Back to Journals » Risk Management and Healthcare Policy » Volume 18
The Barthel Index Scale as an Indicator of Nursing Workload
Authors Karavasileiadou S ![]() , Fountouki A, Savopoulos C, Alyami H, HamdanAlshehri H, Theofanidis D
, Fountouki A, Savopoulos C, Alyami H, HamdanAlshehri H, Theofanidis D
Received 4 May 2025
Accepted for publication 20 October 2025
Published 10 December 2025 Volume 2025:18 Pages 3843—3852
DOI https://doi.org/10.2147/RMHP.S533752
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Gulsum Kaya
Savvato Karavasileiadou,1 Antigoni Fountouki,2 Christos Savopoulos,3 Hanan Alyami,4 Hanan HamdanAlshehri,4 Dimitrios Theofanidis2
1Department of Community, Psychiatric and Mental Health Nursing, College of Nursing, Princess Nourah Bint Abdulrahman University, Riyadh, Saudi Arabia; 2Department of Nursing, International Hellenic University, Nea Moudania, Greece; 3 1ST Medical Propedeutic Department of Internal Medicine, AHEPA Hospital, Thessaloniki, Greece; 4Department of Medical and Surgical Nursing, College of Nursing, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia
Correspondence: Hanan HamdanAlshehri, Department of Medical and Surgical Nursing, College of Nursing, Princess Nourah bint Abdulrahman University, Riyadh, 11671, Saudi Arabia, Email [email protected]
Background: The Barthel Index (BI) is a standardized tool used to evaluate patients’ ability to perform daily activities. Lower scores on the index indicate greater dependency. The distribution of nursing workload is often uneven and rarely assessed using validated measures, particularly on busy days, such as those following patient admission days when care demands are higher.
Purpose: This study aims to quantify nursing workload in two hospital wards using the Barthel Index.
Methods: This cross-sectional comparative study collected patient data through direct observation and interviews with all patients in two hospital wards in northern Greece on a busy working day. The 10-item BI was employed to determine each patient’s level of dependency.
Results: A total of 62 patients (31 females; mean age 74.5 years, range 20– 94) participated in this study. Ward A had 12 nurses, while ward B had 13. On a heavy workday, the mean BI score was 45 in ward A and 20 in ward B, indicating higher patient dependency in Ward B.
Conclusion: The BI provides a quick and objective assessment of patient dependency, which reflects nursing workload. Integrating BI assessments into routine practice could support evidence-based staffing decisions and allow for better alignment of nurse allocation with the specific needs of each ward, especially during high-demand periods.
Keywords: Barthel Index, scale, nursing, workload, indicator
Introduction
The Barthel Index (BI) is used to measure the performance of daily life activities, mobility, and functional dependency of patients. Initially, it was developed to monitor performance in chronic pre- and post-treatment patients and to indicate when to move on to rehabilitation.1 The scale was further developed in 1965 by Mahoney and Barthel,2 with scores ranging from 0 to 20. Although the original version is still widely used, it was modified by Granger et al in 1979,3 and since then, the scores have ranged from 0 to 100. Further improvements were introduced in 1989.4 This clinical assessment tool is used for patients with paralysis, stroke, and other neurological conditions, as well as for patients undergoing rehabilitation to assess the final prognosis or possible length of hospitalization or discharge date.5,6
The time required to be filled out by a researcher is 2–5 min or within 10 min if self-administered by the patient. It evaluates 10 activities, eight concerning routine daily life activities and two concerning mobility. Each question is graded with three distinct ratings to indicate whether the patient is dependent/needing considerable support, requires some help, or can perform activities alone. Thus, the patient’s performance for each individual item on the scale is rated as follows: 0 = full dependence, 5 = needs help, and 10 = complete independence. By adding the individual score for each of the 10 items, an overall score is calculated that can range from 0 (total dependence) to 100 (total independence). This final score highlights the amount of time and helps the patient will need.7
Several authors have proposed qualitative categories of scale scores, although these are used mainly for research purposes rather than for routine clinical use. Shah and Muncer (2000)8 proposed the following categories based on the total score: 0 to 20: complete dependence–institutionalization; 20 to 40: heavy dependence–relying on an assistant; 40 to 60: average level of dependence with the possibility of maximum improvement; 60 to 90: light dependence; 90 to 100: independent.9,10
BI is a well-recognized and reliable tool that helps clinicians manage chronic patients.11 In general, the inter-rater reliability and overall performance of BI are excellent (κw 0.98; 95% confidence interval (CI), 0.90–0.96 by random-effects modeling).12,13 The reliability of BI was also examined by comparing nurses and non-clinical assessors (ie, those without a healthcare background), and inter-rater reliability for both total score and individual item score was found acceptable.14
Moreover, Pietra et al (2011)15 compared Barthel telephone interviews with face-to-face administration for 157 patients and found excellent agreement between the two methods, ie, κw was 0.90 (95% CI, 0.85–0.94) for all patients. These results were consistent with an earlier study that compared Barthel telephone interviews with direct administration for 72 patients and obtained a Cronbach’s α score of 0.98.16
Thus, historically, the reliability of BI has been consistently high. Study found acceptable levels of agreement in total BI scores and other assessment tools when predicting discharge destination of older people from acute general medical wards.17 Another study examined four methods for completing the scale in 25 patients: (a) self-completion, (b) completion by a nurse based on clinical impressions, (c) completion by a nurse, or (d) physiotherapist performing the test at the bedside; it found inter-rater reliability to be satisfactory and found an evaluation factor of 0.93 among the four methods. Patients who self-completed the questionnaire provided less reliable results than the other three methods.18
Different studies have shown that BI is a reliable tool even across languages and cultures.19–22 Study done by Dos Santos Barros et al (2022) tested the convergent construct validity of BI with the Karnofsky Performance Scale (KPS) and the European Organization for Research and Treatment of Cancer-Quality of Life Questionnaire (EORTC-QLQ) on a cancer population.6 They confirmed adequate reliability (intraclass correlation coefficient ≥ 0.962) and internal consistency (Cronbach’s α = 0.942). There were adequate correlations between BI and KPS (rho = 0.766) and the functional capacity domain of the EORTC-QLQ (rho = −0.698).
Overall, BI has been widely used for decades in both clinical and academic settings, and its psychometric properties have been well-validated worldwide.23,24 Furthermore, BI has been used as one of the main measures of endpoint outcomes when comparing multimorbid patients nursed under different nursing care systems, and its greater use should be encouraged in Greek healthcare settings.25
The aim of this study was to quantify the nursing workload in two hospital wards using BI. Thus, the tool can be used to depict nursing reality by exploring the clinical severity and level of dependency of patients cared for by ward nurses. Importantly, it can be valuable for emergency admissions and staff allocation to meet irregular demands.
Materials and Methods
This comparative study used a sample of 62 patients from two medical wards (ie, A and B) in one hospital, northern Greece. These were the total admissions in each ward at the time. The Barthel Index (BI) has been culturally adapted and translated into the Greek language, with the 0–100 rating scale, was used to indicate patient burden and nurses workload.26 Which now helps in applying it in various clinical settings, although it should also be clarified that it is not considered to be universally used, nor is it an enforced standard.
Data Collection Sites
Two wards were chosen, both general medical wards, with a maximum capacity of 35 beds each. There were 12 staff nurses for ward A and 13 for ward B. The total staff also included nursing assistants, as their duties are in essence similar to staff nursing duties in Greece. Thus, with respect to skill mix, ward A had 6 nurses and 6 nursing assistants, while ward B had 7 nurses and 6 nursing assistants. All were working on shifts on a rota basis, except for the ward manager and her deputy, both of whom were on routine morning shifts. Therefore, the two wards were similar in terms of staffing levels. In terms of years of average nursing experience, again, the two wards were similar (13 and 14 years, respectively). The nurse gender balance was also similar, with ≤2 males for each ward.
Data were gathered in the patients’ bedsides by directly observing each patients’ abilities to function. BI was applied to all patients in the two wards the day after the hospital was on a 24-h on-call for admissions, ie, Greek hospitals in major cities are on a rotation for new admissions once or twice a week. In terms of case mix, about half of all patients in each ward suffered strokes, while the rest were admitted for other medical conditions, including gastroenteritis, fever, liver or kidney disease, and blood conditions. In this context, it should be noted that in Greek hospitals, there are no stroke units, although there are bays in certain wards that offer specialized care for stroke patients.27
Statistical Analysis
Data were summarized by computing absolute (counts) and relative frequencies (percentages %), measures of central tendency (mean, mode, and median values), and measures of dispersion (minimum and maximum values, standard deviations). The distributions of BI scores between the two wards were compared using the Mann–Whitney test. The distributions of BI class scores between the two wards were compared using the chi-square test. In all testing procedures, the significance level was preset at a = 0.05 (P ≤ 0.05). All statistical analyses were performed using IBM SPSS v.23.
Ethical Considerations
The institutional review board granted its ethical approval from No. 1035/17.12.2019 from Research & Ethics Committee, International Hellenic University. The participants were given an information of the study’s aim by the researchers. The questionannaire and interview included a cover letter that no identifying information was needed and that the survey was anonymous.
Anonymity and confidentiality were respected, and the names of participants or any other element referring to their identities were not used. Instead, patients were numbered and corresponding questionnaires were encoded. Participants were assured that the information to be collected would be used solely for the purpose of the study, and consent forms were obtained accordingly. Furthermore, the participants were as to participate upon their consent and were informed of their right to refuse to participate and withdraw at any time without explanation. This study was conducted in accordance with the ethical standards of the approving committee and complies with the principles outlined in the Declaration of Helsinki.
Results
The sample consisted of 31 male and 31 female patients: 35 in ward A and 27 in ward B. In ward A, there were 16 males and 19 females, while in ward B, 15 and 12, respectively (Table 1). The mean age of the total sample was 74.5 years (range: 20–94). More specifically, the mean age in ward A was 71 years (range: 20–90), multimodal was 76, 83, and 89, and the median was 78. In ward B, the mean age was 78 (range: 62–94), the mode was 75, and the median was 79. In ward A, the youngest patient was diagnosed with gastroenteritis, and his BI score was 100. In contrast, in ward B, the youngest patient was admitted with a severe stroke and a BI class score of zero.
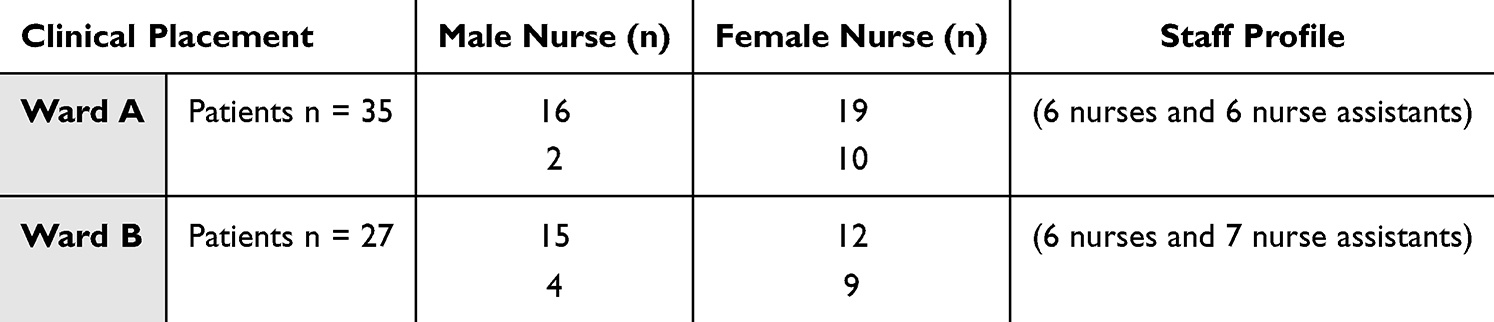 |
Table 1 Number of Staff and Patients in the Two Wards |
Based on the data presented in Table 2, there was a statistically significant difference between the two wards relative to the distribution of BI scores.
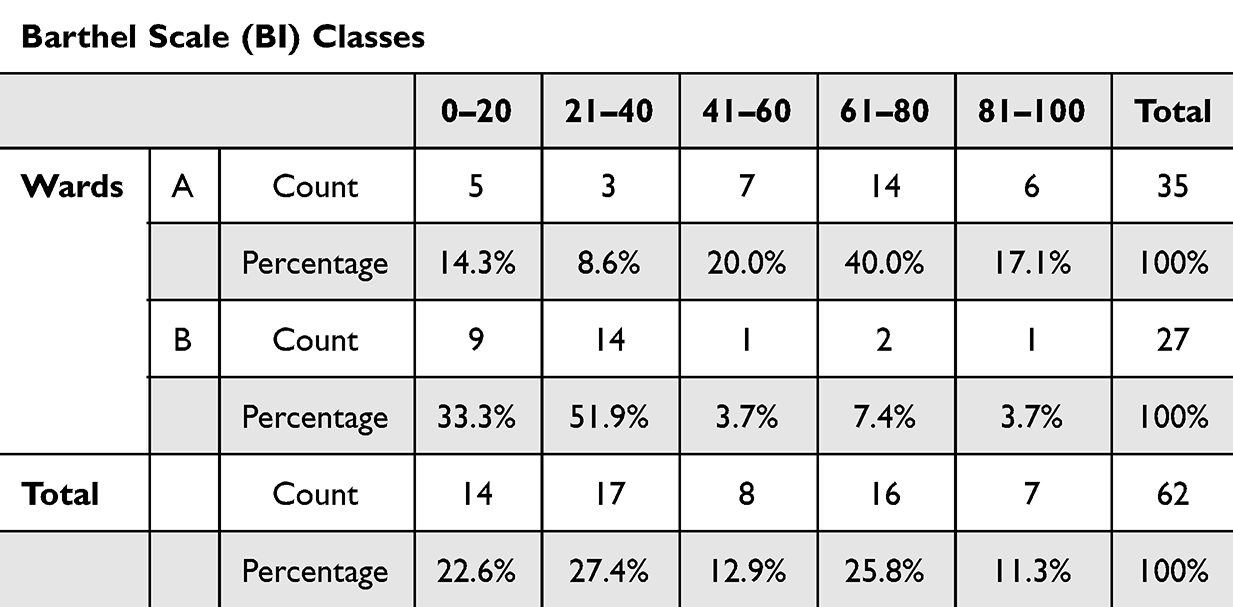 |
Table 2 Distribution of BI Scores Across Wards A and B by Dependency Level |
The chi-square test showed a statistically significant difference between the two wards relative to the distribution of BI class scores (X2 = 24.7, df = 4, P < 0.001, Cramer’s V = 0.631). The data showed that the median BI in ward A was 60, the mean was 60 (SD = 31.059, 95% CI: 49.6–70.3), and the mode was 100, with a range of 0–100. In ward B, the median was 20, the mean was 25.55 (SD = 28.159, 95% CI: 14.4–36.6), and the mode was 20, with a range of 0–100. Thus, the mean difference between the two groups was μ1 − μ2 = 39.45 (95% CI: 24.3–54.5). From this, we conclude that BI scores differed considerably between the two wards, and therefore, the nursing workload in ward B was more demanding despite fewer patients.
Roughly half of the patients in ward A belonged to the “light dependence” category, whereas most patients in ward B fell under the “complete dependence” and “heavy dependence” categories. Yet, despite obvious differences in BI scores and the corresponding nursing workload in the two wards, staffing levels or nurses in each shift were similar, ie, four in the morning, two in the afternoon, and two at night.
Stroke was the most common reason for hospitalization in both wards, ie, 14 and 16 patients, respectively (Table 3). In ward A, for this particular subgroup of patients with a mean age of 81, the mean BI score was 28.2 with a mode of 35 and a median of 40. Similarly, the mean age in ward B was 78, the mean BI score was 9.3, with a mode of 0 and 20, and a median of 5 (Table 4). Thus, the mean difference in the BI score for these patients was 18.9 (SE: 5.1, 95% CI: −29–8.3, df = 25, t-statistic = 3.69, P < 0.05), and the Kruskal–Wallis test showed that the H statistic was 8.1087 (P < 0.05).
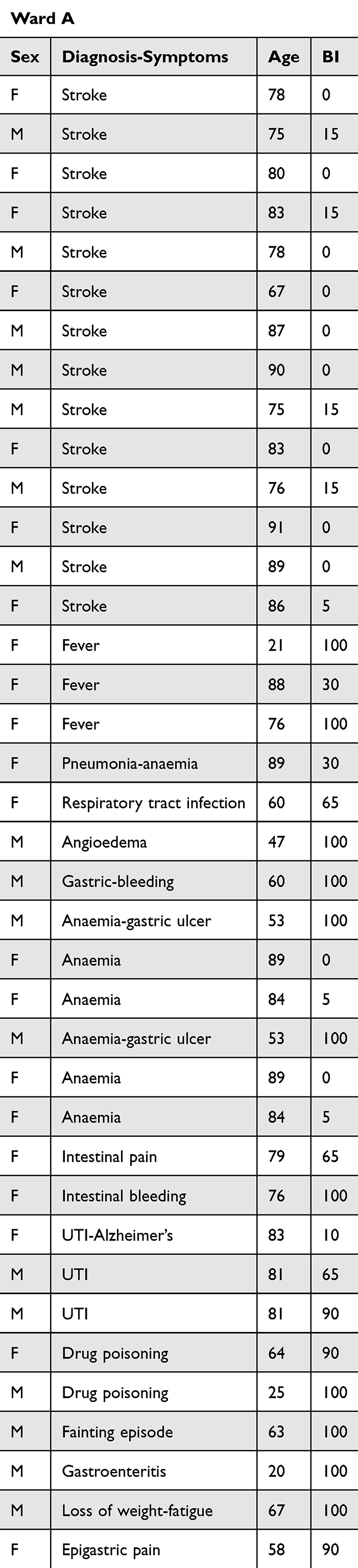 |
Table 3 Patient Case with BI Scores in the Ward A |
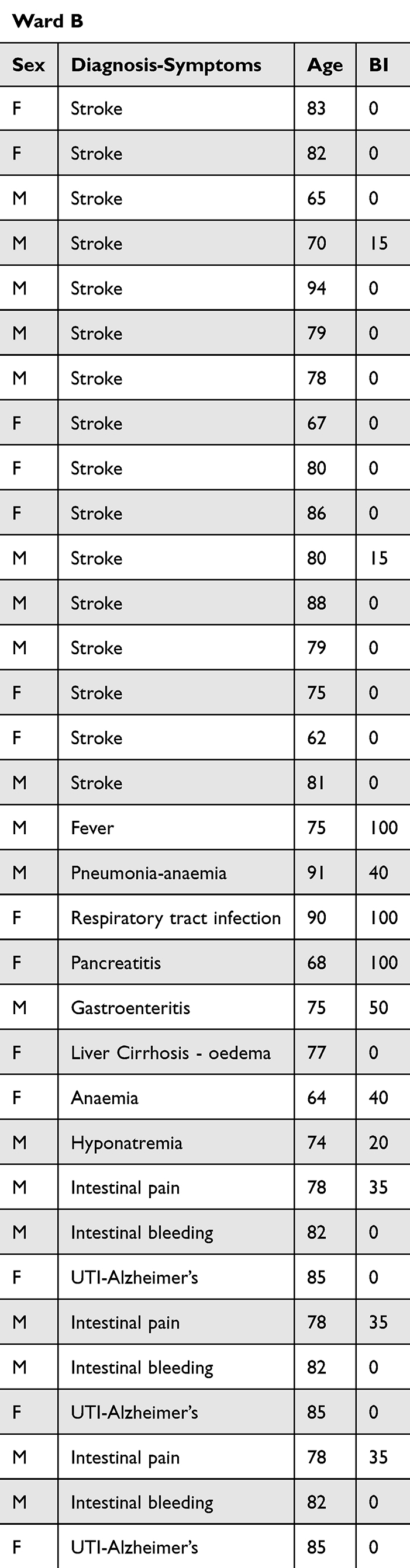 |
Table 4 Patient Case with BI Scores in the Ward B |
With regard to urinary tract infections, there was a pattern showing that patients of similar age had similar (high) BI scores, except for those with concomitant Alzheimer’s disease, whose BI scores fell dramatically. Elderly patients with anemia presented with low BI scores and also needed extra nursing attention. As observed from the results, scores may be affected by many factors. In this case, diagnosis (all stroke cases scored within the 0–20 or “complete dependence” category), age, and gender were three of these factors. Ward A had more females and fewer stroke cases than ward B, which had more males and more stroke cases. In addition, many patients in ward A were aged 60–94 years, but some were aged 20–60 years, as opposed to ward B, which had only elderly subjects aged 60–94 years, resembling a geriatric ward rather than a general medical ward.
Based on the data, the BI score was anticipated to be lower in ward B. Almost 80% of ward B produced a score of 0–20 (ie, “complete dependence”), as would be expected in relation to ward A, where the corresponding portion was almost 50%.
Discussion
This study indicates that BI, a well-established tool for measuring dependency levels in hospitalized patients, can be further used to assess nursing workload. It is a convenient method of measuring patient dependency, despite not including actual clinical tasks of nurses, and it can provide insight into nursing workload to help a ward manager deduce appropriate staffing demands.
On a relatively heavy workday (ie, following a rota admission day), a tool to rapidly assess the potential nursing workload would be beneficial for both staff and patients, as the staffing level would closely correspond to ward needs. This would be especially valuable where there have been serious emergency admissions and problems allocating staff to meet irregular demand.
BI has been proposed as a standard marker for clinical and research purposes. According to the literature, BI is as good as any other instrument at measuring disability, and we recommend that further testing be conducted for potential use in assessing nursing workload.27–29 BI is a user-friendly tool with proven validity and reliability. Although it has been extensively used globally, it has certain limitations in its implementation and evaluation. For instance, it is limited to numerical increases or decreases in the overall score, making it inappropriate for clarifying the clinical significance of the scores or the details of the changes in scores.30
It is also worth mentioning that most patients in both wards were admitted for acute stroke, and in all cases, their BI scores were consistently lower than those of non-stroke patients. Thus, stroke patients had a BI score of ≤15, falling in the category of “complete dependence–institutionalization”. For these particular patients, the nursing workload would be demanding. It should also be noted that the hospital where this study was conducted neither had a stroke unit nor a specialized unit for stroke. Therefore, stroke patients of all ages were admitted to ordinary medical wards and possibly missed out on the highly sophisticated therapies and care offered in stroke-focused clinical settings.
Increased nursing workload also depends on the number of nurses working on a particular day. For example, we observed that on the day after an on-call day, four nurses were working in both wards (including the ward manager and her deputy, both of whom were neither routinely nor directly involved in clinical care delivery) in the morning shift, two nurses were working in the afternoon, and two nurses at night. This is a standardized staff allocation arrangement for most hospitals in Greece.31 In both wards, the case mix was heavy and difficult due to a lack of sufficient nursing staff. Thus, the department’s needs were not fully covered, especially in light of such low BI scores. In essence, the results showed that, according to the recorded BI scores, the nursing workload in ward B was more demanding, and it would have been wise to have access to more nurses for the day.
The study’s findings strongly support the use of Barthel Index (BI) scores as a reliable measure of varying patient care demands, particularly in general hospital settings without specialized units. This evidence provides a strong rationale for integrating the BI into staffing and planning decisions, offering a practical solution for healthcare systems such as Greece’s, which often face staffing shortages and nurse-to-patient ratio challenges.
Although the BI has certain limitations, most particularly its lack of clinical specificity, the discussion highlights its strengths in terms of reliability, uniformity, and validity, making it well-suited for busy clinical environments. Importantly, the research highlights the critical connection between workload and staff allocation policies, emphasizing the need for further investigation to optimize this relationship.
Standardized tools like the BI can also enhance the perceived value of nursing, particularly in healthcare systems where the profession remains undervalued. Future research should therefore examine the long-term utility of the BI across diverse care settings, ideally through multi-site or longitudinal studies. In contexts where specialized stroke units are absent, the incorporation of functional assessments such as the BI represents both a challenge and an opportunity, as they can help compensate for limited resources while supporting more equitable and effective staffing decisions.
However, there is no globally agreed upon instrument for measuring physical disability or patient burden for clinical or research use. It has been argued that accepting a standard daily activity measurement tool could increase awareness of the problems surrounding patient needs and care, thus improving the clinical management of patients. Moreover, using a specific measurement tool could increase the “perceived value” of nursing care and nursing workload.
Limitations
This study has some notable shortcomings, and thus, the conclusions should be read with the following in mind: the number of cases in each ward was too low to make any meaningful comparisons regarding diagnoses and BI scoring, and for stroke, which was the most common diagnosis, patient numbers do not allow for meaningful statistical comparisons. In addition, the full extent of the nursing shift workload, including concomitant situations or clinical tasks such as complicated drug preparation and elaborate administration, was not recorded. However, this study revealed a particular strength, ie, BI can constitute a practical and easy-to-use hands-on reference for estimating nursing workload, providing a more accurate and pragmatic assessment of its effect on care delivery, quality of care, and nursing burnout.
Clinical Implications
BI is a useful tool in clinical practice, as the findings of this study suggest, because the use of the tool can help patients acquire some degree of self-awareness of what they are able to do. The tool may also be of much use to nurses and their managers in particular, as it can monitor the nursing workload needed per shift. Nursing managers need to understand that, in terms of hands-on nursing load (ie, handling, mobilizing, and feeding), the closer the patient reaches a score of 100, the less burdensome the nurse’s job is, and the closer the score is to 0, the heavier and demanding it becomes.
Conclusions
The Barthel Index (BI) has emerged as an important index of the nursing workload and patient dependency as corroborated by the study’s findings: lower BI scores correspond to higher nursing effort. These results support the BI potential for more equitable staff allocation, particularly in environments where nursing staff are systemically underappreciated. Its potential for increased use across the field of nursing, and integration with electronic nursing documentation systems, would streamline workflows, and its reliability is an important consideration. On the other hand, popular nursing workflows and BI do not take emotional or other burdens such as folding adminsitartive responsibilities out into consideration. Additionally, the findings of the study, which was conducted in a single a hospital’s two wards, limit the findings’ external validity. Therefore, generalizability and accurate assessment of the BI across various healthcare environments demand further study with greater heterogeneity and larger populations.
Funding
This study was supported by Princess Nourah bint Abdulrahman University Researchers Supporting Project Number PNURSP2025R873, Princess Nourah bint Abdulrahman University, Riyadh, Saudi Arabia.
Disclosure
The authors declare that there are no conflicts of interest related to this manuscript.
References
1. Mahoney F, Wood O, Barthel D. Rehabilitation of chronically ill patients: the influence of complications on the final goal. South Med J. 1958;51(5):605–609. doi:10.1097/00007611-195805000-00011
2. Mahoney F, Barthel D. Functional evaluation: the Barthel Index. Md Med J. 1965;14:61–65.
3. Granger C, Hamilton B, Keith R, Zielezny M, Sherwin F. Advances in functional assessment for medical rehabilitation. Top Geriatr Rehabil. 1986;1(3):59–74. doi:10.1097/00013614-198604000-00007
4. Shah S, Vanclay F, Cooper B. Improving the sensitivity of the Barthel index for stroke rehabilitation. J Clin Epidemiol. 1989;42(8):703–709. doi:10.1016/0895-4356(89)90065-6
5. Uchinaka EI, Hanaki T, Morimoto M, et al. The Barthel index for predicting postoperative complications in elderly patients undergoing abdominal surgery: a prospective single-center study. Vivo. 2022;36(6):2973–2980. doi:10.21873/invivo.13041
6. Dos Santos Barros V, Bassi-Dibai D, Guedes CLR, et al. Barthel index is a valid and reliable tool to measure the functional independence of cancer patients in palliative care. BMC Palliat Care. 2022;21(1):124. doi:10.1186/s12904-022-01017-z
7. Wylie C, White B. A measure of disability. Arch Environ Health. 1964;8:834–839. doi:10.1080/00039896.1964.10663764
8. Shah S, Muncer S. Sensitivity of Shah, Vanclay and Cooper’s modified Barthel index. Clin Rehabil. 2000;14(5):551–552. doi:10.1191/0269215500cr360oa
9. Shah S, Cooper B, Maas F. The Barthel index and ADL evaluation in stroke rehabilitation in Australia, Japan, the UK and the USA. Aust Occup Ther J. 1992;39(1):5–13. doi:10.1111/j.1440-1630.1992.tb01729.x
10. Vanclay F, Shah S. Validity of outcome following stroke rehabilitation. Arch Neurol. 1989;46(12):1270–1271. doi:10.1001/archneur.1989.00520480012007
11. Duffy L, Gajree S, Langhorne P, Stott D, Quinn T. Reliability (inter-rater agreement) of the Barthel Index for assessment of stroke survivors: systematic review and meta-analysis. Stroke. 2013;44(2):462–468. doi:10.1161/STROKEAHA.112.678615
12. Castiglia SF, Galeoto G, Lauta A, et al. The culturally adapted Italian version of the Barthel index (IcaBI): assessment of structural validity, inter-rater reliability and responsiveness to clinically relevant improvements in patients admitted to inpatient rehabilitation centers. Funct Neurol. 2017;22(4):221–228. doi:10.11138/FNeur/2017.32.4.221
13. Ohura T, Hase K, Nakajima Y, Nakayama T. Validity and reliability of a performance evaluation tool based on the modified Barthel index for stroke patients. BMC Med Res Methodol. 2017;17(1):131. doi:10.1186/s12874-017-0409-2
14. Richards S, Peters T, Coast J, Gunnell D, Darlow M, Pounsford J. Inter-rater reliability of the Barthel ADL index: how does a researcher compare to a nurse? Clin Rehabil. 2000;14(1):72–78. doi:10.1191/026921500667059345
15. Pietra G, Savio K, Oddone E, Reggiani M, Monaco F, Leone M. Validity and reliability of the Barthel index administered by telephone. Stroke. 2011;42(7):2077–2079. doi:10.1161/STROKEAHA.111.613521
16. Shinar D, Gross C, Bronstein K, et al. Reliability of the activities of daily living scale and its use in telephone interview. Arch Phys Med Rehabil. 1987;68(10):723–728.
17. D’Souza AN, Granger CL, Leggett NE, Tomkins MS, Kay JE, Said CM. Predicting discharge destination in older people from acute general medical wards: a systematic review of the psychometric properties of 23 assessment tools. J Geriatr Phys Ther. 2024;47(2):E109–23. doi:10.1519/JPT.0000000000000401
18. Collin C, Wade D, Davies S, Horne V. The Barthel ADL index: a reliability study. Int Disabil Stud. 1988;10(2):61–63. doi:10.3109/09638288809164103
19. Theofanidis D. Validation of international stroke scales for use by nurses in Greek settings. Topics in Stroke Rehabil. 2017;24(3):214–221. doi:10.1080/10749357.2016.1238136
20. Lekamwasam S, Karunatilake K, Lekamwasam V. Physical dependency of elderly and physically disabled; measurement concordance between 10-item Barthel index and 5-item shorter version. Ceylon Med J. 2011;56(3):114–118. doi:10.4038/cmj.v56i3.3603
21. Minosso J, Amendola F, Alvarenga M, Oliveira M. Validation of the Barthel Index in elderly patients attended in outpatient clinics, in Brazil. Acta Paul Enferm. 2010;23(2):218–223. doi:10.1590/S0103-21002010000200011
22. Leung S, Chan C, Shah S. Development of a Chinese version of the modified Barthel index—validity and reliability. Clin Rehabil. 2007;21(10):912–922. doi:10.1177/0269215507077286
23. Sainsbury A, Seebass G, Bansal A, Young J. Reliability of the Barthel index when used with older people. Age Ageing. 2005;34(3):228–232. doi:10.1093/ageing/afi063
24. Hsueh I, Lin J, Jeng J, Hsieh C. Comparison of the psychometric characteristics of the functional Independence measure, 5 item Barthel index, and 10 item Barthel index in patients with stroke. J Neurol Neurosurg Psychiatry. 2002;73(2):188–190. doi:10.1136/jnnp.73.2.188
25. García‐Fernández F, Arrabal‐Orpez M, Rodríguez‐Torres M, Gila‐Selas C, Carrascosa‐García I, Laguna‐Parras J. Effect of hospital case-manager nurses on the level of dependence, satisfaction and caregiver burden in patients with complex chronic disease. J Clin Nurs. 2014;23(19–20):2814–2821. doi:10.1111/jocn.12543
26. Ferfeli S, Galanos A, Dontas IA, Triantafyllou A, Triantafyllopoulos IK, Chronopoulos E. Reliability and validity of the Greek adaptation of the modified Barthel index in neurorehabilitation patients. Eur J Phys Rehabil Med. 2024;60(1):44–54. doi:10.23736/S1973-9087.23.08056-5
27. Theofanidis D, Gibbon G. Nursing interventions in stroke care delivery: an evidence-based clinical review. J Vascular Nurs. 2016;34(4):144–151. doi:10.1016/j.jvn.2016.07.001
28. Torre-García M, Hernández-Santana A, Moreno-Moreu N, Luis-Jacinto R, Maggiolo J, Rodríguez J. Use of the Barthel index to measure functional recovery in an elderly population after hip fracture. Revista Española de Cirugía Ortopédica y Traumatología. 2011;55(4):263–269. doi:10.1016/S1988-8856(11)70317-0
29. Yang Y, Tsaia L, Wu Y, Hsieh Y, Hsieh C, Howe T. The competence of fieldwork students in administering the Barthel index. Hong Kong J Occup Ther. 2008;28(1):28–33. doi:10.1016/S1569-1861(08)70010-X
30. Houlden H, Edwards M, Mcneil J, Greenwood R. Use of the Barthel index and the functional independence measure during early inpatient rehabilitation after single incident brain injury. Clin rehabilitat. 2006;20(2):153–159. doi:10.1191/0269215506cr917oa
31. Kwon S, Hartzema A, Duncan P, Min-Lai S. Disability measures in stroke: relationship among the Barthel Index, the Functional Independence Measure, and the Modified Rankin Scale. Stroke. 2004;35(4):918–923. doi:10.1161/01.STR.0000119385.56094.32
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.