Back to Journals » Journal of Inflammation Research » Volume 18
The Association Between Phenotypic Age and Primary Loss of Response to Biologic Agent in Patients with Crohn’s Disease
Authors Chen X ![]() , Liu J, Zhang Y
, Liu J, Zhang Y ![]() , Wang Y, Chen X, Zhao Q
, Wang Y, Chen X, Zhao Q
Received 17 September 2025
Accepted for publication 31 October 2025
Published 7 November 2025 Volume 2025:18 Pages 15587—15595
DOI https://doi.org/10.2147/JIR.S565012
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Nadia Andrea Andreani
Xin Chen,1 Jingjing Liu,2,3 Yiping Zhang,2 Yu Wang,2 Xiao Chen,2 Qiufeng Zhao1
1Department of Radiology, Longhua Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, 200032, People’s Republic of China; 2Department of Radiology, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China; 3Funan County People’s Hospital, Funan Hospital Affiliated to Fuyang Normal University School of Medicine, Fuyang, 236399, People’s Republic of China
Correspondence: Xiao Chen, Department of Radiology, Affiliated Hospital of Nanjing University of Chinese Medicine, Nanjing, 210029, People’s Republic of China, Email [email protected] Qiufeng Zhao, Department of Radiology, Longhua Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, Shanghai, 200032, People’s Republic of China, Email [email protected]
Purpose: Loss of response (LOR) to biological agents is challenging in Crohn’s disease (CD) therapy. Identifying and predicting factors associated with therapeutic responses enables proactive intervention in high-risk LOR populations, such as adjusting therapeutic intensity or initiating second-line agents earlier, to avoid ineffective treatment and improve clinical outcomes. A few studies have also shown that biological age may be associated with treatment responses. This study aimed to show the association between phenotypic age, a type of biological age, and the primary loss of response to biological agents in patients with CD.
Methods: This retrospective study included 94 CD patients, with 81 followed-up at the eighth week and 76 at the twelfth week in our institution. LOR was defined as biochemical remission (fecal calprotectin level < 250 μg/g or a reduction of > 50% from baseline levels). The phenotypic age was calculated based on a series of clinical biomarkers. Multivariate regression analysis was used to determine the association between phenotypic age and the LOR. The receiver operating characteristic curve (ROC) was used to show the performance of biological age in predicting the 8-week and 12-week LOR.
Results: 33 patients had LOR at 8 weeks and 34 patients had LOR at 12 weeks. Patients with LOR had a higher phenotypic age and age gap than those with response (p < 0.001). Multivariable regression analyses further showed that phenotypic age and age gap were associated with LOR (8-week LOR, odds ratio (OR) = 1.18, 95% confidence interval (CI):1.07– 1.32 and OR = 0.84, 0.76– 0.94; 12-week LOR, OR = 1.12, 95% CI:1.02– 1.24 and OR = 0.89, 95% CI:0.81– 0.98). ROC curves showed that both phenotypic age and age gap had acceptable performance in predicting 8-week and 12-week LOR (the area under the curve (AUC) was 0.739– 0.784).
Conclusion: Phenotypic age is associated with LOR to biological agent in patients with CD, and has acceptable performance in predicting 8-week and 12-week LOR.
Keywords: Crohn’s disease, biologic agent, biological age, loss of response
Introduction
Crohn’s disease (CD) is a type of inflammatory bowel disease that affects any segment of the gastrointestinal tract. Crohn’s typically affects the terminal ileum and colon, and presents with symptoms such as abdominal pain and diarrhea. Although the incidence of CD is stabling in Europe and North America,1 the incidence in Africa, Asia, and South America countries has also been rising in recent years.1,2 The estimated prevalence of CD worldwide continued to arise.1 The global burden of inflammatory bowel disease poses significant challenges to healthcare systems.1
CD treatment is primarily based on the severity and extent of the disease. The goal is to induce and maintain remission, prevent complications, and improve patients’ quality of life.3 Pharmacological therapy remains the cornerstone of CD management, including aminosalicylates, corticosteroids, immunosuppressants, and biological agents.4 Commonly utilized biological therapy include anti-TNF medicines (such as infliximab and adalimumab), anti-integrin antibodies (vedolizumab), and anti-interleukin medications (ustekinumab, which targets IL-12 and IL-23).5 However, Primary or secondary loss of response to biological agents, particularly anti-TNF drugs, continues to pose a significant challenge in the management of CD. Therefore, optimizing biological agents and developing novel therapeutic strategies is essential for enhancing the prognosis and long-term outcomes of patients with CD.
Unfortunately, anti-TNF therapy is ineffective in patients with inflammatory bowel disease (IBD). The rate of primary nonresponse to anti-TNF therapy in CD varies between 13.4% and 63.1%, with certain patients failing to attain remission after one year of treatment.6 Studies have shown that the incidence of secondary loss of response (LOR) to anti-TNF agents in CD patients is also high, with rates reported to be as high as 47.9%.7 Therefore, identifying and predicting factors associated with therapeutic response is extremely important for the individualization and optimization of clinical treatment strategies.
Several markers have been used for the prediction of LOR in patients with CD, including genetic and non-genetic factors,8 such as genetic variants in TNF, TNFRSF1B, and NFkB genes, fecal calprotectin, Th17 signature cytokines and microbial markers. Biological age serves as a quantitative tool to estimate an individual’s rate of aging, reflecting their level of physiological decline relative to their chronological age.9 Biological age offers a more reliable assessment of aging than chronological age. An increasing number of studies have shown an association between biological age and health issues such as chronic respiratory diseases10 and COVID-19 severity.11 Severe inflammation may lead to high biological age.12 Few studies have shown that biological age may be associated with treatment response.13,14 We hypothesized that higher biological age may be associated with a more severe inflammatory state and altered response to biological agents. Therefore, this study aimed to show the association between biological age, defined by phenotypic age (PhenoAge), and primary loss of response to biological agents in patients with CD.
Methods
Patients
Patients with CD who received biological therapy (anti-TNF agents), at the Affiliated Hospital of Nanjing University of Chinese Medicine from July 2019 to December 2021 were retrospectively included. Inclusion criteria: CD patients diagnosed by clinical/endoscopic criteria; older than 18 years; receiving anti-TNF agents treatment. Exclusion criteria (1) Lack of baseline laboratory tests, and endoscopic pathological examinations at the start of biological therapy; (2) Patients lost to follow-up within 8 or 12 weeks after starting biological therapy (including those who did not continue treatment or continued treatment in other hospitals but with unclear follow-up data); (3) Patients with chronic kidney disease, chronic obstructive pulmonary disease, malignant tumors, congestive heart failure, neuromuscular diseases, limited activity, or long-term immobilization; (4) History of biological therapy; (5) Allergy to biological agents; (6) Patients in pregnancy and lactation. A total of 94 CD patients receiving anti-TNF agents was found. This retrospective study included 81 patients who were followed up at 8 weeks and 76 patients who were followed up at 12 weeks in the outpatient clinic. The flowchart of the study subjects can be seen in Figure 1. Ethics approval was obtained from the Affiliated Hospital of Nanjing University of Chinese Medicine (2020NL-KS11). This retrospective study was performed in accordance with the Declaration of Helsinki. The need for informed consent was waived by the Ethics Committee of the Affiliated Hospital of Nanjing University of Chinese Medicine due to the retrospective nature of the study. For this study, we were granted access to all data elements necessary to create the study cohort and perform the analyses, including demographics, diagnoses, laboratory data, procedures, medications. The study was reported adhered to RECORD guidelines (see Supplementary Material).
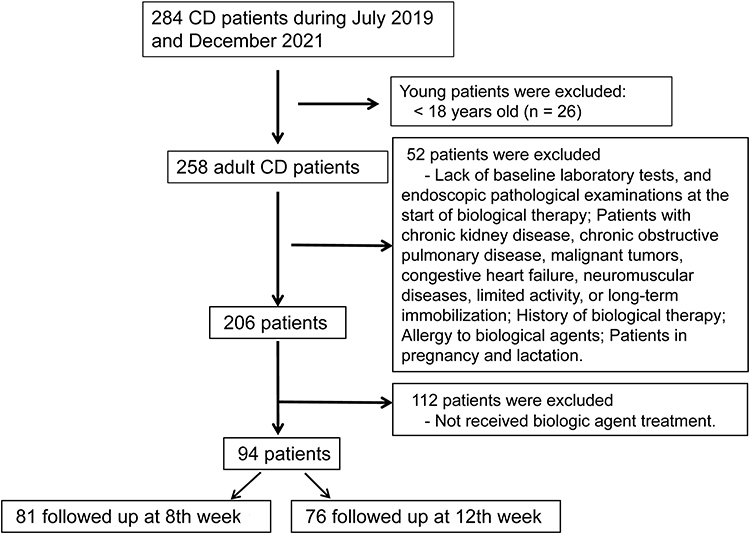 |
Figure 1 Patients inclusion flowchart. |
Data Collection and Definition of Loss to Response
Patient demographic information, use of biological agents, baseline laboratory examinations (complete blood count, biochemistry, C-reactive protein, coagulation function, fecal calprotectin (FC), and detection of granulomas by endoscopy were collected from the electronic medical record system. Fecal calprotectin levels were dynamically recorded from the beginning of the biological treatment to 8 and 12 weeks after treatment. The monthly location and presence of perianal lesions were evaluated by Computed Tomographic Enterography (CTE) or Magnetic Resonance Enterography (MRE). Biological agent response and non-response were defined based on biochemical remission at approximately 8–12 weeks of treatment (biochemical remission: fecal calprotectin < 250 μg/g or a reduction of > 50% from baseline levels; LOR: fecal calprotectin ≥ 250 μg/g or a reduction of ≤ 50% from baseline levels).
PhenoAge Calculation
PhenoAge was calculated based on a series of clinical biomarker data, including blood glucose, serum creatinine, serum albumin, C-reactive protein, lymphocyte percentage, mean corpuscular volume, red blood cell distribution width, alkaline phosphatase, and white blood cell count. The formula for calculating PhenoAge was as follows:15

Where xb is calculated by the formula:
Xb = −19.907 − 0.0336 × albumin + 0.0095 × creatinine + 0.1953 × glucose +0.0954 × ln (C-reactive protein) −0.012 × lymphocyte percentage +0.0268 × mean corpuscular volume + 0.3306 × erythrocyte distribution width +0.00188 × alkaline phosphatase + 0.0554 × leukocytes count + 0.0804 × chronological age.
After calculating PhenoAge, the age gap was obtained by subtracting the actual chronological age from PhenoAge.
Statistical Analyses
Statistical analyses were performed using SPSS software (version 24.0). Quantitative data are presented as mean ± standard deviation (SD). Categorical variables were expressed as numbers (percentages). Univariate and multivariate logistic regression analyses were used to examine the associations between quantitative data of PhenoAge, the age gap, and loss of response. Receiver operating characteristic (ROC) curve analysis was used to evaluate the predictive power of biological age and age gap for loss of response. Using PASS11 software, we estimated the sample size based on “Test for two means”, if the age gap was 3.0 year in response group and 5.0 years in LOR group, and standard deviation was 1.0 and 3.0 years, respectively, powder = 0.95, ɑ = 0.05, the estimated sample size was 35 in each group. Statistical significance was set at p < 0.05.
Results
Characteristic of Patients
Eighty one patients were followed up at 8 weeks and 76 patients were followed up at 12 weeks. The characteristics of the patients, based on their responses to biological agents, are shown in Table 1. Thirty three patients had LOR at 8 weeks and 34 patients had LOR at 12 weeks. Patients with LOR had low serum albumin levels (p < 0.05), red blood cell distribution width (p < 0.001), and mean corpuscular volume (p < 0.05). Consequently, patients with LOR had a higher PhenoAge and age gap than those with response (p < 0.001). The differences between the chronological age and phenotype in each patient are shown in Figure 2.
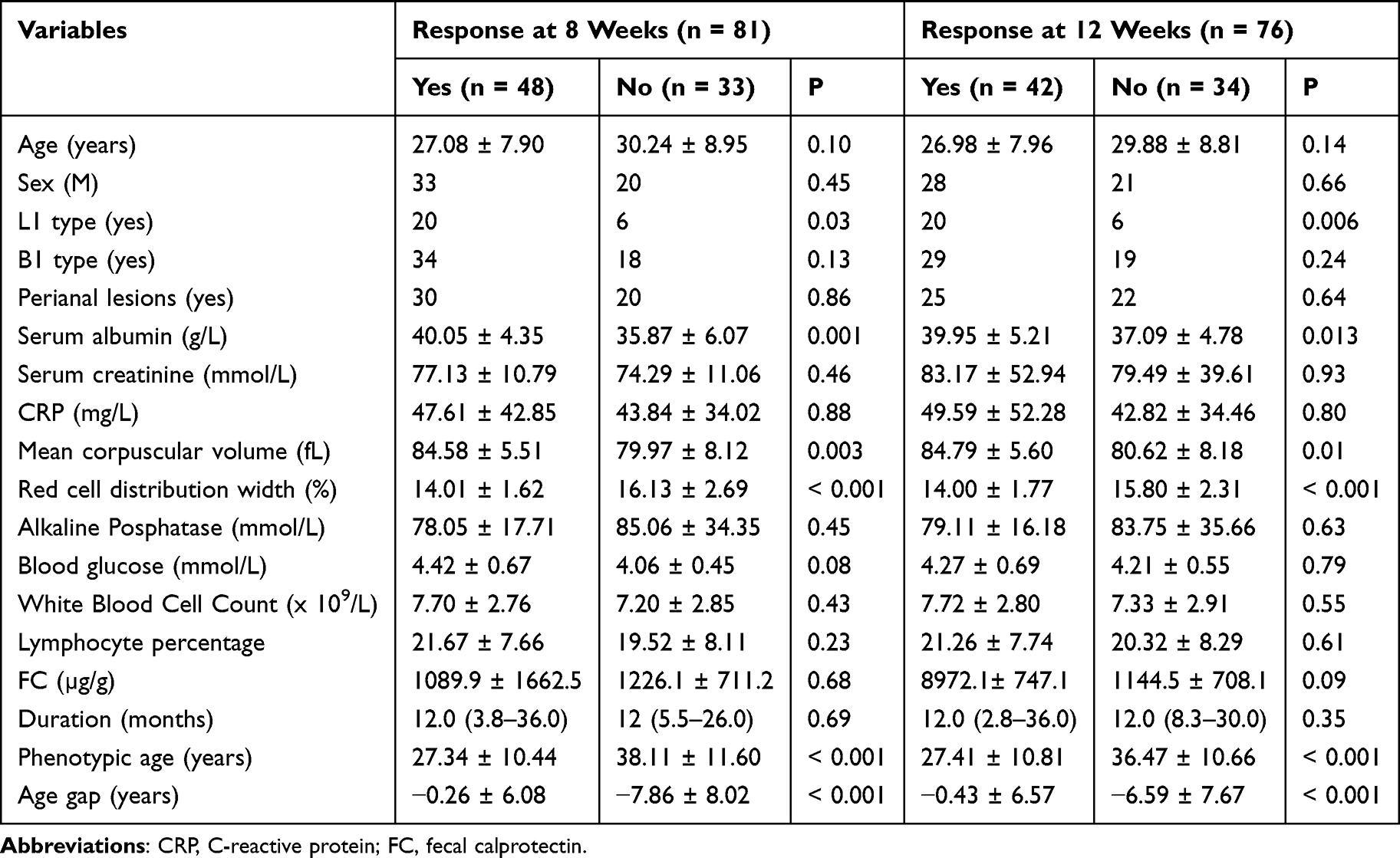 |
Table 1 Characteristic of Patients Based on Loss to Response |
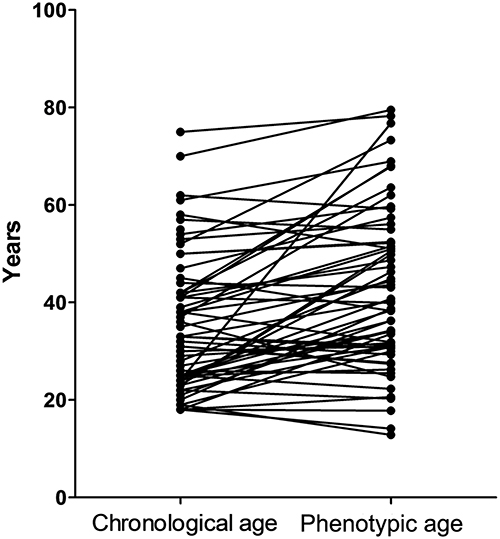 |
Figure 2 The differences between phenotypic age and chronological age. |
The Association Between Phenotypic Age/Age Gap and LOR
Subsequently, we investigated the association between PhenoAge/age gap and LOR using logistic regression analysis (Table 2). Univariable analysis showed that PhenoAge was associated with 8-week (odds ratio (OR) = 1.09, 95% CI: 1.04–1.15) and 12-week LOR (OR = 1.08, 1.03–1.14). Similar associations were observed for age gap (OR = 0.85, 95% CI:0.78–0.93; OR = 0.88, 0.81–0.95). Multivariable regression analyses further showed that PhenoAge and age gap were associated with LOR (for 8-week LOR, OR = 1.18, 95% CI:1.07–1.32 and OR = 0.84, 0.76–0.94; for 12-week LOR, OR = 1.12, 95% CI:1.02–1.24 and OR = 0.89, 95% CI:0.81–0.98) after controlling for sex, L1 type, perianal lesions, disease duration, baseline FC and chronological age.
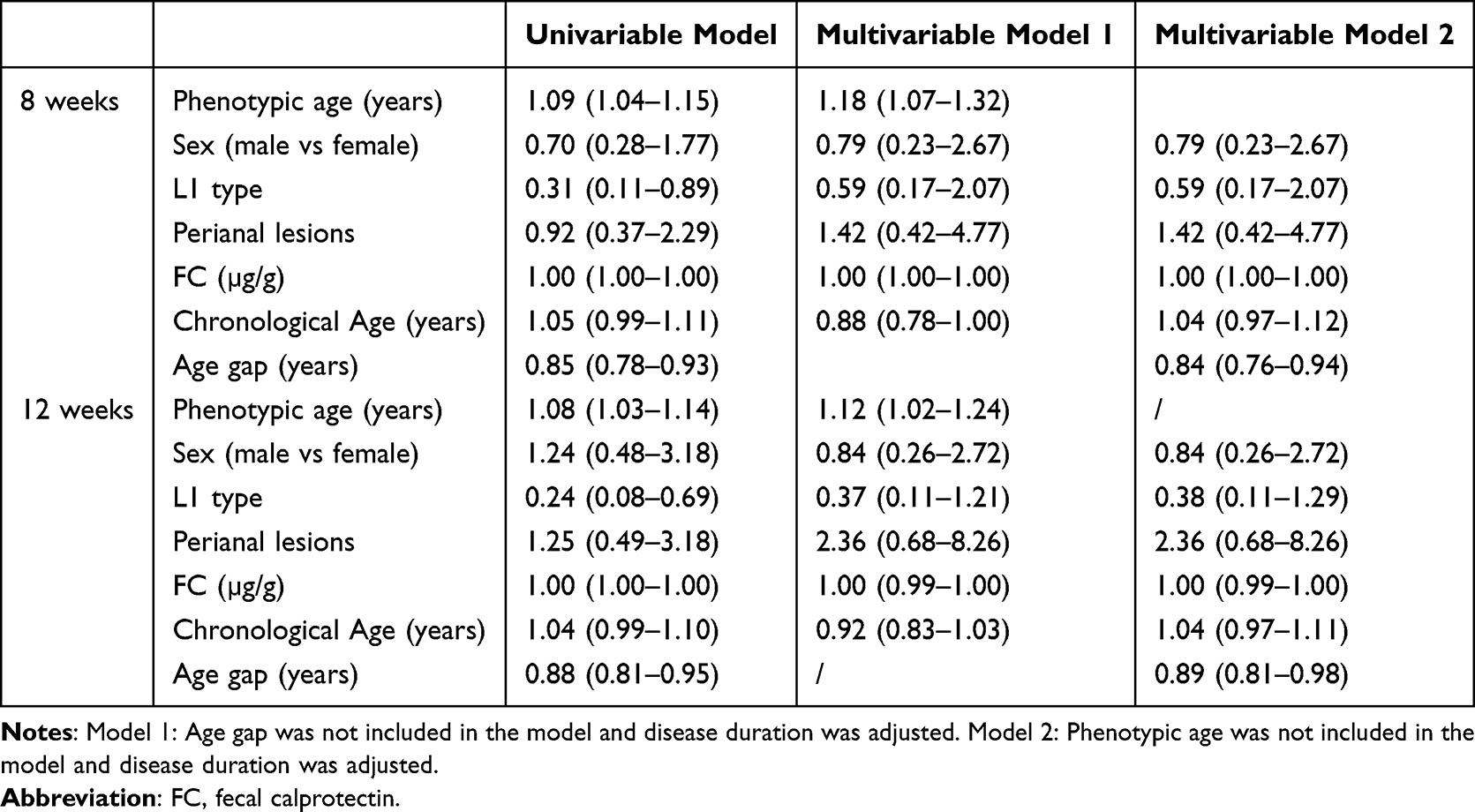 |
Table 2 Association Between Phenotype Age/Age Gap and Response at 8 and 12 Weeks |
Models to Predict LOR
Next, we observed the role of PhenoAge and the age gap in predicting LOR in patients with CD (Figure 3). ROC curves showed that both PhenoAge and age gap had acceptable performances in predicting 8-week and 12-week LOR. The area under the curve (AUC) was 0.774 (95% CI: 0.67–0.87) for PhenoAge and 0.784 (95% CI:0.68–0.87) for age gap in predicting 8-week LOR. The AUC was 0.742 (95% CI: 0.63–0.85) for PhenoAge and 0.739 (95% CI:0.63–0.83) for age gap in predicting 12-week LOR. PhenoAge showed better performance than chronological age in predict the 8 weeks LOR (AUC 0.774 vs 0.618, p < 0.001) and 12 weeks LOR (AUC 0.742 vs 0.616, p = 0.006) (Figure 4).
 |
Figure 3 Receiver operating characteristic curves of phenotypic age and age gap in predicting loss of response at the 8th week (A) and 12th week (B). |
 |
Figure 4 Receiver operating characteristic curves showed the performance of phenotypic age and chronological age in predicting loss of response at the 8th week (A) and 12th week (B). |
We also combined L1 type with phenotypic age or age gap to establish models. The AUC was 0.77 (95% CI: 0.67–0.87) for PhenoAge and 0.795 (95% CI:0.70–0.89) for age gap in predicting 8-week LOR. The AUC was 0.76 (95% CI: 0.65–0.87) for PhenoAge and 0.77 (95% CI: 0.66–0.88) for age gap (95% CI:0.63–0.83) in predicting 12-week LOR.
Discussion
Identifying predictors of therapeutic response, especially in patients who relapse soon after initiating therapy, could reshape clinical decision making and optimize management strategies for CD. This study aimed to explore the relationship between PhenoAge/age gap and loss of response to biological therapies in adult patients with Crohn’s disease. Our study presents the association between PhenoAge and immunotherapy loss response in Crohn’s disease and establishes a reliable predictive model, which will provide a new approach for predicting the immunotherapy loss response of patients in the clinic.
The PhenoAge/age gap is closely related to disease progression and prognosis.9,16 Understanding the correlation between PhenoAge/age gap and the length of remission in patients with CD is crucial for improved therapy management and the prevention of negative outcomes. Nevertheless, there are insufficient data regarding the correlation between the PhenoAge/age gap and the depletion of biological agents in adult Crohn’s disease patients.
Previous studies have shown that the development of anti-drug antibodies (ADAs) against biologic agents, especially anti-TNF therapies like infliximab and adalimumab, is the leading cause of LOR.17 These antibodies reduce serum drug levels and neutralize drug activity, leading to decreased effectiveness over time.17 Low serum drug concentrations due to increased drug clearance or suboptimal dosing contribute to loss of response. However, monitoring of anti-TNF drugs and drug antibody concentrations is expensive and not covered by medical insurance, which places a high economic burden on patients. It is relatively poorly available in clinical practice and is affected by various factors, resulting in large individual differences in the blood drug concentrations. Interestingly, Hibi et al reported that CRP showed better performance in detecting an infliximab level,18 a type of anti-TNF drugs. Our study showed that PhenoAge and age differences have the potential to predict immune failure in response to biological agents in Crohn’s patients.Given CRP is an important parameter in calculating Phenotypic age and the link between CRP and anti-drugs level, it is hypothesized that the association between PhenoAge and LOR is mediated by level of anti-TNF drugs. The association between PhenoAge and anti-TNF drugs level should be investigated in future.
As individuals age at different rates,19 biological age was proposed as a term to estimate the rate and extent of biological aging and reflect the biological and physiological functions of individuals.9 Liu et al, reported that the positive association between age gap and some chronic disorders and infections (any or bacterial infections).16 This is consistent with our results. In addition, our data indicated that PhenoAge or age gap had better performance than chronological age in predict the 8 weeks LOR (AUC 0.774/0.784 vs 0.618) and 12 weeks LOR (AUC 0.742/0.739 vs 0.616). Moreover, the combination of L1 type with PhenoAge or age gap showed slightly better performance than PhenoAge or age gap alone in predicting 12 weeks LOR.
The effect of a high biological age or a large age gap on LOR is unknown. PhenopAge was calculated based on several inflammatory biomarkers, including C-reactive protein, lymphocyte percentage, and white blood cell count. High biological age may be related to severe inflammation, which is associated with LOR. A recent study reported that white cell count was associated with secondary LOR to infliximab in CD patients.20 C-reactive protein could serve as a biomarker of serum infliximab concentrations.18 High C-reactive protein is related to low serum infliximab concentrations21 which is closely associated with LOR.22 In addition, it has been shown that CST3 is an essential gene for biological aging, which is associated with immune traits.16 High biological age may be associated with immune status in patients with CD. Moreover, body fat-free mass was inversely associated with a higher age gap.16 Interestingly, our previous study showed that sarcopenia is related to a high LOR in patients with CD.23 Biological age may affect LOR by its influence on muscle mass.
This study has several limitations that should be acknowledged. First, this study was conducted at a single center, resulting in a relatively small sample size because CD is rare disease in Asia country although the incidence of CD is increasing. This limits the statistical power and generalizability of the findings. In addition, our study focused on biological agent treatments which further reduces the sample size of the eligible study population. The scarcity of patients receiving biologic therapy makes it difficult to assemble an adequately sized cohort for external validation. Second, this study only focused on biochemical remission. Clinical remission, which incorporates patient symptoms and quality of life, was not evaluated, potentially providing an incomplete picture of the treatment outcomes. Third, owing to the inherent challenges of studying CD, a relatively uncommon condition in Asian countries, predictive models (eg, based on biological age or age gap) were not validated in an independent external cohort. Fourth, several potentially significant confounding variables such as dietary habits, concomitant medication use, and lifestyle factors were not systematically controlled in the analyses. However, their influence on the outcomes (eg,LOR) remains unknown. Additionally, this study focused solely on the primary loss of response. Secondary loss of response, which may have different underlying mechanisms, was not further analyzed, limiting the comprehensiveness of the findings regarding treatment failure.
Conclusion
In conclusion, this study showed that PhenoAge and age gap were associated with loss of response to biologic therapies in adult patients with CD. In addition, PhenoAge and age gap also had acceptable performance in predicting LOR at 8 and 12 weeks. Our study reported potential novel markers for predicting LOR to anti-TNF agents in CD patients. PhenoAge and age gap may be useful in CD treatment management.
Data Sharing Statement
All the data generated or analyzed during this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the Affiliated Hospital of the Nanjing University of Chinese Medicine. This study was conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived by the Ethics Committee of the Affiliated Hospital of Nanjing University of Chinese Medicine owing to the retrospective nature of the study.
Author Contributions
Conceptualization: Xin Chen, Xiao Chen, and Qiufeng Zhao. Data curation: Xin Chen, Jingjing Liu, Yiyping Zhang and Yu Wang. Formal analysis: Xin Chen, Jingjing Liu, Yiping Zhang, Yu Wang and Xiao Chen. Funding acquisition: Qiufeng Zhao. Investigation: Xin Chen, Jingjing Liu, Yiping Zhang, Yu Wang, Xiao Chen and Qiufeng Zhao. Methodology: Xin Chen, Jingjing Liu and Yiping Zhang. Project administration: Xin Chen, Xiao Chen and Qiufeng Zhao. Resources: Xin Chen, Xiao Chen and Qiufeng Zhao. Supervision: Xiao Chen and Qiufeng Zhao. Visualization: Xin Chen, Xiao Chen and Qiufeng Zhao. Writing-original draft: Xin Chen, Jingjing Liu, Yiping Zhang, Yu Wang, Xiao Chen and Qiufeng Zhao. Writing-review and editing: Xin Chen, Xiao Chen and Qiufeng Zhao. All authors gave final approval of the version to be published, have agreed on the journal to which the article has been submitted, and agree to take responsibility and be accountable for the contents of the article.
Funding
This study was funded by the Science and Technology Commission of Shanghai Municipality (24SF1904202) and the Shanghai Shenkang Hospital Development Center Project (SHDC22022310-A, SHDC22022310-B).
Disclosure
The authors declare that they have no competing interests.
References
1. Ng SC, Shi HY, Hamidi N, et al. Worldwide incidence and prevalence of inflammatory bowel disease in the 21st century: a systematic review of population-based studies. Lancet. 2017;390(10114):2769–2778. doi:10.1016/S0140-6736(17)32448-0
2. Prideaux L, Kamm MA, De Cruz PP, et al. Inflammatory bowel disease in Asia: a systematic review. J Gastroenterol Hepatol. 2012;27(8):1266–1280. doi:10.1111/j.1440-1746.2012.07150.x
3. Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn’s disease. Lancet. 2017;389(10080):1741–1755. doi:10.1016/S0140-6736(16)31711-1
4. Torres J, Bonovas S, Doherty G, et al. ECCO guidelines on therapeutics in crohn’s disease: medical treatment. J Crohns Colitis. 2020;14(1):4–22. doi:10.1093/ecco-jcc/jjz180
5. Papay P, Ignjatovic A, Karmiris K, et al. Optimising monitoring in the management of crohn’s disease: a physician’s perspective. J Crohns Colitis. 2013;7(8):653–669. doi:10.1016/j.crohns.2013.02.005
6. Papamichael K, Rivals-Lerebours O, Billiet T, et al. Long-term outcome of patients with ulcerative colitis and primary non-response to infliximab. J Crohns Colitis. 2016;10(9):1015–1023. doi:10.1093/ecco-jcc/jjw067
7. Singh S, George J, Boland BS, et al. Primary non-response to tumor necrosis factor antagonists is associated with inferior response to second-line biologics in patients with inflammatory bowel diseases: a systematic review and meta-analysis. J Crohns Colitis. 2018;12(6):635–643. doi:10.1093/ecco-jcc/jjy004
8. Kumar M, Murugesan S, Ibrahim N, Elawad M, Al Khodor S. Predictive biomarkers for anti-TNF alpha therapy in IBD patients. J Transl Med. 2024;22(1):284. doi:10.1186/s12967-024-05058-1
9. Khan SS, Singer BD, Vaughan DE. Molecular and physiological manifestations and measurement of aging in humans. Aging Cell. 2017;16(4):624–633. doi:10.1111/acel.12601
10. Wang T, Duan W, Jia X, et al. Associations of combined phenotypic ageing and genetic risk with incidence of chronic respiratory diseases in the UK Biobank: a prospective cohort study. Eur Respir J. 2024;63(2):2301720. doi:10.1183/13993003.01720-2023
11. Kuo CL, Pilling LC, Atkins JL, et al. Biological aging predicts vulnerability to COVID-19 severity in UK Biobank participants. J Gerontol a Biol Sci Med Sci. 2021;76(8):e133–e141. doi:10.1093/gerona/glab060
12. Maté I, Martínez de Toda I, Arranz L, Álvarez-sala JL, De la Fuente M. Accelerated immunosenescence, oxidation and inflammation lead to a higher biological age in COPD patients. Exp Gerontol. 2021;154:111551. doi:10.1016/j.exger.2021.111551
13. Nannini DR, Cortese R, Egwom P, Palaniyandi S, Hildebrandt GC. Time to relapse in chronic lymphocytic leukemia and DNA-methylation-based biological age. Clin Epigenet. 2023;15(1):81. doi:10.1186/s13148-023-01496-8
14. Verschoor CP, Belsky DW, Andrew MK, et al. Advanced biological age is associated with improved antibody responses in older high-dose influenza vaccine recipients over four consecutive seasons. Immun Ageing. 2022;19(1):39. doi:10.1186/s12979-022-00296-7
15. Chen L, Zhao Y, Liu F, et al. Biological aging mediates the associations between urinary metals and osteoarthritis among U.S. adults. BMC Med. 2022;20(1):207. doi:10.1186/s12916-022-02403-3
16. Liu WS, You J, Ge YJ, et al. Association of biological age with health outcomes and its modifiable factors. Aging Cell. 2023;22(12):e13995. doi:10.1111/acel.13995
17. Fine S, Papamichael K, Cheifetz AS. Etiology and management of lack or loss of response to anti–tumor necrosis factor therapy in patients with inflammatory bowel disease. Gastroenterol Hepatol. 2019;15(12):656–665.
18. Hibi T, Sakuraba A, Watanabe M, et al. C-reactive protein is an indicator of serum infliximab level in predicting loss of response in patients with Crohn’s disease. J Gastroenterol. 2014;49(2):254–262. doi:10.1007/s00535-013-0807-0
19. Hamczyk MR, Nevado RM, Barettino A, et al. Biological versus chronological aging: JACC Focus Seminar. J Am Coll Cardiol. 2020;75(8):919–930. doi:10.1016/j.jacc.2019.11.062
20. Chanchlani N, Lin S, Bewshea C, et al. Mechanisms and management of loss of response to anti-TNF therapy for patients with Crohn’s disease: 3-year data from the prospective, multicentre PANTS cohort study. Lancet Gastroenterol Hepatol. 2024;9(6):521–538. doi:10.1016/S2468-1253(24)00044-X
21. Adedokun OJ, Xu ZH, Gasink C, et al. Pharmacokinetics and exposure response relationships of ustekinumab in patients with Crohn’s disease. Gastroenterology. 2018;154(6):1660–1671. doi:10.1053/j.gastro.2018.01.043
22. Mitchell RA, Shuster C, Shahidi N, et al. The utility of infliximab therapeutic drug monitoring among patients with inflammatory bowel disease and concerns for loss of response: a retrospective analysis of a real-world experience. Can J Gastroenterol Hepatol. 2016;2016:5203898. doi:10.1155/2016/5203898
23. Liu J, Tang H, Lin T, et al. Sarcopenia assessed by computed tomography or magnetic resonance imaging is associated with the loss of response to biologic therapies in adult patients with Crohn’s disease. Clin Transl Sci. 2023;16(11):2209–2221. doi:10.1111/cts.13621
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.