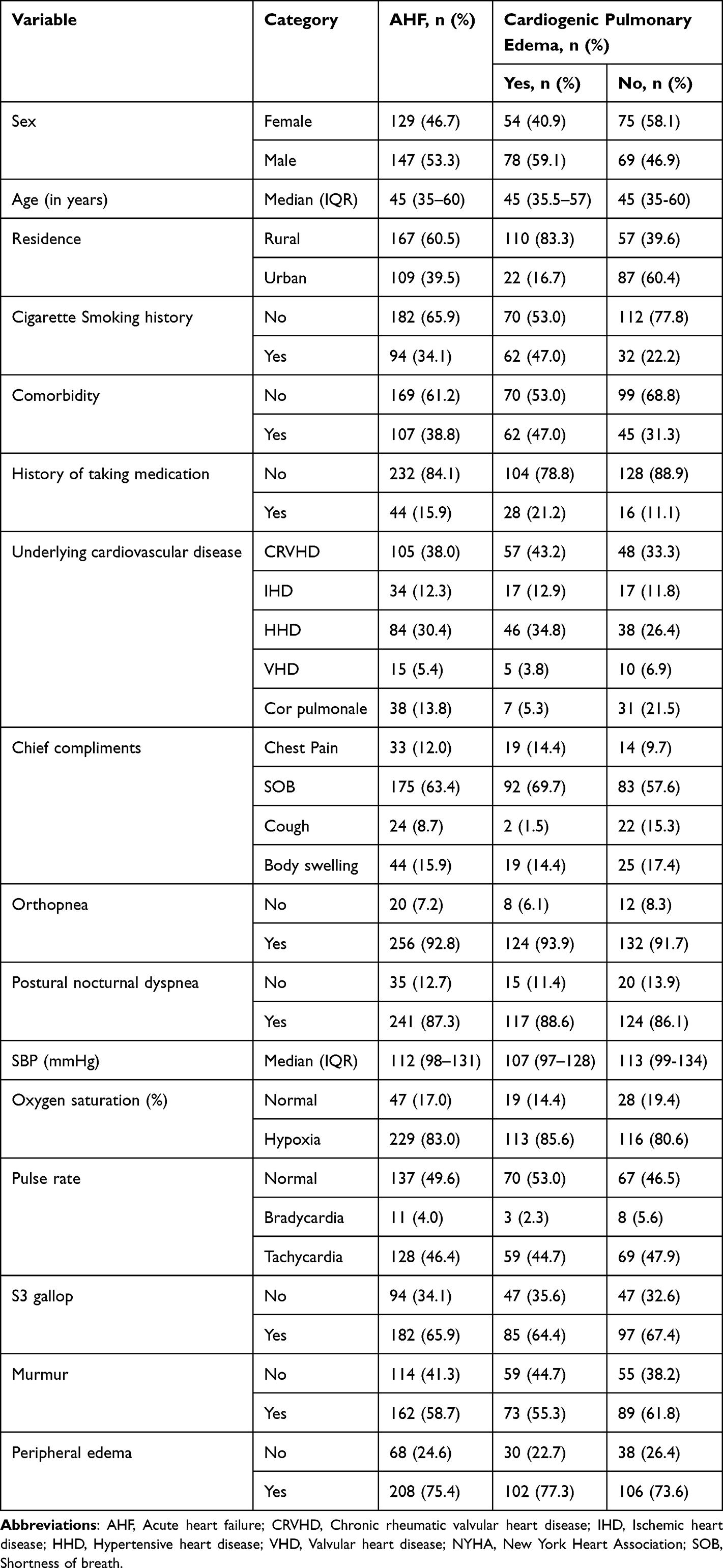 |
Table 1 Socio-Demographic and Clinical Characteristics Among AHF and Cardiogenic Pulmonary Edema Patients Admitted to Tertiary Hospital, Eastern Ethiopia |
The prevalence of cardiogenic pulmonary edema was 47.8% (132) among AHF patients. More than half of patients with pulmonary edema had no history of cigarette smoking (70, 53.0%) and comorbidity (70, 53.0%). Similar to AHF, among patients who had cardiogenic pulmonary edema CRVHD (57, 43.2%) was the commonest cause of underlying cardiovascular disease followed by HHD (46, 34.8%) and ischemic heart disease (IHD) (17, 12.9%). Non-rheumatic valvular heart disease (VHD) and cor pulmonale were the less common presentation of AHF, (15,5.4%) and (38, 13.8%), respectively. Shortness of breath was the commonest (92, 69.7%) chief compliant of patients with pulmonary edema for their hospital visit. Orthopnea (124, 93.9%) was the most common symptom among patients with cardiogenic pulmonary edema. Most of the patient with cardiogenic pulmonary edema were hypoxic at the time of presentation (113, 85.6%) (Table 1). The overall in-hospital mortality of patients among AHF was 8.7%, while patients who had cardiogenic pulmonary edema was 11.4%.
More than half of the patients with AHF and pulmonary edema had normal hemoglobin level, (159, 57.6%) and (83, 62.88%), respectively. The median serum creatinine value was 0.9 mg/dl with IQR of 0.68 mg/dl and 1.23 mg/dl among AHF. Out of 201 participants, who had echocardiography, nearly one third of patients were having reduced ejection fraction. Among AHF patients who had chest x ray (227), pulmonary edema (152, 66.9%) was the commonest finding followed by pleural effusion (167, 60.5%). Among patients who had point of care ultrasound (POCUS) of chest (259), multiple B-lines (234, 90.3%) and pleural effusion (232, 84.1%) were commonly seen in bed side POCUS among patients with AHF. Similarly, multiple B-lines were the commonest finding with POCUS among patient with cardiogenic pulmonary edema (122, 96.8%) (Table 2).
 |
Table 2 Laboratory and Radiologic Characteristics Among AHF and Cardiogenic Pulmonary Edema Patients Admitted to Tertiary Hospital, Eastern Ethiopia |
Infection, hypertension, and anemia were the common precipitating factors for AHF and cardiogenic pulmonary edema (Figure 1).
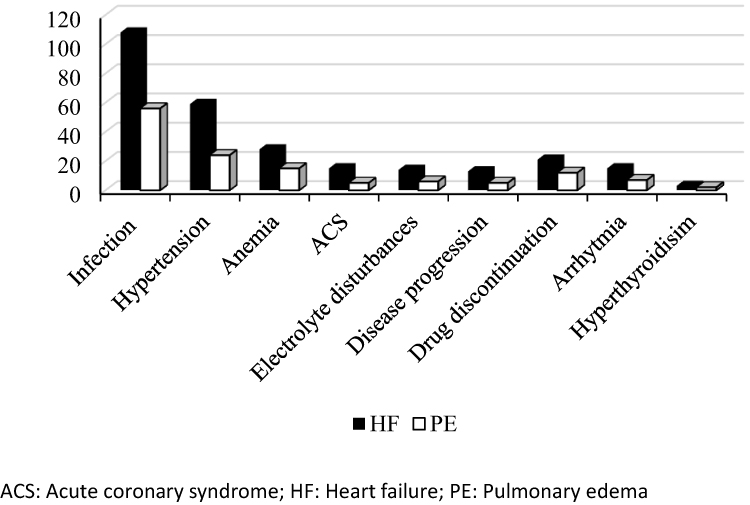 |
Figure 1 Types of precipitating factors among Acute Heart Failure and Cardiogenic Pulmonary Edema patients admitted to Tertiary Hospital, Eastern Ethiopia. |
Factors Associated with Cardiogenic Pulmonary Edema
The variables that had P-value less than 0.25 in bivariable analysis were transformed to multivariable logistic regression. In the final model, sex, residence, cigarette smoking, comorbidity, underlying cardiovascular disease, and systolic blood pressure (SBP) were significantly associated with cardiogenic pulmonary edema as shown in Table 3.
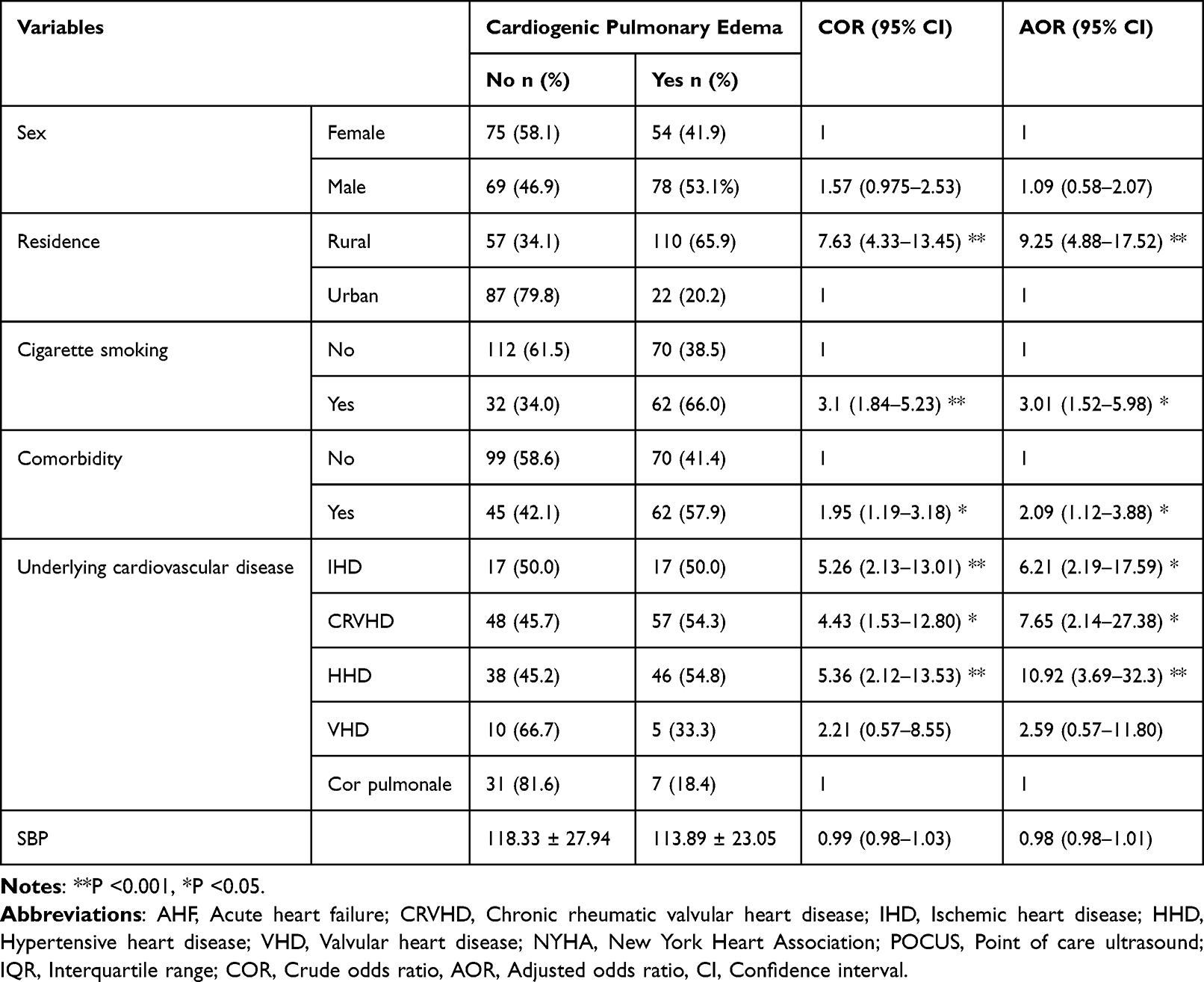 |
Table 3 Factors Associated with Cardiogenic Pulmonary Edema Among AHF Patients Admitted to Tertiary Hospital, Eastern Ethiopia |
The odds of developing cardiogenic pulmonary edema were increased 9.25 times more likely among rural dwellers than urban residents (adjusted odds ratio (AOR): 9.25, 95% CI: 4.88–17.52). Patients who smoke cigarette were 3 times more likely to develop cardiogenic pulmonary edema as compared to those who do not smoke (AOR: 3.01, 95% CI: 1.52–5.98). The odds of cardiogenic pulmonary edema were doubled among patients with comorbidity than those who do not have comorbidity (AOR: 2.09, 95% CI: 1.12–3.88).
The odds of developing cardiogenic pulmonary edema were higher in patients with IHD, CRVHD, and HHD compared to patients who had corpulmonale, (AOR: 6.71, 95% CI: 2.30–19.67), (AOR: 8.47, 95% CI: 2.29–31.33), and (AOR: 12.07, 95% CI: 3.96–36.76), respectively.
Discussion
This study demonstrated that being rural dweller, cigarette smoking, having comorbidity, and underlying cardiac illness were significantly associated with the development of cardiogenic pulmonary edema among patients with AHF.
In this study, the median age of the patients was similar to the previous study conducted in the tertiary hospital Addis Ababa, Ethiopia.10 In contrast to this study, however, our patients are younger than previously reported in the global study and in developed countries (median age 67 to 79 years).16–18 The discrepancy could be due to difference in underlying cardiac illness and modifiable risk factors for cardiovascular disease.
In this study, CRVHD was the most common (43.2%) underlying cardiovascular disease among patients with cardiogenic pulmonary edema. Similarly, a study conducted in the tertiary center in Addis Ababa, Ethiopia,10 also showed that CRVHD was the most common cause of AHF and cardiogenic pulmonary edema. On the contrary, the study done in Spain,19 the Netherlands,20 and Poland21 showed that IHD was the most common cause. This discrepancy was due to poor health-care access and poor living standards resulting in exposure to group A streptococcus, which resulted in high prevalence of rheumatic heart disease in developing countries, Ethiopia.22 The odds of developing cardiogenic pulmonary edema increased among patients with underlying cardiovascular disease of HHD (11 times), CRVHD (7.6 times), and IHD (6.2 times) compared to patients who had corpulmonale (AOR: 6.71, 95% CI: 2.30–19.67). This result supports that cardiogenic pulmonary edema is the result of left ventricular systolic and/or diastolic impairment resulting in increased capillary hydrostatic pressure secondary to elevated pulmonary venous pressure.7
Point of care ultrasound is widely used in emergency and critical care unit or department for the evaluation of AHF.23,24 In the present study, the majority (96.8%) of patients with cardiogenic pulmonary edema had multiple B lines in POCUS. Similarly, the study done by Dobbe et al, the systematic review demonstrates a correlation between sonographic B-lines and cardiogenic pulmonary edema, and the sensitivity and specificity of POCUS for the identification of pulmonary edema was 94.1% and 92.4%, respectively.25 The previous study by Al Deeb et al and Martindale et al revealed that the pooled sensitivity and specificity of cardiogenic lung edema using POCUS with B lines were (94% and 92%) and (85% and 92%), respectively.26,27 The use of reproducible, rapid, non-invasive, and inexpensive POCUS will be helpful in the resource-limited setting of our study area, where there are no specific laboratory tests, such as brain natriuretic peptide and arterial monitoring for pulmonary edema among patients with decompensated AHF.
In the current study, the prevalence of cardiogenic pulmonary edema was 47.8% among patients with AHF. The findings of this study were lower than those reported by Platz et al where the prevalence of cardiogenic pulmonary oedema at baseline in trials enrolling patients with HF-REF ranged from 75% to 83% and in trials enrolling both patients with HF-REF and HF-PEF from 51% to 100%.9 Attias et al also revealed that the prevalence of cardiogenic pulmonary edema was 75% among those with valvular heart disease (mitral regurgitation).13 The findings of this study were higher than those of the study done in 133 centers in 30 countries of European countries (16%) and (30 countries, 133) center.28 In the RO-AHFS registry, pulmonary edema was the second most common clinical profile after ADHF, accounting for 28.7% of the study population. Pulmonary edema was found to be a high-acuity clinical presentation that can be further refined based on the left ventricular ejection fraction and the presenting SBP.29 The difference could be attributed by difference in clinical characteristics, underlying cardiovascular disease and study setting.
In the current study, patients who smoke cigarette were 3.17 times more likely to develop cardiogenic pulmonary edema as compared to those who do not smoke (AOR: 3.17, 95% CI: 1.56–6.43). Cigarette smoking is the leading cause of cardiovascular comorbidities associated with pulmonary endothelial cell injuries or toxicity of smoke exposure, resulting in structural lung disease, reduced lung function, and permanent damage to the air sacs of the lungs.30,31 Having structural lung disease as a result of smoking, the odds of developing cardiogenic pulmonary edema will be high in patients with acute decompensated heart failure.
The odds of developing cardiogenic pulmonary edema were doubled among patients with comorbidities (AOR: 2.1, 95% CI: 1.12–3.92). Triposkiadis et al revealed that there is a complex association between the comorbidities themselves and between the co-morbidities and the cardiovascular system leading to the development of acute decompensated heart failure phenotypes, both the heart failure persevered and the reduced ejection fraction.32 These patients with multiple comorbidities will have polypharmacy that will affect poor adherence to medication and early decompensation for AHF. The odds of cardiogenic pulmonary edema were increased 9.54 times more likely among rural dwellers than urban residents (AOR: 9.54, 95% CI: 4.97–18.30). This could be explained by patients who is from rural area will have health care disparity leads to poor access to health facility, poor literacy level and health seeking behavior which resulted in late visit to tertiary level both diagnosis and management.
In the present study, the common precipitating factors were infection, hypertension, anemia, and discontinuation of drugs. Similar to our study, a previous study done in Ethiopia also showed that pneumonia, atrial fibrillation, anemia, and drug discontinuation were the most common precipitating factors.10 The ALARM-HF and OPTIMISE-HF registry studies also reported infection, ischemia/acute coronary syndrome, and noncompliance to medication were the leading precipitating factors.33,34
Strengths and Limitations
There is a paucity of studies on the prevalence and its associated risk factors of cardiogenic pulmonary edema among AHF patients in resource-limited countries. The present study provides information on the clinical characteristics, underlying cardiovascular disease, comorbidities, and factors associated with the development of lung edema in resource-limited tertiary center in Eastern Ethiopia. The study’s weaknesses were related to its retrospective design, which caused the demographic information gleaned from the review of patient medical records to be less accurate than information gleaned from a prospective study. The other constraint concerned inadequate and incomplete patient medical records, and in many instances, the handwriting of the medical staff made it challenging to understand medical records.
Conclusions
Nearly half of AHF patients had cardiogenic pulmonary edema. Being from rural dweller, cigarette smoking, comorbidity, and underlying cardiac illness were significantly associated with the development of cardiogenic pulmonary edema among AHF patients.
Abbreviations
AHF, acute heart failure; AOR, Adjusted odds ratio; CI, Confidence interval; COR, Crude odds ratio; CRVHD, Chronic rheumatic valvular heart disease; ED, Emergency department; HHD, Hypertensive heart disease; IHD, Ischemic heart disease; IQR, Interquartile range; NYHA, New York Heart Association; PEF, Preserved ejection fraction; POCUS, point-of-care ultrasound; REF, Reduced ejection fraction; SBP, Systolic blood pressure.
Data Sharing Statement
The datasets of this study are available from the corresponding author on reasonable request.
Ethical Consideration
Ethical clearance was obtained from the Institutional Health Research Ethics Review Committee of Haramaya University College of Health and Medical Sciences (reference number: IHRERC/196/2022). Permission was obtained from the chief clinical director of HFCSH to conduct the study. Because this is a retrospective medical record study, patient informed permission was waived, and no personal information was included on the data collection form to maintain confidentiality. All methods were performed in compliance with the Declaration of Helsinki.
Acknowledgments
We extend our gratitude to the College of Health and Medical Sciences at Haramaya University for their support. We would also like to thank the Hiwot Fana Comprehensive Specialized Hospital administrators and medical record room staff for their cooperation during data collection. The results of this study were shared with the emergency medicine staff at the Hiwot Fana Comprehensive Specialized Hospital through a formal presentation.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Kurmani S, Squire I. Acute heart failure: definition, classification and epidemiology. Curr Heart Fail Rep. 2017;14(5):385–392. doi:10.1007/s11897-017-0351-y
2. Ware LB, Matthay MA. Acute pulmonary edema. N Engl J Med. 2005;353(26):2788–2796. doi:10.1056/NEJMcp052699
3. Malek R, Soufi S. Pulmonary Edema, in StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
4. King KC, Goldstein S. Congestive Heart Failure and Pulmonary Edema. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
5. Clark AL. Almanac 2013: heart failure. Heart. 2013;99(21):1562–1566. doi:10.1136/heartjnl-2013-304761
6. Chioncel O, Collins SP, Ambrosy AP, et al. Pulmonary Oedema-Therapeutic Targets. Card Fail Rev. 2015;1(1):38–45. doi:10.15420/CFR.2015.01.01.38
7. Iqbal MA, Gupta M. Cardiogenic Pulmonary Edema. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
8. Go AS, Mozaffarian D, Roger VL, et al. Heart disease and stroke statistics--2013 update: a report from the American Heart Association. Circulation. 2013;127(1):e6–e245. doi:10.1161/CIR.0b013e31828124ad
9. Platz E, Jhund PS, Campbell RT, et al. Assessment and prevalence of pulmonary oedema in contemporary acute heart failure trials: a systematic review. Eur J Heart Fail. 2015;17(9):906–916. doi:10.1002/ejhf.321
10. Tirfe M, Nedi T, Mekonnen D, et al. Treatment outcome and its predictors among patients of acute heart failure at a tertiary care hospital in Ethiopia: a prospective observational study. BMC Cardiovasc Disord. 2020;20(1):16. doi:10.1186/s12872-019-01318-x
11. Ababa A. Federal Democratic Republic of Ethiopia Central Statistical Agency Population Projection of Ethiopia for All Regions at Wereda Level from 2014–2017. Addis Ababa: Central Statistical Agency; 2014.
12. Nigussie S, Treatment Outcome and Associated Factors Among Patients Admitted with Acute Poisoning in a Tertiary Hospital in Eastern Ethiopia: A Cross-Sectional Study. Vol. 10. SAGE Open Med; 2022:20503121221078155.
13. Attias D, Mansencal N, Auvert B, et al. Prevalence, characteristics, and outcomes of patients presenting with cardiogenic unilateral pulmonary edema. Circulation. 2010;122(11):1109–1115. doi:10.1161/CIRCULATIONAHA.109.934950
14. Ponikowski P, Voors AA, Anker SD, et al. 2016 ESC Guidelines for the diagnosis and treatment of acute and chronic heart failure: the Task Force for the diagnosis and treatment of acute and chronic heart failure of the European Society of Cardiology (ESC) Developed with the special contribution of the Heart Failure Association (HFA) of the ESC. Eur Heart J. 2016;37(27):2129–2200. doi:10.1093/eurheartj/ehw128
15. Rodgers BN, Acute decompensated heart failure. 2020.
16. Filippatos G, Angermann CE, Cleland JGF, et al. Global differences in characteristics, precipitants, and initial management of patients presenting with acute heart failure. JAMA Cardiol. 2020;5(4):401–410. doi:10.1001/jamacardio.2019.5108
17. Storrow AB, Jenkins CA, Self WH, et al. The burden of acute heart failure on US emergency departments. JACC. 2014;2(3):269–277. doi:10.1016/j.jchf.2014.01.006
18. Logeart D, Isnard R, Resche‐Rigon M, et al. Current aspects of the spectrum of acute heart failure syndromes in a real‐life setting: the OFICA study. Eur J Heart Fail. 2013;15(4):465–476. doi:10.1093/eurjhf/hfs189
19. Pena-Gil C, Figueras J, Soler-Soler J. Acute cardiogenic pulmonary edema--relevance of multivessel disease, conduction abnormalities and silent ischemia. Int J Cardiol. 2005;103(1):59–66. doi:10.1016/j.ijcard.2004.08.029
20. Germans T, Tim J, Visser CA, et al. Acute pulmonary congestion in patients with systolic heart failure versus diastolic heart failure: experience of a heart emergency unit. Neth Heart J. 2005;13(6):208–213.
21. Fiutowski M, Waszyrowski T, Krzemińska-Pakuła M, et al. Clinical presentation and pharmacological therapy in patients with cardiogenic pulmonary oedema. Kardiol Pol. 2004;61(12):561–9; discussion 570.
22. Dass C. Kanmanthareddy, Rheumatic Heart Disease, in StatPearls. Treasure Island (FL): StatPearls Publishing; 2023.
23. Mayo PH, Beaulieu Y, Doelken P, et al. American college of chest physicians/la société de réanimation de langue française statement on competence in critical care ultrasonography. Chest. 2009;135(4):1050–1060. doi:10.1378/chest.08-2305
24. Hashim A, Tahir MJ, Ullah I, et al. The utility of point of care ultrasonography (POCUS). Ann Med Surg. 2021;71:102982. doi:10.1016/j.amsu.2021.102982
25. Dobbe L, Rahman R, Elmassry M, et al. Cardiogenic Pulmonary Edema. Am J Med Sci. 2019;358(6):389–397. doi:10.1016/j.amjms.2019.09.011
26. Martindale JL, Wakai A, Collins SP, et al. Diagnosing acute heart failure in the emergency department: a systematic review and meta-analysis. Acad Emerg Med. 2016;23(3):223–242. doi:10.1111/acem.12878
27. Al Deeb M, Barbic S, Featherstone R, et al. Point-of-care ultrasonography for the diagnosis of acute cardiogenic pulmonary edema in patients presenting with acute dyspnea: a systematic review and meta-analysis. Acad Emerg Med. 2014;21(8):843–852. doi:10.1111/acem.12435
28. Nieminen MS, Brutsaert D, Dickstein K, et al. EuroHeart Failure Survey II (EHFS II): a survey on hospitalized acute heart failure patients: description of population. Eur Heart J. 2006;27(22):2725–2736. doi:10.1093/eurheartj/ehl193
29. Chioncel O, Ambrosy AP, Bubenek S, et al. Epidemiology, pathophysiology, and in-hospital management of pulmonary edema: data from the Romanian acute heart failure syndromes registry. J Cardiovasc Med. 2016;17(2):92–104. doi:10.2459/JCM.0000000000000192
30. Lu Q, Gottlieb E, Rounds S. Effects of cigarette smoke on pulmonary endothelial cells. Am J Physiol Lung Cell Mol Physiol. 2018;314(5):L743–l756. doi:10.1152/ajplung.00373.2017
31. Milner D. The physiological effects of smoking on the respiratory system. Nurs Times. 2004;100(24):56–59.
32. Triposkiadis F, Giamouzis G, Parissis J, et al. Reframing the association and significance of co-morbidities in heart failure. Eur J Heart Fail. 2016;18(7):744–758. doi:10.1002/ejhf.600
33. Abdo AS. Hospital management of acute decompensated heart failure. Am J Med Sci. 2017;353(3):265–274. doi:10.1016/j.amjms.2016.08.026
34. Mebazaa A, Parissis J, Porcher R, et al. Short-term survival by treatment among patients hospitalized with acute heart failure: the global ALARM-HF registry using propensity scoring methods. Intensive Care Med. 2011;37(2):290–301. doi:10.1007/s00134-010-2073-4
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.