Back to Journals » International Journal of Women's Health » Volume 18
The Association of Methylenetetrahydrofolate Reductase C677T Polymorphism, Serum 5-Methyltetrahydrofolate, and Homocysteine Levels with Adenomyosis: A Cross-Sectional Study in an Indonesian Population
Authors Hermawan M ![]() , Tjahyadi D, Rachmawati A, Permadi W, Syam HH
, Tjahyadi D, Rachmawati A, Permadi W, Syam HH ![]() , Suardika A, Anwar R
, Suardika A, Anwar R ![]()
Received 25 March 2026
Accepted for publication 1 July 2026
Published 9 July 2026 Volume 2026:18 612012
DOI https://doi.org/10.2147/IJWH.S612012
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marta Barba
Video abstract of “MTHFR C677T Polymorphism, 5-MTHF, and Homocysteine Levels with Adenomyosis” [612012].
Views: 18
Martin Hermawan,1 Dian Tjahyadi,1 Anita Rachmawati,1 Wiryawan Permadi,1 Hanom Husni Syam,1 Anom Suardika,2 Ruswana Anwar1
1Division of Reproductive Endocrinology and Infertility, Department of Obstetrics and Gynecology, Hasan Sadikin General Teaching Hospital, Faculty of Medicine, Padjadjaran University, Bandung, West Java, Indonesia; 2Division of Reproductive Endocrinology and Infertility, Department of Obstetrics and Gynecology, Prof. Dr. I.G.N.G. Ngoerah General Hospital / Faculty of Medicine, Udayana University, Denpasar, Bali, Indonesia
Correspondence: Martin Hermawan, Division of Reproductive Endocrinology and Infertility, Department of Obstetrics and Gynecology, Hasan Sadikin General Teaching Hospital, Faculty of Medicine, Padjadjaran University, Pasteur No. 38 Street, Pasteur, Bandung, West Java, 40161, Indonesia, Tel +628122015015, Email [email protected]
Purpose: Adenomyosis is a complex uterine condition, with emerging evidence indicating epigenetic alterations play a role in its pathogenesis. The methylenetetrahydrofolate reductase (MTHFR) gene polymorphism C677T may reduce enzyme activity, affecting DNA methylation and increasing adenomyosis risk. This study compares the MTHFR C677T polymorphism, 5-methyltetrahydrofolate (5-MTHF) levels, and homocysteine levels in patients with adenomyosis.
Patients and Methods: This cross-sectional study involved 61 subjects: 31 patients with adenomyosis and 30 patients as controls. The MTHFR C677T polymorphism was analyzed using PCR-RFLP, serum 5-MTHF and homocysteine levels were measured using ELISA. Statistical analyses were performed to compare genotype distributions and metabolite levels between groups and within the adenomyosis group based on genotype.
Results: The study found a significant difference in the distribution of the MTHFR C677T genotype between adenomyosis and control groups (p=0.018), with a higher prevalence of the CT genotype in the adenomyosis group (35.5% vs 10.0%). The frequency of the T allele was also elevated in the adenomyosis group (17.7% vs 5.0%; p=0.027). Serum 5-MTHF levels were notably lower in the adenomyosis group (23.92 ± 4.599 nmol/l) compared to controls (32.45 ± 3.019 nmol/l; p< 0.0001), while homocysteine levels were significantly higher in the adenomyosis group (12.87 ± 8.916 µmol/L vs 8.61 ± 1.352 µmol/L; p=0.019). Further analysis of MTHFR genotypes indicated lower 5-MTHF levels in both CC and CT genotypes among the adenomyosis group compared to controls (p< 0.0001). Homocysteine levels showed no significant difference across genotypes (p=0.074), though there was a trend towards higher levels in the adenomyosis group.
Conclusion: This study demonstrates a significant difference in the distribution of the MTHFR C677T polymorphism, lower 5-MTHF levels, and higher homocysteine levels in patients with adenomyosis compared to controls. Lower 5-MTHF levels were also shown to be strongly linked with the heterozygous C677T polymorphism in the adenomyosis group.
Keywords: DNA methylation, epigenetic, heterozygous, progesterone resistance
Introduction
Adenomyosis is a chronic, estrogen-dependent inflammatory condition characterised by the ectopic infiltration of endometrial tissue into the myometrium.1 The prevalence of adenomyosis exhibits substantial diversity across diverse populations, with notable discrepancies even within a single population. For example, among patients presenting clinical symptoms, the prevalence of adenomyosis ranges from 12% to 55%. The frequency of adenomyosis in infertile women varies from 4% to 89%.2 Although there were no definitive data on adenomyosis in Indonesia, a study conducted at Dr. Hasan Sadikin General Hospital in 2018 showed that the majority of adenomyosis patients (70.7%) were over 35 years of age and suffered from secondary infertility.3
The pathogenesis and pathophysiology of adenomyosis are not yet fully understood, and further research is therefore required to elucidate this condition. One of the mechanisms underlying the pathogenesis of adenomyosis involves epigenetic processes. Adenomyosis stromal cells exhibit a large number of epigenetic abnormalities.4 Recent research has increasingly focused on the role of epigenetic modifications in the pathogenesis of adenomyosis. Studies by Ebisch et al and Natadisastra showed that patients with endometriosis have higher homocysteine levels compared to the general population. The hyperhomocysteinemia found in endometriosis is associated with inflammatory processes, and there is an increase in homocysteine levels in follicular fluid.5 Furthermore, several studies have identified MTHFR polymorphisms as risk factors for the development of endometriosis. In 2022, Clement et al found that the prevalence of the homozygous C677T isoform was twice as high in the endometriosis group.6
Methylenetetrahydrofolate reductase (MTHFR) is an enzyme encoded by the MTHFR gene, which consists of 12 exons and is situated on chromosome 1p36.22. MTHFR is an enzyme dependent on flavin adenine dinucleotide (FAD) that is crucial for the metabolism of folate and homocysteine, both of which are derived from folic acid and other B vitamins. This enzyme facilitates the NADPH-dependent reduction of 5,10-methylenetetrahydrofolate to 5-methyltetrahydrofolate (5-MTHF). 5-MTHF, or levomefolic acid, is the principal physiologically active metabolite of consumed folic acid. This form is present in plasma at the highest concentration, constituting about 90% of the total folate content.7 It facilitates the conversion of homocysteine to methionine.8 Homocysteine is a non-protein amino acid found in the blood, containing sulphur in the form of a free thiol group (sulphhydryl -SH), and formed from methionine via S-adenosylmethionine (SAM).9
The C677T polymorphism (rs1801133) is the most extensively studied variant of the MTHFR gene. A point mutation at position 677 in the MTHFR gene, characterized by the substitution of cytosine (C) with thymine (T). The mutation in the MTHFR gene responsible for the C677T polymorphism is situated in exon 4. This mutation causes the replacement of alanine with valine at codon 222. It is expressed as the genotype (CC/CT/TT). An MTHFR polymorphism causes enzyme malfunction, possibly resulting in elevated homocysteine levels (as shown in Figure 1).7,10,11 Elevated levels of homocysteine have significant ramifications for human health and disease. Clinical studies demonstrate that hyperhomocysteinemia is an independent risk factor for cardiovascular diseases (CVDs) and can exacerbate glucose intolerance, insulin resistance, and hepatic steatosis, while being closely associated with an increased susceptibility to CVD, ischemic and pediatric hemorrhagic stroke, as well as recently identified links to adult-onset Alzheimer’s and other neurological disorders.12
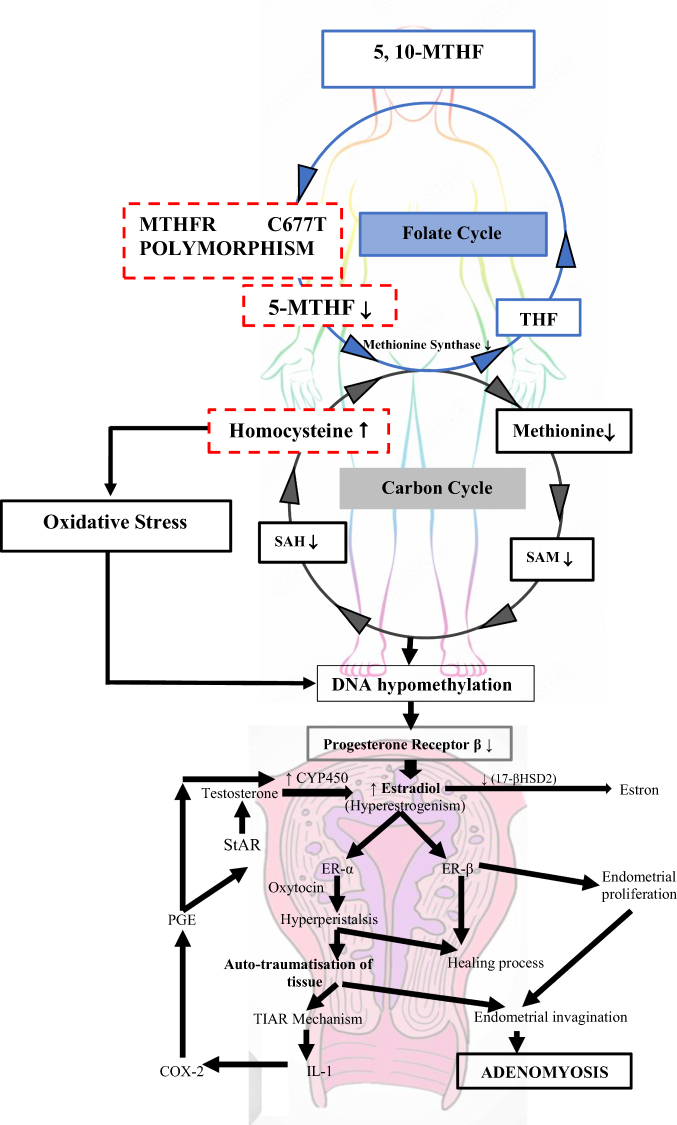 |
Figure 1 Illustration of the mechanism of action of the MTHFR C677T polymorphism. When the MTHFR C677T polymorphism occurs, it leads to a decrease in 5-MTHF production, which in turn causes a decrease in methionine synthase activity. Methionine synthase, which converts homocysteine into methionine, becomes less effective, resulting in reduced homocysteine conversion (and consequently increased homocysteine levels) and a decrease in methionine levels. The reduced levels of methionine lead to a decrease in SAM levels, followed by a corresponding decrease in SAH levels. Elevated homocysteine levels, which contribute to low SAM levels, result in DNA hypomethylation. DNA hypomethylation leads to reduced production of the β-progesterone receptor; consequently, the function of the β-progesterone receptor as an estrogen regulator is disrupted, resulting in hyperestrogenism. High estrogen levels in the body can trigger the development of adenomyosis via the TIAR mechanism, leading to endometrial invagination. Abbreviations: 5, 10-MTHF, 5,10-methylenetetrahydrofolate; MTHFR, methylenetetrahydrofolate reductase; THF, tetrahydrofolate; SAH, S-Adenosyl-L-homocysteine; SAM, S-adenosylmethionine; DNA, deoxyribonucleic acid; CYP450, Cytochrome P450; 17-βHSD2, 17β-hydroxysteroid dehydrogenase type 2; StAR, steroidogenic acute regulatory protein; PGE, prostaglandin E; ERα, estrogen receptors alpha; ERβ, estrogen receptors beta; TIAR, tissue injury and repair; COX-2, cyclooxygenase-2; IL-1, interleukin-1. Notes: The variables marked with a red dotted line were the variables tested in this study. |
The similarities observed in the epigenetic profiles of adenomyosis and endometriosis suggest that these two conditions may share the same underlying mechanisms.4 A number of previous studies have indeed explored the role of epigenetic modifications, particularly DNA methylation, in the pathogenesis of adenomyosis and endometriosis; similarly, several studies have linked the MTHFR C677T polymorphism with endometriosis. However, no study has comprehensively integrated these three aspects (MTHFR C677T polymorphism, 5-MTHF levels, and homocysteine) simultaneously in the context of adenomyosis, particularly with a direct comparison between adenomyosis patients and a control group. Therefore, this study aims to examine the comparison of the MTHFR C677T polymorphism, 5-MTHF levels and homocysteine levels in adenomyosis patients and controls.
Materials and Methods
Study Design and Settings
This was a cross-sectional analytic design conducted at Dr. Hasan Sadikin General Hospital and Bandung Kiwari Hospital (both from Bandung, West Java, Indonesia) from February to April 2025.
Study Population
The study population consisted of All female patients diagnosed with adenomyosis based on transvaginal ultrasound examinations and confirmed by post-operative histopathological findings who attended Dr Hasan Sadikin General Hospital and Bandung Kiwari Regional General Hospital between February and April 2025.
Inclusion and Exclusion Criteria
The inclusion criteria for the group of women with adenomyosis were: women aged 20–45 years, diagnosed with adenomyosis via transvaginal ultrasound using MUSA criteria and confirmed by post-operative anatomical pathology results at Dr. Hasan Sadikin General Hospital and Bandung Kiwari Regional General Hospital, and willing to participate in the study. On the other hand, the inclusion criteria for the control group are women aged 20–45 years, with good reproductive health, willing to participate in the study, and diagnosed as having a uterus without adenomyosis or malignancy via transvaginal ultrasound examination, confirmed by post-operative anatomical pathology results at Dr. Hasan Sadikin General Hospital and Bandung Kiwari Regional General Hospital.
Exclusion criteria for both groups were patients receiving 5-MTHF treatment, patients who had consumed excessive amounts of protein in the previous 8 hours (up to 15 grams), smokers, patients consuming alcohol, patients with the genetic disorder homocystinuria, pregnant patients, patients with cardiovascular, cerebrovascular and thromboembolic diseases, patients with malignancies, patients with severe infections/sepsis, patients with renal and liver disorders, patients with thyroid disorders, and patients undergoing methotrexate therapy.
Sample Size Estimation
In this study, the sample size was calculated using the Sample Size 2.0 programme by Hosmer and Lemeshow.13 Based on these calculations, the minimum sample size for each group was found to be 30, resulting in a minimum total sample size of 60.
Data Collection and Measurements
Baseline Characteristics
Participants completed questionnaires on sociodemographic factors, such as age (years), body weight (kg), body height (cm), body mass index (kg/m2), history of primary infertility, history of secondary infertility, history of excessive menstrual bleeding, the severity of menstrual pain (using the VAS), the coexistence of adenomyosis and endometriosis, and the phenotype of adenomyosis. BMI is a commonly used measure for assessing a person’s nutritional status; it is calculated as body weight in kilograms divided by the square of height in metres. BMI is categorised as follows: less than 18.5 kg/m2 (underweight), 18.5–24.9 kg/m2 (normal weight), 25.0–29.9 kg/m2 (overweight), and 30.0 kg/m2 or more (obese).14 The Visual Analogue Scale (VAS) is a commonly used tool for subjectively assessing pain intensity. The VAS scale typically ranges from 0 (no pain) to 10 (the worst pain imaginable).15
MUSA Criteria
Patients diagnosed with adenomyosis via transvaginal ultrasound using MUSA criteria: these include a globular uterine enlargement, asymmetric myometrial thickening, myometrial cysts, echogenic subendometrial lines and nodules, hyperechoic islands, fan-shaped shadows, irregular or interrupted transition zones, and translesional vascularisation on colour Doppler ultrasound, as well as direct and indirect features.16–18
The MTHFR C677T Polymorphism
Testing for the MTHFR C677T polymorphism begins with DNA isolation, which separates the DNA from other cellular components. Next, a polynucleotide electrophoresis procedure was carried out on an agarose gel. Subsequently, a PCR test for the MTHFR gene was carried out. This method was used to amplify the MTHFR gene. The PCR kit used was Kapa 2 G Fast. The denaturation, extension, final extension and hot start temperatures follow those specified in the Kapa 2 G Fast kit. In the final stage, a procedure was carried out for the restriction fragment length polymorphism (RFLP) digestion of the MTHFR gene with the aim of cutting the MTHFR gene at RS1801133 using the restriction enzyme Hinf I.
5-MTHF in Blood Plasma
The test was performed using a venous blood sample taken without fasting. The sample was collected into a tube containing EDTA as an anticoagulant. Once prepared, the sample was analysed using reagents in a stepwise dilution. The final result was then determined using the ELISA method.
Homocysteine in Blood Plasma
Homocysteine levels were obtained from plasma using EDTA or heparin as anticoagulants. The samples were centrifuged for 15 minutes at 1000 × g (or 3000 rpm) at a temperature of 2–8°C within 30 minutes of collection. The test was then performed immediately, and the samples were stored at −20°C or −80°C. The ELISA method was used to determine homocysteine levels.
Statistical Analysis
Statistical calculations were performed analytically using SPSS Software 26th Edition (IBM Corp. Released 2019. IBM SPSS Statistics for Window, Version 26.0. Armonk, NY: IBM Corp). The data obtained will be tested for normality using the Shapiro–Wilk test if the sample size was less than 50; alternatively, the Kolmogorov–Smirnov test will be used if the sample size was greater than 50. These tests were used to determine whether the data were normally distributed or not. Furthermore, the variables in this study used univariate analysis with T-test and Mann–Whitney test if the data were not normally distributed. The Chi-square test was then utilized in bivariate analysis. The significance of the test results was determined based on the p value <0.05.
Results
During the study period, a total of 61 subjects sought treatment at Dr. Hasan Sadikin General Hospital in Bandung and Bandung Kiwari Regional General Hospital between February and April 2025; they were divided into two groups: the adenomyosis group and the non-adenomyosis group, which served as the control group. The baseline characteristics of the subjects participating in this study were shown in Table 1. There were several characteristics that showed significant differences between the two groups, including a history of primary infertility (35.5% vs 3.3% in the adenomyosis group vs the control group, respectively; p=0.002), a history of secondary infertility (41.9% vs 10% in the adenomyosis group vs the control group, respectively; p=0.005), a history of excessive menstrual bleeding (58.1% vs 30% in the adenomyosis group vs the control group, respectively; p=0.027), and perceived severity of menstrual pain (7.06±1.914 vs 2.13±1.332 in the adenomyosis group vs the control group, respectively; p=0.0001). Table 2 presents the distribution of genotypes and alleles for the C677T polymorphism in the MTHFR gene within the study population (N=61). The results indicate that the CC genotype was the most common, found in 47 subjects (77.1%). The CT heterozygous genotype was found in 14 subjects (22.9%), whilst the TT homozygous genotype was not found at all in this study population (0.0%). Allele analysis showed that the C allele was the dominant allele with a frequency of 88.5% (108 out of 122 alleles), whilst the frequency of the T allele was 11.5% (14 out of 122 alleles).Table 3 presents the differences in the distribution of the MTHFR C677T genotype and the C and T alleles between the adenomyosis group and the control group. In the adenomyosis group, 20 cases (64.5%) were of the CC genotype, 11 cases (35.5%) were of the CT genotype, and no cases (0%) were of the TT genotype; whereas, based on allele distribution, 51 cases (82.3%) had the C allele and 11 cases (17.7%) had the T allele. In the control group, 27 cases (90%) were of the CC genotype, 3 cases (10%) were of the CT genotype, and no cases (0%) were of the TT genotype. Based on allele distribution, 57 cases (95%) were of the C allele and 3 cases (5%) were of the T allele. According to statistical tests, significant differences were found between the two groups in terms of genotype and allele distribution (p=0.018 and p=0.027, respectively).Table 4 presents a comparison of 5-MTHF levels between the adenomyosis group and the control group. In the adenomyosis group, the mean 5-MTHF level was 23.92±4.599 nmol/l, whereas in the control group, the mean 5-MTHF level was 32.45±3.019 nmol/l. Statistically, a significant difference was found between the two groups (p=0.0001).Table 5 presents a comparison of homocysteine levels between the adenomyosis group (n=31) and the control group (n=30). The mean homocysteine level in the adenomyosis group (12.87 ± 8.916 µmol/L) was significantly higher than that in the control group (8.61 ± 1.352 µmol/L) (p=0.019).Table 6 aims to compare homocysteine and 5-MTHF levels between patients with adenomyosis and the control group, with consideration of MTHFR genotype variations (CC and CT). Statistical analysis revealed significantly different results for 5-MTHF levels, but not for homocysteine levels, amongst the four groups studied.Table 7 presents a comparison of 5-MTHF levels in the adenomyosis group based on the MTHFR C677T genotypes CC and CT. 5-MTHF levels were grouped into two categories using the median value of 23.66 nmol/L from the total measured data: those with levels above the median and those below it. This approach was used to ensure that the population was divided fairly based on the midpoint of the 5-MTHF level distribution. In the CC genotype group (N=20), the majority of subjects had 5-MTHF levels ≥23.66 nmol/L (65.0%), whilst the remainder (35.0%) had levels <23.66 nmol/L. In the CT genotype group (N=11), the proportion of patients with 5-MTHF levels ≥23.66 nmol/L was significantly lower (27.3%) compared to the group with levels <23.66 nmol/L (72.7%). Statistical analysis revealed an odds ratio (OR) of 4.952 with a 95% confidence interval (CI) ranging from 0.986 to 24.875, and a p-value of 0.044. A p-value <0.05 indicates that the observed difference was statistically significant.
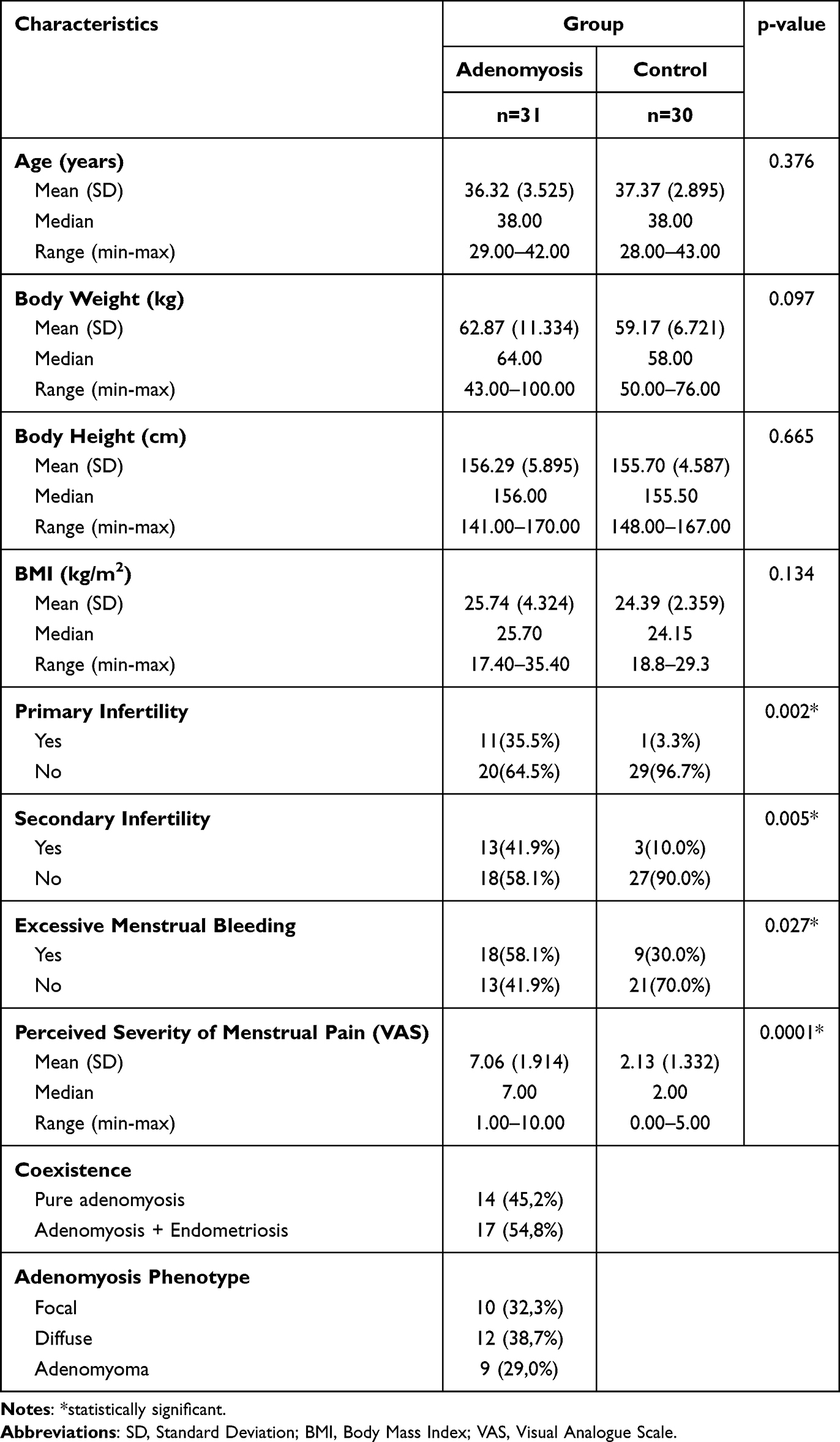 |
Table 1 Baseline Characteristics of Study Subject |
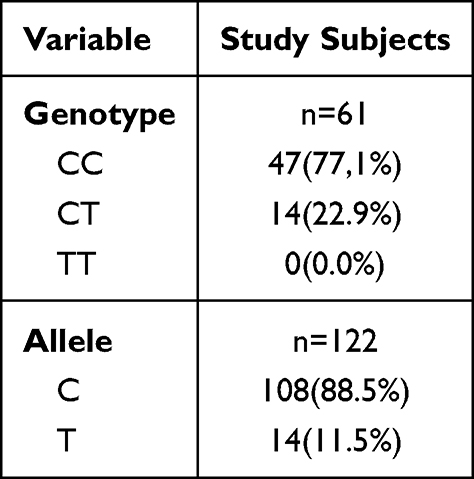 |
Table 2 Distribution of Genotypes and Alleles of the MTHFR C677T Polymorphism in Study Subjects |
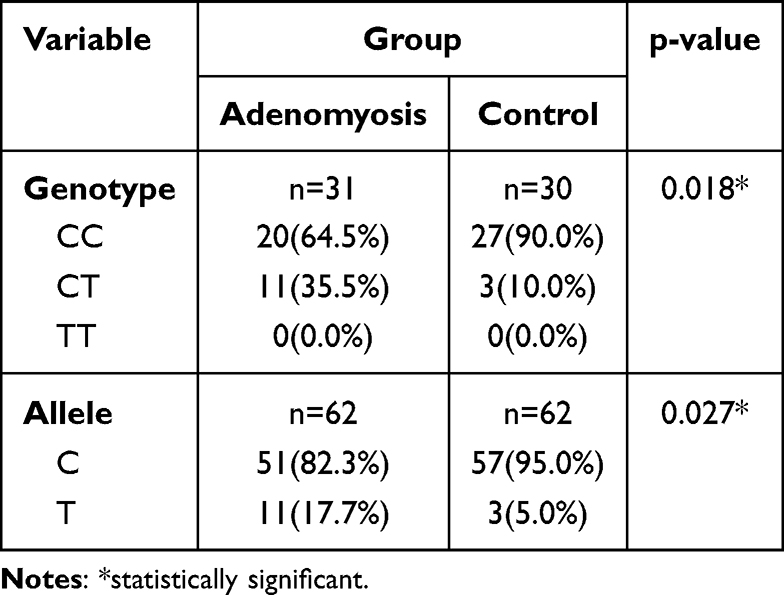 |
Table 3 Comparison of the C677T MTHFR Genotype Polymorphism in the Adenomyosis and the Control Group |
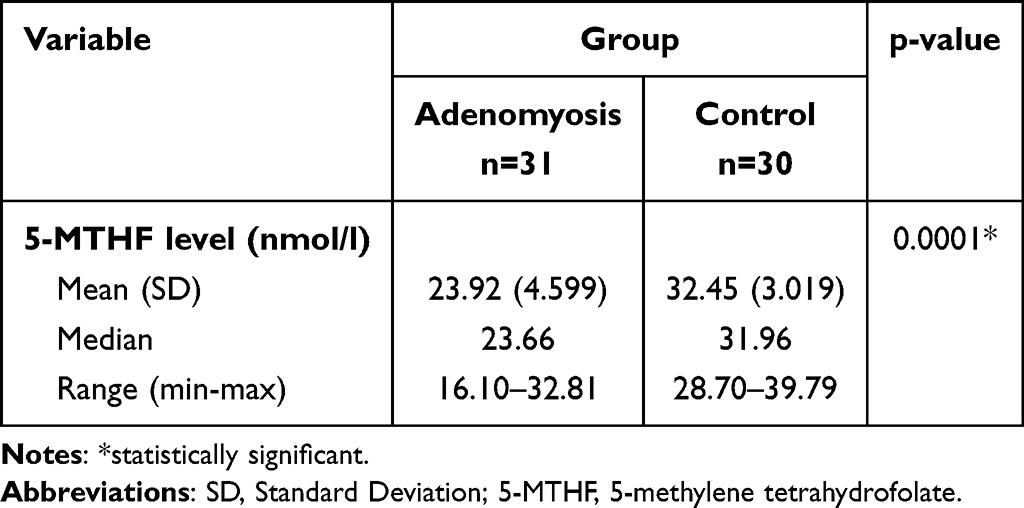 |
Table 4 Comparison of 5-MTHF Levels Between the Adenomyosis and the Control Group |
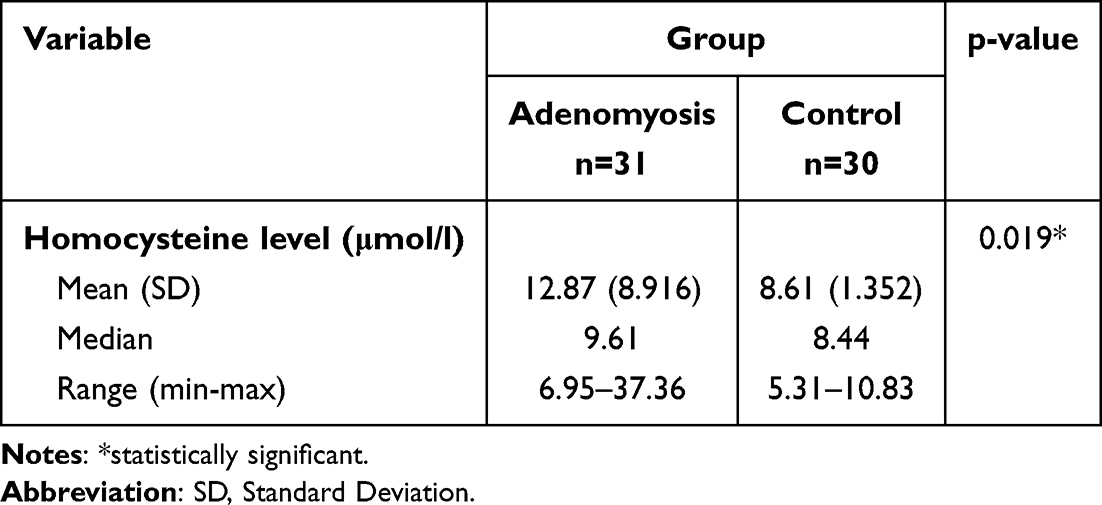 |
Table 5 Comparison of Homocysteine Levels Between the Adenomyosis and the Control Group |
 |
Table 6 Comparison of MTHFR C677T Polymorphism, 5-MTHF Levels and Homocysteine Levels in the Adenomyosis and the Control Group |
 |
Table 7 Correlation Between the MTHFR C677T Polymorphism Genotypes CC and CT and 5-MTHF Levels in a Group with Adenomyosis |
Discussion
In this study, there were no differences in the characteristics of the research subjects in both groups in terms of age and body mass index. The average age of the research participants in the adenomyosis group was 36.32 ± 3.525 years. This finding diverges slightly from other epidemiological research, which indicate that adenomyosis typically manifests in women of reproductive age, especially during their fourth and fifth decades.19,20 The disparity can be attributed to the increased utilization of non-invasive imaging techniques, such as transvaginal ultrasound and MRI, in diagnosing adenomyosis, facilitating the identification of additional cases among younger patients, especially those aged 30 to 40.21 These findings are further supported by a study conducted at Dr Hasan Sadikin General Hospital in 2018, which also showed that the majority of patients with adenomyosis (70.7%) were over 35 years of age.3
The mean BMI of 25.74 ± 4.324 kg/m2 in the adenomyosis group indicates that, on average, the subjects in this group fall into the overweight category. Whilst this study did not directly explore a causal relationship between BMI and adenomyosis, these findings are consistent with the literature review stating that adenomyosis is a condition influenced by hormones, particularly estrogen. Adipose tissue is known to be a site of extra-ovarian estrogen production, and excess adipose tissue, as seen in individuals who are overweight or obese, can lead to increased circulating estrogen levels. This increase in estrogen levels is thought to play a role in the development or worsening of adenomyosis.22–24
The adenomyosis group showed a proportion of subjects with primary infertility of 35.5% and secondary infertility of 41.9%. Several pathophysiological mechanisms have been proposed to explain the association between adenomyosis and primary infertility. Anatomical distortion of the uterus caused by endometrial invasion into the myometrium, leading to enlargement and changes in the shape of the uterine cavity, as well as uterotubal dysfunction that impairs the transport of sperm and ova. Furthermore, changes in the junctional zone caused by adenomyosis may affect uterine peristalsis, endometrial receptivity, and embryo implantation. Furthermore, adenomyotic tissue can produce inflammatory mediators, such as cytokines, which create an unfavourable uterine environment for embryo implantation and development. Finally, adenomyosis is associated with steroid hormone imbalances, progesterone resistance, and changes in the expression of molecular genes involved in the embryo implantation process.23,25–27 A higher proportion of secondary infertility (41.9%) is also a significant finding. Multiparity, a history of caesarean section, or previous abortion curettage are potential risk factors for the development of adenomyosis. This condition may be caused by physical and physiological trauma at the endometrial-myometrial interface, which contributes to the pathogenesis of adenomyosis.28
The high prevalence of excessive menstrual bleeding (58.1%) in the adenomyosis group in this study indicates that excessive menstrual bleeding is a clinically relevant issue in women with adenomyosis. This finding is consistent with the literature, which states that adenomyosis is a structural cause of abnormal uterine bleeding and excessive menstrual bleeding. The mechanisms underlying adenomyosis-induced excessive menstrual bleeding can be explained by several mechanisms, including an increase in endometrial surface area, impaired uterine contractility, dysregulation of prostaglandin production and signalling, disruption of hypoxia signalling or PGE2 signalling that inhibits endometrial repair, fibrosis and stiffness of adenomyosis lesions, and increased and dysregulated levels of inflammatory mediators and angiogenic factors.28,29
The results of the study showed that the adenomyosis group had an average score for the perceived severity of menstrual pain of 7.06 ± 1.914. The average VAS score of 7.06 indicates that the subjects in the adenomyosis group experienced significant menstrual pain. Dysmenorrhoea can be explained by the mechanism of myometrial hypercontractility, as evidenced by higher expression of oxytocin receptors and increased amplitude of uterine smooth muscle cell contractions in the adenomyosis uterus. Changes in the expression or activity of potassium channels in uterine smooth muscle cells may lead to inadequate membrane depolarisation, resulting in abnormal uterine activity.28,30
The results of this study showed that the proportion of isolated adenomyosis (45.2%) was slightly lower than that of cases involving the coexistence of adenomyosis and endometriosis (54.8%). These findings suggest that adenomyosis is often not isolated, but rather tends to occur alongside endometriosis. This is consistent with the 2019 study by Khan et al, which reported coexistence between external adenomyosis and endometriomas (40%), peritoneal endometriosis (60%), whilst the proportion of pure internal adenomyosis was 47.8% and only 10% for pure external adenomyosis.20 The findings from these studies consistently highlight the high incidence of adenomyosis accompanied by endometriosis, further reinforcing the potential for interrelated pathophysiological mechanisms between the two conditions.
The results of this study demonstrate a diverse distribution of adenomyosis phenotypes within the study population. The diffuse phenotype was the most commonly found (38.7%), followed by the focal phenotype (32.3%), whilst adenomyoma was the least frequently observed phenotype (29%). These findings suggest that adenomyosis exhibits a broad spectrum of anatomical manifestations within the myometrium. The predominance of the diffuse phenotype in this study suggests that a more widespread and uniform distribution of adenomyosis within the uterine wall may be the more common presentation in the studied population. Focal adenomyosis, by contrast, represents a localised adenomyotic lesion with more distinct borders and was less frequently observed in this study population. This is consistent with a study conducted by Byun et al in 1999, which found an incidence of 66.7% for diffuse adenomyosis and 33.3% for focal adenomyosis based on MRI findings.31
The distribution of MTHFR genotypes presented in Table 2 shows that the majority of study subjects have the normal/wild-type MTHFR genotype (CC), which is associated with normal or near-normal MTHFR enzyme activity. The presence of the CT genotype indicates a genetic variation that has the potential to reduce MTHFR enzyme activity compared to the CC genotype, although the impact is generally not as severe as in individuals with the TT genotype (which was not detected in this study). The observed frequency of the CT genotype (22.9%) and the T allele (11.5%) in this study population is consistent with findings in the Indonesian population, as reported in Soewarlan’s (2019) study, which showed frequencies of the CT genotype and T allele of 29% and 15%, respectively, in postmenopausal Indonesian women with osteoporosis. These results also show similarities with the T allele frequencies found in Indian (16.7%) and Chinese (19.7%) populations.32
The results in Table 3 show a significant difference in genotype distribution between the two groups. The significant difference in implies a potential association between this genetic variation and the development of adenomyosis. The dominance of the CC genotype in both groups suggests that the C allele may be the more common allele in the studied population. However, the lower percentage of the CC genotype in the adenomyosis group compared to the control group suggests that the T allele or genotypes containing the T allele (CT) may play a role in susceptibility to adenomyosis. Although the TT genotype was not detected in this study, the presence of the T allele in the CT genotype in both the adenomyosis group (35.5%) and the control group (10%) indicates that this allele is present in the population. The higher frequency of the T allele in the adenomyosis group (17.7%) compared to the control group (5%) may indicate that the T allele is a genetic risk factor for adenomyosis. The absence of the TT genotype in this study population can be explained by the variability in the prevalence of the MTHFR C677T polymorphism, which is known to depend on ethnicity and geographical location, as demonstrated by previous studies. In Indonesia, a study conducted by Soewarlan et al in 2019 reported a frequency of the heterozygous (CT) genotype of 29%, the homozygous (TT) genotype of 1%, and the normal homozygous (CC) genotype of 70%, with an allele distribution of 84.5% for the C allele and 15.5% for the T allele.32 The frequency of the TT homozygous genotype was recorded as highest in Mexico (32%), southern Italy (26%), and northern China (20%).33
The results of this study, shown in Table 4, reveal a statistically significant difference in 5-MTHF levels between the adenomyosis group and the control group. These findings suggest that 5-MTHF levels may play a role in the pathogenesis of adenomyosis. Low 5-MTHF levels in the adenomyosis group may contribute to the development and progression of the disease through several potential mechanisms, particularly disturbances in DNA methylation. 5-MTHF plays a crucial role in methylation as it functions as a methyl donor to convert homocysteine into methionine, and serves as a precursor to SAM, with methionine synthase acting as the enzyme catalysing this conversion.7,11,34 Disruptions in DNA methylation can lead to epigenetic changes that modulate gene expression. Genomic integrity is maintained by DNMTs, which utilise SAM as a cofactor or methyl group donor.34
The results of the statistical analysis in Table 5 show that the mean homocysteine level in the adenomyosis group (12.87 ± 8.916 µmol/L) was significantly higher than that in the control group (8.61 ± 1.352 µmol/L). These findings indicate the presence of hyperhomocysteinemia in the group of women with adenomyosis. These results are consistent with the 2016 study by Natadisastra et al, which found higher homocysteine levels in women with endometriosis compared to the control group (8.34 ± 2.68 µmol/L vs 6.71 ± 1.56 µmol/L, p=0.007; 95% CI: 0.02417–0.14657).5 Hyperhomocysteinemia has been associated with various health conditions, including cardiovascular disease and reproductive disorders such as adenomyosis and endometriosis.35 Homocysteine promotes endothelial damage, inflammation, and oxidative stress in various in vitro and in vivo models. In vitro studies have shown that homocysteine damages endothelial cells by increasing H2O2 production, affecting the antioxidant defence system, and promoting lipid peroxidation, as well as triggering apoptosis via the production of mitochondrial oxidants.36 Methylation abnormalities resulting from homocysteine cycle dysfunction can lead to epigenetic changes affecting abnormal mRNA and protein expression in genes such as aromatase, and oestrogen and progesterone receptors in stromal cells, all of which are relevant to the pathogenesis of adenomyosis.4,23,24,26,28
One important finding in Table 6 is the statistically significant difference (p=0.0001) in mean 5-MTHF levels among the groups. The diminished 5-MTHF levels in these adenomyosis patients signify a disturbance in folate metabolism attributable to MTHFR polymorphisms. In the adenomyosis group, those with the CT genotype demonstrated the lowest average 5-MTHF levels (22.28±4.039 nmol/l) in contrast to those with the CC genotype (24.82±4.733 nmol/l). This pattern aligns with the research indicating that the CT genotype of the MTHFR C677T polymorphism is frequently linked to diminished MTHFR enzyme activity. The decrease in enzyme activity leads to a diminished conversion of 5,10-methylenetetrahydrofolate to 5-MTHF, resulting in reduced circulating levels of 5-MTHF. A same trend was noted in the control group, albeit with a lesser disparity, where the CT genotype (31.12±2.801 nmol/l) exhibited a little lower mean 5-MTHF level than the CC genotype (32.60±3.055 nmol/l).34,37
In contrast to 5-MTHF levels, the statistical analysis did not found a statistically significant difference in mean homocysteine levels between the four groups (p=0.074). Further examination of the mean values revealed a trend towards higher homocysteine levels in the adenomyosis group (CC: 12.69±9.001 µmol/L; CT: 13.18±9.186 µmol/L) compared with the control groups (CC: 8.68±1.399 µmol/L; CT: 7.91±0.485 µmol/L). The relatively large standard deviation in homocysteine levels, particularly in the adenomyosis group, indicates high inter-individual variability within that group. This variability may mask any actual differences or suggest that factors other than the MTHFR genotype under investigation also exert a strong influence on homocysteine levels in patients with adenomyosis. The insignificance of the difference in homocysteine levels, despite a significant reduction in 5-MTHF in the adenomyosis group, may be attributed to several factors. The reduction in 5-MTHF may not have been drastic enough to cause a statistically significant accumulation of homocysteine in this sample size. Furthermore, the homocysteine metabolic pathway is also influenced by other factors such as vitamin B6 and B12 intake, which were not evaluated in this study. Another factor that may be quite influential is the absence of the homozygous MTHFR C677T polymorphism in this study population; it is known that the presence of this polymorphism can reduce enzyme activity by up to 60–70%.38
The comparison of 5-MTHF levels between the MTHFR C677T CC and CT genotypes in the adenomyosis group is presented in Table 7. An odds ratio (OR) of 4.952 indicates that adenomyosis patients with the CT genotype are nearly five times more likely to have 5-MTHF levels < 23.66 nmol/L compared with adenomyosis patients with the CC genotype. The 95% confidence interval (0.986–24.875) supports this finding, although the lower limit of the interval is close to 1, suggesting that the effect may vary, yet still tends to support an increased odds ratio in the CT group. Statistical significance (p=0.044) indicates that the difference in the proportion of 5-MTHF levels between the CC and CT genotype groups is not a coincidence.
This study has several limitations. Firstly, the absence of the homozygous (TT genotype) MTHFR C667T polymorphism in the study population was a major limitation preventing a more in-depth analysis of the effect of this genotype on 5-MTHF and homocysteine levels in women with adenomyosis. Furthermore, the use of a cross-sectional design, chosen due to funding constraints, did not allow for the determination of the direction of the causal relationship or the assessment of the strength of the correlation between variables. Finally, the heterogeneity of the adenomyosis group constituted another significant limitation. Ideally, this group should have comprised only subjects with pure adenomyosis; however, the limited number of cases of pure adenomyosis meant that some subjects also had endometriosis. This heterogeneity has the potential to influence the interpretation of the results, as endometriosis may have its own effects on the variables under investigation.
In terms of the limitations of this study, further research should involve populations from various ethnic groups and geographical regions known to have a significant frequency of the homozygous MTHFR C677T polymorphism, with the aim of further investigating the relationship between this polymorphism and 5-MTHF levels in cases of adenomyosis. Furthermore, future studies could employ a comparative design to compare groups with pure adenomyosis against those with coexisting adenomyosis and endometriosis (would yield more homogeneous subgroups); a longitudinal design, such as a prospective cohort study, to address the limitations of cross-sectional designs (prospective cohort designs allow for the assessment of temporal sequences and the identification of risk factors associated with the MTHFR C677T polymorphism and 5-MTHF levels in relation to factors involved in the pathogenesis of adenomyosis and the progression of adenomyosis symptoms, whilst measuring the strength of the correlation between these variables), or; preclinical studies may be employed to assess the modulatory effects of 5-MTHF levels on the progression of adenomyosis in animal models.
Conclusion
This study demonstrates a significant difference in the distribution of the MTHFR C677T polymorphism, lower 5-MTHF levels, and higher homocysteine levels in patients with adenomyosis compared to controls. Lower 5-MTHF levels were also significantly associated with the heterozygous C677T polymorphism in the adenomyosis group.
Ethics Approval and Consent to Participate
This study complies with the Declaration of Helsinki and was approved by the Ethics Committee of Dr. Hasan Sadikin General Hospital, Bandung with number of DP.04.03/D.XIV.6.5/51/2025. Informed consent was obtained from all individual participants included in the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This publication charge is funded by Unpad through the Indonesian Endowment Fund for Education (LPDP) on behalf of the Indonesian Ministry of Higher Education, Science and Technology and managed under the EQUITY Programme (Contract No. 4303/B3/DT.03.08/2025 and 3927/UN6.RKT/HK.07.00/2025).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Santulli P, Vannuccini S, Bourdon M, Chapron C, Petraglia F. Adenomyosis: the missed disease. Reprod Biomed Online. 2025;50(4):104837. doi:10.1016/j.rbmo.2025.104837
2. Wang MH, Chen JH, Qi XY, Li ZX, Huang Y. Global prevalence of adenomyosis and endometriosis: a systematic review and meta-analysis. Reprod Biol Endocrinol. 2025;23(1):148. doi:10.1186/s12958-025-01483-z
3. Fitrina M, Bayuaji H, Husnitawati Madjid T, Armawan E. Karakteristik pasien adenomiosis dengan gambaran ultrasonografi di rumah sakit Dr. Hasan sadikin bandung periode 2015-2016. Obgynia. 2018;1:35. doi:10.24198/obgynia.v1i1.16
4. Bulun SE, Yildiz S, Adli M, et al. Endometriosis and adenomyosis: shared pathophysiology. Fertil Steril. 2023;119(5):746–14. doi:10.1016/j.fertnstert.2023.03.006
5. Abdulmuthalib A, Natadisastra M, Jacoeb TZ. Homocysteine level in the blood and follicular fluid is higher in infertile women with endometriosis kadar homosistein darah dan zalir folikel pada perempuan infertil dengan endometriosis lebih tinggi. Indonesian J. Obstet. Gynecol. 2021;37:92–98.
6. Clement P, Alvarez S, Jacquesson-Fournols L, et al. T677T methylenetetrahydrofolate reductase single nucleotide polymorphisms increased prevalence in a subgroup of infertile patients with endometriosis. J Womens Health. 2022;31:1501–1506. doi:10.1089/jwh.2022.0019
7. Zarembska E, Ślusarczyk K, Wrzosek M. The Implication of a Polymorphism in the Methylenetetrahydrofolate Reductase Gene in Homocysteine Metabolism and Related Civilisation Diseases. Int J Mol Sci. 2024;25(1). doi:10.3390/ijms25010193
8. Clément A, Menezo Y, Cohen M, Cornet D, Clément P. 5-Methyltetrahydrofolate reduces blood homocysteine level significantly in C677T methyltetrahydrofolate reductase single-nucleotide polymorphism carriers consulting for infertility. J Gynecol Obstet Hum Reprod. 2020;49(1):101622. doi:10.1016/j.jogoh.2019.08.005
9. McCaddon A, Miller JW. Homocysteine—a retrospective and prospective appraisal. Front Nutr. 2023. doi:10.3389/fnut.2023.1179807
10. Wrzosek M, Ślusarczyk K. Methylenetetrahydrofolate Reductase C677T Gene Variant in Relation to Body Mass Index and Folate Concentration in a Polish Population. Biomedicines. 2022;10(12):3140. doi:10.3390/biomedicines10123140
11. Liew SC, Das GE. Methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism: epidemiology, metabolism and the associated diseases. Eur J Med Genet. 2015;58(1):1–10. doi:10.1016/j.ejmg.2014.10.004
12. Agostini D, Bartolacci A, Rotondo R, et al. Homocysteine, nutrition, and gut microbiota: a comprehensive review of current evidence and insights. Nutrients. 2025;17(8):1325. doi:10.3390/nu17081325
13. Lwanga S, Lemeshow S. Sample size determination in health studies: a practical manual. XF2006303260. 1991. doi:10.2307/2290547
14. Centers for Disease Control and Prevention. Centers for Disease Control and Prevention. [Internet]. 2024. Adult BMI Categories. Available from: https://www.cdc.gov/bmi/adult-calculator/bmi-categories.html.
15. Koo M, Yang SW. Visual Analogue Scale. Encyclopedia. 2025;5(4):190. doi:10.3390/encyclopedia5040190
16. Moawad G, Fruscalzo A, Youssef Y, et al. Adenomyosis: an updated review on diagnosis and classification. J Clin Med. 2023;12(14):4828. doi:10.3390/jcm12144828
17. den Bosch T V, Dueholm M, Leone FPG, et al. Terms, definitions and measurements to describe sonographic features of myometrium and uterine masses: a consensus opinion from the Morphological Uterus Sonographic Assessment (MUSA) group. Ultrasound Obstet Gynecol. 2015;46(3):284–298. doi:10.1002/uog.14806
18. Harmsen MJ, Van den Bosch T, de Leeuw RA, et al. Consensus on revised definitions of Morphological Uterus Sonographic Assessment (MUSA) features of adenomyosis: results of modified Delphi procedure. Ultrasound Obstet Gynecol. 2022;60(1):118–131. doi:10.1002/uog.24786
19. KM USA, Missmer SA. Epidemiology of Adenomyosis. Semin Reprod Med. 2020;38(02/03):89–107. doi:10.1055/s-0040-1718920
20. Khan K, Fujishita A, Koshiba A, et al. Biological differences between intrinsic and extrinsic adenomyosis with coexisting deep infiltrating endometriosis. Reprod Biomed Online. 2019;39:343–353. doi:10.1016/j.rbmo.2019.03.210
21. Bourdon M, Oliveira J, Marcellin L, et al. Adenomyosis of the inner and outer myometrium are associated with different clinical profiles. Hum Reprod. 2020;36. doi:10.1093/humrep/deaa307
22. d’Otreppe J, Patiño-García D, Piekos P, et al. Exploring the Endocrine Mechanisms in Adenomyosis: from Pathogenesis to Therapies. Endocrines. 2024;5:46–71. doi:10.3390/endocrines5010004
23. Khan KN, Fujishita A, Mori T. Pathogenesis of human adenomyosis: current understanding and its association with infertility. J Clin Med. 2022;11(14):4057. doi:10.3390/jcm11144057
24. Rossi M, Vannuccini S, Capezzuoli T, et al. Mechanisms and Pathogenesis of Adenomyosis. Curr Obstet Gynecol Rep. 2022;11(2):95–102. doi:10.1007/s13669-022-00326-7
25. Kim H, Frisch EH, Falcone T. From diagnosis to fertility: optimizing treatment of adenomyosis for reproductive health. J Clin Med. 2024;13(16). doi:10.3390/jcm13164926
26. Pados G, Gordts S, Sorrentino F, Nisolle M, Nappi L, Daniilidis A. Adenomyosis and infertility: a literature review. Medicina. 2023;59:1551. doi:10.3390/medicina59091551
27. Abu Hashim H, Elaraby S, Fouda AA, El RM. The prevalence of adenomyosis in an infertile population: a cross-sectional study. Reprod Biomed Online. 2020;40(6):842–850. doi:10.1016/j.rbmo.2020.02.011
28. Silvia Z, Felice P, JV GLC, Giudice LC. Adenomyosis: mechanisms and Pathogenesis. Semin Reprod Med. 2020;38(02/03):129–143. doi:10.1055/s-0040-1716687
29. Guo SW. Cracking the enigma of adenomyosis: an update on its pathogenesis and pathophysiology. Reproduction. 2022;164:R101–R121. doi:10.1530/REP-22-0224
30. Vannuccini S, Tosti C, Carmona F, et al. Pathogenesis of adenomyosis: an update on molecular mechanisms. Reprod Biomed Online. 2017;35(5):592–601. doi:10.1016/j.rbmo.2017.06.016
31. Byun JY, Kim SE, Choi BG, Ko GY, Jung SE, Choi KH. Diffuse and focal adenomyosis: mr imaging findings. RadioGraphics. 1999;19(suppl_1):S161–70. doi:10.1148/radiographics.19.suppl_1.g99oc03s161
32. Soewarlan W, Joenoes H, Bawazier S, Suryandari D, Auerkari E. Distribution of methylenetetrahydrofolate reductase (MTHFR) C677T polymorphism in postmenopausal Indonesian women with osteoporosis – a preliminary study.
33. Wilcken B, Bamforth F, Li Z, et al. Geographical and ethnic variation of the 677C>T allele of 5, 10 methylenetetrahydrofolate reductase (MTHFR): findings from over 7000 newborns from 16 areas world wide. J Med Genet. 2003;40:619–625. doi:10.1136/jmg.40.8.619
34. Ledowsky C, Schloss J, Steel A. Variations in folate prescriptions for patients with the MTHFR genetic polymorphisms: a case series study. Explor. Res. Clin. Soc. Pharm. 10;100277. doi:10.1016/j.rcsop.2023.100277
35. Onwumere K, Musa BOP, Kolawole A, Ameh N, Danga C, El-Fulaty A. Serum homocystein and C-reactive protein in predicting outcome of in-vitro fertilization in infertile women with polycystic ovary syndrome. Afr. J. Infertil. Assist. Concept. 2022. doi:10.4103/ajiac.ajiac_1_22
36. Hoffman M. Hypothesis: hyperhomocysteinemia is an indicator of oxidant stress. Med Hypotheses. 2011;77:1088–1093. doi:10.1016/j.mehy.2011.09.009
37. Tabatabaei RS, Fatahi Meybodi N, Meibodi B, et al. Association of Fetal MTHFR C677T polymorphism with susceptibility to neural tube defects: a systematic review and update meta-analysis. Fetal Pediatr Pathol. 2020;41:1–17. doi:10.1080/15513815.2020.1775734
38. Delli Carpini G, Giannella L, Di Giuseppe J, et al. Homozygous C677T Methylenetetrahydrofolate Reductase (MTHFR) Polymorphism as a risk factor for endometriosis: a retrospective case–control study. Int J Mol Sci. 2023;24(20):15404. doi:10.3390/ijms242015404
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.