Back to Journals » Clinical Ophthalmology » Volume 20
The Association Between Retinal Nerve Fibre Layer Loss and Forceps Trauma During Surgery for Idiopathic Full Thickness Macular Hole
Authors Raimondi R ![]() , Ferrara M, Rivera-Real A, Hillier RJ, Habib MS, Sandinha MT, Peto T, Curran K, Muldrew A, Steel DHW
, Ferrara M, Rivera-Real A, Hillier RJ, Habib MS, Sandinha MT, Peto T, Curran K, Muldrew A, Steel DHW ![]()
Received 11 December 2024
Accepted for publication 13 June 2025
Published 2 February 2026 Volume 2026:20 507581
DOI https://doi.org/10.2147/OPTH.S507581
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Raffaele Raimondi,1 Mariantonia Ferrara,1,2,* Antonio Rivera-Real,3,* Roxane J Hillier,4,5 Maged S Habib,1,3 Maria T Sandinha,6,7 Tunde Peto,8 Katie Curran,8 Alyson Muldrew,8 David H W Steel1,3
1Sunderland Eye Infirmary, South Tyneside and Sunderland NHS Foundation Trust, Sunderland, UK; 2School of Medicine, University of Malaga, Malaga, 29016, Spain; 3Bioscience Institute, Newcastle University, Newcastle Upon Tyne, UK; 4Newcastle Eye Centre, Royal Victoria Infirmary, Newcastle Upon Tyne, UK; 5Translational and Clinical Research Institute, Newcastle University, Newcastle Upon Tyne, UK; 6St. Paul’s Eye Unit, the Royal Liverpool University Hospital, Liverpool, UK; 7Department of Eye and Vision Science, Institute of Ageing & Chronic Disease, University of Liverpool, Liverpool, UK; 8Centre for Public Health, Queen’s University of Belfast, Belfast, UK
*These authors contributed equally to this work
Correspondence: David H W Steel, Sunderland Eye Infirmary, South Tyneside and Sunderland NHS Foundation Trust, Queen Alexandra Road, Sunderland, SR2 9HP, UK, Email [email protected] Raffaele Raimondi, Sunderland Eye Infirmary, South Tyneside and Sunderland NHS Foundation Trust, Queen Alexandra Road, Sunderland, SR2 9HP, UK, Email [email protected]
Purpose: This study investigated the relationship between forceps trauma during internal limiting membrane (ILM) peeling and its effects on focal and overall retinal nerve fibre layer (RNFL) loss and their impact on central visual fields following macular hole surgery.
Methods: We conducted a post hoc analysis of ILM peeling surgeries for idiopathic full thickness macular hole collected previously as part of a prospective study. This included video analysis to assess the position of ILM pick-up points (PUPs), associated retinal hemorrhages, and the overall duration of ILM peeling. Subsequently, we correlated these findings with multimodal imaging as well as visual field data at 3 weeks and 6 months postoperatively.
Results: The analysis encompassed a total of 43 eyes of 43 patients, with 213 PUPs performed by four experienced surgeons. The median peeling time was 263 seconds and the median number of PUPs per case was 5.6. PUPs were found to be associated with hemorrhages and subacute nerve fibre layer swelling (SANFL) lesions in approximately 20% of cases overall. Although PUPs, especially those linked with SANFL lesions and hemorrhages, were associated with focal RNFL defects, most defects were in the outer temporal sector of the macula and unrelated to PUPs. There were 192 focal RNFL defects observed but only 16% were associated with PUPs. PUPs in the inner and temporal sectors of the macula, and the severity of a DONFL appearance, demonstrated a significant correlation with peripapillary RNFL loss on multivariate analysis. No correlation between central visual field improvement and any of the anatomical changes was found.
Conclusion: Whilst forceps trauma can result in SANFL lesions and focal RNFL loss, over 80% of focal RNFL defects observed after ILM peeling are not associated with PUPs and may be more associated with the act of ILM avulsion from the underlying retina during peeling.
Keywords: ILM peeling, forceps, SANFL, DONFL, iatrogenic damage, peel maculopathy
Key Messages
What is known
- Dissociated optic nerve fiber layer appearance (DONFL) and subacute nerve fiber layer swelling (SANFL) can be observed after ILM peeling surgery.
- Forceps trauma during ILM pick up can result in SANFL lesions and focal RNFL loss.
What is new
- Over 80% of focal RNFL defects observed after ILM peeling are not associated with forceps pickup points.
- Focal RNFL defects may be more associated with the act of ILM avulsion from the underlying retina during peeling than with the ILM peeling pickup points.
Introduction
Peeling of the Internal limiting membrane (ILM) as part of vitreoretinal surgery has become a common procedure with several advantages in a range of conditions. These include a reduction in the recurrence rate of epiretinal membranes (ERM) by removing the scaffold; and an increased likelihood of idiopathic full thickness macular hole (iFTMH) closure with a decrease in reopening rates.1,2 However, there have been a variety of retinal changes observed after ILM peeling with potential adverse effects.3 These include a dissociated optic nerve fibre layer appearance (DONFL), and subacute nerve fibre layer swelling (SANFL).3–5 DONFL describes a characteristic irregular appearance to the inner retina starting 1-2-months post ILM peeling and associated with focal depressions in the inner retinal surface. SANFL can be seen as areas of arcuate hypo-reflectivity on infrared imaging in the first few weeks after surgery, associated with inner retinal thickening and sometimes later atrophy. Local pick-up point (PUP) trauma when using “pinch peeling” has been proposed as the aetiological factor for at least some of these changes, particularly SANFL.6 It has also been shown using intraoperative Optical Coherence Tomography (OCT) that an acute diffuse post-peel increase in inner retinal thickness is associated with the development of a later DONFL appearance, and it has been postulated that peeling techniques may influence this.7 Similarly, peeling using a diamond dusted membrane scraper on the ILM to propagate ILM peeling has been shown to result in a heightened DONFL appearance as compared to conventional forceps peeling.8 It has recently been proposed that all these changes could be given the umbrella term “peel induced maculopathy”.9 The exact relationship between surgical trauma and the extent of any inner retinal thinning and RNFL damage remains uncertain at present.
It has been suggested that focal areas of inner retinal thinning could be used as a measure of surgical competence although the precise association between instrument trauma and focal retinal thinning is unclear.10 The determinants of overall retinal nerve fibre layer loss, including the association with DONFL and instrument trauma are also ill defined.
Using prospectively collected data, we sought to investigate these relationships as well as their association with central visual fields after macular hole surgery.
Method
This was a retrospective analysis of data that had been previously prospectively collected during a feasibility randomised controlled trial (RCT) using two different types of ILM peeling forceps, namely the Alcon Grieshaber FINESSE SHARKSKIN ILM and REVOLUTION DSP ILM forceps (Alcon Grieshaber, Schaffhausen, Switzerland). In that study, there were no significant differences between any of the retinal nerve fibre layer nor inner retinal changes evaluated between the two forceps types.8
Surgeries had been performed by 4 experienced fellowship-trained vitreoretinal surgeons in 3 large ophthalmology centres in the United Kingdom. All surgeons had independently performed over 100 surgeries for iFTMH with ILM peeling prior to study start and hence could be regarded as experienced “pinch peelers”. All surgeons were right-handed. This study conformed to the Declaration of Helsinki and UK multicentre ethical approval was obtained (North of Scotland Research Ethics Committee reference 19/NS/0124) for the original RCT and no further ethical review was required for this post hoc analysis. After a comprehensive discussion, all patients signed a written consent form.
Inclusion and Exclusion Criteria
Patients had been included in the original RCT if they were over 50 years old and having surgery for an iFTMH of any size and less than 12-month (12-m) duration. Patients had been excluded when ILM peeling was not planned, or in presence of any of the following conditions: secondary FTMH, previously vitrectomized eyes, pre-existing significant macular disease (early AMD allowed), glaucoma, optic nerve disease, any diabetic retinopathy, any intraocular inflammation, myopia > -6 dioptres or axial length > 26 mm, amblyopia, and conditions affecting ability to perform visual fields or imaging. Patients with any ERM causing retinal surface irregularity or with visible bridging between retinal adhesion points were excluded.
A total of 43 eyes of 43 patients of the original 65 included in the RCT were included in this analysis. The 22 patients not included had missing surgical videos due to inadvertent data loss at one of the hospitals. All surgeons performed 11 cases except one surgeon who performed 10.
Surgical Procedure
Surgery was standardised with 25-gauge transconjunctival pars plana vitrectomy with posterior hyaloid face separation, if not pre-existing. All phakic patients underwent combined phacoemulsification and posterior chamber intraocular lens implantation irrespective of the lens state. After core and peripheral vitrectomy, ILM staining was performed with heavy brilliant blue G 0.025% for 30-second contact time. All surgeons used pinch peeling as their preferred ILM peeling initiation technique and the ILM peeling was extended up to a radius of 1.5-disc diameters. After air-fluid exchange, 16% C2F6 was used as tamponade and patients were instructed to position face-down for 3 days then non supine for 7 days. All surgeries were digitally recorded.
Surgical Video Evaluation
Surgical videos were graded by two independent observers, with arbitration by a third in cases of disagreement. Position and number of ILM primary and secondary pick up points (PUPs) or attempts, any retinal haemorrhage, retinal trauma and ILM peeling size and duration were recorded. The position of PUPs on the ETDRS and 8 by 8 OCT grid overlays were recorded.
Follow Up Data
Patients’ visual acuity (VA), visual field and imaging data at the baseline, 3 week and 6-month visits were analysed. Visual acuity was assessed on a 4-metre logMAR chart after a protocol refraction. Central Visual fields (Humphrey Field Analyzer Central 10–2 Swedish Interactive Threshold Algorithm-Standard test, Carl Zeiss Meditec, San Leandro, CA) were performed preoperatively and 6 months postoperatively. The test was performed in both eyes with the fellow eye first and repeated if they failed to achieve a pre-defined reliability criterion of <15% false positives. The change in mean decibels between the two scans was recorded.
Imaging Protocol and Analysis
All eyes were imaged with the Heidelberg Spectralis spectral-domain OCT device (Heidelberg Engineering, Heidelberg, Germany). Posterior pole scan, 30°x25°, 240 sections (30 μm), high speed, ART 20 and a peri-papillary pre-set RNFL scan ART 100 were acquired preoperatively and at each follow-up (FU) visit. In addition, a 5°x15°, 49 sections (30 μm), high speed, ART 20 was performed preoperatively and a separate high-definition infrared (IR) image with high ART (25) preoperatively to allow precise hole measurements. MLD was defined as the horizontal minimum hole diameter in the approximate mid-zone of the hole away from any operculum, in the OCT slice with the widest dimensions.11 Blue fundus autofluorescent (FAF) images were taken at baseline, 3 weeks postoperatively and 6 months. Images were exported anonymised for masked grading at a certified image grading centre (NetwORC UK, Central Angiographic Resource Facility, Queen’s University, Belfast, Northern Ireland).
Image Grading
The 3-week IR images were graded for the presence and number of haemorrhages and dark RNFL lesions with corresponding RNFL thickening on SD-OCT representing SANFL lesions (Figure 1). The FAF images were graded for the presence of areas of change from baseline using the 3-week and 6-month images and correspondence of SANFL lesions at 3 weeks.
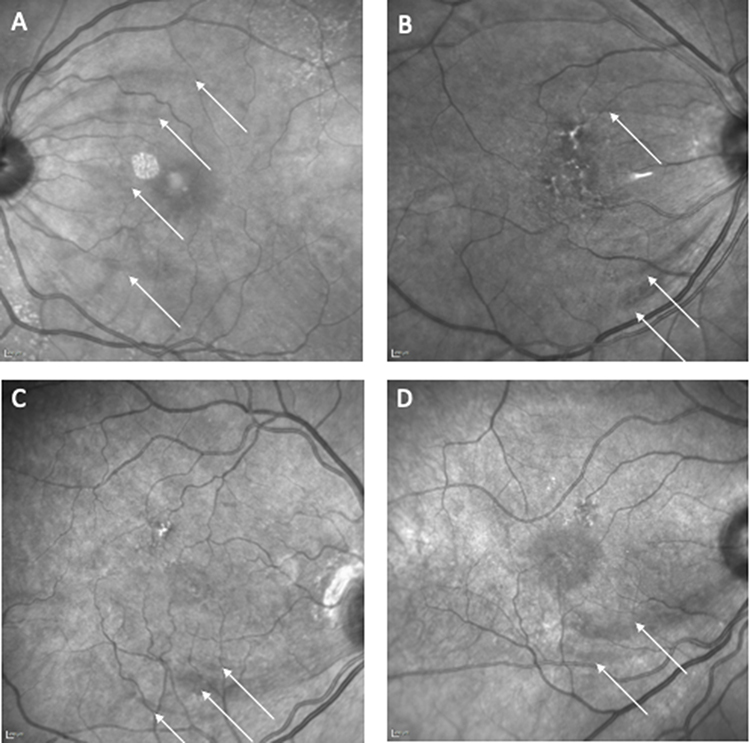 |
Figure 1 Four examples (A–D) of sub acute nerve fibre swelling lesions (SANFL) at 3 weeks postoperatively on infra-red (IR) imaging, highlighted by white arrows. All occurred at surgical pick-up points. Note: On Figures 1B–D areas of retinal pigment epithelial change are visible that pre-dated the surgery. |
On the 6-month images using the Heidelberg auto-segmentation algorithm, the RNFL thickness was recorded in the inner and outer retinal zones of a 1, 3, 6 mm ETDRS grid, as well as a custom Heidelberg generated 8 × 8 grid centred on the fovea. From the ETDRS grid, the change in the 8 inner and outer grid zones from baseline to 6 months was calculated. For the RNFL data from the 8 × 8 grid data, the central 4 squares encompassing the foveal area were excluded, meaning that 60 pre-defined grid positions were included in the analysis, totalling 2,580 squares. RNFL defects in these 60 grid positions were calculated after adjustment for the mean thickness in each square. A “defect” was defined as a value below 1.96 standard deviations below the mean using a normalised RNFL variable. Once the threshold was identified, for each patient the number of defect areas was calculated (Figure 2).
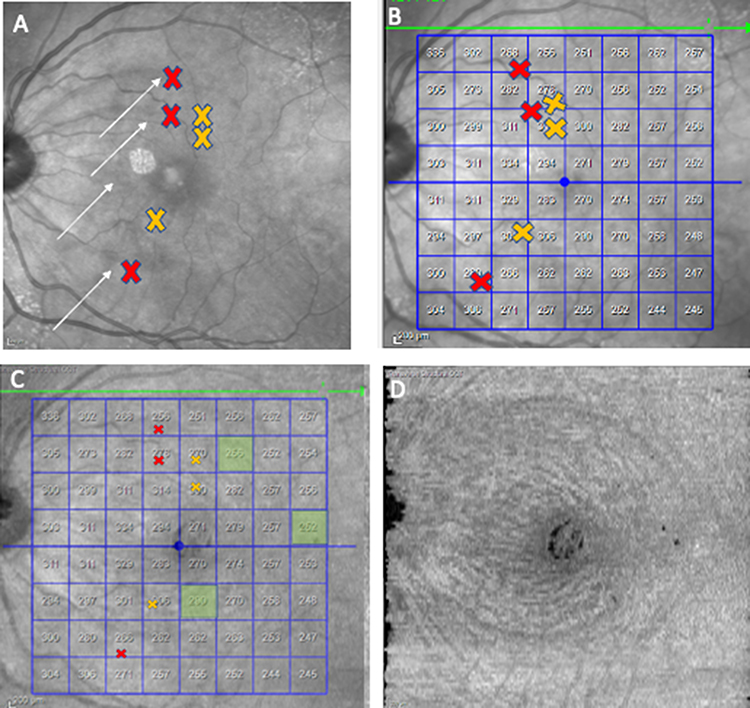 |
Figure 2 An example of a case with (A) Pick-up points (PUPs) (red cross marking PUP with hemorrhage and yellow cross PUP without hemorrhage) and SANFL lesions (white arrows) marked on the 3-week postoperative IR image. (B) PUPs shown on a 64-grid retinal thickness overlay with a default crossline (green arrow) (C) Position of 64 grid squares with a focal retinal nerve fibre layer (RNFL) defects identified at 6 months postoperatively (green shading) on SDOCT with a default crossline (green arrow) (D) Corresponding en-face segmented RNFL slab image. |
The ETDRS and 8 by 8 grids from the 6-month OCTs were exported and mapped to the surgical videos, allowing the position of all PUP changes to be recorded in terms of their position within the grids (Figure 3).
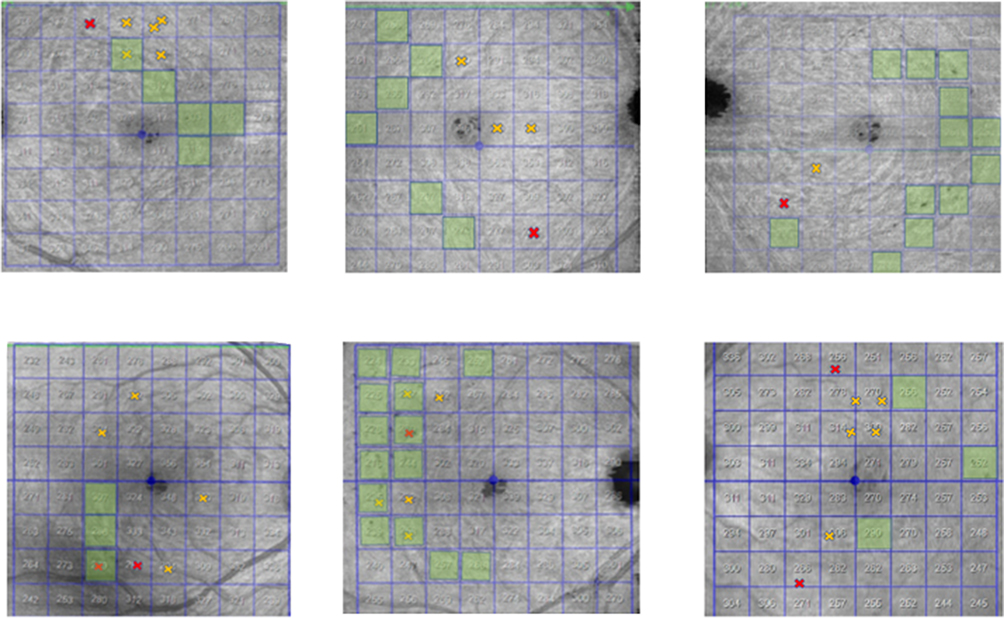 |
Figure 3 Six examples of eyes showing PUPs (red cross marking PUP with hemorrhage and yellow cross PUP without hemorrhage) and focal RNFL defects (green shading) identified at 6 months postoperatively on SDOCT. |
The peripapillary RNFL thickness was measured using the automated Heidelberg RNFL thickness algorithm and changes from baseline calculated.
All automatic segmentations were manually checked and adjusted by masked graders in case of gross segmentation errors were noted.
Finally, the severity of any associated DONFL appearance was calculated using the en-face OCT from the 6-month scans. An axial slab encompassing the inner surface of the ILM to outer border of the RNFL using the automated segmentation algorithm was selected. This en-face image was then exported as a TIFF file and imported into FIJI, a biological-image analysis program.12,13 The images were converted to 8-bit images and had their scale set using the marker on each image. The ILM surgical peel outline was traced using the selection brush tool to calculate the area of the ILM peeling. To represent the natural depression of the fovea, a circle of diameter 1000 µm centred at the foveal centre was placed. The area within this circle and outside of the ILM surgical peel was cleared. The automatic thresholding algorithm “MaxEntropy”13 was then applied to the remaining area by using the XOR function from the region of interest manager; this selected the DONFL “dimples”. The ImageJ analyse particles function was used to obtain measurements for the number of distinct DONFL dimples which were normalised by peel size for analysis (Figure 4).
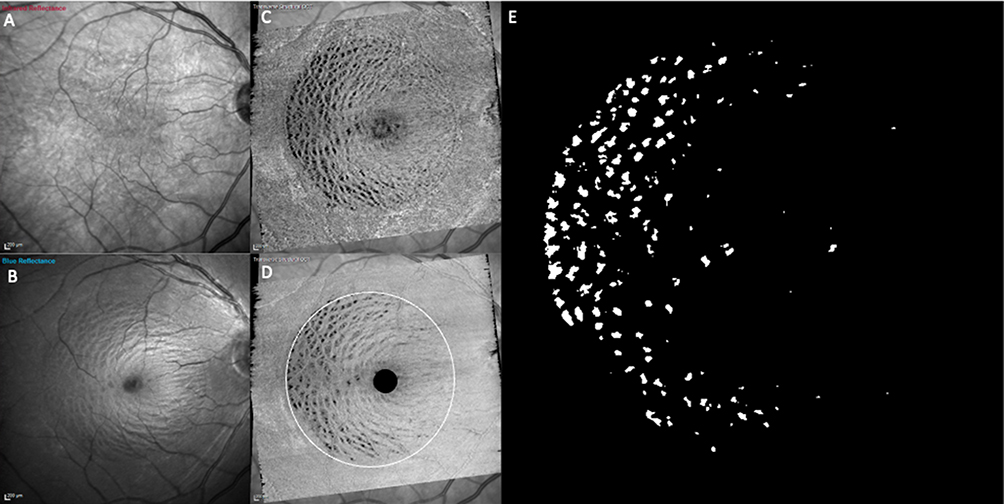 |
Figure 4 Methodology to measure the extent of a dissociated optic nerve fibre layer (DONFL) appearance. (A) shows infra-red image of 6-month postoperative SLO image. (B) Corresponding blue reflectance image. (C) Axial slab of en-face SDOCT encompassing the inner surface of the ILM to outer border of the RNFL layer. (D) The images were converted to an 8-bit image, the edges of the peeled area were demarcated and a mask applied to the central fovea (E) After applying the automatic thresholding algorithm “MaxEntropy” to the image, the dimples are seen as bright areas, which were then counted. |
Statistical Analysis
Descriptive statistics are presented for baseline and postoperative variables. Associations between several key study parameters were examined using Pearson correlation.
The association between PUP locations and the presence of an RNFL defect using the 8 × 8 grid data was assessed using the chi-square test, as was the association between these two factors for PUPs with or without associated hemorrhages and/or SANFL.
Factors associated with global peripapillary NFL loss were examined using linear regression. To limit the number of variables in this stage of the analysis, only those showing some evidence of an association with the outcomes in the univariable analyses (p < 0.2) were included in this analysis. A backwards selection procedure was used to retain only the significant variables in the final model.
Results
The baseline characteristics of the 43 patients analysed are shown in Table 1. The mean age was 69 ± 5.9 years, and 74% of the patients were female. All were of white British ethnicity. The median duration of symptoms was 6 months and the mean minimum linear diameter was 474 microns. Thirty-five (82%) had vitreopapillary attachment at the time of surgery.
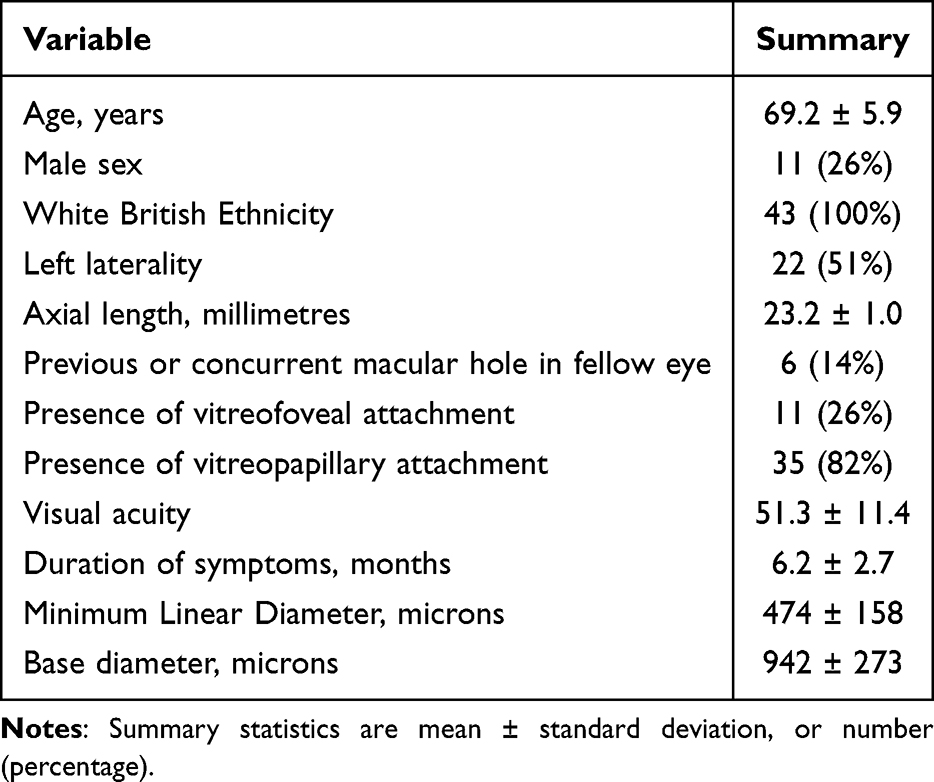 |
Table 1 Baseline Variables |
The median peeling time was 263 seconds (IQR: 202 to 377) and the mean ILM peeled area was 27 mm2 (SD 7.1). The median number of SANFL lesions identified by case was 1 (IQR: 0 to 2) with a mean of 5.6 PUPs in total per case (see Table 2).
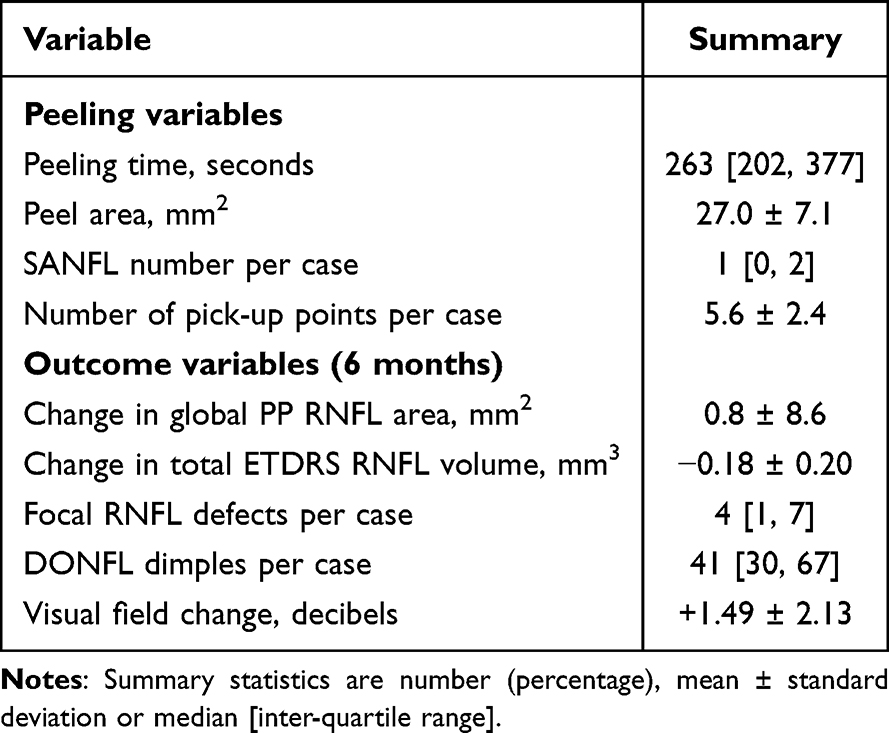 |
Table 2 Summaries of Peeling and Outcome Variables |
Intraocular pressure was recorded at below 22 mmHg in all patients at all 3 visits pre and postoperatively.
There were no significant differences in the number of PUPS, SANFL occurrence, haemorrhages, number of focal RNFL defects nor global RNFL loss and the type of forceps used. Similarly, none of the peel and outcome parameters varied significantly between the 4 surgeons.
Changes in RNFL Measures and Visual Fields
Overall, there was a significant RNFL reduction from a mean total volume of 1.12 to 0.93 mm3 in the area enclosed by a standard ETDRS grid (P < 0.001). There were significant reductions in all sectors other than the outer temporal and inferior sectors. (Supplementary table 1).
There was no overall significant change in the peri-papillary (PP) RNFL. The mean change in the average global PP RNFL measurements was a gain of 0.8 microns (95% confidence limits −2 to +3.5 microns) from 95.2 to 96.0 microns (p = 0.58), with no significant changes in any sector, but the greatest reduction in the inferior temporal sector of 1 micron. (Supplementary table 2). However, 17 patients had a loss in global PP RNFL, 3 patients had a loss of 10% or more and 9 a loss of 5% or higher.
There was a mean improvement of +1.49 decibels (standard deviation (SD) 2.13) in the central visual field. The mean change was +1.4 (SD 2.21) decibels in patients with phacovitrectromy as compared to +1.7 (SD 2.23) decibels in patients without phacovitrectromy. (p = 0.73).
PUPs Were Associated with Hemorrhages and SANFL Lesions in Approximately 20% of Cases Overall
There was a total of 213 forceps PUPs, 43 primary and 170 secondary. Of these PUPs, 37 (17%) were associated with a haemorrhage and 43 (20%) an SANFL lesion. (See supplementary table 3) There was a significant relationship between a hemorrhage at a pick-up point and the occurrence of an SANFL lesion (P < 0.001), in similar proportions between primary and secondary PUPs. We did not observe any pick-up points changes associated with changes in the RPE or outer retina on SD-OCT or FAF either at 3 weeks or 6 months.
PUPs, Particularly Ones Associated with SANFL Lesions and Haemorrhages Were Associated with Focal RNFL Defects, but Most Defects Were Not Associated with PUPs
We analysed the association between the location of RNFL defects and PUP location on an 8 by 8 grid distribution as well as the occurrence of a retinal haemorrhage or SANFL lesion associated with a PUP within the square where the pick-up occurred. The results suggested a significant association between PUPs associated with haemorrhage or SANFL and the presence of an RNFL defect. A quarter (26%) of locations with a haemorrhagic PUP had a defect, compared to only 13% of locations with a non-haemorrhagic PUP. However, although defects were more common when there was a PUP, the majority (74%) of locations with fundoscopically visible PUP trauma identified had no defect. Similarly, most focal RNFL defects were in areas without a PUP (Table 3). Of the 192 focal RNFL defects observed, only 31 (16%) were associated with a PUP.
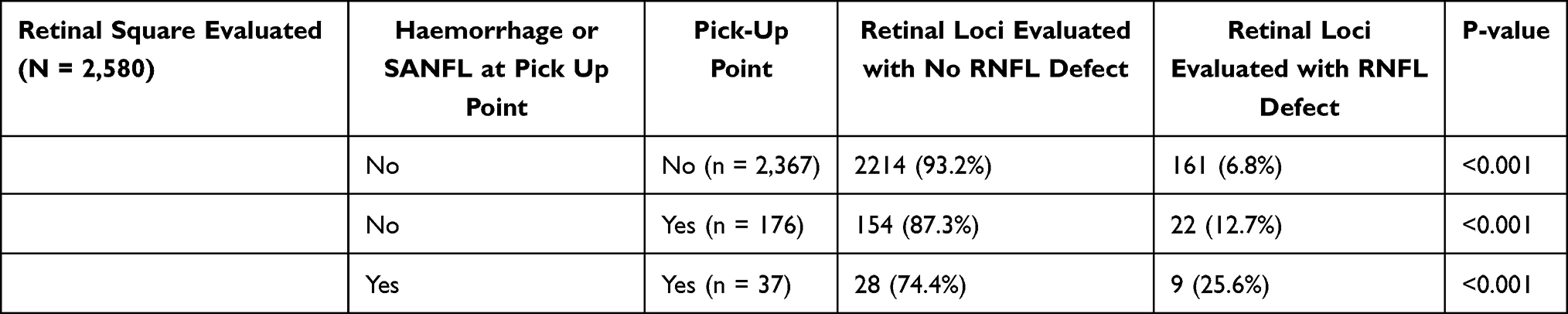 |
Table 3 Pick-Up Point Locations and in Peripapillary (PP) RNFL Defects |
RNFL Defects Were Most Common in the Outer Temporal Sector but the Inner Inferior Sector Has the Strongest Association for RNFL Defects Associated with PUPs
The location of RNFL defects in each of the 8 eccentric ETDRS sectors was analysed as well as their association with PUPs. This was performed using the individual 8 by 8 grid squares that occurred within each ETDRS sector. The outer temporal sector had the most retinal defects, the majority of which were not associated with a PUP (Table 4) There was no statistically significant association between PUPs and defects for most of the locations. The exception was for the inner inferior sector only. In this sector, 29% of the squares had a defect associated with a PUP whilst only 1% of the squares had a defect where there was no PUP.
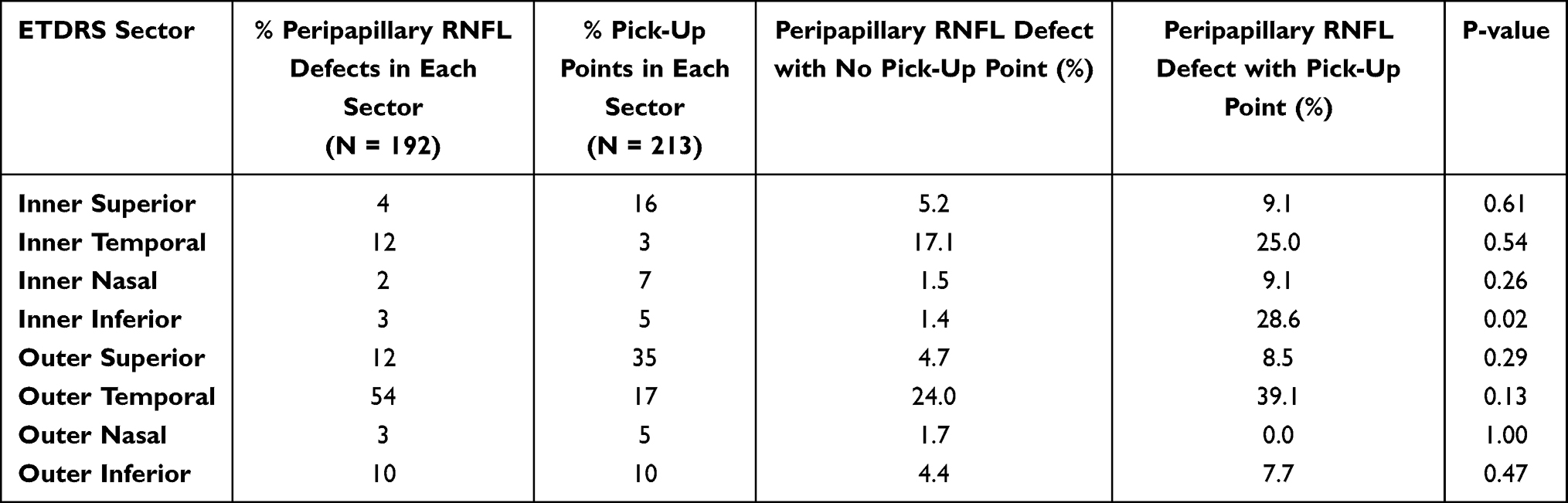 |
Table 4 Pick-Up Point Locations and Defects by ETDRS Sectors |
Inner Zone and Temporal Zone Retinal Pick-Up Points and Number of DONFL Dimples Were Associated with Peripapillary RNFL Loss
A multivariate linear regression analysis was conducted with global PP RNFL as the outcome of interest, incorporating surgeon and forceps type as variables. Supplementary Table 4 presents the univariate analysis, while Table 5 summarizes the multivariate results.
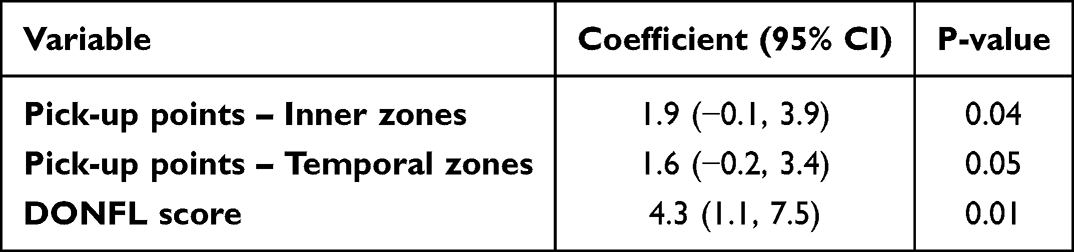 |
Table 5 Multivariable Associations with in Peripapillary (PP) RNFL Loss |
For this analysis, the PUPs were categorized using the ETDRS grid and grouped into Outer (all four outer zones), Inner (all four inner zones), Temporal (two temporal zones), and Superior (two superior zones), among others. The findings indicate that a higher DONFL score was significantly correlated with PP RNFL loss. Specifically, a 10-unit increase in the DONFL score corresponded to a 4.3-micron increase in RNFL loss. Additionally, the number of pick-up points in the inner and temporal zones was also associated with greater loss, with each additional inner pick-up point leading to a 1.9-micron increase and each additional temporal pick-up point contributing to a 1.6-micron increase in RNFL loss. The R squared of the model was 0.40, with the DONFL changes contributing 70% of the total.
Discussion
In this study, we were able to make several important and previously unreported observations regarding the relationship between focal instrument trauma and features which have been described with peel associated maculopathy.
That forceps can cause focal RNFL trauma is undisputed but how much RNFL loss is unrelated to instrument trauma has not previously been known. We studied cases with iFTMH to avoid the confounding effects of epiretinal membrane which can variably alter the adhesion of ILM to the underlying retina and also used a standardised surgical protocol. We show that SANFL lesions, as seen on postoperative scans, were all attributable to forceps grasp sites. Whilst these lesions were more likely to be associated with focal RNFL defects than PUPs without these lesions, temporal and inner ETDRS zone PUPs were more commonly associated with RNFL loss. Importantly, however, we also show that over 80% of RNFL defects do not occur at PUPs. Loss of the global PP RNFL was associated with the number of inner and temporal area PUPs, but more strongly with the extent of a DONFL appearance. Our studies suggest that PUP trauma is not responsible for most of the focal RNFL loss seen after surgery, and apparently atraumatic surgery can still have several areas of focal RNFL loss. Focal areas of retinal thinning have been suggested as a possible discriminator of surgical performance based on PUP trauma, but our finding that most areas occur at sites unrelated to PUPs puts the validity of this in doubt.10 Importantly, it also means that other surgical variables should be considered to reduce surgically related RNFL loss.
Several authors have described SANFL lesions and examined their association with PUPs. Diaz et al, reported arcuate striations in the early post-operative period following ILM peeling that followed the course of axonal pathways to the optic nerve and that corresponded to focal SANFL at forceps PUPs.14 Similarly, we found that all identified SANFL lesions could be attributed to a PUP. Balducci et al reported that SANFL lesions occurred in all ETDRS sectors except the temporal ones, while RNFL thinning was greatest in the temporal macula.15 Although we found that focal RNFL defects were more common in areas of SANFL, the majority of RNFL defects we observed were unrelated to PUPs and SANFL, and SANFL lesions were not correlated with PP RNFL thinning. SANFL lesions are clearly related to PUPs but do not fully explain the temporal RNFL thinning observed after ILM peeling nor most focal RNFL defects.
At least some of the temporal RNFL thickness reduction after ILM peeling in patients with iFTMH has been ascribed to the retinal redistribution that occurs following hole closure with thinning of the temporal retina and thickening of the nasal retina.16 The temporal macula being thinner than the other zones may also make it more vulnerable to RNFL defects than other areas.17 Interestingly, a number of other retinal conditions predominantly target the temporal macula including macular telangiectasia and ischaemic retinopathies perhaps suggesting common pathogenic factors.
Some RNFL damage is likely due to instrument trauma, and we were able to show that instrument trauma in the inner and temporal ETDRS zones was more commonly associated with RNFL defects than in other areas. However, it is evident that most RNFL thinning in these areas is not related to instrument trauma and may be related to other factors.
We also found that a higher DONFL score was associated with a greater PP RNFL loss. The precise cause of DONFL is uncertain but it is thought to relate to Muller cell trauma with end feet avulsion as the ILM is peeled off from their end feet. To concur with this, the severity of DONFL has been related to the amount of Muller cell debris found on peeled ILM on electron microscopy.18 Its association with RNFL loss has been disputed. The depressions observed may mainly represent volume loss in the ganglion cell layer secondary to Muller cell loss. The RNFL is thin and local changes in shape of the inner retinal surface can confound its measurement. To avoid this problem, we used loss in the PP RNFL as the outcome in a multivariate analysis and found a clear association between the extent of DONFL with PP RNFL loss, independent of the associations we found with PUPs. Several factors have been related to DONFL severity including dye type and the presence of ERM.19 The cleavage plane of ILM from the retina is reportedly deeper in the presence of ERM and we therefore chose to study ILM peeling in the absence of ERM which could have confounded previous studies. Modelling studies have suggested that the angle ERM are peeled at could influence their cleavage plane from the retina.7,20 Indeed, a prospective study of 36 patients with ERM suggested that peeling under perfluorocarbon liquids could reduce the occurrence of DONFL by altering the peeling angle, and also reducing the number of PUPs required.20
Despite the recorded RNFL loss, it did not adversely affect visual outcomes in the 6-month time frame we studied. We found no correlation between central visual field improvement and any of the anatomical changes we studied, concurring with previous studies using microperimetry, although others have found microscotomata associated with both DONFL and grasp sites.21–25 Other retrospective studies have also found an association between central visual field loss and RNFL thinning in patients with iERM. Some have been confounded by field loss secondary to indocyanine green (ICG) whilst other have not.26–28 Similar to our study, Tsuchiya et al, in a retrospective study of 45 patients with iERM and iFTMH, did not find any deterioration in the 10° central visual fields in non-glaucomatous eyes undergoing ILM peeling for ERM or MH and found no association between DONFL and visual field sensitivity despite showing inner retinal thinning.29 They did however find field loss in patients with glaucoma, which was excluded in our study. It has long been known that considerable RNFL loss can occur prior to clinically detectable field loss.30 The fact that we did not find field loss corresponding to the RNFL loss observed does not negate its significance for future functional deficits.
We acknowledge that our study has several limitations. We did not assess microperimetry that should be considered in future studies to focally investigate the relationship between iatrogenic damage and functional loss. Moreover, visual fields results may have been influenced by the concomitant cataract surgery. Our study only examined patients up to 6 months postoperatively and conducting longer term follow up might provide valuable insights into the reorganization of retinal layers following iatrogenic damage. Only 4 surgeons and 43 surgeries were included, and it is possible other surgeons and cases may have shown different results. Other studies have used intraoperative OCT to document instrument trauma and have demonstrated effects on retinal microarchitecture during surgical manoeuvres in a large proportion of cases, and this technique may have improved the interpretation of our results.31,32
In conclusion, whilst forceps pick-up points in the temporal and inner retinal zones were more commonly associated with focal RNFL defects, most pick-up points were not responsible for the majority of focal RNFL defects observed after ILM peeling. This observation and the finding that the extent of a DONFL appearance was associated with the extent of peripapillary RNFL loss suggests that some RNFL loss be related solely to the act of ILM avulsion from the retinal surface. Reducing the RNFL loss associated with peeling may be possible by surgical modifications including dye type, pressure exerted on the retina during peeling and the angle the ILM is peeled at with respect to the retinal surface which require further study. We advise caution before using inner retinal trauma as a measure of surgical performance, without further understanding of the mechanisms.
Funding
The study was funded as an IIS (IIT#38075469) by Alcon, with payment to Newcastle University.
Disclosure
D Steel discloses that his institution has received research grants from Alcon, DORC, Bayer, BVI, Roche and Boehringer-Ingelheim and he has acted as a consultant to Alcon, BVI, DORC, Roche, Alimera, Complement therapeutics, Sitala and Gyroscope for projects unrelated the subject matter in this manuscript. T Peto discloses research grants from Boehringen-Inhelheim, Novartis, OPTOS paid to her Institution and she has acted as consultant to Apellis, Abbvie, Bayer, Roche, Novartis, OPTOS, Zeiss and Heidelberg for projects unrelated to the subject matter in this manuscript. A Muldrew reports grants from QUB, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Spiteri Cornish K, Lois N, Scott NW, et al. Vitrectomy with internal limiting membrane peeling versus no peeling for idiopathic full-thickness macular hole. Ophthalmology. 2014;121(3):649–12. doi:10.1016/j.ophtha.2013.10.020
2. Chatziralli IP, Theodossiadis PG, Steel DHW. INTERNAL LIMITING MEMBRANE PEELING IN MACULAR HOLE SURGERY; WHY, WHEN, AND HOW? Retina. 2018;38(5):870–882. doi:10.1097/IAE.0000000000001959
3. Pichi F, Lembo A, Morara M, et al. Early and late inner retinal changes after inner limiting membrane peeling. Int Ophthalmol. 2014;34(2):437–446. doi:10.1007/s10792-013-9831-6
4. Tadayoni R. Dissociated optic nerve fiber layer appearance of the fundus after idiopathic epiretinal membrane removal. Ophthalmology. 2001;108(12):2279–2283. doi:10.1016/S0161-6420(01)00856-9
5. Clark A, Balducci N, Pichi F, et al. Swelling of the arcuate nerve fiber layer after internal limiting membrane peeling. Retina. 2012;32(8):1608–1613. doi:10.1097/IAE.0b013e3182437e86
6. Charles S. Techniques and tools for dissection of epiretinal membranes. Graefe’s Arch Clin Exp Ophthalmol. 2003;241(5):347–352. doi:10.1007/s00417-003-0624-x
7. Dogramaci M, Williamson TH. Dynamics of epiretinal membrane removal off the retinal surface: a computer simulation project. Br J Ophthalmol. 2013;97(9):1202–1207. doi:10.1136/bjophthalmol-2013-303598
8. Ferrara M, Rivera-Real A, Hillier RJ, et al. A randomised controlled trial evaluating internal limiting membrane peeling forceps in macular hole surgery. Graefe’s Arch Clin Exp Ophthalmol. 2023;261(6):1553–1562. doi:10.1007/s00417-022-05932-y
9. Thomas AS, Thomas MK, Davis EC, et al. A comparison of peel-induced maculopathy following ilm peeling using a microvacuum pick versus forceps. Ophthalmic Surg Lasers Imaging Retina. 2023;54(1):37–42. doi:10.3928/23258160-20221216-01
10. Alberti M, Jacobsen MF, Hermann MN, et al. Quantifying surgical skill in macular surgery. Acta Ophthalmol. 2022;100(4):440–446. doi:10.1111/aos.15023
11. Duker JS, Kaiser PK, Binder S, et al. The international vitreomacular traction study group classification of vitreomacular adhesion, traction, and macular hole. Ophthalmology. 2013;120(12):2611–2619. doi:10.1016/j.ophtha.2013.07.042
12. Schindelin J, Arganda-Carreras I, Frise E, et al. Fiji: an open-source platform for biological-image analysis. Nat Methods. 2012;9(7):676–682. doi:10.1038/nmeth.2019
13. Kapur JN, Sahoo PK, Wong AKC. A new method for gray-level picture thresholding using the entropy of the histogram. Computer Vision Graphics Image Process. 1985;29(3):273–285. doi:10.1016/0734-189X(85)90125-2
14. Diaz RI, Randolph JC, Sigler EJ, Calzada JI. Intraoperative grasp site correlation with morphologic changes in retinal nerve fiber layer after internal limiting membrane peeling. Ophthalmic Surg Lasers Imaging Retina. 2014;45(1):45–49. doi:10.3928/23258160-20131220-06
15. Balducci N, Morara M, Veronese C, Torrazza C, Pichi F, Ciardella AP. Retinal nerve fiber layer thickness modification after internal limiting membrane peeling. Retina. 2014;34(4):655–663. doi:10.1097/IAE.0000000000000004
16. Ishida M, Ichikawa Y, Higashida R, Tsutsumi Y, Ishikawa A, Imamura Y. Retinal displacement toward optic disc after internal limiting membrane peeling for idiopathic macular hole. Am J Ophthalmol. 2014;157(5):971–977. doi:10.1016/j.ajo.2014.01.026
17. Ooto S, Hangai M, Tomidokoro A, et al. Effects of age, sex, and axial length on the three-dimensional profile of normal macular layer structures. Invest Ophthalmol Vis Sci. 2011;52(12):8769–8779. doi:10.1167/iovs.11-8388
18. Steel DHW, Dinah C, White K, Avery PJ. The relationship between a dissociated optic nerve fibre layer appearance after macular hole surgery and M uller cell debris on peeled internal limiting membrane. Acta Ophthalmol. 2017;95(2):153–157. doi:10.1111/aos.13195
19. Kenawy N, Wong D, Stappler T, et al. Does the presence of an epiretinal membrane alter the cleavage plane during internal limiting membrane peeling? Ophthalmology. 2010;117(2):320–3.e1. doi:10.1016/j.ophtha.2009.07.024
20. Caporossi T, Picardi SM, Gambini G, et al. Dynamics of epiretinal membrane peeling under perfluorocarbon liquid evaluated by intraoperative OCT. Life. 2023;13(2):253. doi:10.3390/life13020253
21. Tadayoni R, Svorenova I, Erginay A, Gaudric A, Massin P. Decreased retinal sensitivity after internal limiting membrane peeling for macular hole surgery. Br J Ophthalmol. 2012;96(12):1513–1516. doi:10.1136/bjophthalmol-2012-302035
22. Mayer WJ, Fazekas C, Schumann R, et al. Functional and morphological correlations before and after video-documented 23-gauge pars plana vitrectomy with membrane and ilm peeling in patients with macular pucker. J Ophthalmol. 2015;2015:297239. doi:10.1155/2015/297239
23. Blautain B, Glacet-Bernard A, Blanco-Garavito R, et al. Long-term follow-up of retinal sensitivity assessed by microperimetry in patients with internal limiting membrane peeling. Eur J Ophthalmol. 2022;32(1):539–545.
24. Imai H, Ohta K. Microperimetric determination of retinal sensitivity in areas of dissociated optic nerve fiber layer following internal limiting membrane peeling. Jpn J Ophthalmol. 2010;54(5):435–440. doi:10.1007/s10384-010-0839-4
25. Runkle AP, Srivastava SK, Yuan A, et al. Factors associated with development of dissociated optic nerve fiber layer appearance in the pioneer intraoperative optical coherence tomography study. RETINA. 2018;38(1):S103–S109. doi:10.1097/IAE.0000000000002017
26. Sato T, Yamauchi-Mori R, Yamamoto J, Hayashi K. Longitudinal change in retinal nerve fiber layer thickness and its association with central retinal sensitivity after epiretinal membrane surgery. Asia-Pacific J Ophthalmol. 2022;11(3):279–286.
27. von Jagow B, Höing A, Gandorfer A, et al. Functional outcome of indocyanine green-assisted macular surgery: 7-year follow-up. Retina. 2009;29(9):1249–1256. doi:10.1097/IAE.0b013e3181a91dd3
28. Akino K, Nagai N, Watanabe K, et al. Risk of newly developing visual field defect and neurodegeneration after pars plana vitrectomy for idiopathic epiretinal membrane. Br J Ophthalmol. 2021;105(12):1683–1687. doi:10.1136/bjophthalmol-2020-317478
29. Tsuchiya S, Higashide T, Sugiyama K, Vavvas DG. Visual field changes after vitrectomy with internal limiting membrane peeling for epiretinal membrane or macular hole in glaucomatous eyes. PLoS One. 2017;12(5):e0177526. doi:10.1371/journal.pone.0177526
30. Sommer A, Katz J, Quigley HA, et al. Clinically detectable nerve fiber atrophy precedes the onset of glaucomatous field loss. Arch Ophthalmol. 1991;109(1):77–83. doi:10.1001/archopht.1991.01080010079037
31. Uchida A, Srivastava SK, Ehlers JP. Analysis of retinal architectural changes using intraoperative OCT following surgical manipulations with membrane flex loop in the discover study. Invest Ophthalmol Vis Sci. 2017;58(9):3440–3444. doi:10.1167/iovs.17-21584
32. Maberley DAL, Beelen M, Smit J, et al. A comparison of robotic and manual surgery for internal limiting membrane peeling. Graefe’s Arch Clin Exp Ophthalmol. 2020;258(4):773–778. doi:10.1007/s00417-020-04613-y
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.