Back to Journals » Biologics: Targets and Therapy » Volume 18
The Association Between the rs2200733 SNP and Atrial Fibrillation Among Arabs: A Study from Jordan
Authors Al-Kasasbeh AH, Khabour OF ![]() , Almomani R, Ababneh M
, Almomani R, Ababneh M ![]() , Ibdah R
, Ibdah R ![]() , Jarrah MI
, Jarrah MI ![]() , Rawashdeh SI
, Rawashdeh SI ![]() , Seif AM
, Seif AM ![]()
Received 10 August 2024
Accepted for publication 10 December 2024
Published 17 December 2024 Volume 2024:18 Pages 389—395
DOI https://doi.org/10.2147/BTT.S490891
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Shein-Chung Chow
Abdullah H Al-Kasasbeh,1 Omar F Khabour,2 Rowida Almomani,2 Muhannad Ababneh,1 Rashid Ibdah,1 Mohamad Ismail Jarrah,1 Sukaina I Rawashdeh,1 Abdelsamea Mohammed Seif1
1Department of Internal Medicine, Faculty of Medicine, Jordan University of Science and Technology, Irbid, Jordan; 2Department of Medical Laboratory Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, Irbid, Jordan
Correspondence: Omar F Khabour, Department of Medical Laboratory Sciences, Faculty of Applied Medical Sciences, Jordan University of Science and Technology, P.O.Box 3030, Irbid, 22110, Jordan, Tel +962 790453765, Email [email protected]
Introduction: Atrial fibrillation (AFib) is a common disorder featured by an irregular and fast heartbeat. The etiology of AFib is complex and involves genetic and environmental factors. The rs2200733 single nucleotide polymorphism (SNP) is located in close proximity to the promoter of paired-like homeodomain transcription factor 2 (PITX2) which plays a role in heart development.
Objective: In this study, the association between the rs2200733 SNP and AFib was examined in the Jordanian population.
Methods: The study included 450 subjects (274 controls and 176 patients with AFib). Patients were recruited from King Abdullah University Hospital based on the European Society of Cardiology criteria. The rs2200733 SNP was genotyped using restriction fragment length polymorphism-polymerase chain reaction (RFLP-PCR) technique.
Results: The mutant T allele of the rs2200733 SNP was common in the studied population with a frequency of 19%. The T allele and CT/TT genotypes were prevalent among patients with AFib compared with the controls (P< 0.05, OR [CI]: 1.65 [1.12– 2.43]). In addition, body mass index, diabetes, and hypertension were found to be associated with AFib risk.
Conclusion: The rs2200733 SNP was associated with AFib among Jordanian patients. The mutant T allele of the rs2200733 SNP might increase the risk of AFib.
Keywords: atrial fibrillation, rs2200733, PITX2, RFLP, Jordan, Arabs
Introduction
Atrial fibrillation (AFib) is a common cardiac arrhythmia affects about 1% of the population.1 This is manifested by irregular and rapid cardiac rhythm with the potential for subsequent development of thromboembolic events.2 AFib can significantly increase the risk of stroke and heart failure.3 AFib can be symptomatic as patients may typically experience palpitations and dyspnea, however it can also be asymptomatic and discovered incidentally.4
The disease is usually caused by structural problems with the heart. Causes of AFib include coronary artery disease, congenital heart disorders, heart valve disease, high blood pressure, pulmonary diseases, history of heart surgery, and thyroid disorders.5 AFib is also related to aging, alcoholism, body mass index, diabetes mellitus, and sleep apnea.6
The risk of developing AFib can also be influenced by family history. For example, it is estimated that about 30% of all cases of AFib have a history of the condition in their family.7 Therefore, inherited genetic variations can affect the risk of AFib.8 Among the proposed variants that increase the risk of AFib is the rs2200733 single nucleotide polymorphism (SNP) located near the promoter of paired-like homeodomain transcription factor 2 (PITX2), thus modulating PITX2 transcription as previously reported.9,10 PITX2 plays an important embryonic role in left/right asymmetry signaling including heart development. PITX2 is also expressed in cardiac tissue during adulthood where it is involved in atrial ions balance including calcium.11,12 The rs2200733 SNP has been shown to modulate risk of AFib in several populations.13–16 Conversely, the rs2200733 SNP was not associated with AFib risk among a Hispanic/Latino cohort in the USA.17 Therefore, the association between the rs2200733 SNP and AFib could vary according to the genetic background of the population.
In Arab countries, there is still a need to study the contribution of the rs2200733 SNP to the risk of AFib. Therefore, the current study aimed to examine the association of the rs2200733 SNP with AFib risk in the Jordanian population.
Methods
Subjects
The study is case-control in design and was conducted between April 2022 and May 2024. Subjects with AFib (62.5 ±15.9 years old) were recruited from cardiology out-patient clinics in King Abdullah University Hospital (KAUH), Irbid, Jordan, which is the largest tertiary healthcare provider in northern Jordan and the only center providing percutaneous coronary interventional service, serving approximately 3 million inhabitants. Health controls (without history of AFib, 60.2±12.3 years old) volunteered to be part of the study. Patients with evidence of AFib were selected and invited to participate in the study. AFib was confirmed by a consultant physician (Dr. Abdullah Al-Kasasbeh) according to the European Society of Cardiology diagnostic criteria and based on electrocardiogram data.18 Patients with defects/disorders of heart structure, congestive heart failure, none-AFib arrhythmias, cancer, autoimmune/blood conditions, liver/renal diseases, and thyroid dysfunction were excluded from the study.19,20 The study was approved by the Ethics Committee at King-Abdullah University Hospital (KAUH, ID: 213–2022), and was conducted in accordance with the Declaration of Helsinki and its amendments. Informed consent was granted from all subjects before beginning study procedures. This includes access to the clinical records of patients in KAUH. Sociodemographic characteristics such as age, gender, weight, height, smoking status, and family history of atrial fibrillation were obtained using a paper questionnaire.
Blood Sampling and DNA Extraction
Whole blood in EDTA tubes (3 mL) was obtained from all participants for DNA analysis. Samples were stored at −20°C until use. Blood DNA was isolated using a column-based extraction kit (Qiagen, Düsseldorf, Germany). The integrity of the extracted DNA was assessed using electrophoresis and spectrometric techniques (BioRad-Smart Spec 3000, USA). Isolated DNA was kept at −20°C until used.
The rs2200733 Genotyping Assay
The rs2200733nSNP was genotyped using PCR as previously described.19 The PCR primers were forward: “5′TATTCACAGGCTTCCCTCTA3′” and reverse: “5′AATGCTGTGGGAACATAAAC3′”. PCR steps were 95°C for 5min, thirty cycles of 95°C/35sec, 60°C/40sec, and 72°C/40sec, and extension of 72°C/5min. The PCR product (178bp) was exposed to Kzo9I enzyme (cuts at GATC site, Biolabs, USA) at 37°C overnight. The amplified fragment containing the C allele is cleaved by the enzyme to give 109bp and 69bp fragments (Figure 1). The amplified fragment containing T allele is resistant to the enzyme. DNA fragments were analyzed after enzymatic digestion with 3% agarose and ethidium bromide.
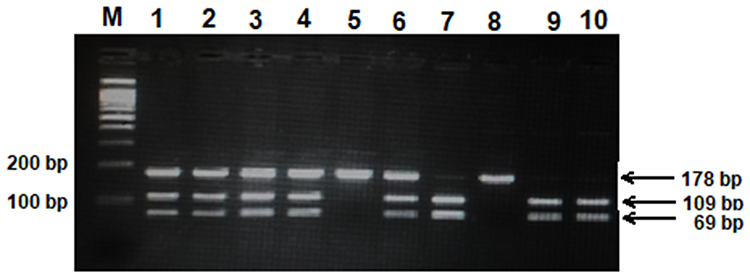 |
Figure 1 Gel electrophoresis image of restriction fragment length polymorphism – polymerase chain reaction (RFLP-PCR) of rs2200733 polymorphism. The amplified PCR product containing rs2200733 polymorphism (178bp) were exposed to Kzo9I restriction enzyme. Digestion of the amplified product with the enzyme produces 109bp and 69bp fragments. Lane M represents a 100bp marker. Lanes 1–4, and 6 represent CT genotype. Lanes 7.9, and 10 represent CC genotype. Lane 5 represents TT genotype. |
Statistical Analysis
Sample size calculation was performed using G*Power 3.1 software with an effect size of 0.25, alpha=0.05 and power of 0.95. The calculated sample size was 164 participants. Continuous variables were assessed using GraphPad program (version 7, USA). The association between genotype frequencies and haplotype frequencies with AFib was conducted using SNPstats program. SNPstats was also used to assess Hardy Weinberg equilibrium for the examined SNP. A p-value of less than 0.05 indicates a significant difference.
Results
Table 1 shows characteristics of the study subjects. Age (mean ± SD) was 60.2±12.3 for the control group and 62.5±15.9 for the AFib group (p=0.085). The ratio of men to women and smoking frequency were similar between the two groups (P>0.05). Other parameters (hypertension, family history and diabetes) were more frequent in AFib compared with controls (P<0.01). Moreover, body mass index (BMI) was higher in AFib than controls (P<0.01).
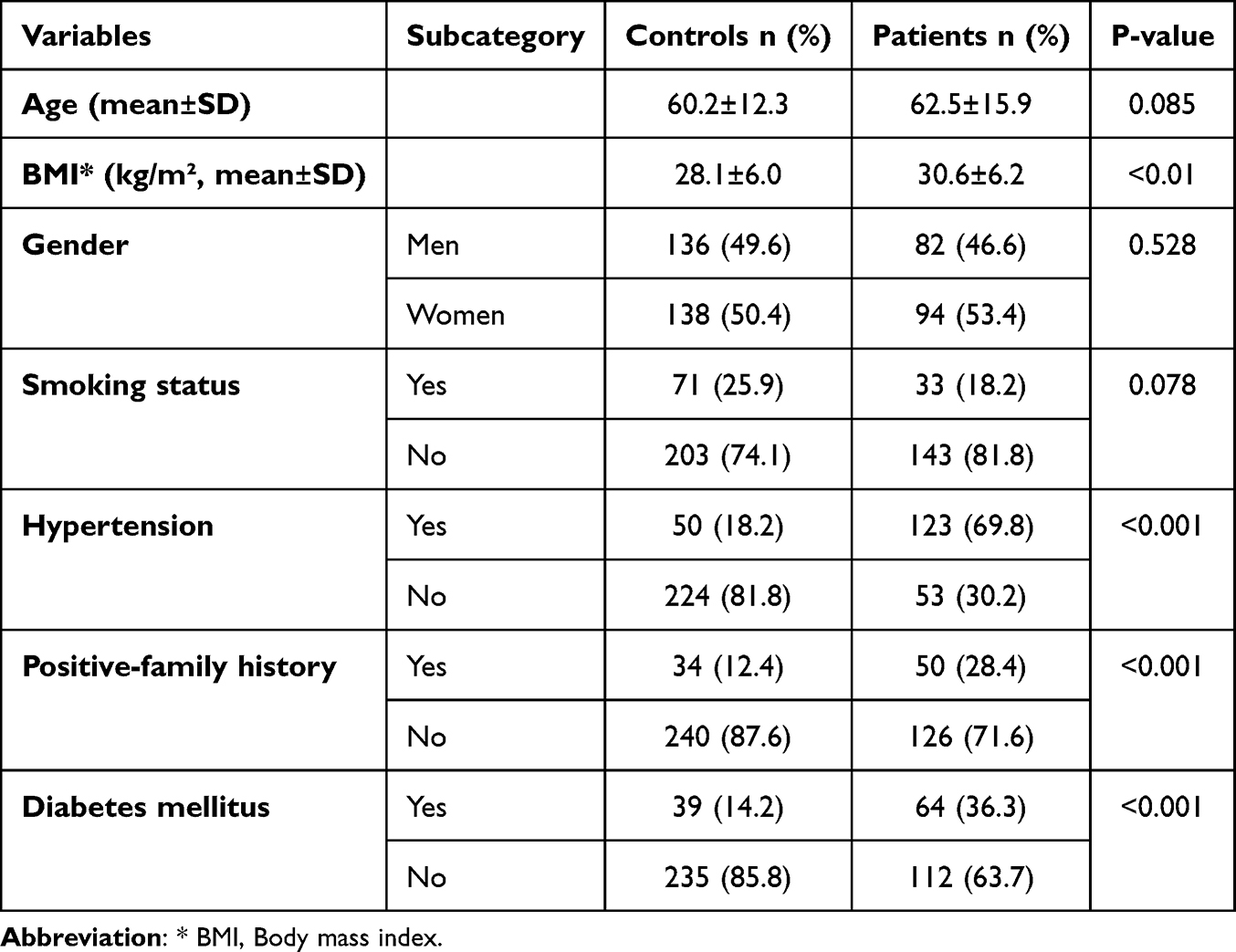 |
Table 1 The Demographic Characteristics of the Participants |
The distribution of rs2200733 SNP genotypes among the study groups is shown in Table 2. The C allele and CC genotype are prevalent among the study subjects (78% and 62%, respectively). The mutant T allele and C/T+TT genotypes were higher among AFib compared to controls (P<0.05, OR [CI]: 1.65 [1.12–2.43]).
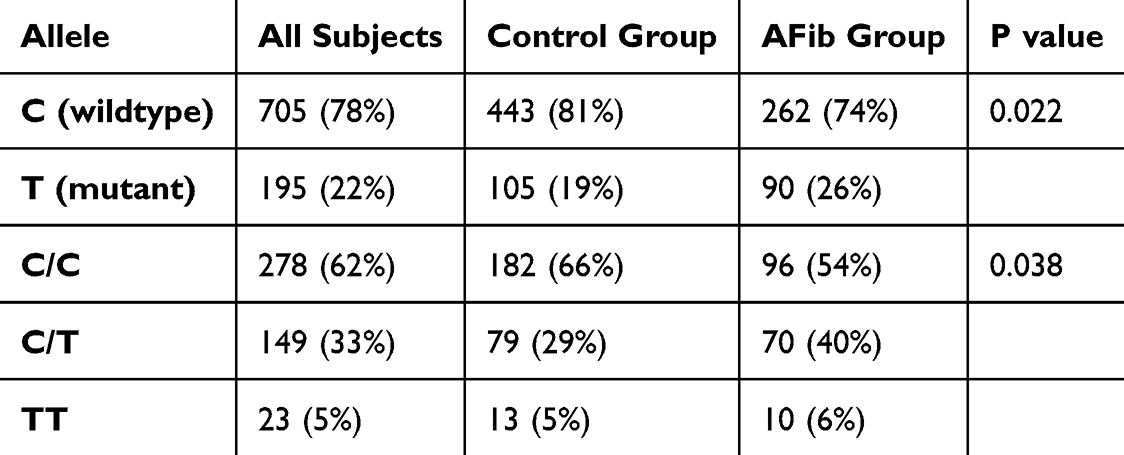 |
Table 2 The Distribution of rs2200733 Alleles and Genotypes Among the Study Groups |
Table 3 shows the association between rs2200733 and AFib according to different inheritance models. The results showed an association between rs2200733 and AFib in all inheritance models except the recessive model. The C/T and T/T genotypes increase the risk of AFib by odd ratios of 1.63 to 1.68 (P<0.05). Therefore, the presence of the T allele significantly increased the risk of AFib in the studied population.
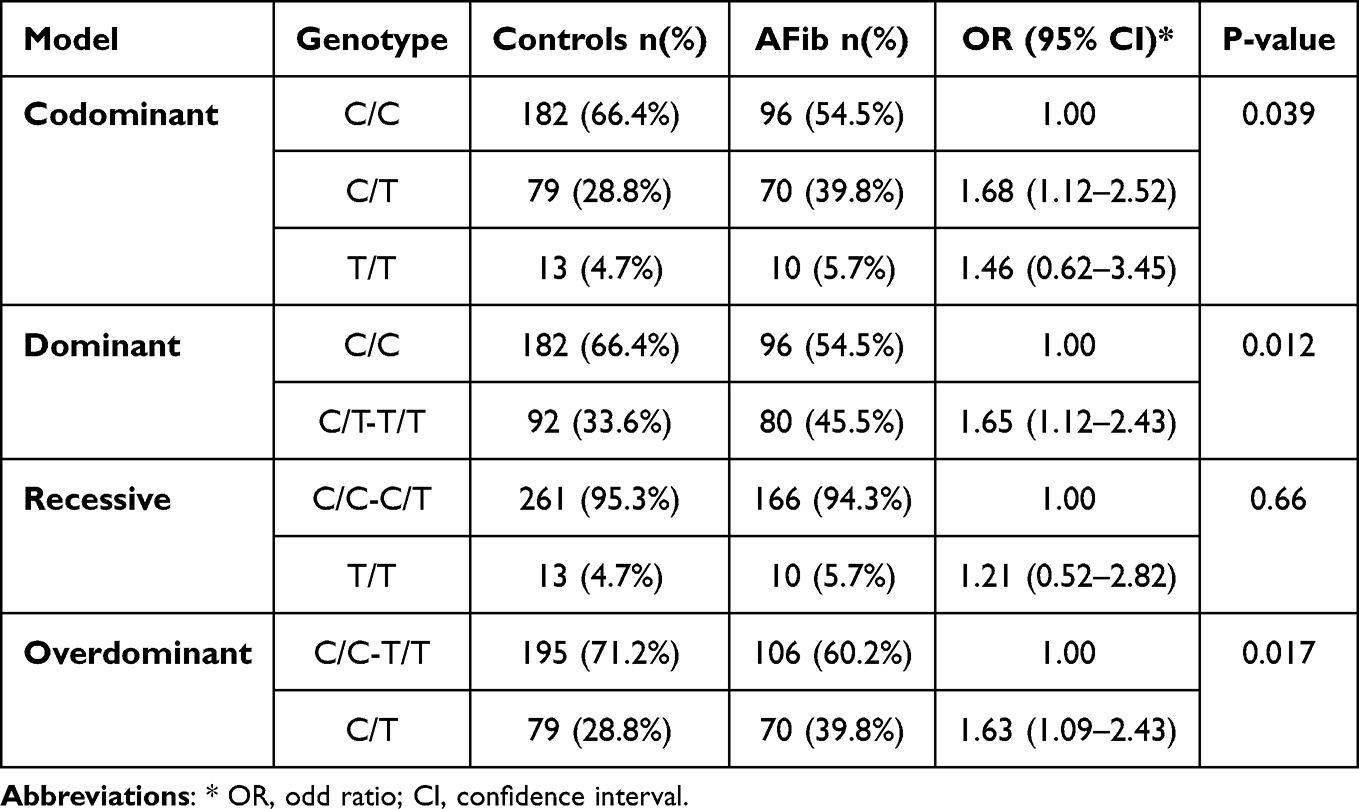 |
Table 3 The Association Between rs2200733 and Atrial Fibrillation Among the Studied Population |
Table 4 shows the frequency of the mutant rs2200733 T allele among different world populations. The T allele is common in Chinese and Taiwanese populations (50–60%). However, the mutant T allele is less common in European and Middle Eastern populations (range 10–23%). In the United States, the frequency of the T allele is about 31%. Thus, the T allele frequency spectrum is observed among the world populations.
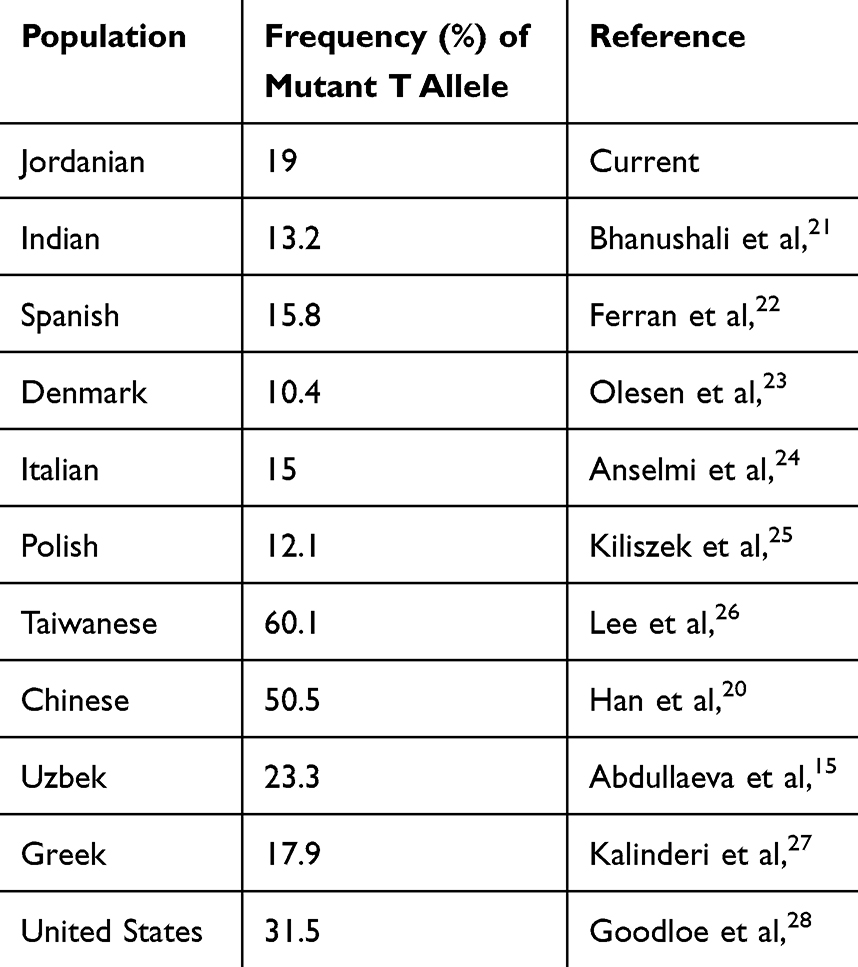 |
Table 4 The Frequency of the rs2200733 T Allele in Different World Populations |
Discussion
In the current study, the rs2200733 was associated with AFib in the Jordanian population. The mutant T allele and the CT and TT genotypes were found to increase the risk of AFib. These findings are consistent with previous reports from other populations. In a genome-wide association study, rs2200733 was found to be associated with AFib in European and Asian populations.29 The mutant T allele has been reported to increase the risk of AFib by 3 folds in the Indian population.21 In a Spanish study, the rs2200733 was found to increase the risk of AFib by an odd ratio of 1.87.22 Similar findings have been reported among Italian, Uzbek, Polish, Chinese, Greek and Taiwanese populations.20,24–27 Among Danish and US populations, rs2200733 was associated with onset of lone AFib.23,28,30 The rs2200733 was found to increase the risk of cardioembolic stroke related to AF in Polish subjects.31 Finally, the rs2200733 has been reported to increase the risk of AFib recurrence after catheter ablation.32 Conversely, the rs2200733 was not associated with AFib risk among the Hispanic/Latino cohort in the USA.17
The clinical significance of the rs2200733 is well documented. In addition to Afib, this variant has been shown to be associated with the incidence of congenital esophageal atresia in the Chinese population,33 the development of preeclampsia in the Indian population,34 ischemic stroke in the non-Asian populations,35 and obstructive sleep apnea in the US population.36
The rs2200733 is in close proximity to the PITX2 gene and can modulate gene transcription.9,10 PITX2 plays a role in left-right anatomical asymmetry, pulmonary cardiomyogenesis, and atrial resting membrane potential.11,12 PITX2 is also involved in regulating ionic conduction and calcium balance in atrial cardiomyocytes.37,38 A significant reduction in PITX2 has been reported in patients with sustained AFib.39 In-silico investigations suggested that Pitx2 insufficiency induced arrhythmia by inductive structural remodeling and the subsequent depolarizations and re-entrant excitation modulation.40,41
In the current study, the frequency of the mutant T allele was found to be 19%. This frequency is close to what has been reported in European and Asian countries such as Greece, Italy, Spain, Poland, Uzbekistan, and India.19,21–25,27 However, higher frequencies (31–60%) have been reported in populations from China, Taiwan, and USA.20,26–28 Thus, a wide spectrum of mutant T allele frequencies has been observed globally.
In the present study, body mass index, diabetes, and hypertension were reported to be associated with AFib. This finding is consistent with several previous studies.42–46 In general, obesity negatively impacts cardiovascular hemodynamics and causes structural cardiac remodeling that can cause cardiovascular diseases including AFib.42 In addition, hypertension is a common risk factor for AFib by inducing atrial structural and electrophysiologic manifestations.44,45 Similarly, diabetes is linked to AFib by causing structural and electrical remodeling in the myocardium.46
A limitation of the study is that the impact of rs2200733 on the expression of PITX2 in subjects was not investigated. In addition, other SNPs affecting the expression of PITX2 such as the rs6843082 SNP have not been investigated. Future studies that address such limitations are highly recommended.
Conclusion
The rs2200733 is associated with AFib among Jordanian patients. The mutant T allele of the rs2200733 might increase the risk of AFib. In addition, factors such as obesity, diabetes, and hypertension are associated with the development of AFib. Combining the rs2200733 polymorphism with other identified risk factors in a model predicting the occurrence of AFib could identify the at-risk group in Jordan. Finally, future studies linking the rs2200733 polymorphism with the expression of PITX2 in patients could shed light on the mechanisms by which the rs2200733 polymorphism increases the risk of AFib.
Acknowledgment
The authors would like to thank Miss. Ayat Alazam and Miss. Balqis Abu-Musa for their help in recruitment of subjects and experimental work.
Funding
The study was funded by a grant from Jordan University of Science and Technology (grant number 213-2022) to OK.
Disclosure
Authors have nothing to disclose.
References
1. Staerk L, Sherer JA, Ko D, Benjamin EJ, Helm RH. Atrial fibrillation: epidemiology, pathophysiology, and clinical outcomes. Circ Res. 2017;120(9):1501–1517. doi:10.1161/CIRCRESAHA.117.309732
2. Wijesurendra RS, Casadei B. Mechanisms of atrial fibrillation. Heart. 2019;105(24):1860–1867. doi:10.1136/heartjnl-2018-314267
3. Healey JS, Amit G, Field TS. Atrial fibrillation and stroke: how much atrial fibrillation is enough to cause a stroke? Curr Opin Neurol. 2020;33(1):17–23. doi:10.1097/WCO.0000000000000780
4. Verma KP, Wong M. Atrial fibrillation. Aust J Gen Pract. 2019;48(10):694–699. doi:10.31128/AJGP-12-18-4787
5. Zimetbaum P. Atrial Fibrillation. Ann Internal Med. 2017;166(5):Itc33–itc48. doi:10.7326/AITC201703070
6. Csengeri D, Sprünker NA, Di Castelnuovo A, et al. Alcohol consumption, cardiac biomarkers, and risk of atrial fibrillation and adverse outcomes. Eur Heart J. 2021;42(12):1170–1177. doi:10.1093/eurheartj/ehaa953
7. Lozano-Velasco E, Franco D. Genetics and epigenetics of atrial fibrillation. Int J Mol Sci. 2020;21(16):5717. doi:10.3390/ijms21165717
8. Campbell HM, Wehrens XHT. Genetics of atrial fibrillation: an update. Curr Opin Cardiol. 2018;33(3):304–310. doi:10.1097/HCO.0000000000000505
9. Li N, Dobrev D, Wehrens XH. PITX2: a master regulator of cardiac channelopathy in atrial fibrillation? Cardiovasc Res. 2016;109(3):345–347. doi:10.1093/cvr/cvw008
10. Shoemaker MB, Bollmann A, Lubitz SA, et al. Common genetic variants and response to atrial fibrillation ablation. Circulation. 2015;8(2):296–302. doi:10.1161/CIRCEP.114.001909
11. Mommersteeg MT, Brown NA, Prall OW, et al. Pitx2c and Nkx2-5 are required for the formation and identity of the pulmonary myocardium. Circ Res. 2007;101(9):902–909. doi:10.1161/CIRCRESAHA.107.161182
12. Syeda F, Holmes AP, Yu TY, et al. PITX2 modulates atrial membrane potential and the antiarrhythmic effects of sodium-channel blockers. J Am Coll Cardiol. 2016;68(17):1881–1894. doi:10.1016/j.jacc.2016.07.766
13. He J, Zhu W, Yu Y, Hu J, Hong K. Variant rs2200733 and rs10033464 on chromosome 4q25 are associated with increased risk of atrial fibrillation after catheter ablation: evidence from a meta-analysis. Cardiol J. 2018;25(5):628–638. doi:10.5603/CJ.a2017.0143
14. Lubitz SA, Sinner MF, Lunetta KL, et al. Independent susceptibility markers for atrial fibrillation on chromosome 4q25. Circulation. 2010;122(10):976–984. doi:10.1161/CIRCULATIONAHA.109.886440
15. Mohanty S, Santangeli P, Bai R, et al. Variant rs2200733 on chromosome 4q25 confers increased risk of atrial fibrillation: evidence from a meta-analysis. J Cardiovasc Electrophysiol. 2013;24(2):155–161. doi:10.1111/jce.12017
16. Hu Z, Zou D. Genotype-phenotype associations in atrial fibrillation: meta-analysis. J Interv Card Electrophysiol. 2019;54(3):283–288. doi:10.1007/s10840-018-0484-2
17. Chalazan B, Mol D, Sridhar A, et al. Genetic modulation of atrial fibrillation risk in a Hispanic/Latino cohort. PLoS One. 2018;13(4):e0194480. doi:10.1371/journal.pone.0194480
18. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2020;42(5):373–498.
19. Abdullaeva G, Abdullaev A, Kevorkov A, Abduvaliyeva G, Zakirov N, Kurbanov R. Interrelation between the rs2200733 polymorphism of the ATFB5 gene and atrial fibrillation in Uzbek patients. Turk Kardiyoloji Dernegi Arsivi. 2021;49(5):404–409. doi:10.5543/tkda.2021.08434
20. Shen Han Y, Ahmed AM, Chao Z, Jun W, Xiaochen Y. Association between rs2200733 polymorphism of PITX2 gene and the risk of atrial fibrillation. Anatol J Cardiol. 2023;27(3):160–166. doi:10.14744/AnatolJCardiol.2022.2276
21. Bhanushali A, Nair A, Jagdale G, Suvarna T, Das BR. Association of genetic variants at the 4q25 locus with atrial fibrillation in Indian population. J Clin Lab Analysis. 2017;31(1). doi:10.1002/jcla.22017
22. Ferrán A, Alegret JM, Subirana I, et al. Association between rs2200733 and rs7193343 genetic variants and atrial fibrillation in a Spanish population, and meta-analysis of previous studies. Revista Espanola de Cardiologia (English Ed). 2014;67(10):822–829. doi:10.1016/j.recesp.2013.12.021
23. Olesen MS, Holst AG, Jabbari J, et al. Genetic loci on chromosomes 4q25, 7p31, and 12p12 are associated with onset of lone atrial fibrillation before the age of 40 years. Can J Cardiol. 2012;28(2):191–195. doi:10.1016/j.cjca.2011.11.016
24. Viviani Anselmi C, Novelli V, Roncarati R, et al. Association of rs2200733 at 4q25 with atrial flutter/fibrillation diseases in an Italian population. Heart. 2008;94(11):1394–1396. doi:10.1136/hrt.2008.148544
25. Kiliszek M, Franaszczyk M, Kozluk E, et al. Association between variants on chromosome 4q25, 16q22 and 1q21 and atrial fibrillation in the Polish population. PLoS One. 2011;6(7):e21790. doi:10.1371/journal.pone.0021790
26. Lee KT, Yeh HY, Tung CP, et al. Association of RS2200733 but not RS10033464 on 4q25 with atrial fibrillation based on the recessive model in a Taiwanese population. Cardiology. 2010;116(3):151–156. doi:10.1159/000318172
27. Kalinderi K, Fragakis N, Koskinas KC, et al. Association between rs2200733 polymorphism on chromosome 4q25 and atrial fibrillation in a Greek population. Hell J Cardiol. 2015;56(3):224–229.
28. Goodloe AH, Herron KJ, Olson TM. Uncovering an intermediate phenotype associated with rs2200733 at 4q25 in lone atrial fibrillation. Am J Cardiol. 2011;107(12):1802–1805. doi:10.1016/j.amjcard.2011.02.326
29. Gudbjartsson DF, Arnar DO, Helgadottir A, et al. Variants conferring risk of atrial fibrillation on chromosome 4q25. Nature. 2007;448(7151):353–357. doi:10.1038/nature06007
30. Henningsen KM, Olesen MS, Haunsoe S, Svendsen JH. Association of rs2200733 at 4q25 with early onset of lone atrial fibrillation in young patients. Scan Cardiovasc J. 2011;45(6):324–326. doi:10.3109/14017431.2011.594081
31. Wnuk M, Pera J, Jagiełła J, et al. The rs2200733 variant on chromosome 4q25 is a risk factor for cardioembolic stroke related to atrial fibrillation in Polish patients. Neurologia i neurochirurgia polska. 2011;45(2):148–152. doi:10.1016/S0028-3843(14)60026-8
32. Rattanawong P, Chenbhanich J, Vutthikraivit W, Chongsathidkiet P. A chromosome 4q25 variant is associated with atrial fibrillation recurrence after catheter ablation: a systematic review and meta-analysis. J Atr Fibrillation. 2018;10(6):1666. doi:10.4022/jafib.1666
33. Ke J, Tao J, Chen K. The association between polymorphisms in PITX2 and congenital esophageal atresia susceptibility. Am J Transl Res. 2021;13(8):9808–9813.
34. Rani U, Praveen Kumar KS, Munisamaiah M, Rajesh D, Balakrishna S. Atrial fibrillation associated genetic variation near PITX2 gene increases the risk of preeclampsia. Pregnancy Hypertens. 2018;13:214–217. doi:10.1016/j.preghy.2018.06.023
35. Wang D, Hu X, Yang X, Yang M, Wu Q. Variants rs2200733 and rs6843082 show different associations in Asian and Non-Asian populations with ischemic stroke. Front Genetics. 2022;13:905560. doi:10.3389/fgene.2022.905560
36. Patel NJ, Wells QS, Huang S, Upender RP, Darbar D, Monahan K. Relation of obstructive sleep apnea and a common variant at chromosome 4q25 to atrial fibrillation. Am j Cardiol. 2017;119(9):1387–1391. doi:10.1016/j.amjcard.2017.01.038
37. Kim K, Blackwell DJ, Yuen SL, et al. The selective RyR2 inhibitor ent-verticilide suppresses atrial fibrillation susceptibility caused by Pitx2 deficiency. J Mol Cell Cardiol. 2023;180:1–9. doi:10.1016/j.yjmcc.2023.04.005
38. Bai J, Zhu Y, Lo A, Lu Y, Zhao J In silico assessment of genetic variation in PITX2 reveals the molecular mechanisms of calcium-mediated cellular triggered activity in atrial fibrillation. In:
39. Chinchilla A, Daimi H, Lozano-Velasco E, et al. PITX2 insufficiency leads to atrial electrical and structural remodeling linked to arrhythmogenesis. Circulation. 2011;4(3):269–279. doi:10.1161/CIRCGENETICS.110.958116
40. Bai J, Lo A, Gladding PA, Stiles MK, Fedorov VV, Zhao J. In silico investigation of the mechanisms underlying atrial fibrillation due to impaired Pitx2. PLoS Comput Biol. 2020;16(2):e1007678. doi:10.1371/journal.pcbi.1007678
41. Bai J, Lu Y, Zhu Y, et al. Understanding PITX2-dependent atrial fibrillation mechanisms through computational models. Int J Mol Sci. 2021;22(14):7681. doi:10.3390/ijms22147681
42. Lavie CJ, Pandey A, Lau DH, Alpert MA, Sanders P. Obesity and atrial fibrillation prevalence, pathogenesis, and prognosis: effects of weight loss and exercise. J Am Coll Cardiol. 2017;70(16):2022–2035. doi:10.1016/j.jacc.2017.09.002
43. Bizhanov KA, Аbzaliyev KB, Baimbetov AK, Sarsenbayeva AB, Lyan E. Atrial fibrillation: epidemiology, pathophysiology, and clinical complications (literature review). J Cardiovasc Electrophysiol. 2023;34(1):153–165. doi:10.1111/jce.15759
44. Dzeshka MS, Shantsila A, Shantsila E, Lip GYH. Atrial fibrillation and hypertension. Hypertension. 2017;70(5):854–861. doi:10.1161/HYPERTENSIONAHA.117.08934
45. Dzeshka MS, Shahid F, Shantsila A, Lip GYH. Hypertension and atrial fibrillation: an intimate association of epidemiology, pathophysiology, and outcomes. Am J Hypertens. 2017;30(8):733–755. doi:10.1093/ajh/hpx013
46. Wang A, Green JB, Halperin JL, Piccini JP. Atrial fibrillation and diabetes mellitus: JACC review topic of the week. J Am Coll Cardiol. 2019;74(8):1107–1115. doi:10.1016/j.jacc.2019.07.020
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.