")
Back to Journals » Risk Management and Healthcare Policy » Volume 14
The Association Between Medical Liability Insurance Coverage and Medical Disturbances in Tertiary Psychiatric Hospitals in China: A National Survey
Authors Luo J, Liu H, Liu Y, Jiang F , Tang YL
Received 6 July 2021
Accepted for publication 30 August 2021
Published 13 September 2021 Volume 2021:14 Pages 3767—3774
DOI https://doi.org/10.2147/RMHP.S328046
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jongwha Chang
Jin Luo,1 Huanzhong Liu,2 Yuanli Liu,3 Feng Jiang,1 Yi-Lang Tang4,5
1Institute of Healthy Yangtze River Delta, Shanghai Jiao Tong University, Shanghai, People’s Republic of China; 2Department of Psychiatry, Chaohu Hospital of Anhui Medical University, Hefei, People’s Republic of China; 3School of Health Policy and Management, Chinese Academy of Medical Sciences & Peking Union Medical College, Beijing, People’s Republic of China; 4Department of Psychiatry and Behavioral Sciences, Emory University, Atlanta, GA, USA; 5Atlanta VA Medical Center, Atlanta, Ga, USA
Correspondence: Feng Jiang
Institute of Healthy Yangtze River Delta, Shanghai Jiao Tong University, Shanghai, People’s Republic of China
Email [email protected]
Yi-Lang Tang
Department of Psychiatry and Behavioral Sciences, Emory University, Atlanta, GA, USA
Email [email protected]
Background: Medical disturbances (MD), a severe type of medical disputes, are common in Chinese hospitals. Medical liability insurances were introduced to establish a new system of conflict resolution and risk management. However, data are scarce on the effects of medical liability insurance coverage and MD in psychiatric hospitals. This study was set to address it based on a nationwide survey.
Methods: A national cross-sectional survey was conducted in March 2019. Physicians in 41 tertiary psychiatric hospitals participated in a smartphone based anonymous questionnaire. Experience of MD, sociodemographic and occupational characteristics, and job satisfaction information were reported by physicians. The hospital medical liability insurance status was reported by participating hospitals. Multi-level logistic regression analysis was used to examine the association between medical liability insurance coverage and MD.
Results: In total, 4511 physicians completed the survey, 3760/4511 (83.35%) physicians in 32 hospitals had medical liability insurance coverage, and 1401/4511 (31.06%) physicians had encountered medical disturbances in the previous year. After adjusting for confounding factors, medical liability insurance coverage was not significantly associated with MD (OR=1.28, 95% CI: 0.93– 1.76). Female gender, working in West China, and higher job satisfaction were protective factors for MD. Higher outpatient volume/week (> 50 patients/week) and longer working hours/week were risk factors for MD.
Conclusion: Nearly one-third of physicians in Chinese top-tier psychiatric hospitals reported experience of MD. There was no significant association between medical liability insurance coverage and MD experienced among physicians in Chinese psychiatric hospitals. Policymakers and hospital administrators need to tailor the scope of medical liability insurance and to focus on other factors to reduce MD, including reducing workload and improving the doctor–patient relationship.
Keywords: medical disturbance, medical liability insurance, physicians, public psychiatric hospitals, China
Background
Medical disputes are often caused by differing perceptions of treatment outcomes between patients (or their close relatives) and physicians (or medical institutions).1 Although medical disputes are often due to negligence, they may or may not correlate with medical malpractice. In the past decades, the number of global medical disputes has increased dramatically in China.2–5 Many studies showed that one of the important reasons for this phenomenon is aggravated doctor-patient mistrust.5–7
The mechanism to resolve medical disputes in China has not been well established. Patients and their families in China often seek to settle disputes outside the legal system by magnifying them. The dissatisfied patients and families, especially those with financial motives, often resort to disrupting and attacking hospitals to obtain compensation.2 Intense behaviors related to “seeking justice” include engaging in long-running public mourning for the “victim” at the hospital, protest, public shaming, petitioning, parading coffins, and engaging in verbal or even physical violence against healthcare professionals by demanding greater compensation. Due to the disruptive nature, these severe medical disputes have been called medical disturbances (MD) or “Yi Nao” in Chinese language.8
When facing medical disputes or MD, neither hospitals nor patients favor the legal resolution of disputes. The former tend to offer under-the-table payments to avoid further conflicts. The latter often take advantage of this by demanding greater compensation.8 In the face of the increasingly high frequency and amount of claims for MD, the risk of liability for medical malpractice has negatively impacted healthcare in China. Therefore, it is imperative to explore better ways to resolve medical disputes through mediation, arbitration, or litigation.9
Medical liability insurance is a type of insurance that may protect physicians against claims of medical negligence.10 Markets of medical liability insurance have occasionally experienced crisis, such as in the mid-1970s, mid-1980s, and early 2000s.11 Since the 2000s, the medical liability insurance markets have been moderately stable.12 As the cost of medical liability insurance depends on the liability system, it can fluctuate widely.13 Along with the tort reforms, medical liability insurance has increased the effectiveness of dealing with medical malpractice.14
Since 2007, China’s government has promoted medical liability insurance to find better ways of risk management and risk-sharing for medical disputes. Medical liability insurance is available through insurance companies, with different premiums. Public hospitals in China are encouraged (not mandated) to purchase medical liability insurance annually for all physicians against claims of medical negligence. A recent study in China demonstrated that medical liability insurance could mediate the doctor-patient relationship and reduce intense medical disputes or MD.15 Other studies from general hospitals showed that medical liability insurance was not associated with decrease in MD, due to low efficiency, low payment, and high premiums.16,17 Overall, the effect of medical liability insurance on MD in China is inconclusive.
So far, no studies have examined the association between medical liability insurance and MD in psychiatric hospitals. Therefore, using data from a national survey of psychiatric hospitals and healthcare professionals, this study aimed to 1) investigate the proportion of physicians who encountered MD in tertiary psychiatric hospitals, 2) examine the association between medical liability insurance and MD, and 3) explore factors associated with MD among physicians in tertiary psychiatric hospitals.
Materials and Methods
Study Design and Samples
This national cross-sectional study was carried out in March 2019. The National Health Commission approved this project. In total, 41 provincial tertiary public psychiatric hospitals were selected from 29 provinces, except Gansu and Tibet, due to the lack of tertiary psychiatric hospitals. In China’s healthcare system, public hospitals played an important role for healthcare delivery.18 The 41 hospitals that participated in the study accounted for 2.65% of all psychiatric hospitals in China, they delivered 15.67% of the inpatient care among all psychiatric hospitals, and there were 6986 physicians working in these hospitals (17.10% of all physicians in psychiatric hospitals).18
All physicians in these target hospitals were recruited to participate in this survey. Each physician voluntarily responded to a smartphone-based questionnaire anonymously through WeChat (a popular social application in mainland China), as reported previously.19 Through email, each hospital reported whether their physicians were covered by medical liability insurance in 2018.
This study was conducted in accordance with the Declaration of Helsinki, and the Ethics Committee in Chaohu Hospital of Anhui Medical University approved the study protocol. Each participant obtained an electronic consent form before they responded to the questionnaire.
Measures
Exposure Variable
The officials of target hospitals reported whether their hospitals had purchased medical liability insurance for physicians in 2018. In China, each hospital only buys one package of medical liability insurance to cover all physicians.15 Therefore, if the hospital had a medical liability insurance package in 2018, then the physicians in this hospital were defined as covered by medical liability insurance.
Outcome Variable
Physicians were asked to report whether they experienced MD in 2018. Detailed operational definitions for MD were included in the questionnaire for better reliability.20
Confounding Variables
This part involved sociodemographic and occupational characteristics such as age, gender, marital status, number of children, educational level, professional title, administrative position, monthly income, geographical region, outpatient volume/week, number of charged beds, night shifts/month, and working hours/week. The job satisfaction of physicians was measured through the short version of the Minnesota Satisfaction Questionnaire (MSQ).21
Data Analysis
We used t-tests or Chi-square tests for continuous variables and categorical variables, as appropriate, to examine the relationships between MD and sociodemographic characteristics, job-related factors, and medical liability insurance coverage. Variables that achieved a marginal significance (p<0.10) in the univariate analysis were included in the logistic regression. We set the p-level of the univariate analysis at 0.1 intentionally, to include more potentially significant variables.
The physicians were nested in 41 hospitals, so we used a multi-level logistic regression model.22 Finally, the relationship between MD and medical liability insurance coverage was determined through a multi-level logistic regression, adjusted for other confounding variables within the whole sample, with the significance level at the p-value of 0.05 (two-tailed).
All statistical analyses were conducted through the STATA software version 16.0 (Stata Corporation, College Station, TX, USA).
Results
Sample Characteristics and Univariate Analysis
In total, all physicians (6986) in 41 hospitals were invited to participate; 4576 physicians responded (response rate=65.5%). Finally, 4511 completed the questionnaire with no logical errors and were included in the statistical analysis. Table 1 shows the samples’ characteristics.
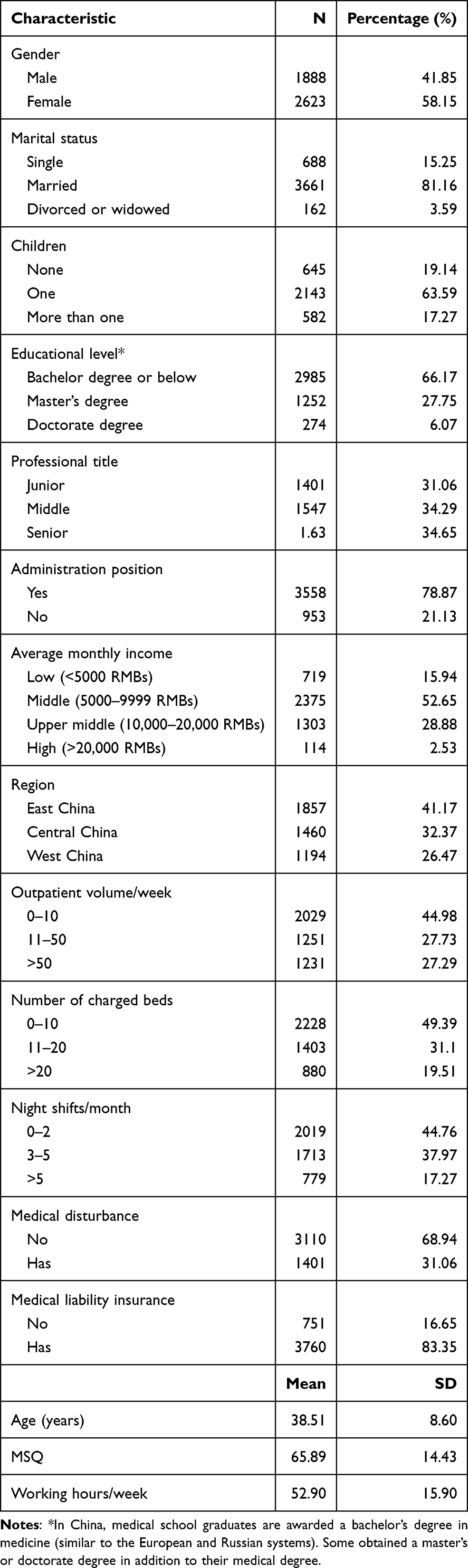 |
Table 1 Characteristics of Physicians in Chinese Tertiary Psychiatric Hospitals (N=4511) |
Among them, 3760 (83.35%) physicians in 32 hospitals had medical liability insurance coverage, and 1401 (31.06%) physicians reported having experienced MD in the past year. Among the hospitals which had medical liability insurance, 14 are in East China, 8 in central China, and 10 in west China (p=0.212) (see Table 2).
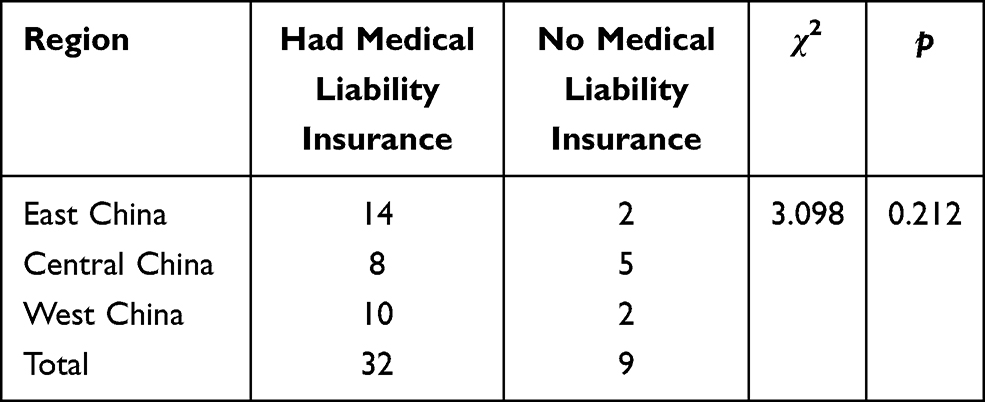 |
Table 2 Medical Liability Insurance Status in Hospitals |
Univariate Analysis
The Univariate analysis demonstrated that MD was significantly associated with social-demographic factors (age, gender, marital status, region) and occupational characteristics (professional title, administration position, outpatient volume/week, number of charged beds, night shifts/month, working hours/week, and MSQ), at the p=0.05 level. At the p=0.1 level, it was also significantly associated with the number of children (p=0.083).
In physicians with medical liability insurance coverage, 31.17% of them reported experiencing MD, with 30.49% among those without medical liability insurance (p=0.714) who experienced MD. In other words, no significant difference was found between the two groups (see Table 3).
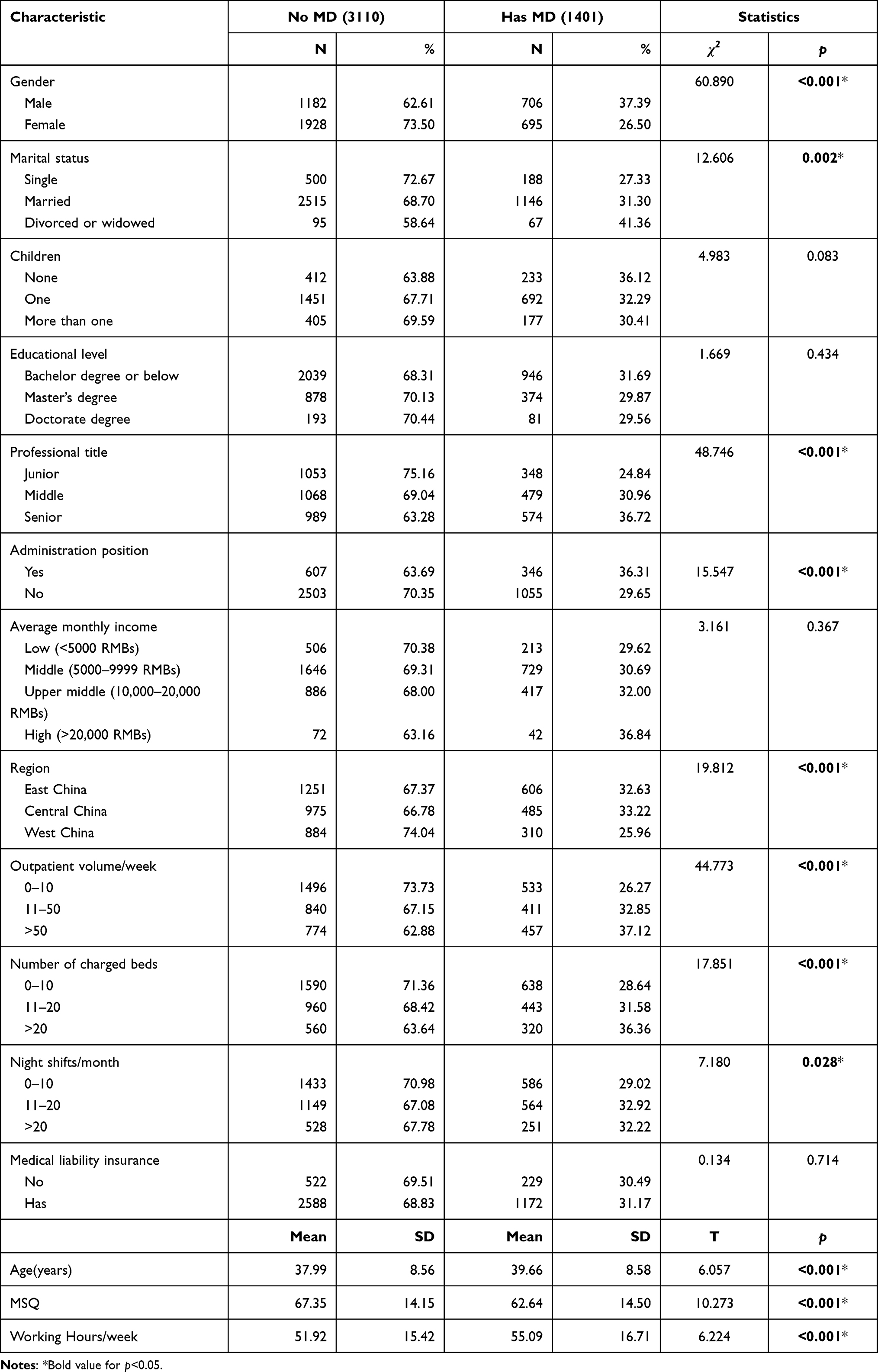 |
Table 3 Univariate Analysis of MD |
Multi-Level Logistic Regression
At the hospital level, medical liability insurance coverage was not significantly associated with MD. While physicians in West China were less likely to encounter MD (OR=0.68, 95% CI: 0.50–0.93, p=0.015). After adjusting for confounding factors in multi-level logistic regression analysis, female gender and higher MSQ were significantly associated with a lower likelihood of MD (p<0.001). Higher outpatient volume/week (>50 patients/week) and longer working hours/week were associated with higher risk of MD (OR=1.44, 95% CI: 1.17–1.77, p<0.001; OR=1.01, 95% CI: 1.00–1.01, p<0.001, respectively) (see Table 4).
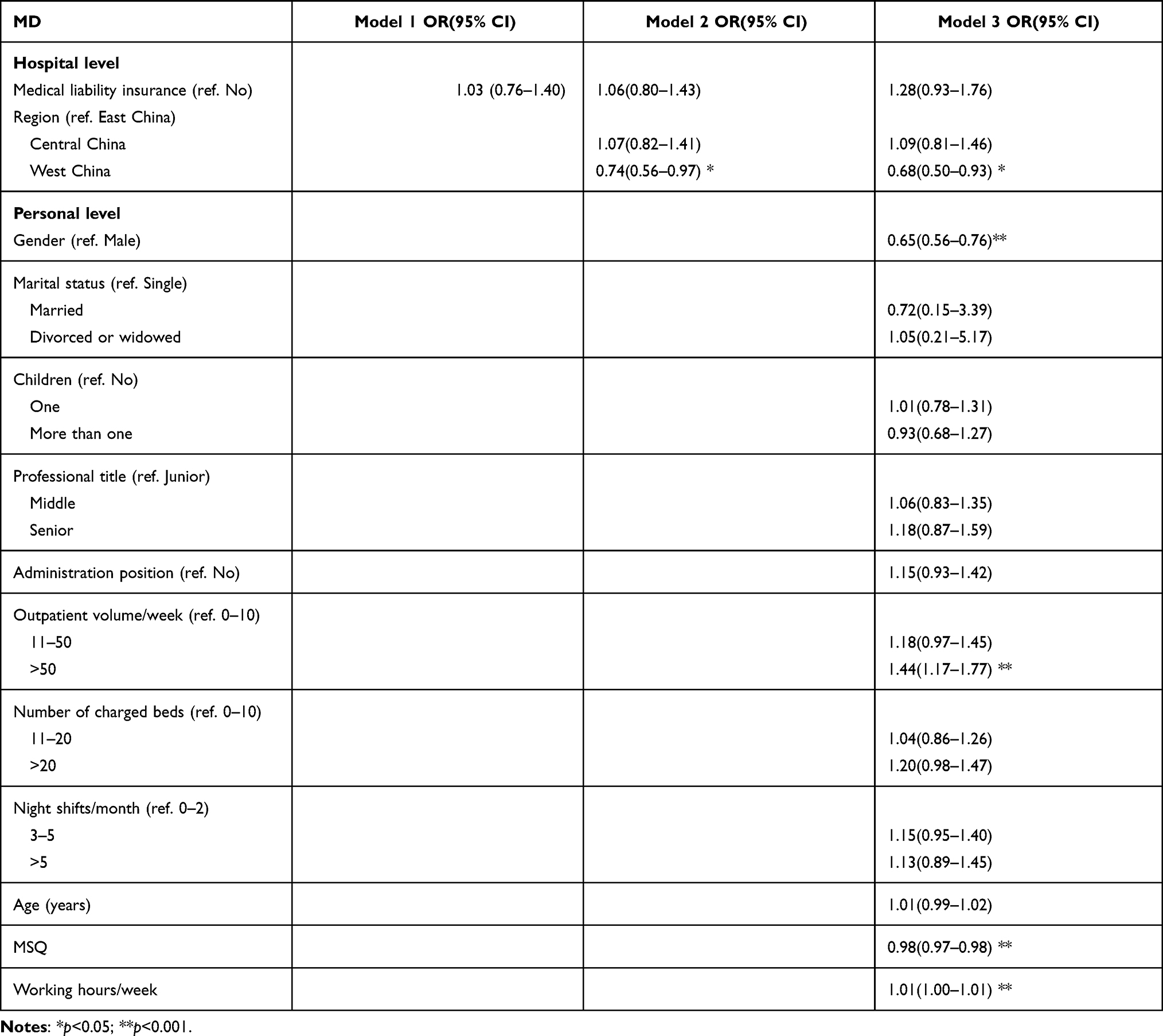 |
Table 4 Multi-Level Logistic Regression Model for MD (N=4511) |
Discussion
To our best knowledge, this study was one of the first studies focusing on medical liability insurance and MD based on a nationally representative physician sample from tertiary psychiatric hospitals in China. We found that medical liability insurance coverage was not significantly associated with MD. We also found that a few demographic and occupational factors were significantly associated with MD.
One surprising finding from our study is that medical liability insurance was not associated with a decrease in MD, which is different from a previous study. Zhang et al reported that, based on data from six provinces in China between 2011 and 2016, medical liability insurance was associated with lower MD.15 Of note, the data on MD in the above study were collected by insurance companies, so underreporting or underestimating was likely. On the other hand, the study was based on data from general hospitals. This finding is in line with another survey from a top Chinese hospital, which demonstrated that the effectiveness of medical liability insurance to reduce MD was not significant, and policymakers should promote the validity of medical liability insurance.17
There are several possible explanations for our findings. First, our finding may be due to the scope of medical liability insurance coverage. The medical liability insurance companies in China only pay for medical malpractice, as in the US and other countries.23 As the financial benefits were important motives in MD, patients or their relatives were often motivated to disturb the normal process to make the issues identified as medical malpractices or get more compensation through an under-the-table settlement.2,24 To solve this problem, the government of China should improve funding for the health care system to reduce hospitals’ profit-minded motivation and to improve the doctor-patient relationship.25 Meanwhile, a more powerful and effective medical liability system is needed to reduce MD.1,26–29
This study showed that males, longer working hours/week, and lower job satisfaction were associated with MD, which was in line with other studies and empirical evidence. Female physicians usually have more patience and better communication skills than their male counterparts.30,31 Physicians with a heavy workload and low job satisfaction usually undermine the quality of clinical encounters and have a worse doctor-patient relationship, which may trigger medical disputes.3,32 Therefore, policymakers and hospital management should pay more attention to physician job satisfaction and workload to reduce MD.
We found that 31.06% of physicians in psychiatric hospitals reported experience of MD in the past year, which was significantly higher than the physicians in other countries and general hospitals in China. In the US, only 2–3% of all psychiatrists have faced a malpractice claim per year.12 This tremendous difference may be due to differences in the healthcare systems, the patient populations and their expectations, and the definitions of medical disputes in different studies. Wu et al recently reported that 20.86% of physicians in general hospitals had encountered MD, which was much lower than our findings.20 This gap may be due to the characteristics of the patients and their families,33 the nature of psychiatric service, and the relative shortage of mental health resources.34
There are several limitations about this study. First, as is the case in almost all cross-sectional studies, the causal relationship between MD and medical liability insurance cannot be established. Second, we did not have data on the frequency and intensity of each MD incident and the amount of settled compensation. Third, the detailed information on the scope of medical liability insurance coverage in each hospital was not available. Fourth, the sample was from tertiary public psychiatric hospitals, so the findings may not be generalizable to all physicians in China. Finally, the study was conducted anonymously, and we believe the confidentiality and anonymity would have decreased the response bias. However, response bias is still possible and it might affect our findings.
Conclusions
In conclusion, we found that among physicians working in public psychiatric hospitals in China, nearly one-third reported experiencing medical disturbances in the past year. We did not find significant association between medical liability insurance coverage in physicians and their experience of MD. Male gender, lower MSQ score, more outpatient volume/week, and longer working hours per week were significantly associated with likelihood of experiencing MD, while working in West China appeared to have a lower risk of MD.
While our findings are somewhat surprising, it is worth noting that MD is a multifactorial phenomenon, and it also needs to take multidisciplinary actions. Like any insurance, the primary goal of medical liability insurance is not to prevent certain adverse events from happening. Rather, it is for risk management after it happened. Therefore, policymakers need to focus on the bigger picture and other important aspects of the healthcare system, such as optimizing healthcare resources, reducing physicians’ workload and working hours, and improving doctor-patient relationship.
Data Sharing Statement
The datasets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Acknowledgment
We would like to thank Ms. Brianna Wong, BS, CCRC, at the Atlanta VA Medical Center for her excellent editing on the final draft.
Disclosure
The authors declare no conflicts of interest related to this study.
References
1. Yu F, Xie X, Ding F, Xue C, Sun Z. Changing procedures for resolving medical disputes in China. Intern Med J. 2018;48(12):1552–1553. doi:10.1111/imj.14133
2. He AJ, Qian J. Explaining medical disputes in Chinese public hospitals: the doctor-patient relationship and its implications for health policy reforms. Health Econ Policy Law. 2016;11:359–378. doi:10.1017/s1744133116000128
3. Lancet T. Protecting Chinese doctors. Lancet. 2020;395(10218):90. doi:10.1016/s0140-6736(20)30003-9
4. Wang M, Liu GG, Zhao H, Butt T, Yang M, Cui Y. The role of mediation in solving medical disputes in China. BMC Health Serv Res. 2020;20:225. doi:10.1186/s12913-020-5044-7
5. Zeng Y, Zhang L, Yao G, Fang Y. Analysis of current situation and influencing factor of medical disputes among different levels of medical institutions based on the game theory in Xiamen of China: a cross-sectional survey. Medicine. 2018;97:e12501. doi:10.1097/md.0000000000012501
6. Tucker JD, Cheng Y, Wong B, et al. Patient-physician mistrust and violence against physicians in Guangdong Province, China: a qualitative study. BMJ Open. 2015;5:e008221. doi:10.1136/bmjopen-2015-008221
7. Yip W, Hsiao W. Harnessing the privatisation of China’s fragmented health-care delivery. Lancet. 2014;384:805–818. doi:10.1016/s0140-6736(14)61120-x
8. Pan D. “Doctors killed my baby”: argumentative patterns in medical disputes in China. Health Commun. 2018;33(10):1267–1276. doi:10.1080/10410236.2017.1351271
9. Yin T, Liu Z, Xu Y. Analysis of crisis management of medical disputes in China and Australia: a narrative review article. Iran J Public Health. 2019;48:2116–2123.
10. Marshall DC, Punglia RS, Fox D, Recht A, Hattangadi-Gluth JA. Medical malpractice claims in radiation oncology: a Population-Based Study 1985–2012. Int J Radiat Oncol Biol Phys. 2015;93:241–250. doi:10.1016/j.ijrobp.2015.05.040
11. Baker T. Medical Malpractice and the Insurance Underwriting Cycle. Social Science Electronic Publishing; 2005.
12. Jena AB, Seabury S, Lakdawalla D, Chandra A. Malpractice risk according to physician specialty. N Engl J Med. 2011;365:629–636. doi:10.1056/NEJMsa1012370
13. Sage WM, Boothman RC, Gallagher TH. Another medical malpractice crisis?: try something different. JAMA. 2020;324:1395–1396. doi:10.1001/jama.2020.16557
14. Childers RG. Tort reform: do details matter? Health Econ Policy Law. 2021;16:308–324. doi:10.1017/s1744133121000025
15. Zhang X-Z, Yang L-G, Zhao Y. The medical malpractice insurance and medical disputes. Sci Decis Mak. 2019;25–48. Chinese. doi:10.3773/j.issn.1006-4885.2019.11.025
16. Bertoli P, Grembi V. Courts, scheduled damages, and medical malpractice insurance. Empir Econ. 2018;55:831–854. doi:10.1007/s00181-017-1279-5
17. Sun X-Q, Peng H, Guo X-J, Qin M-W. AnaIysis and reflection on the effect of medical liability insurance in the hospital for ten years. Chin Hosp Manage. 2016;36:88–89.
18. National Health Commission of the People’s Republic of China. China Health Statistical Yearbook. Beijing: Press of Peking Union Medical College; 2019.
19. Xia L, Jiang F, Rakofsky J, et al. Cigarette smoking, health-related behaviors, and burnout among mental health professionals in China: a nationwide survey. Front Psychiatry. 2020;11:706. doi:10.3389/fpsyt.2020.00706
20. Wu Y, Jiang F, Ma J, Tang YL, Wang M, Liu Y. Experience of medical disputes, medical disturbances, verbal and physical violence, and burnout among physicians in China. Front Psychol. 2020;11:556517. doi:10.3389/fpsyg.2020.556517
21. Jiang F, Hu L, Rakofsky J, et al. Sociodemographic characteristics and job satisfaction of psychiatrists in China: results from the first nationwide survey. Psychiatr Serv. 2018;69:1245–1251. doi:10.1176/appi.ps.201800197
22. Goldstein H. Multilevel Statistical Models.
23. Jiang Y-H. Introduction to the development model of medical liability insurance in the United States, Japan, Britain and Germany. Chin Insur. 2021;(3)60–64. Chinese. Available from: https://navi.cnki.net/knavi/journals/ZGBX/detail?uniplatform=NZKPT. Accessed September 10, 2021.
24. Liu T, Tan X. Troublemaking in hospitals: performed violence against the healthcare professions in China. Health Sociol Rev. 2021;30:157–170. doi:10.1080/14461242.2020.1779105
25. Yip W, Fu H, Chen AT, et al. 10 years of health-care reform in China: progress and gaps in universal health coverage. Lancet. 2019;394(10204):1192–1204. doi:10.1016/s0140-6736(19)32136-1
26. Kessler DP, Summerton N, Graham JR. Effects of the medical liability system in Australia, the UK, and the USA. Lancet. 2006;368(9531):240–246. doi:10.1016/s0140-6736(06)69045-4
27. Hsieh MT, Lu LH, Lin CW, Chen YW. Correlation between malpractice litigation and legislation reform in Taiwan over a 30-year period. Int J Gen Med. 2021;14:1889–1898. doi:10.2147/ijgm.s312640
28. Frierson RL, Joshi KG. Malpractice law and psychiatry: an overview. Focus. 2019;17(4):332–336. doi:10.1176/appi.focus.20190017
29. Nakajima K, Keyes C, Kuroyanagi T, Tatara K. Medical malpractice and legal resolution systems in Japan. JAMA. 2001;285:1632–1640. doi:10.1001/jama.285.12.1632
30. Hojat M, Gonnella JS, Nasca TJ, Mangione S, Vergare M, Magee M. Physician empathy: definition, components, measurement, and relationship to gender and specialty. Am J Psychiatry. 2002;159:1563–1569. doi:10.1176/appi.ajp.159.9.1563
31. Chaitoff A, Sun B, Windover A, et al. Associations between physician empathy, physician characteristics, and standardized measures of patient experience. Acad Med. 2017;92:1464–1471. doi:10.1097/acm.0000000000001671
32. Liu Z, Zhang Y, Asante JO, Huang Y, Wang X, Chen L. Characteristics of medical disputes arising from dental practice in Guangzhou, China: an observational study. BMJ Open. 2018;8:e018738. doi:10.1136/bmjopen-2017-018738
33. Caruso R, Antenora F, Riba M, et al. Aggressive behavior and psychiatric inpatients: a narrative review of the literature with a focus on the European experience. Curr Psychiatry Rep. 2021;23:29. doi:10.1007/s11920-021-01233-z
34. Xia L, Jiang F, Rakofsky J, et al. Resources and workforce in top-tier psychiatric hospitals in China: a nationwide survey. Front Psychiatry. 2021;12:573333. doi:10.3389/fpsyt.2021.573333
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.