")
Back to Journals » Clinical Ophthalmology » Volume 17
The Association of Cardiovascular and Neurological Comorbidities in Geriatric Patients Sustaining Ocular Trauma
Authors Pham VQ, Miller HM, Fernandez EO , de Marchi D, Zhu H, Fleischman D
Received 12 September 2023
Accepted for publication 2 November 2023
Published 14 November 2023 Volume 2023:17 Pages 3409—3417
DOI https://doi.org/10.2147/OPTH.S434804
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Vincent Q Pham,1 Hannah M Miller,2 Elise O Fernandez,3 Daniel de Marchi,4 Hongtu Zhu,4 David Fleischman2
1Northeast Ohio Medical University, Rootstown, OH, USA; 2Department of Ophthalmology, University of North Carolina, Chapel Hill, NC, USA; 3School of Medicine, University of North Carolina, Chapel Hill, NC, USA; 4Department of Biostatistics, University of North Carolina at Chapel Hill, Chapel Hill, NC, USA
Correspondence: David Fleischman, Department of Ophthalmology, University of North Carolina, 5126 Bioinformatics Bldg #7040, Chapel Hill, NC, 27599-7040, USA, Tel +1 919 966-5296, Fax +1 919 966-1908, Email [email protected]
Purpose: Falls are associated with ocular trauma in the elderly. However, it is unlikely for a fall to cause ocular injury unless there is a disruption in the protective maneuvers that shield the face. We suspect ocular injury may be an early indicator of systemic or neurologic degeneration. This study investigates the 5-year incidence of cardiovascular and neurodegenerative diseases in older patients who sustained ocular or periorbital injuries.
Patients and Methods: This was a retrospective cohort study. The study population included 141 patients over the age of 65 who sustained trauma to the eye, orbit, or eyelid between April 2011 and June 2016. The control population included 141 patients with a similar range of comorbidities who received cataract surgery during the same period. The study measured new diagnoses of various disorders during the 5-year period following presentation.
Results: There were a total of 180 females and 102 males in the study. The mean ages of the control and subject group were 76 and 81.8, respectively. Of our twelve tested comorbidity types, patients that suffered a periocular trauma were more likely to develop heart failure (p=0.00244), dementia (p=0.00002), Alzheimer’s disease (p=0.00087), and vascular disease (p=0.00037).
Conclusion: Geriatric patients who sustained ocular and periocular injuries had a greater incidence of heart failure, dementia, Alzheimer’s disease, and atherosclerosis diagnoses in the 5-year period following injury. The findings of this study suggest that periocular trauma may be an early indicator of underlying degenerative or systemic disease. Ophthalmologists should ensure proper primary care follow-up in conjunction with recovery from injury.
Keywords: ocular injury, comorbidities, eye injury, degenerative disease
Introduction
Falls are a major cause of ocular and periocular injury in elderly individuals.1–4 Fall-related eye injuries are associated with increased morbidity and worse outcomes when compared with non-fall-related eye injuries.2 Ocular injury due to a fall is more likely to result in worse final visual acuity5 and blindness.6 Additionally, eye injuries due to a fall, compared to non-fall-related injury, are associated with increased risk of hospitalization and more severe ocular injuries, such as open globe injury, ruptured globe, retinal detachment, and larger wound size.7,8 Data from the National Electronic Injury Surveillance System, a national database of emergency department-treated injuries in the US, revealed that eye injuries that presented to the hospital often included older patients or those whom were coming from a nursing home.7 A 10-year review from a state trauma service showed that falls in the elderly were associated with serious ocular injuries; the presence of ocular injury was further tied to poor functional outcomes.9 This study, looking at fall-related ocular trauma in the elderly, found that the in-hospital mortality rate was similar to the in-hospital mortality rate associated with hip fracture in the elderly.9
Common ocular injuries in the elderly include contusion of the eye/adnexa, open wound of the ocular adnexa, foreign body, eyelid wounds, orbital wall fractures, and open globe injuries. Other less common but severe ocular injuries include retrobulbar hematoma, retinal detachment, and traumatic optic neuropathy.9 Risk factors for fall-related eye injury include older age, female sex, black race, and presentation from a nursing home.7 Orbital fractures are the most common type of fall-related injury requiring ophthalmology consultation.9 Apart from falls, a common cause of orbital fractures is motor vehicle accidents.10 Patients with penetrating ocular trauma, visual acuity deficits, and a fracture depth involving the posterior orbit are at high risk for vision loss.11
It is well known that falls in the elderly can be a signal of declining health and function. They are often associated with the existence and development of significant comorbidities. Some risk factors for falls in the elderly include chronic medical conditions, polypharmacy, cognitive impairment, reduced vision, and neurologic decline.12 Following a fall, older individuals are more likely to have subsequent hospitalizations/nursing home admissions and are more likely to experience difficulties with activities of daily living.13
Several chronic medical conditions have been found to be associated with falls in the elderly, including musculoskeletal disease, diabetes, cardiovascular and cerebrovascular disease, and cognitive impairment.14 Furthermore, the risk of falls increases as the number of chronic conditions an individual has increases.15 According to the most recent estimate by the CDC, 85% of individuals age 65 and older have at least one chronic medical condition and 56% have two or more.16 The rising age of the US population and the prevalence of multimorbidity place many individuals at risk of falls and potential ocular injury. Further understanding of the relationship between chronic medical conditions and traumatic eye injuries is warranted, especially given that reduced vision can further increase the risk of falls.
This study focuses on comorbidities associated with traumatic eye injuries compared to non-traumatic cataract surgery patients. Older patients sustain falls more frequently and typically have a greater set of comorbidities, such as metabolic disease, sensory deficits, malignancy, or neurological disease.17 One of the ways to attempt to protect the face from potential injury is typically with an outstretched hand or arm. While these may result in other injuries, such as wrist fractures, they may be sufficient to prevent head or facial injury. For a patient to sustain a periocular injury from a fall, there may be a breakdown in the instinctual response to break the fall effectively before injuring the face. This may be just one of the myriad factors that influence falls and ocular trauma among the elderly. We hypothesized that patients who suffered ocular trauma may be more likely to have cardiovascular and neurological comorbidities. We suspect that impaired protective instincts during falls may be a harbinger of incipient systemic or neurologic conditions.
Materials and Methods
This is a retrospective cohort study utilizing data from the I2B2 Carolina Data Warehouse for Health, specifically data on geriatric patients presenting to the hospital with ocular trauma. Queries were submitted using the I2B2 database to receive patient information. The study group included patients who had injury to the eye and orbit, open wound of the eyelid and periocular area, orbital floor fracture, fracture of facial bones, injury of conjunctiva, contusion of eyeball, contusion of orbital tissues, open wound of the eyeball, ocular ulceration, penetrating wound of the orbit with foreign body, avulsion of the eye, or laceration of the eyelid and periocular area. The exclusion criteria excluded patients who suffered motor vehicle and transport accidents, were victims of homicide, assault, or purposeful injury, or died within 1 month of presentation of the ocular trauma. The study group consisted of patients presenting to University of North Carolina (UNC) hospitals between April 2011 and June 2016. The control group included patients who presented for cataract surgery between April 2014 and June 2016 in one or both eyes. Using python coding through the Jupyter Notebook platform, data was extracted and filtered for 699 patients in the initial ocular trauma study group and 1066 patients in the initial cataract surgery control group. Within the study group 97 patients were excluded, including 88 patients that suffered motor vehicle and transport accidents and 9 victims of homicide, assault, or purposeful injury, resulting in a study group of 602 patients. Within the initial control group, 31 patients were excluded, including 29 patients that suffered motor vehicle and transport accidents, 2 victims of homicide, assault, or purposeful injury, and 2 patients that died within 1 month of presentation, resulting in a control group of 1066 patients (see Figure 1). This included patients with a diverse array of medical conditions and comorbidities ranging across all systems, including pulmonary, cardiovascular, renal, etc. From here, patients were restricted to those who had follow-up within five years and had cardiovascular or neurological comorbidities, providing a treatment group of 141 patients. Each treatment patient was matched with the most similar control patient by a nearest-neighbor algorithm that found the control patient with the most similar counts of initial comorbidities across twelve subcategories of cardiovascular and neurological disorders at baseline. These categories were cardiac arrhythmias, type 2 diabetes, ischemic heart diseases, heart failure, dementia, degenerative diseases of the nervous system, polyneuropathies and other disorders of the peripheral nervous system, encephalopathy, Alzheimer’s disease, Parkinson’s disease, vascular disease, and hypertensive heart diseases (see Table 1). For the diagnoses, information was gathered using I2B2 guidelines. If the patient presented before 2015, the ICD-9 format that had a numerical list of codes and index of diagnoses, surgeries, and procedures was used. If a patient presented after 2015, the ICD-10 format that utilized different codes and slightly different groups to code diagnoses was used. Patient demographics including age, sex, race, and insurance status in the final study group and final control group were examined.
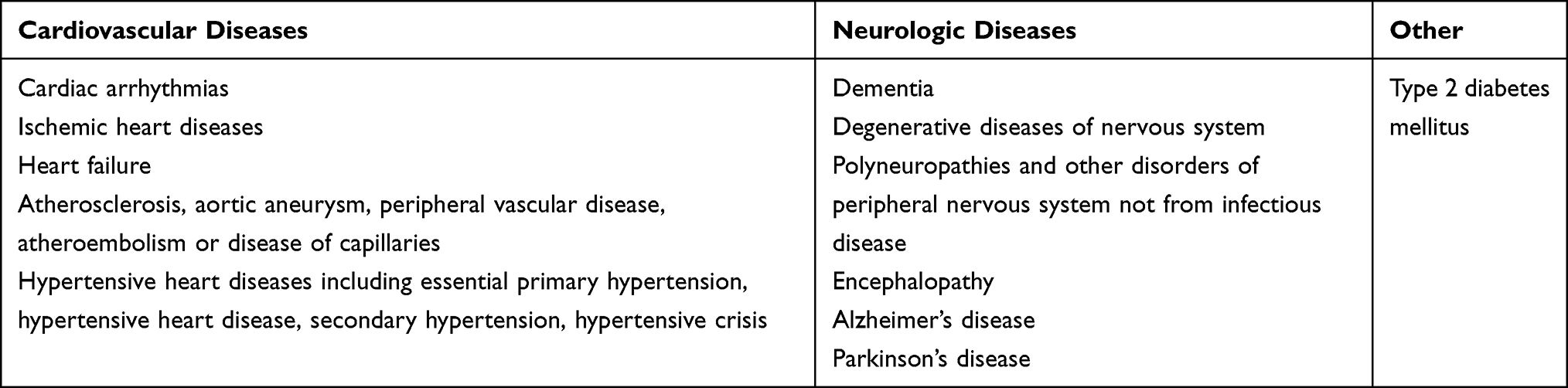 |
Table 1 List of Cardiovascular and Neurological Morbidities Evaluated for in Patient Subset B |
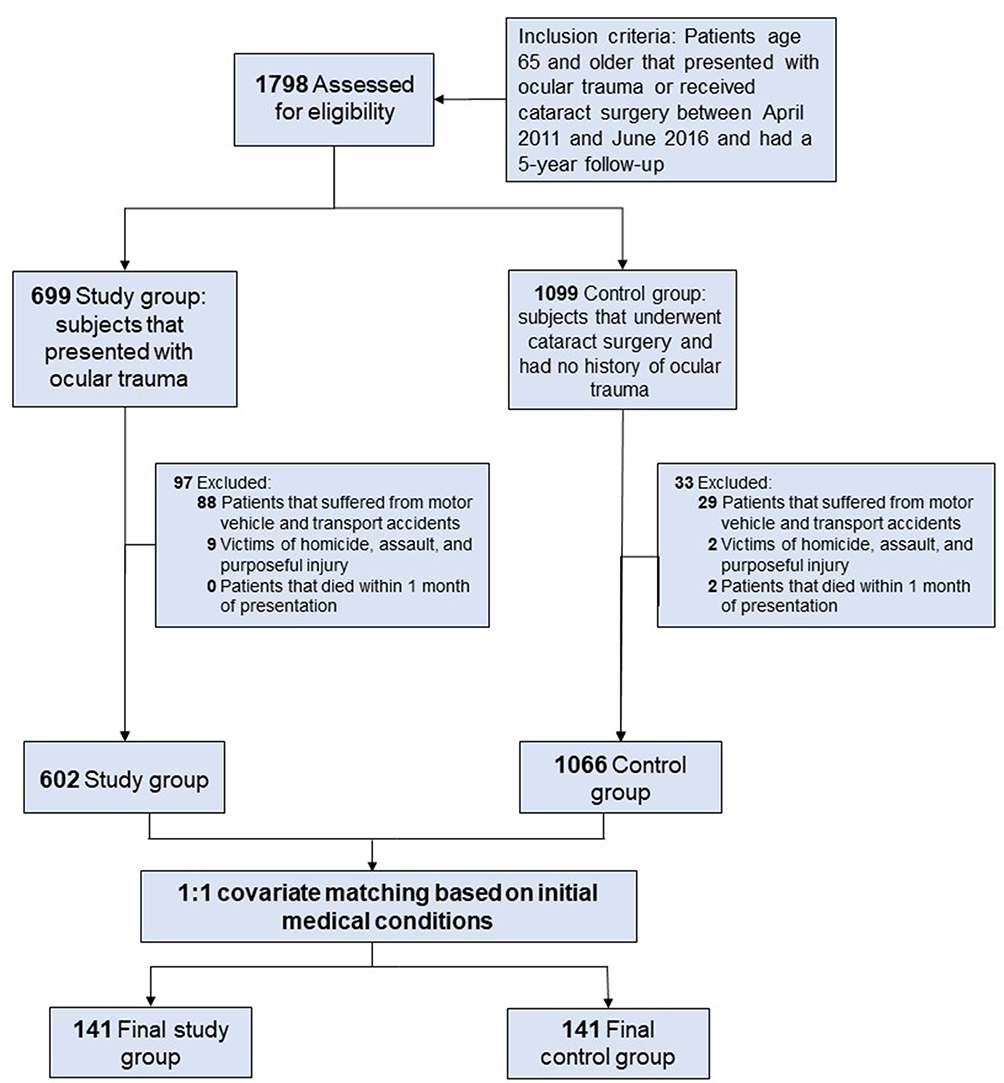 |
Figure 1 From the 1798 patients assessed for eligibility, 602 patients sustained ocular trauma, whereas 1066 patients received non traumatic cataract surgery; both groups were assessed within a 5-year follow up window. Covariate matching was performed based on initial medical conditions, such as baseline cardiovascular and neurological conditions resulting in 141 patients in the final study group and 141 patients in the final control group. |
After it was established that the baseline counts of comorbidities were similar, two-sided Chi-square tests of the final counts between treatment and control were conducted to see if patients in the treatment group developed significantly more comorbidities over the study period. Percent change between final and initial comorbidities was also calculated. The p-values were adjusted using a strict Bonferroni correction to account for the number of comorbidity categories being tested. The family-wise error rate had a p-value < 0.05 chosen for statistical significance when comparing the comorbidities. However, the p-value for individual hypotheses was adjusted using the Bonferroni correction for target p-values of 0.00417 in each category.
The funding source of the study was the NIH 2-T35-AG038047 grant through the Chapel Hill National Training Center's MSTAR program. There were no conflicts of interest amongst the authors of this study. This study was approved by the UNC Institutional Review Board (IRB) prior to starting the project. The research conducted adhered to the tenets of the Declaration of Helsinki. The data accessed complied with all relevant data protection and privacy regulations.
Statistics
Two-sided Chi-squared tests of the comorbidity counts for the twelve subcategories were performed, both at the beginning and end of the study period, to see if there was significant change in the development of cardiovascular or neurological disease. Proportion tests for patient sex and two-sided t-tests for patient age were conducted. All hypothesis tests were controlled at a type I error rate of 0.05. Twelve tests for the differing counts of comorbidities were run, and a Bonferroni correction was applied to each individual test at a type I error rate of 0.05/12, keeping the family error rate at 0.05. The tests for age, sex, and initial comorbidity counts were used to establish similarity between treatment and paired control groups. The tests for the final counts at the end of the study were used to establish the validity of the hypothesis that ocular trauma is associated with an increased risk of developing cardiovascular and neurological comorbidities. The statistical package used was Scipy 1.9, and the software used in this study was Python 3.7.4.
Results
The initial queries identified 1798 patients aged 65 or older who presented with ocular trauma or received cataract surgery between April 2011 and June 2016 and had a 5-year follow-up period. This consisted of 699 patients in the study group presenting with ocular trauma and 1099 patients in the control group presenting for cataract surgery. Subsequent 1:1 covariate matching based on initial medical conditions resulted in a final study group of 141 patients and a final control group of 141 patients. See Table 2 for the full demographic breakdown of the control and study groups.
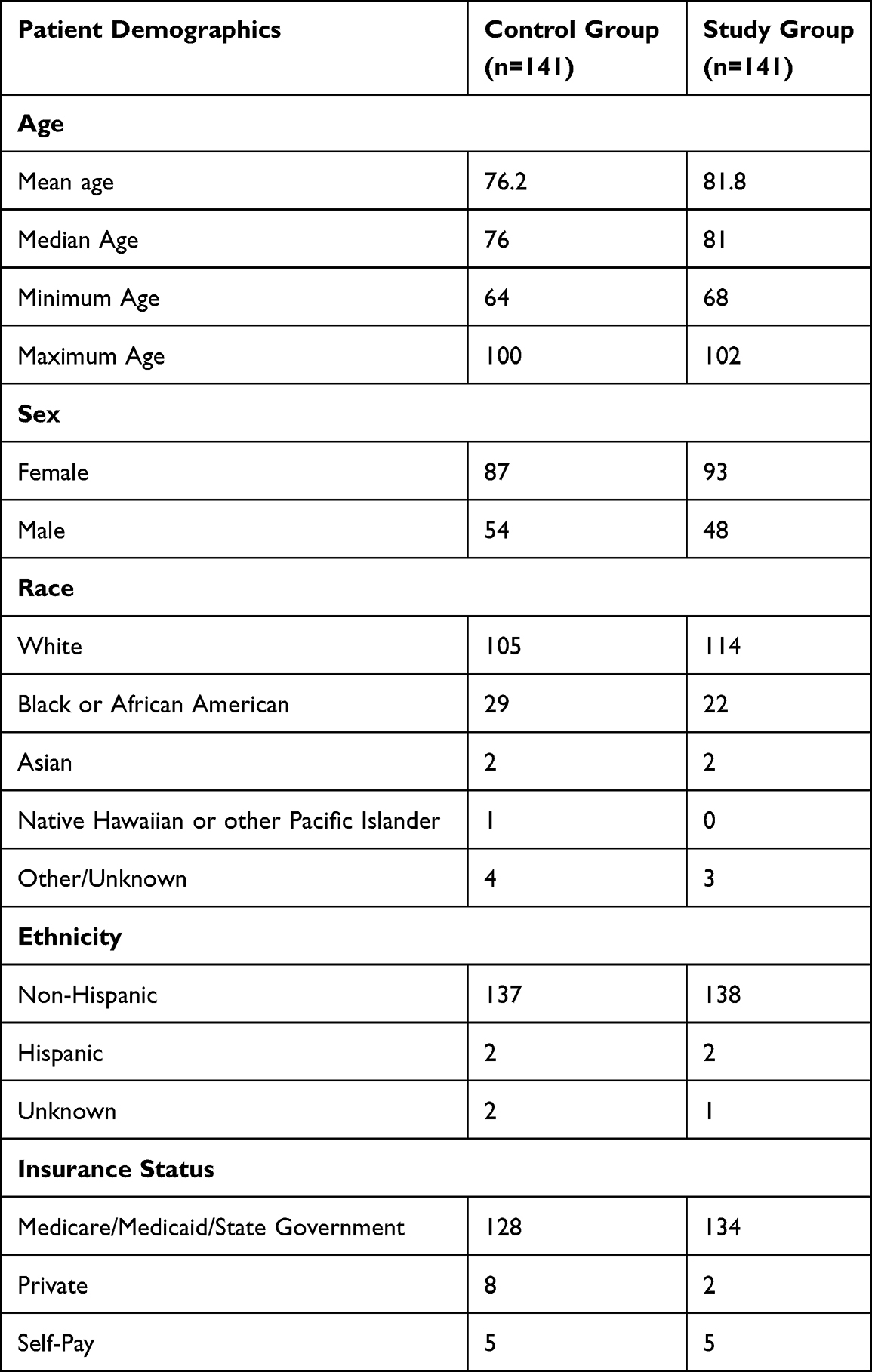 |
Table 2 Patient Demographics of Subjects in Control and Study Group |
The cardiovascular and neurological comorbidities that were compared included cardiac arrhythmias, ischemic heart disease, heart failure, dementia, degenerative disease of the nervous system, polyneuropathy, encephalopathy, Alzheimer’s disease, Parkinson’s disease, vascular disease, hypertensive heart disease, and type 2 diabetes. Initial and final counts of the comorbidities of the study and control group can be found in Table 3. Comorbidity counts record the total number of comorbidities within the group, which may be higher than the number of subjects as individuals may have multiple comorbidities of the same type. The percent change between the final and initial counts of each comorbidity within the study group versus the control group can be found in Table 3. There was a 266% increase in heart failure diagnoses, 234% increase in dementia diagnoses, 153% increase in Alzheimer’s disease diagnoses, and 136% increase in atherosclerosis diagnoses in the study group during the 5 years of follow-up. The study found that patients who sustained ocular trauma were significantly more likely to be diagnosed with heart failure (p=0.00244), dementia (p=0.00002), Alzheimer’s disease (p=0.00087), and vascular disease (p=0.00037). The increased incidence of cardiac arrhythmias (p=0.00463) and degenerative diseases of the nervous system (p=0.00545) in the study group were approaching statistical significance. There was no significant difference in the development of ischemic heart diseases, polyneuropathies, and other disorders of the peripheral nervous system, encephalopathy, Parkinson’s disease, hypertensive heart diseases, and type 2 diabetes.
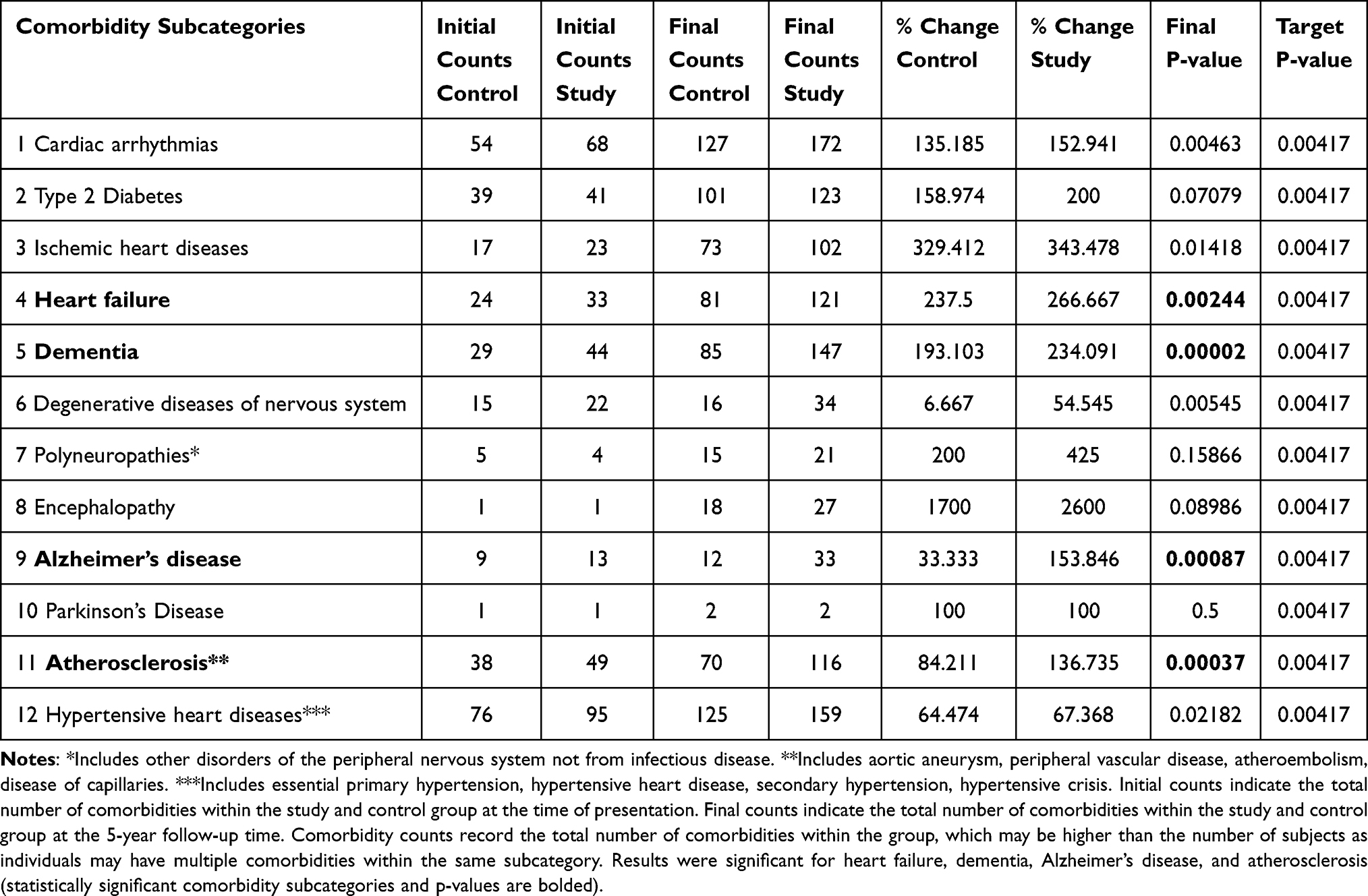 |
Table 3 Comorbidities, Counts, and Statistics |
Discussion
The older population is highly susceptible to falls which can result in ocular injury. To sustain trauma to the eye, there may be a breakdown of the instinctual protective mechanisms that would ordinarily shield the face. We believe that the breakdown of these mechanisms may be an early indicator for underlying systemic disease. In this study, patients who sustained ocular trauma were significantly more likely to develop heart failure (p=0.00244), dementia (p=0.00002), Alzheimer’s disease (p=0.00087), or vascular disease (p=0.00037) within a 5-year window. Of the 141 patients in the study group that presented for ocular trauma with cardiovascular or neurological disease, several presented with cardiac arrhythmias, type 2 diabetes, ischemic heart disease, dementia, degenerative disease, atherosclerosis, and hypertensive heart disease. Further studies are needed to evaluate if they are potential risk factors for ocular injury in the elderly.
Over 800,000 patients are hospitalized every year due to fall-related accidents with associated injuries, such as hip fractures and cranial injuries.18 One study noted that of all the forms of ocular trauma, falls were the most serious and frequent cause; ocular injury can lead to permanent visual or functional deficit.1 Another study focusing on elderly patients in the Bronx corroborated similar findings noting that ocular injuries occurred in patients mostly due to falls in homes or nursing homes.2 Some studies even indicated that fall-related ocular trauma leads to more patient hospitalizations.7 There are an exorbitant number of studies delineating falls as leading causes of ocular trauma or describing the visual outcomes of fall-related trauma. However, there is a lack of literature discussing systemic sequelae of ocular injuries in geriatric patients.3,4 One study does note increased ocular morbidity in fall-associated open globe injury, but few studies underscore the relationship between cardiovascular or neurological comorbidities and ocular trauma in geriatric patients.5 The dearth of research exploring the relationship between ocular trauma and systemic comorbidities is shocking given more than 85% of geriatric patients age 65 and older have 1 or more chronic conditions, as reported by the CDC.16 Certain reasons that contribute to the high risk of falls in geriatric patients include environmental factors, impaired mobility, vestibular dysfunction, cognitive impairment, visual deficit, and medication side effects.19 For a geriatric patient to suffer an injury to the eye or orbit during a fall, there may be impairment of intrinsic protective mechanisms that would normally allow one to protect oneself from the fall. This study’s objective was to explore the development of systemic, cardiovascular, and neurological comorbidities in patients with ocular trauma.
Heart failure affects more than 20 million people worldwide and is associated with significant morbidity and mortality.20 Cardiovascular disease continues to be the leading cause of mortality, morbidity, and healthcare costs. Meanwhile, the interplay between gait and cognition, specifically in terms of executive function and cognitive flexibility, may explain the high prevalence of falls in patients with dementia.21 While the results of this study indicate that elderly individuals who sustain ocular trauma are at higher risk of developing neurologic or cardiovascular disease, it is unclear whether this is an early sign of underlying disease or the precipitating factor. Many studies note that cognitive impairment may be a risk factor for falls in the geriatric community, making ocular trauma more likely in this group.21 However, brain injury can be an associated injury in patients who sustain orbital fractures and may contribute to the development of cognitive impairment.22 Our results indicate that older patients with ocular trauma are at higher risk of developing vascular disease and heart failure. However, vascular diseases such as atherosclerosis or heart failure are typically long-term conditions that gradually worsen over time.23 Atherosclerosis in particular progresses quietly for decades and often manifests in a debilitating manner in the elderly.23 More studies are warranted to understand the mechanisms behind the development of neurologic and cardiovascular disease in ocular trauma patients.
Limitations
Certain limitations of the study include the use of ICD-9 and ICD-10 codes. There was a change from ICD-9 to ICD-10 in 2015, as a result there may be mild changes in grouping of diseases, conditions, procedures, and disorders. Furthermore, there will always be small inconsistencies in the description of some diseases when using databases such as the North Carolina Warehouse for Data that group several diseases together. While using Python and Jupyter Notebook minimizes human error of data collection, there are limitations to using this code as the information is listed in spreadsheets; electronic medical record reviews were not directly conducted. When considering the generalizability of the study, it is important to acknowledge that the majority of patients in this study are non-Hispanic white individuals, which is not representative of the demographic makeup of the United States. Another limitation to consider is that at baseline, patients with cataract surgery have better vision than patients with ocular injury, which could decrease their tendency to fall. Furthermore, patients who have cataract surgery may be more established in their healthcare network and have more thorough management of systemic illnesses. Additionally, due to the covariate matching being based on initial comorbidities, the control group was on average 5 years older than the study group. This age difference may have biased the results regarding development of new comorbidities for which age is a risk factor. One of the limitations of the study includes confounding bias in the elderly population. While the study showed a relationship between cardiovascular and neurological outcomes and ocular trauma, the loss of protective mechanism is not the only factor that leads to falls and ocular injury. There is a plethora of other types of systemic comorbidities and external factors that can influence geriatric health outcomes. Some older patients may have social structures like home health care or a support system to help take care of them. There may be socioeconomic factors to evaluate in future studies including health insurance, type of residence, medical management, polypharmacy, primary care visits. These factors may further explain why there are several older patients with similar comorbidities that do not present with ocular trauma at all.
Conclusion
Older patients that experience an ocular or periocular injury are significantly more likely to develop certain cardiovascular and neurologic diseases in the 5-year period following the injury, including heart failure, dementia, Alzheimer’s disease, or vascular diseases. These patients would benefit from close follow up with a primary care physician so they can be evaluated for underlying cardiovascular or neurologic diseases such as heart failure, vascular disease, and dementia, in particular, Alzheimer’s disease. Further studies are warranted to assess the impact of ocular trauma on mortality and the advent of new comorbidities, especially on systems outside the cardiovascular and neurological systems.
Acknowledgments
NIA 2-T35-AG038047 grant through the UNC-CH Summer Research Training in Aging for Medical Students.
The project described was supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR002489. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIH.
The research reported in this publication was supported by the National Institute on Aging, of the National Institutes of Health, through Grant Award Number T35AG038047. The content is solely the responsibility of the authors and does not necessarily represent the official views of the NIA or NIH.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Sahraravand A, Haavisto AK, Holopainen JM, Leivo T. Ocular trauma in the Finnish elderly - Helsinki Ocular Trauma Study. Acta Ophthalmol. 2018;96(6):616–622. doi:10.1111/aos.13714
2. Chocron IM, Goduni L, Poulsen DM, MbekeanI JN. Patterns of ocular trauma in elderly patients in an urban population-the Bronx experience. Arq Bras Oftalmol. 2020;83(2):113–119. doi:10.5935/0004-2749.20200025
3. Zamani M, Tabatabaei SA, Fotouhi A, Naderan M, Soleimani M. Open globe injuries in geriatric population in Iran: characteristics and outcomes. Int J Ophthalmol. 2021;14(8):1237–1240. doi:10.18240/ijo.2021.08.16
4. Toivari M, Suominen AL, Apajalahti S, Lindqvist C, Snäll J, Thorén H. Isolated orbital fractures are severe among geriatric patients. J Oral Maxillofac Surg. 2018;76(2):388–395. doi:10.1016/j.joms.2017.09.019
5. Emami-Naeini P, Ragam A, Bauza AM, et al. Characteristics, outcomes, and prognostic indicators of fall-related open globe injuries. Retina. 2013;33(10):2075–2079. doi:10.1097/IAE.0b013e31828abe50
6. Kuhn F, Morris R, Witherspoon CD, Mann L. Epidemiology of blinding trauma in the United States Eye Injury Registry. Ophthalmic Epidemiol. 2006;13(3):209–216. doi:10.1080/09286580600665886
7. Halawa O, Mitchell W, Zebardast N. Fall-related eye injury among older adults in the United States. Am J Ophthalmol. 2021;229:82–89. doi:10.1016/j.ajo.2021.03.063
8. Morikawa S, Okamoto Y, Okamoto F, et al. Clinical characteristics and outcomes of fall-related open globe injuries in Japan. Graefes Arch Clin Exp Ophthalmol. 2018;256(7):1347–1352. doi:10.1007/s00417-018-3959-z
9. Lee WS, McNamara P, English J, Meusemann R. Ocular trauma associated with falls in older people: a 10-year review from a state trauma service. Injury. 2020;51(9):2009–2015. doi:10.1016/j.injury.2020.07.029
10. Chang SL, Patel V, Giltner J, Lee R, Marco CA. The relationship between ocular trauma and substance abuse in emergency department patients. Am J Emerg Med. 2017;35(11):1734–1737. PMID: 28705744. doi:10.1016/j.ajem.2017.07.015
11. Andrews BT, Jackson AS, Nazir N, Hromas A, Sokol JA, Thurston TE. Orbit fractures: identifying patient factors indicating high risk for ocular and periocular injury. Laryngoscope. 2016;126(Suppl 4):S5–S11. PMID: 26690301. doi:10.1002/lary.25805
12. Fuller GF. Falls in the elderly. Am Fam Physician. 2000;61(7):2159–68, 2173–4. PMID: 10779256.
13. Kiel DP, O’Sullivan P, Teno JM, Mor V. Health care utilization and functional status in the aged following a fall. Med Care. 1991;29(3):221–228. doi:10.1097/00005650-199103000-00004
14. Vieira ER, Palmer RC, Chaves PH. Prevention of falls in older people living in the community. BMJ. 2016;353:i1419. doi:10.1136/bmj.i1419
15. Lawlor DA, Patel R, Ebrahim S. Association between falls in elderly women and chronic diseases and drug use: cross sectional study. BMJ. 2003;327(7417):712–717. doi:10.1136/bmj.327.7417.712
16. Centers for Disease Control and Prevention. Health Policy Data Requests - Percent of U.S. Adults 55 and over with chronic conditions. Centers for Disease Control and Prevention; 2015. Available from: https://www.cdc.gov/nchs/health_policy/adult_chronic_conditions.htm.
17. Vu T, Finch CF, Day L. Patterns of comorbidity in community-dwelling older people hospitalised for fall-related injury: a cluster analysis. BMC Geriatr. 2011;11(1):45. PMID: 21851627; PMCID: PMC3171714. doi:10.1186/1471-2318-11-45
18. Centers for Disease Control and Prevention, National Center for Injury Prevention and Control. Web–based Injury Statistics Query and Reporting System (WISQARS) [online]; 2023.
19. Institute of Medicine (US) Division of Health Promotion and Disease Prevention. Falls in older persons: risk factors and prevention. In: Berg RL, Cassells JS, editors. The Second Fifty Years: Promoting Health and Preventing Disability. Washington (DC): National Academies Press (US); 1992:15.
20. Orso F, Fabbri G, Maggioni AP. Epidemiology of heart failure. In: Bauersachs J, Butler J, Sandner P, editors. Heart Failure. Handbook of Experimental Pharmacology. Cham: Springer; 2016:243. doi:10.1007/164_2016_74
21. Zhang W, Low LF, Schwenk M, Mills N, Gwynn JD, Clemson L. Review of gait, cognition, and fall risks with implications for fall prevention in older adults with Dementia. Dement Geriatr Cogn Disord. 2019;48(1–2):17–29. PMID: 31743907. doi:10.1159/000504340
22. McCarty JC, Kiwanuka E, Gadkaree S, Siu JM, Caterson EJ. Traumatic brain injury in trauma patients with isolated facial fractures. J Craniofac Surg. 2020;31(5):1182–1185. PMID: 32282477. doi:10.1097/SCS.0000000000006379
23. Ibanez B, Fernández-Ortiz A, Fernández-Friera L, García-Lunar I, Andrés V, Fuster V. Progression of Early Subclinical Atherosclerosis (PESA) Study: JACC Focus Seminar 7/8. J Am Coll Cardiol. 2021;78(2):156–179. doi:10.1016/j.jacc.2021.05.011
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.