Back to Journals » Journal of Pain Research » Volume 19
The Bidirectional Relationship Between Perioperative Sleep Deprivation and Postoperative Pain — Mechanisms and Clinical Implications: A Narrative Review
Authors Liu J, Liang Z, Wang H, Chen S, Xie Y, Xing F, Wang Z ![]() , Yuan J
, Yuan J ![]()
Received 7 January 2026
Accepted for publication 23 March 2026
Published 31 March 2026 Volume 2026:19 590177
DOI https://doi.org/10.2147/JPR.S590177
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jinlei Li
Jing Liu,1 Zenghui Liang,1 Heng Wang,1 Shuhan Chen,1,2 Yanle Xie,3 Fei Xing,1,2 Zhongyu Wang,1,2 Jingjing Yuan1,2
1Department of Anesthesiology, Pain and Perioperative Medicine, the First Affiliated Hospital of Zhengzhou University, Zhengzhou, Henan, People’s Republic of China; 2Henan Province International Joint Laboratory of Pain, Cognition and Emotion, Zhengzhou, Henan, People’s Republic of China; 3Department of Anesthesiology, Henan Provincial Chest Hospital, Chest Hospital of Zhengzhou University, Weiwu Road, Zhengzhou, 450000, People’s Republic of China
Correspondence: Jingjing Yuan, Department of Anesthesiology, Pain and Perioperative Medicine, the First Affiliated Hospital of Zhengzhou University, No. 1 Jian She East Road, Er Qi District, Zhengzhou, Henan, People’s Republic of China, Tel +86-13513719631, Email [email protected]
Abstract: Although the understanding of pain mechanism and management has made substantial progress, postoperative pain relief is still an important health care problem. Surgical patients also often report preoperative and postoperative sleep problems. Clinical and experimental studies show that chronic pain and sleep disorders influence each other. Pain disturbs sleep, and sleep deprivation or sleep disorders increase pain. However, there are still many problems about the direction of causality between them and the mechanism that may explain their relationship. In-depth subjective and objective evaluation of pain and sleep supports the view that sleep disorder is a more powerful and reliable predictor of pain, and pain is a predictor of sleep disorder. Recent progress in multimodal imaging, molecular biology, and neural circuit analysis has uncovered how sleep deprivation — especially in the perioperative setting — influences pain sensitivity, the transition to chronic pain, and brain function through mechanisms spanning peripheral nerves, the spinal cord, subcortical areas, and cortical structures.
Keywords: postoperative pain, sleep disturbance, sleep deprivation, mechanisms
Introduction
Chronic pain is a major global health burden, affecting approximately 20–30% of the adult population worldwide, with significant implications for quality of life, mental health, and socioeconomic costs. According to the Global Burden of Disease Study, chronic pain conditions—such as low back pain, headache disorders, and osteoarthritis—are among the leading causes of years lived with disability.1 In the perioperative context, inadequate pain management remains a persistent challenge, contributing to delayed recovery, increased opioid use, and the transition from acute to chronic postoperative pain.2
Accumulating evidence has revealed a robust and bidirectional relationship between sleep and pain. Epidemiological studies estimate that individuals with chronic pain are two to three times more likely to experience sleep disturbances than those without pain, while poor sleep quality—particularly insomnia and short sleep duration—has been shown to predict the onset and exacerbation of pain.3 Meta-analyses suggest that sleep problems increase the risk of developing chronic pain by approximately 30–50%, and that improvements in sleep are associated with clinically meaningful reductions in pain intensity.4 Despite this well-established association, the mechanistic pathways linking sleep disruption and pain remain incompletely understood, particularly in the postoperative setting.
Although several reviews have addressed the general relationship between sleep and pain, most have focused on chronic pain populations or experimental sleep deprivation in healthy volunteers. Few have systematically synthesized the bidirectional interplay between postoperative sleep disturbance (PSD) and postoperative pain, especially in light of recent advances in neuroimaging, molecular biology, and neural circuit research. Moreover, the perioperative period offers a unique window to study the dynamic interaction between sleep and pain under controlled surgical and anesthetic conditions.3 Given the increasing recognition of PSD as a modifiable risk factor for poor surgical outcomes, there is a pressing need to update and integrate current knowledge to inform clinical practice and guide future research.
This narrative review aims to: (1) summarize the clinical evidence supporting the bidirectional relationship between postoperative sleep disturbance and pain; (2) synthesize findings from experimental sleep deprivation studies that elucidate causal mechanisms; and (3) explore the underlying neurobiological mechanisms—from peripheral and spinal pathways to brain circuits and molecular signaling—that link sleep disruption and pain processing. By integrating clinical and mechanistic perspectives, this review seeks to provide a comprehensive framework for understanding sleep–pain interactions in the perioperative setting and to identify potential targets for therapeutic intervention.
Methods
We here conducted a literature search of the electronic databases of PubMed, Embase, Web of Science, and Cochrane Library between January 1990 and December 2025, the search terms used including combinations of “postoperative pain”, “sleep disturbanc”, “sleep deprivation” and “mechanisms”. Only peer-reviewed original articles published in English were included in the study. The study selection process for the narrative review is shown in Figure 1. A systematic literature search identified 406 potentially relevant studies. After eliminating duplicates and excluding all ineligible studies, 33 studies were included. Furthermore, two crucial studies retrieved through manual search were also included. Ultimately, 35 studies were included in the narrative review.
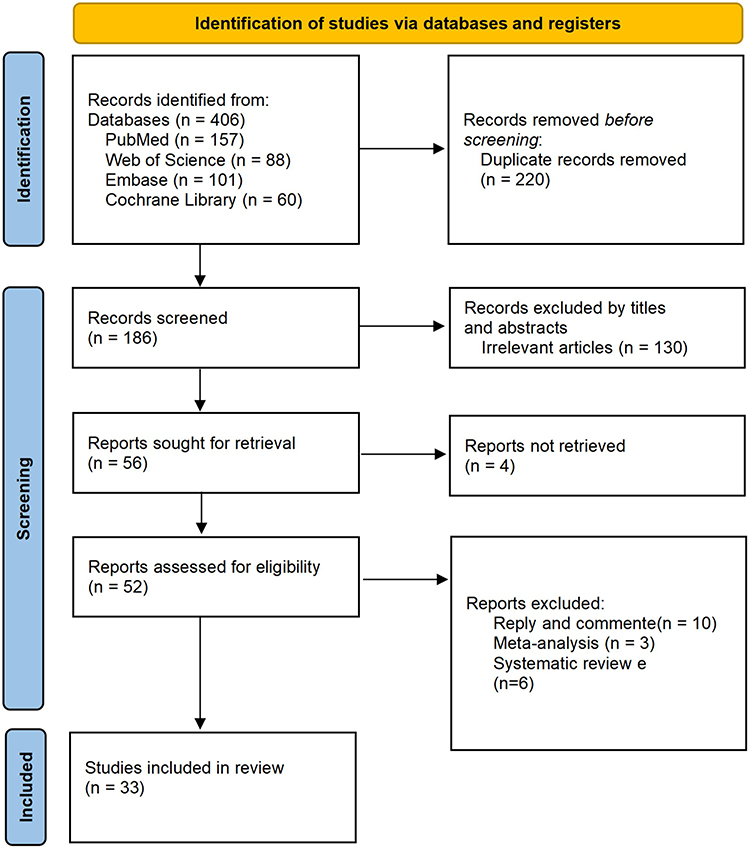 |
Figure 1 Flowchart of study selection. |
The Bidirectional Relationship Between Sleep and Pain Experiences
Postoperative pain and sleep disturbances are two of the most common challenges faced by surgical patients during recovery. Extensive clinical observations and studies have shown that these two issues are not isolated but rather form a mutually reinforcing vicious cycle. For details, see Table 1.
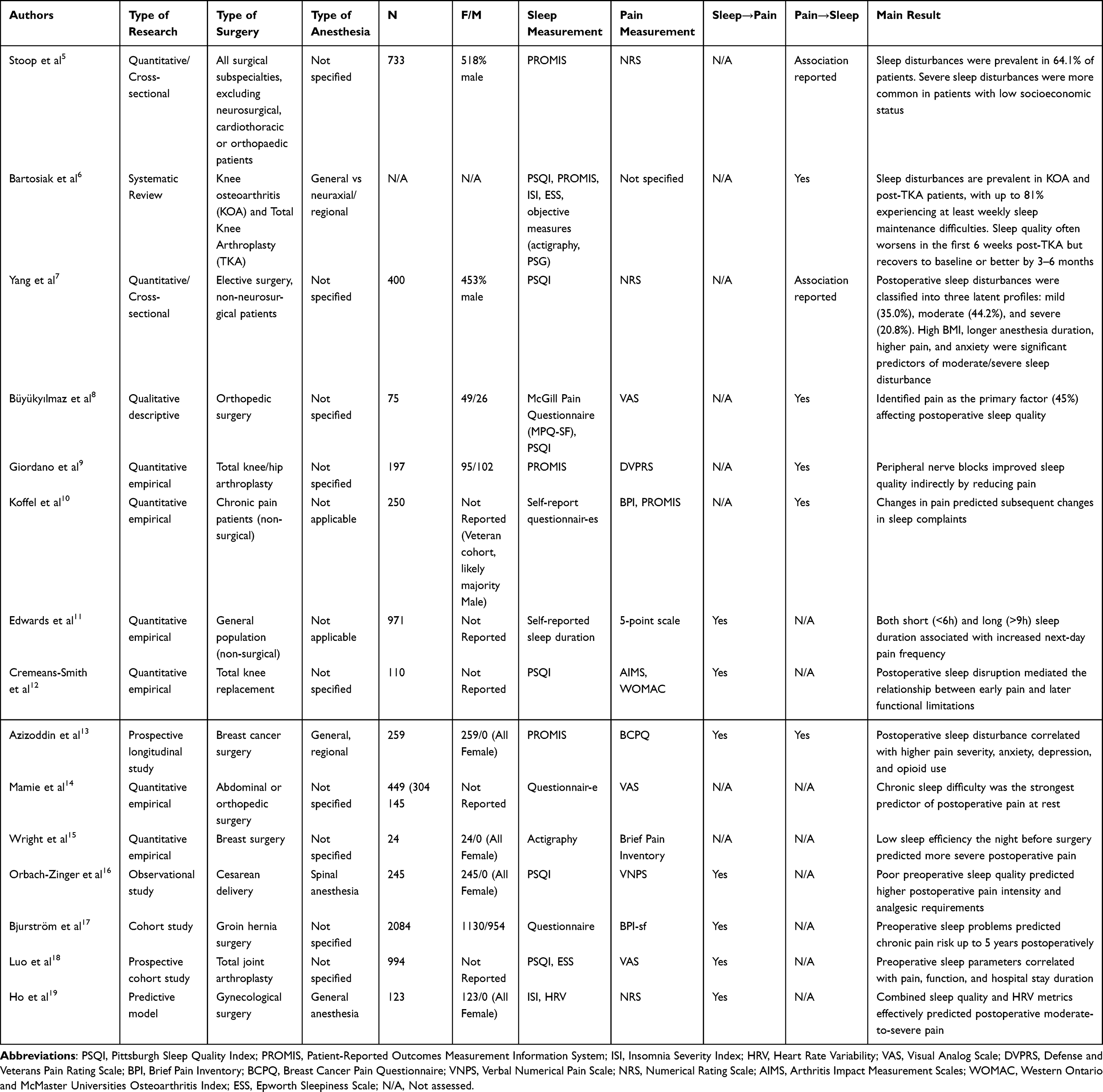 |
Table 1 Clinical Studies of Sleep and Pain in Surgical and Related Populations |
Sleep Disturbances are Prevalent Among Surgical Patients Postoperatively
PSD is a common phenomenon, as evidenced by multiple studies from various perspectives. Stoop et al, in a large Dutch multi-center study, found that 64.1% of surgical patients reported sleep disturbances, establishing PSD as a common perioperative complication. In recent years, research methods have evolved from describing prevalence rates towards exploring patient heterogeneity and underlying mechanisms.5 Bartosiak et al focused on knee arthroplasty patients, highlighting the complex bidirectional relationships between sleep, pain, and psychosocial factors such as anxiety, and emphasizing the high prevalence of obstructive sleep apnea (OSA).6 Yang et al identified three PSD severity subgroups (mild, moderate, severe) using Latent Profile Analysis. They quantified key modifiable risk factors: higher body mass index, longer anesthesia duration, greater pain, and higher anxiety increase the risk of moderate-to-severe PSD. This underscores the heterogeneity of PSD and guides personalized care.7 These studies have all revealed the existence and prevalence of PSD.
Postoperative Pain is a Key Driver of Sleep Disturbances
After establishing the prevalence of postoperative sleep disturbances, researchers began to explore their underlying causes and consistently identified postoperative pain as a critical driver. Büyükyılmaz et al, in their study of Turkish orthopedic patients, explicitly identified pain as the primary factor affecting postoperative sleep quality (accounting for 45%), and found a significant correlation between nighttime pain intensity and deteriorated sleep quality.8 Giordano et al provided corroborating evidence from another angle, demonstrating that effective pain management—specifically, peripheral nerve blocks—indirectly improved postoperative sleep quality by alleviating pain.9 Multimodal analgesic strategies, such as the combined use of dexmedetomidine and regional nerve blocks, can reduce opioid consumption, thereby improving postoperative sleep and cognitive function.20 This indicates that the level of postoperative pain directly determines the severity of sleep disturbances, and pain control is a crucial pathway to improving sleep. Additionally, Koffel et al, in their analysis of data from veterans with chronic musculoskeletal pain, supported this directional relationship, showing that changes in pain predicted subsequent changes in sleep complaints.10
Sleep Disturbances, in Turn, Exacerbate Pain Perception and Delay Recovery
As research deepened, it became evident that the relationship between sleep and pain is not unidirectional; sleep disturbances themselves can exacerbate pain perception, forming a vicious cycle. Edwards et al, in a microlongitudinal study of the general population, first revealed a prospective association between sleep duration and next-day pain reports, finding that both sleeping less than 6 hours and more than 9 hours were associated with increased pain frequency the following day. This finding has been repeatedly validated in surgical populations.11 The study by Cremeans-Smith et al on total knee arthroplasty patients was groundbreaking, as it was the first to confirm that postoperative sleep disruption mediates the relationship between early postoperative pain and later functional limitations.12 In other words, pain not only directly leads to functional decline but also indirectly affects long-term recovery through the intermediary of disrupted sleep. Azizoddin et al, in a longitudinal study of breast cancer patients, also found that postoperative sleep disturbance was significantly associated with higher pain severity, anxiety, depression, and opioid use, highlighting the central role of sleep within the cluster of postoperative negative symptoms.13 The relationship between psychoactive substance use and sleep disturbance extends beyond surgical populations. Large-scale epidemiological studies demonstrate that even single use of opioids or sedatives is independently associated with poor sleep quality, reduced sleep efficiency, and impaired daytime function.21,22 These findings suggest that opioid use may both result from and exacerbate postoperative sleep disturbance, creating a complex bidirectional relationship that warrants careful consideration in pain management strategies.
Preoperative Sleep Disturbance is a Significant Predictor of Acute and Chronic Postoperative Pain
The most clinically proactive finding is that pre-existing sleep problems are an independent risk factor for predicting adverse postoperative pain outcomes. This view has been confirmed across various types of surgery. The early work of Mamie et al identified chronic sleep difficulty as the strongest predictor of postoperative pain at rest.14 Subsequently, Wright et al found that low sleep efficiency the night before breast cancer surgery predicted more severe pain during the first postoperative week.15 Similarly, Orbach-Zinger et al, in a study of women undergoing planned cesarean delivery, showed that those with poor preoperative sleep quality experienced significantly higher pain intensity within the first 24 hours postoperatively and required additional analgesia more frequently.16 Recent research has further revealed its impact on long-term outcomes. Bjurström et al, in patients undergoing groin hernia surgery, found that preoperative sleep problems not only predicted chronic pain at 12 months postoperatively but also the risk of persistent pain at a median follow-up of 5 years.17 Studies by Luo et al and Bjurström et al in patients undergoing total joint arthroplasty further indicated that preoperative sleep disturbances were also associated with poorer joint function, longer hospital stays, and higher opioid consumption postoperatively.18,23 The latest research, such as that by Ho et al, is attempting to combine preoperative sleep quality (eg., Insomnia Severity Index) with intraoperative physiological indicators (eg., heart rate variability) to develop more accurate predictive models for postoperative pain, signaling a move towards personalized and precision medicine in this field.19
Hyperalgesia Induced by Experimental Sleep Deprivation
Experimental sleep deprivation, as a controlled research method, is widely used to investigate the mechanisms by which sleep loss affects pain perception. Experimental, observational, and meta-analytic evidence have elucidated the effects of sleep deprivation on pain (for details, see Table 2).
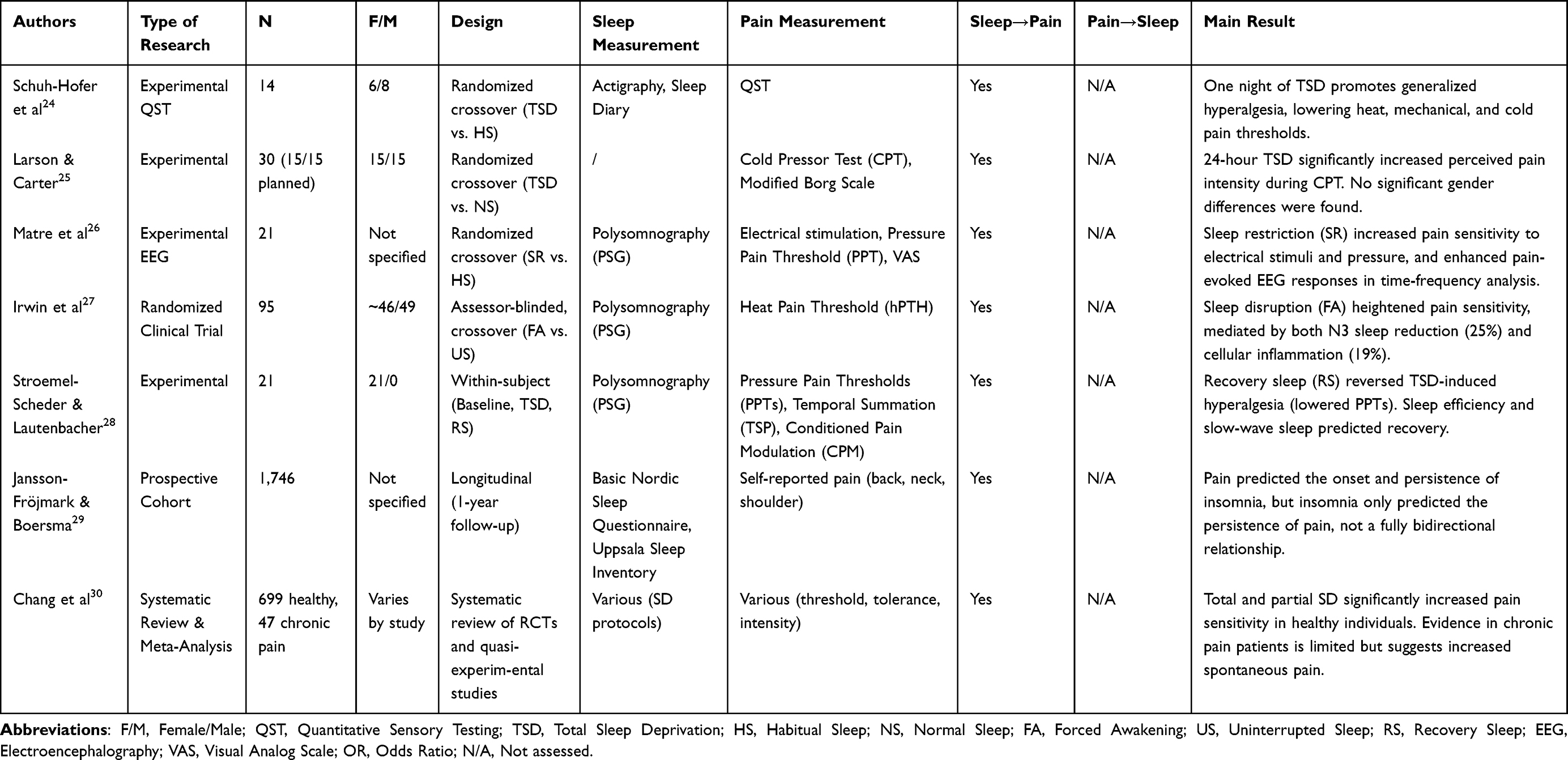 |
Table 2 Experimental and Observational Studies on the Effects of Sleep Deprivation on Pain Perception |
Early Studies: Establishing the Basic Impact of Sleep Deprivation on Pain Perception
Early research primarily focused on the effects of total sleep deprivation on pain perception in healthy populations. For example, Larson and Carter, in their study, they found that 24 hours of total sleep deprivation significantly increased pain ratings in healthy subjects during the cold pressor test, but no gender differences were observed.25 This study systematically evaluated the impact of TSD on clinically relevant pain induced by sustained cold stimulation for the first time, providing an important experimental paradigm for subsequent research.
In the same year, Schuh-Hofer et al used the standardized Quantitative Sensory Testing protocol from the German Research Network on Neuropathic Pain to comprehensively assess the effects of one night of TSD on multimodal nociception.24 The study found that TSD significantly reduced thresholds for heat, mechanical, and cold pain, while non-nociceptive sensory functions remained unaffected. This suggests that TSD-induced hyperalgesia selectively enhances the nociceptive system.
Mechanistic Exploration: From Subjective Pain to Neurophysiological Mechanisms
As research advanced, scholars began to investigate the neurobiological mechanisms underlying the effects of sleep deprivation on pain. Matre et al combined time-frequency electroencephalography analysis and found that sleep restriction increased the magnitude of pain-evoked EEG responses, whereas no changes were observed in the time-domain N2P2 amplitude.26 This indicated that traditional ERP analyses might underestimate the impact of sleep deprivation on pain-related neural activity, and time-frequency analysis offered a new perspective for revealing its neural mechanisms.
Irwin et al further demonstrated in a randomized clinical trial that sleep disruption not only enhanced pain sensitivity but also mediated this effect through dual pathways: reduction in N3 sleep and activation of cellular inflammation. Specifically, N3 sleep accounted for 25.0% of the mediation, inflammation for 19.0%, and the dual mediation pathway accounted for 34.9%.27 This study was the first to quantify the mediating roles of sleep architecture and inflammation in pain perception within a causal framework, providing mechanistic evidence for the “sleep-inflammation-pain axis.”
From Healthy Populations to Clinical Amples: Expansion of Research Subjects
As experimental paradigms matured, researchers began to shift their focus to chronic pain patients. Chang et al, in a systematic review, noted that both total and partial sleep deprivation significantly exacerbated spontaneous pain intensity in individuals with chronic pain, but their effects on pain thresholds and tolerance remained unclear.30 This study emphasized the need to distinguish the effects of different sleep deprivation paradigms on pain outcomes and called for the establishment of standardized experimental protocols.
Jansson-Fröjmark and Boersma, in a prospective study, found that in the general population, pain predicted the onset and persistence of insomnia symptoms, whereas insomnia symptoms were only associated with the persistence of pain, not its onset, partially refuting the hypothesis of a fully bidirectional relationship.29
The Interventional Value of Recovery Sleep
In recent years, researchers have begun to explore the reversibility of pain perception through recovery sleep. Stroemel-Scheder and Lautenbacher found that one night of recovery sleep significantly reversed the decrease in pain thresholds caused by total sleep deprivation, with sleep efficiency and slow-wave sleep duration being important predictors of pain recovery. This provides experimental evidence for intervening in pain by improving sleep quality.28
In conclusion, the academic community generally agrees that: experimental sleep deprivation can induce hyperalgesia; its mechanisms involve multiple pathways including altered central nervous system processing and inflammatory activation; and recovery sleep exhibits some degree of pain-reversing effects. However, the following issues remain controversial: the similarities and differences in the effects of various sleep deprivation paradigms (total, partial, selective, and fragmented) on pain; the differential impacts of sleep deprivation between chronic pain patients and healthy populations; and the interactive effects between sleep architecture and inflammation in mediating pain mechanisms. Future research should further deepen efforts in standardizing experimental paradigms, integrating multi-mechanism analyses, and developing individualized intervention strategies to advance this field toward precision sleep medicine and pain management.
The Mechanism Underlying the Interaction Between Sleep and Pain Has Not Been Fully Elucidated
Sleep and pain are interrelated physiological processes, with sleep disorders and chronic pain frequently co-occurring in clinical settings. However, the underlying neurobiological mechanisms remain incompletely understood. In recent years, advances in multimodal techniques, molecular biology, and neural circuit research have revealed the effects of sleep deprivation—particularly perioperative sleep deprivation—on pain sensitivity, chronic pain development, and brain function across multiple levels, from the periphery and spinal cord to subcortical and cortical regions. The mechanism of the bidirectional relationship between perioperative sleep deprivation and postoperative pain is shown in Figure 2.
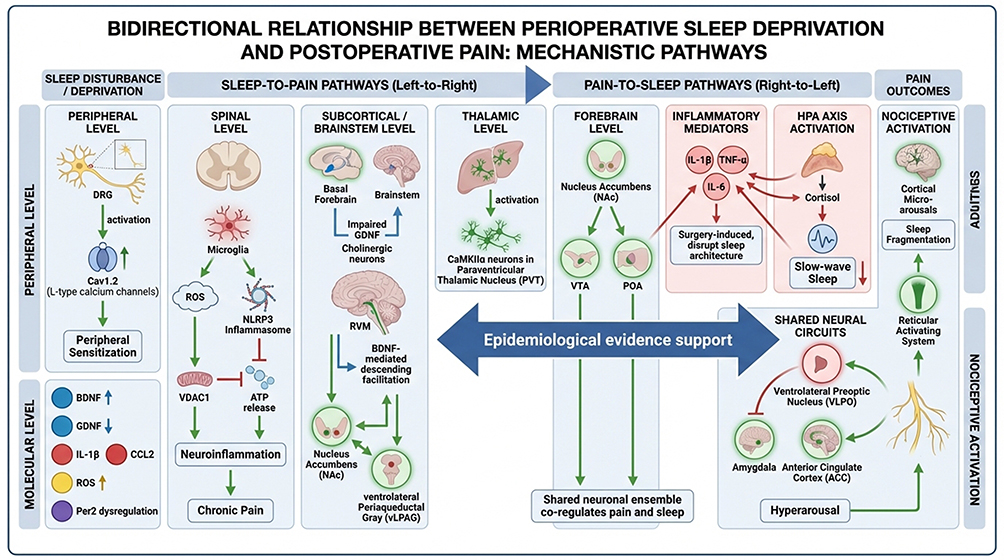 |
Figure 2 The mechanistic pathways of bidirectional relationship between perioperative sleep deprivation and postoperative pain. |
Peripheral and Spinal Mechanisms: L-Type Calcium Channels, Microglial Activation, and Oxidative Stress
Early research focused on the effects of sleep deprivation on peripheral pain transmission pathways, such as the dorsal root ganglion (DRG). Li et al found that perioperative sleep deprivation upregulates the expression and activity of L-type calcium channels (Cav1.2) in the DRG of rats, thereby prolonging postoperative pain recovery. This effect could be reversed using the calcium channel blocker nifedipine or by knocking down Cav1.2, suggesting that L-type calcium channels are important peripheral targets through which sleep deprivation prolongs pain.31 Subsequently, Huang et al further demonstrated at the spinal level that sleep deprivation increases reactive oxygen species (ROS) levels, activates microglia and the NLRP3 inflammasome, and leads to DNA damage and hyperalgesia. These changes could be reversed by the ROS inhibitor PBN.32 Wei et al focused on the voltage-dependent anion channel 1 (VDAC1) signaling in microglia, showing that sleep deprivation promotes VDAC1 oligomerization, increases ATP release and inflammatory factor (IL-1β, CCL2) expression, thereby driving the transition from acute to chronic pain. Inhibiting VDAC1 with DIDS or its oligomerization with VBIT-4 produced analgesic effects similar to those of the microglial inhibitor minocycline.33 Together, these studies elucidate a cascade of mechanisms—involving ion channels, oxidative stress, and neuroimmune responses—through which sleep deprivation promotes pain chronicity at the peripheral and spinal levels.
Brain Region and Circuit Regulation: NAc-vLPAG Functional Connectivity, Basal Forebrain Cholinergic System, and PVT Nucleus
As research has advanced, attention has shifted to the impact of sleep deprivation on central pain modulation networks. Guo et al, using multimodal techniques (fMRI, c-Fos, electrophysiology), found that preoperative acute sleep deprivation (ASD) inhibits functional connectivity and neuronal activity between the nucleus accumbens (NAc) and the ventrolateral periaqueductal gray (vLPAG), leading to postoperative hyperalgesia.34 Sun et al further revealed that a population of D1 neurons in the NAc co-regulates pain and sleep. Projections from these neurons to the ventral tegmental area (VTA) and preoptic area (POA) specifically modulate pain responses and sleep architecture, respectively, providing a unified neural ensemble basis for pain-sleep comorbidity.35 At the subcortical level, Wang et al demonstrated that perioperative sleep deprivation reduces glial cell line-derived neurotrophic factor (GDNF) signaling in basal forebrain cholinergic neurons, leading to neuronal apoptosis and autophagy dysfunction, which promotes chronic postoperative pain. Overexpression of GDNF reversed these effects.36 Li et al focused on the paraventricular thalamic nucleus (PVT), showing that rapid eye movement sleep deprivation (REMSD) activates CaMKIIα neurons in the PVT, prolonging postoperative pain duration. Chemogenetic inhibition of these neurons abolished the pain-promoting effects of REMSD.37 Collectively, these studies progressively map a distributed brain network—spanning the NAc, vLPAG, basal forebrain, and PVT—clarifying how sleep deprivation exacerbates pain by disrupting descending pain modulation and sleep-wake circuits.
Molecular and Signaling Pathways: BDNF, GDNF, and Circadian Genes
At the molecular level, Xue et al were the first to propose that paradoxical sleep deprivation enhances brain-derived neurotrophic factor (BDNF) expression in the rostral ventromedial medulla (RVM), activating descending facilitation pathways and exacerbating incision-induced hyperalgesia. This effect could be reversed by lesioning the dorsolateral funiculus or administering BDNF antibodies.38 Russell et al approached the issue from a circadian rhythm perspective, finding that knockout of the circadian clock gene Per2 disrupts corticosterone secretion rhythms, leads to hypothalamic-pituitary-adrenal (HPA) axis dysfunction, and induces depressive-like behaviors and deficits in startle responses. This suggests that circadian rhythm disruption may exacerbate pain-affective comorbidity via neuroendocrine pathways.39 These findings, together with research on GDNF signaling and inflammatory pathways, collectively construct a molecular network through which sleep deprivation influences pain, encompassing neurotrophic factors, circadian rhythms, stress hormones, and inflammatory mediators.32,33,36
The interaction between sleep and pain involves multiple levels, including peripheral sensitization, spinal immune activation, brain network remodeling, and molecular signaling dysregulation. From early focus on local channels and inflammatory responses to recent emphasis on distributed brain circuits and neurotrophic factor systems, the field is gradually progressing from phenomenological description to mechanistic integration. Future research should adopt cross-level, cross-species strategies to deeply elucidate the neurobiological basis of sleep-pain comorbidity and provide novel insights for developing targeted interventions.
Pain-to-Sleep Mechanisms: Nociceptive Activation, Inflammation, and Stress-Induced Sleep Fragmentation
While the preceding sections detail how sleep deprivation exacerbates pain, the reciprocal pathway—how postoperative pain disrupts sleep architecture—is equally important for understanding the bidirectional relationship. Pain interferes with sleep through multiple interconnected mechanisms involving nociceptive arousal, neuroinflammation, and stress system activation.
Nociceptive arousal and sleep fragmentation. Ascending nociceptive inputs during sleep activate the ascending reticular activating system and trigger cortical micro-arousals, leading to sleep fragmentation and reduced slow-wave sleep. Experimental studies in rodents have shown that nociceptive stimulation during sleep increases the frequency of sleep–wake transitions and suppresses NREM and REM sleep maintenance. In surgical patients, nighttime pain is strongly correlated with the number of awakenings and reduced sleep efficiency.8
Inflammatory mediators as sleep-modulating signals. Surgical trauma induces systemic and central neuroinflammation, with elevated pro-inflammatory cytokines such as IL-1β, TNF-α, and IL-6. These cytokines are well-established somnogenic regulators: IL-1β and TNF-α promote NREM sleep under physiological conditions but, when chronically elevated, disrupt sleep architecture and reduce sleep quality. In the postoperative setting, persistent pain maintains inflammatory signaling, creating a feedback loop where inflammation both amplifies pain and fragments sleep.27
HPA axis activation and stress hormone dysregulation. Pain is a potent activator of the hypothalamic-pituitary-adrenal (HPA) axis, increasing cortisol (corticosterone in rodents) release. Circadian disruption of glucocorticoid secretion—as seen in patients with poorly controlled postoperative pain—impairs sleep continuity and reduces slow-wave sleep. Russell et al demonstrated that disruption of the circadian gene Per2 leads to HPA axis dysfunction and behavioral abnormalities, suggesting a molecular link between pain-induced stress and sleep disruption.39
Shared neural circuits: Pain and sleep regulatory nuclei overlap. Brain regions involved in pain processing—such as the parabrachial nucleus, thalamus, and insula—project to sleep-regulatory centers including the ventrolateral preoptic nucleus (VLPO) and the lateral hypothalamus. Nociceptive inputs can directly inhibit VLPO sleep-promoting neurons, reducing sleep pressure and promoting wakefulness. Conversely, pain-induced activation of the amygdala and anterior cingulate cortex enhances hyperarousal, further disrupting sleep continuity.
Clinical correlation. The clinical relevance of these mechanisms is supported by studies demonstrating that effective pain control—such as peripheral nerve blocks or multimodal analgesia—improves sleep quality postoperatively.9,20 This provides indirect evidence that pain drives sleep disruption through identifiable neurobiological pathways.
Conclusion
Limitations of Current Research
Several methodological limitations should be acknowledged in the context of perioperative sleep and pain research. First, heterogeneity in sleep assessment tools across studies—ranging from subjective scales (PSQI, ISI) to objective measures (actigraphy, polysomnography)—limits cross-study comparability in surgical populations. Second, mechanistic insights derive predominantly from preclinical models, creating translational gaps between rodent studies and human postoperative pain. Third, limited follow-up durations in most clinical studies of surgical patients fail to capture the long-term evolution of sleep–pain interactions and the transition to chronic postsurgical pain. Fourth, inadequate control for confounders specific to the perioperative setting (anxiety, depression, opioid use, surgical factors, anesthetic technique) may introduce bias in effect estimates.
Unanswered Questions in Perioperative Sleep-Pain Research
Key questions remain unresolved in the perioperative context: (1) Do different sleep deprivation patterns (total vs. partial, N3 reduction vs. REM deprivation) exert differential effects on postoperative pain outcomes? (2) What is the role of sex differences in sleep–pain interactions among surgical patients? (3) What is the critical perioperative time window during which sleep disturbance most strongly promotes the transition from acute to chronic postsurgical pain? (4) How do peripheral and central mechanisms interact in surgical patients—does peripheral sensitization from surgical trauma trigger central changes, or do preoperative sleep disturbances prime central pain circuits before surgery?
Controversies in the Field
Three major controversies persist in perioperative sleep-pain research. First, causality direction: Is sleep disturbance a cause or consequence of chronic postsurgical pain? While Jansson-Fröjmark and Boersma29 found in a general population that pain predicted insomnia onset but not vice versa, numerous perioperative studies demonstrate that preoperative sleep disturbance predicts postoperative pain outcomes, suggesting that the causal relationship may differ between surgical and non-surgical contexts. Second, reversibility: Can perioperative sleep optimization completely reverse sleep deprivation-induced hyperalgesia in surgical patients? Evidence from recovery sleep studies in healthy volunteers shows partial reversal with substantial individual variability34, but data in postoperative populations remain limited. Third, mechanism dominance: Are central or peripheral mechanisms primary in mediating the effects of perioperative sleep deprivation on postsurgical pain? Recent discoveries of peripheral L-type calcium channels35 and spinal microglial VDAC1 signaling37 challenge traditional “central dominance” views and suggest that multi-level interventions may be required.
Future Directions for Perioperative Research
Based on the perioperative focus of this review, we propose six research priorities tailored to surgical populations:
- Standardized longitudinal perioperative studies: Implement uniform sleep assessment tools (PSQI + actigraphy) from preoperative baseline through acute recovery to chronic follow-up (6–12 months), with multimodal data collection including inflammatory markers and neuroimaging to identify predictors of chronic postsurgical pain.
- Translational research with surgical relevance: Develop clinically relevant animal models that combine postoperative pain with chronic sleep fragmentation, rather than acute sleep deprivation alone, to better model the clinical reality of surgical patients.
- Sex-specific mechanisms in surgical populations: Ensure adequate female representation in perioperative clinical studies and preclinical surgical models to elucidate hormonal modulation of sleep–pain circuits in the context of surgical trauma and recovery.
- Perioperative sleep-targeted interventions: Conduct randomized controlled trials in surgical patients targeting sleep improvement through preoperative optimization (CBT-I), intraoperative strategies (anesthetic technique), and postoperative interventions (pharmacotherapy, neuromodulation) to establish causality and therapeutic potential for improving postsurgical pain outcomes.
- Multi-omics integration in surgical cohorts: Combine transcriptomics, proteomics, and neuroimaging in well-characterized perioperative cohorts to identify key molecular targets and brain networks mediating the transition from acute to chronic postsurgical pain.
- Mechanism-based therapies for perioperative use: Explore targeted interventions with potential for perioperative application, including L-type calcium channel blockers, ROS inhibitors, VDAC1 inhibitors, GDNF enhancement, PVT modulation, and slow-wave sleep restoration, with careful consideration of safety in surgical patients.
While the bidirectional relationship between sleep and pain is well-established in general populations, its specific manifestations in the perioperative context involve unique considerations related to surgical trauma, anesthesia, and the postoperative recovery trajectory. Mechanistic understanding of how perioperative sleep deprivation influences chronic postsurgical pain remains incomplete, but recent advances have identified promising peripheral, spinal, and central targets for intervention. Addressing the limitations, unanswered questions, and controversies outlined above through rigorous translational research focused on surgical populations will pave the way for mechanism-based perioperative interventions that improve postoperative recovery and reduce the burden of chronic postsurgical pain.
Funding
This research received financial support from the China National Natural Science Foundation (Grant No. 82371235).
Disclosure
The authors declare no conflict of interest.
References
1. Zhang YL, Wu XC, Chen XY, Gao F, Wang J. Global and regional burden, temporal trends, and projections of chronic pain from 1990 to 2032, and its association with cardiovascular diseases: analyses based on global burden of diseases study 2021. Front Public Health. 2025;13:1636949. doi:10.3389/fpubh.2025.1636949
2. Cohen SP, Vase L, Hooten WM. Chronic pain: an update on burden, best practices, and new advances. Lancet. 2021;397(10289):2082–13. doi:10.1016/S0140-6736(21)00393-7
3. Ma D, Li L, Liu W, Xu J. The impact of postoperative pain interventions on circadian rhythm disruptions: mechanisms and clinical implications. Front Neurosci. 2025;19:1543421. doi:10.3389/fnins.2025.1543421
4. George RJ, Kumar R, Achenbach SJ, et al. Sleep disorders in rheumatoid arthritis: incidence, risk factors and association with dementia. Semin Arthritis Rheum. 2025;73:152722. doi:10.1016/j.semarthrit.2025.152722
5. Stoop JM. Prevalence and severity of pain, anxiety, stress, and sleep disturbances among surgical patients: a nationwide single-day multicentre flash mob study. Br J Surg. 2025;112(7):znaf124. doi:10.1093/bjs/znaf124
6. Bartosiak K, Schwabe M, Lucey B, Lawrie C, Barrack R. Sleep disturbances and disorders in patients with knee osteoarthritis and total knee arthroplasty. J Bone Jt Surg. 2022;104(21):1946–1955. doi:10.2106/JBJS.21.01448
7. Yang B, Li J, Feng D, et al. Latent profiles and determinants of postoperative sleep quality in elective surgery patients. Sci Rep. 2025;15(1):617–626. doi:10.1038/s41598-024-84896-x
8. Büyükyılmaz FE, Şendir M, Acaroğlu R. Evaluation of night-time pain characteristics and quality of sleep in postoperative turkish orthopedic patients. Clin Nurs Res. 2011;20(3):326–342. doi:10.1177/1054773811406110
9. Giordano NA, Kent M, Andersen SG, Scott-Richardson M, Highland KB. Postoperative pain mediates the association between peripheral nerve blocks and postoperative sleep following lower extremity arthroplasty. Clin J Pain. 2021;37(7):487–493. doi:10.1097/AJP.0000000000000942
10. Koffel E, Kroenke K, Bair MJ, Leverty D, Polusny MA, Krebs EE. The bidirectional relationship between sleep complaints and pain: analysis of data from a randomized trial. Health Psychol. 2016;35(1):41–49. doi:10.1037/hea0000245
11. Edwards RR, Almeida DM, Klick B, Haythornthwaite JA, Smith MT. Duration of sleep contributes to next-day pain report in the general population ☆. Pain. 2008;137(1):202–207. doi:10.1016/j.pain.2008.01.025
12. Cremeans-Smith JK, Millington K, Sledjeski E, Greene K, Delahanty DL. Sleep disruptions mediate the relationship between early postoperative pain and later functioning following total knee replacement surgery. J Behav Med. 2006;29(2):215–222. doi:10.1007/s10865-005-9045-0
13. Azizoddin DR, Soens MA, Beck MR, Flowers KM, Edwards RR, Schreiber KL. Perioperative sleep disturbance following mastectomy: a longitudinal investigation of the relationship to pain, opioid use, treatment, and psychosocial symptoms. Clin J Pain. 2024;39(2):76–84. doi:10.1097/AJP.0000000000001090
14. Mamie C, Bernstein M, Morabia A, Klopfenstein CE, Sloutskis D, Forster A. Are there reliable predictors of postoperative pain? Acta Anaesthesiol Scand. 2004;48(2):234–242. doi:10.1111/j.0001-5172.2004.00298.x
15. Wright CE, Bovbjerg DH, Montgomery GH, et al. Disrupted sleep the night before breast surgery is associated with increased postoperative pain. J Pain Symptom Manage. 2009;37(3):352–362. doi:10.1016/j.jpainsymman.2008.03.010
16. Orbach‐Zinger S, Fireman S, Ben‐Haroush A, et al. Preoperative sleep quality predicts postoperative pain after planned caesarean delivery. Eur J Pain. 2017;21(5):787–794. doi:10.1002/ejp.980
17. Bjurström MF, Irwin MR, Chen DC, Smith MT, Montgomery A. Sex differences, sleep disturbance and risk of persistent pain associated with groin hernia surgery: a nationwide register-based cohort study. J Pain. 2021;22(11):1360–1370. doi:10.1016/j.jpain.2021.04.008
18. Luo ZY, Li LL, Wang D, Wang HY, Pei FX, Zhou ZK. Preoperative sleep quality affects postoperative pain and function after total joint arthroplasty: a prospective cohort study. J Orthop Surg. 2019;14(1):378. doi:10.1186/s13018-019-1446-9
19. Ho C, Fu P, Hung K, et al. Prediction of early postoperative pain using sleep quality and heart rate variability. Pain Pract. 2024;24(1):82–90. doi:10.1111/papr.13288
20. Ni Y, Yu M, Liu C. Sleep disturbance and cognition in the elderly: a narrative review. Anesthesiol Perioper Sci. 2024;2(3):26–37. doi:10.1007/s44254-024-00066-2
21. Alamir YA, Zullig KJ, Wen S, et al. Association between nonmedical use of prescription drugs and sleep quality in a large college student sample. Behav Sleep Med. 2019;17(4):470–480. doi:10.1080/15402002.2017.1403325
22. Qeadan F, Beaudin S, Reutrakul S, English K. Single use of psychoactive substances and its association with sleep disorders and sleep health in a large US college sample. J Am Coll Health. 2025;73(6):2572–2586. doi:10.1080/07448481.2024.2317171
23. Bjurström MF, Irwin MR, Bodelsson M, Smith MT, Mattsson-C N. Preoperative sleep quality and adverse pain outcomes after total Hip arthroplasty. Eur J Pain. 2021;00:1–11. doi:10.1002/ejp.1761
24. Schuh-Hofer S. One night of total sleep deprivation promotes a state of generalized hyperalgesia: a surrogate pain model to study the relationship of insomnia and pain. PAIN. 2013;0304–3959. doi:10.1016/j.pain.2013.04.046
25. Larson RA, Carter JR. Total sleep deprivation and pain perception during cold noxious stimuli in humans. Scand J Pain. 2016;13(1):12–16. doi:10.1016/j.sjpain.2016.05.037
26. Matre D, Hu L, Viken LA, et al. Experimental sleep restriction facilitates pain and electrically induced cortical responses. Sleep. 2015;38(10).
27. Irwin MR, Olmstead R, Bjurstrom MF, Finan PH, Smith MT. Sleep disruption and activation of cellular inflammation mediate heightened pain sensitivity: a randomized clinical trial. Pain. 2023;164(5):1128–1137. doi:10.1097/j.pain.0000000000002811
28. Stroemel-Scheder C, Lautenbacher S. The effects of recovery sleep on experimental pain. J Pain. 2023;24(3):490–501. doi:10.1016/j.jpain.2022.10.009
29. Jansson‐Fröjmark M, Boersma K. Bidirectionality between pain and insomnia symptoms: a prospective study. Br J Health Psychol. 2012;17(2):420–431. doi:10.1111/j.2044-8287.2011.02045.x
30. Chang JR, Fu SN, Li X, et al. The differential effects of sleep deprivation on pain perception in individuals with or without chronic pain: a systematic review and meta-analysis. Sleep Med Rev. 2022;66:101695. doi:10.1016/j.smrv.2022.101695
31. Li Q, Zhu ZY, Lu J, et al. Sleep deprivation of rats increases postsurgical expression and activity of L-type calcium channel in the dorsal root ganglion and slows recovery from postsurgical pain. Acta Neuropathol Commun. 2019;7(1):217. doi:10.1186/s40478-019-0868-2
32. Huang Y, Hao J, Yang X, et al. Pretreatment of the ROS inhibitor Phenyl-N-tert-butylnitrone alleviates sleep deprivation-induced hyperalgesia by suppressing microglia activation and NLRP3 inflammasome activity in the spinal dorsal cord. Neurochem Res. 2023;48(1):305–314. doi:10.1007/s11064-022-03751-5
33. Wei SN, Zhang H, Lu Y, et al. Microglial voltage-dependent anion channel 1 signaling modulates sleep deprivation-induced transition to chronic postsurgical pain. Sleep. 2023;46(11):zsad039. doi:10.1093/sleep/zsad039
34. Guo M, Wu Y, Zheng D, et al. Preoperative acute sleep deprivation causes postoperative pain hypersensitivity and abnormal cerebral function. Neurosci Bull. 2022;38(12):1491–1507. doi:10.1007/s12264-022-00955-1
35. Sun H, Li Z, Qiu Z, et al. A common neuronal ensemble in nucleus accumbens regulates pain-like behaviour and sleep. Nat Commun. 2023;14(1):4700. doi:10.1038/s41467-023-40450-3
36. Wang D, Wei SN, Zhang L, et al. Impaired basal forebrain cholinergic neuron
37. Li L, Zhang H, Zheng Z, et al. Perioperative sleep deprivation activates the paraventricular thalamic nucleus resulting in persistent postoperative incisional pain in mice. Front Neuroanat. 2022;16:1074310. doi:10.3389/fnana.2022.1074310
38. Xue J, Li H, Xu Z, et al. Paradoxical sleep deprivation aggravates and prolongs incision-induced pain hypersensitivity via BDNF signaling-mediated descending facilitation in rats. Neurochem Res. 2018;43(12):2353–2361. doi:10.1007/s11064-018-2660-2
39. Russell AL, Miller L, Yi H, Keil R, Handa RJ, Wu TJ. Knockout of the circadian gene, Per2, disrupts corticosterone secretion and results in depressive-like behaviors and deficits in startle responses. BMC Neurosci. 2021;22(1):5. doi:10.1186/s12868-020-00607-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.