Back to Journals » Patient Preference and Adherence » Volume 19
The Association Between Ischemic Stroke Patients’ Illness Perception and Adherence to Rehabilitation Exercises: An Analysis of a Moderated Chain Mediation Model
Authors Long Q ![]() , Lee Y
, Lee Y ![]() , Liu Y, Li Y, Shi Z, Cui L
, Liu Y, Li Y, Shi Z, Cui L
Received 22 June 2025
Accepted for publication 9 October 2025
Published 21 October 2025 Volume 2025:19 Pages 3211—3223
DOI https://doi.org/10.2147/PPA.S544741
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Qizhi (Cathy) Yao
Qingwen Long,1,2 Yujun Lee,2 Yina Liu,2 Yongli Li,2 Zijuan Shi,2 Lijun Cui3
1Nursing Department, Affiliated Hospital of North Sichuan Medical College, Nanchong, People’s Republic of China; 2Nursing Department, North Sichuan Medical College, Nanchong, People’s Republic of China; 3Transfusion Medicine Department, Affiliated Hospital of North Sichuan Medical College, Nanchong, People’s Republic of China
Correspondence: Lijun Cui, Transfusion Medicine Department, Affiliated Hospital of North Sichuan Medical College, Nanchong, 637000, People’s Republic of China, Email [email protected]
Background: To investigate the relationship between stroke patients’ illness perception and rehabilitation exercise adherence, while also exploring the potential mediating influences of frailty and family care, as well as the moderating impact of nutrition.
Methods: A total of 307 ischemic stroke patients underwent surveys utilizing the Illness Perception Questionnaire, the Frailty Assessment Scale, the Family APGAR Index, the Rehabilitation Adherence Assessment Scale, and the Mini Nutritional Assessment-Short Form. Pearson correlation analysis was used to examine the associations among the scores of various scales. Following data standardization, mediation and moderation effects were tested using PROCESS v4.1 Models 6 and 83, with the Bootstrap method employed to assess the robustness of these effects.
Results: Illness perception was negatively correlated with rehabilitation exercise adherence (r=− 0.532, P< 0.01). Both frailty (β=− 0.17, 95% CI [− 0.26, − 0.079]) and family care (β=− 0.101, 95% CI [− 0.156, − 0.052]) had significant independent mediating effects between illness perception and rehabilitation exercise adherence, and the chain mediation effect was also significant (β=− 0.087, 95% CI [− 0.14, − 0.045]), accounting for 68.45% of the total effect. Nutrition moderated the relationship between illness perception and frailty (β=− 0.176, P< 0.001), with the positive influence of illness perception on frailty weakening as the level of nutrition increased.
Conclusion: Illness perception is negatively associated with rehabilitation exercise adherence, exacerbating frailty and reducing family care. The impact of illness perception on escalating frailty is primarily manifested through inadequate nutritional status. Therefore, healthcare providers are required to help stroke patients establish correct illness cognitions, prevent the occurrence of frailty, encourage family members to provide sufficient family care, and pay attention to patients’ nutritional status to promote better recovery.
Keywords: stroke, illness perception, frailty, family care, rehabilitation exercise adherence
Introduction
Ischemic stroke, a prevalent form of acute cerebrovascular injury, represents a significant contributor to morbidity and mortality in the adult population of China.1,2 Approximately 80% of patients are left with varying degrees of functional impairment. Rehabilitation exercises, as evidenced by clinical trials, are the most effective method for reducing disability and enhancing activities of daily living.3–6 Rehabilitation exercise adherence (REA) refers to the extent to which patients follow the guidance of healthcare providers or participate in rehabilitation training activities to promote comprehensive recovery of physical, psychological, and social functions. Optimal adherence plays a crucial role in enhancing rehabilitation effectiveness.7 The recovery of stroke patients is characterized by a slow and gradual rehabilitation process, demanding a high level of REA.8 Studies have shown that the early REA of stroke patients is slightly above 50%, impacted by multiple factors, which seriously hinder the maximum functional recovery and increase the risk of disability.9,10 Therefore, it is essential to explore the factors influencing REA and the underlying mechanisms in stroke patients.
Currently, research on REA in stroke patients primarily concentrates on physical function and emotional experiences, with few investigations delving into illness perception (IP). The process of IP entails individuals assessing health threats through cognitive appraisal and emotional responses, which prompt adjustments in self-management and coping strategies, impacting psychological reactions and behaviors.11 Within a cultural framework of collectivism and filial piety, stroke patients’ IP are deeply impacted by family attitudes and care-related decision-making.12,13 The moral imperative of not burdening the family becomes ingrained as “my illness is a family load”, leading to heightened negative IP. Meanwhile, post-stroke functional deficits often elicit stigma-related shame.14 This shame can lead patients to refrain from openly discussing their condition and being active in their community, ultimately limiting their access to crucial rehabilitation information and strengthening negative IP. Studies have revealed that a significant number of stroke patients maintain a heightened negative IP, pointing to a widespread deficiency in their accurate and comprehensive comprehension of the condition.15,16 The deficiency may cause individuals to doubt the effectiveness of rehabilitation exercises, potentially decreasing their REA.17–19 This association has been confirmed by consistent evidence from Chinese and international studies. Domestic studies have reported that stroke survivors, especially those with hemiplegia, exhibit low overall adherence to prescribed rehabilitation exercises, and that more negative IP are significantly and inversely related to REA.9,20 International studies have confirmed this discovery and have also shown that patients usually receive information about strokes from informal sources rather than medical professionals before experiencing symptoms.21,22 This restricted knowledge base fosters a narrow, often catastrophic understanding of the disease, reinforced by cultural narratives that emphasize high morbidity and mortality; in turn, these cognitions evoke negative emotional responses that impede engagement in rehabilitation and prolong recovery. Similar patterns have been observed in various chronic illnesses. Enhancing IP through targeted education has been shown to improve REA in hypertension, chronic kidney disease, breast cancer, and more.23–26 This evidence-based intervention clarifies disease mechanisms, expected benefits of exercise, and self-management strategies, leading to increased therapeutic compliance in routine clinical practice. Nevertheless, the exact mechanisms behind this association are still uncertain. Consequently, we propose Hypothesis 1: More negative IP will be associated with lower REA.
According to Shelley’s stress process model,27 individuals employ both internal and external resources to cope with stressors based on their disease cognitions. Internal resources encompass physiological status and personality traits, while external resources include family and social support. Frailty, a common clinical condition among stroke patients, manifests as dysfunction in various physiological systems, rendering the body more susceptible and less capable of maintaining homeostasis.28,29 Stroke patients, with diminished physiological reserves, reduced psychological resilience, and impaired social functioning, are at an elevated risk of developing frailty to different extents.30 Research has confirmed a significant association between negative IP and increased frailty levels. Adverse IP can exacerbate emotions like anxiety and depression, which in turn weakens patients’ physical functions and psychological resilience, accelerating the process of frailty.18,31 The occurrence of frailty increases physical vulnerability and reduces exercise tolerance, thereby challenging REA. Based on the stress-process framework, we propose Hypothesis 2: frailty mediates the relationship between IP and REA. The high disability and mortality rates associated with stroke significantly increase patients’ care needs and the support and affection from family members. Family care (FC) can provide emotional comfort to patients, reduce negative emotions, and promote healthy behaviors. Studies have shown that poor IP can heighten psychological burden, weaken perceptions of FC, and impact health behaviors.32 We advance Hypothesis 3: FC mediates the association between IP and REA. During the stress process, stressors can influence an individual’s behavioral coping through mediating variables like physiological status, personality traits, and family or social support. Meanwhile, these mediating variables are not entirely independent but interact with and influence each other. Research on the associations between IP, frailty, FC, and REA in stroke patients is currently limited. Existing studies on IP either focus solely on its direct effect on REA or only on indirect pathways, leading to a fragmented understanding of the underlying mechanisms.33–35 Frailty is typically framed as a unilateral risk factor for poor REA, while its potential synergistic and competitive interactions with other variables remain unaddressed.36–38 Studies on FC and REA have mostly been limited to verifying correlations, overlooking the direct impact of FC on REA and its indirect effects through mediating factors.39 However, there is a paucity of research that comprehensively discusses the interrelationships among all four factors. Therefore, this study employs the stress process model as a theoretical framework to investigate the influence of frailty and FC in the relationship between IP and REA. We propose Hypothesis 4: IP will indirectly impact REA through a serial mediation pathway, where heightened frailty diminishes FC, subsequently affecting REA.
Additionally, research indicates that a large proportion of stroke patients are susceptible to malnutrition.40,41 Malnutrition may result in reduced physical function, manifesting as fatigue and weakness, which can further worsen patients’ negative IP and the occurrence of frailty. Therefore, we incorporate nutrition and propose Hypothesis 5: Nutritional status will weaken the positive relationship between IP and frailty. Specifically, it explores the mediating roles of frailty and FC, as well as the moderating influence of nutrition, in the association between IP and REA in ischemic stroke patients. The hypothesized model is depicted in Figure 1.
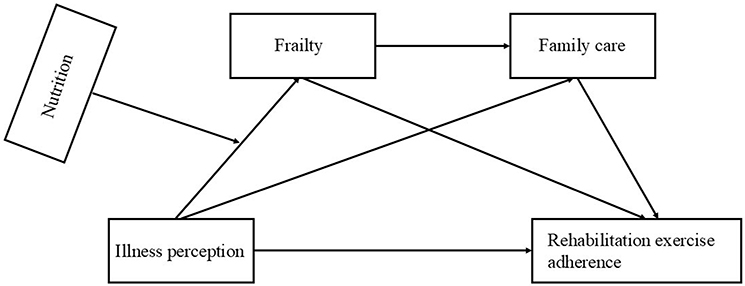 |
Figure 1 The hypothesized model depicting the relationships among the variables. |
Methods
Participants
Using a convenience sampling method, stroke patients who received treatment at two tertiary hospitals in Sichuan Province between January and May 2025 were selected as participants. Inclusion criteria were (1) met the diagnostic criteria for ischemic stroke as outlined in the Diagnostic Criteria for Major Types of Cerebrovascular Diseases in China 201942 and confirmed by CT or MRI imaging; (2) aged≥45 years; (3) had stable conditions after treatment; (4) had limb dysfunction (muscle strength≤Grade 4); (5) were fully aware of the study objectives, voluntarily participated in this study, and provided written informed consent. Exclusion criteria were diagnosed with hemorrhagic stroke; cardiac or pulmonary insufficiency, hepatic or renal failure, and malignant tumors; and the disorders of consciousness, cognition, mental health, or language. Sample size was estimated a priori using G*Power 3.1. Since there are no direct estimates of mediation effect sizes in stroke populations, we adopted Cohen’s conventional benchmark and specified a medium effect size (f² = 0.15) for multiple regression.43 With a two-tailed α of 0.05 and a power (1 – β) of 0.95, the projected sample size was 166 participants after accounting for an anticipated 20% attrition rate. A total of 320 questionnaires were distributed. Thirteen were excluded based on predefined quality-control criteria: five had excessive missing data (>20% blank items), five exhibited straight-line responding (identical answers across all items in a scale), and three contained logically inconsistent responses to paired reverse-keyed items. Consequently, 307 valid questionnaires remained, yielding an effective response rate of 95.9%. Meanwhile, all questionnaires were distributed and collected on site on the same day. In cases of missing responses, participants were approached for consent, and the forms were immediately returned to them for on-the-spot completion to ensure data integrity.
Assessments
Brief Illness Perception Questionnaire
Utilizing the official Chinese version of the scale developed by Broadbent,44 we assessed 9 items, each rated on a scale from 0 to 10 (with items 3, 4, and 7 reverse-scored). Item 9 was used solely for attribution and not included in the scoring. The total score ranges from 0 to 80, with higher scores indicating greater negative perception and a heavier burden of illness. The scale showed satisfactory internal consistency with a Cronbach’s α of 0.770 and adequate structural validity of 0.762 during Chinese stroke hemiplegic individuals.20 In our study, the Cronbach’s α coefficient for this scale was 0.726.
Tilburg Frailty Indicator
The scale was developed by Gobbens from Tilburg University and was adapted into Chinese by scholar Xi Xing.45,46 Li et al subsequently adapted and validated the scale for use among Chinese patients with chronic diseases, reporting a Cronbach’s α of 0.846 and a structural validity coefficient of 0.80.47 It includes three dimensions: physical frailty, psychological frailty, and social frailty, comprising a total of 15 items. The total score ranges from 0 to 15, with higher scores indicating a more severe degree of frailty. A score of 5 or above is determined as frailty. In this study, the Cronbach’s α coefficient for this scale was 0.792.
Family Adaptation, Partnership, Growth, Affection and Resolve (APGAR) Index
The questionnaire, developed by Dr. Smilkstein in the United States, was translated into Chinese by scholar Lu Fan.48,49 It comprises five items, each rated on a 3-point Likert scale from 0 to 2, yielding a total score between 0 and 10. A higher score reflects greater levels of FC. The Chinese-adapted APGAR demonstrated a Cronbach’s α coefficient of 0.83 and a construct validity of 0.80 in patients with cerebrovascular disease.49 In this study, the scale demonstrated a Cronbach’s α coefficient of 0.807.
The Questionnaire on Exercise Adherence
The scale, developed by Lin Beilei,50 encompasses three dimensions: physical participation in exercise (items 1–8), monitoring exercise effects (items 9–11), and seeking advice during exercise (items 12–14). It consists of 14 items, each scored on a 4-point scale from 1 to 4, with a total score range of 0 to 56 reflecting adherence levels. The study quantified REA by employing the REA index, calculated as (total score/56) × 100 and categorized as high (>75), moderate (51–74), and low (<50). The Cronbach’s α coefficient for this scale is 0.923, with a structural validity of 0.921.50 In this study, the Cronbach’s α coefficient was 0.869.
Mini Nutritional Assessment Short Form (MNA-SF)
Nutritional screening was performed with the MNA-SF in this study. The scale is rapid, simple to administer, and has clearly defined scoring criteria, making it ideal for patients who are bedridden or unable to walk. When body mass index cannot be obtained, calf circumference can be substituted; the assessment can be completed at the bedside without biochemical testing. Importantly, calf-circumference cut-offs should be ethnically appropriate, and the Asian-specific thresholds are recommended for accurate classification. Rubenstein et al developed the questionnaire,51 which was later translated into Chinese by a scholar. The Chinese version of MNA-SF exhibited a Cronbach’s α coefficient of 0.711 and a construct validity of 0.827 when used for nutritional screening in hospitalized older adults with chronic diseases.52 The questionnaire comprises six items with a total score of 14 points, where a score of ≤7 signifies malnutrition. The Cronbach’s α coefficient in the current study was 0.725.
Concurrently, we also collected patients’ sociodemographic and clinical disease characteristics, including age, gender, educational level, comorbidities, and so on.
Statistical Analysis
Data analysis was conducted using SPSS 27.0 statistical software. Continuous variables that followed a normal distribution were described using mean (M)±standard deviation (SD), while those that did not follow a normal distribution were described using the median (P25, P75). Independent samples t-tests and analysis of variance (ANOVA) were used to explore differences between general characteristics and the dependent variable. Harman single-factor analysis was conducted to identify common method bias. Pearson correlation analysis was performed to investigate relationships between variables. Mediation and moderation effects were assessed using the Process macro and Bootstrap analysis. The significance level was set at α = 0.05.
Ethical Approval
This study has been approved by the Ethics Committee of the Affiliated Hospital of North Sichuan Medical College in accordance with the Declaration of Helsinki, with the ethics approval number being 2025ER49-1.
Results
Assessment of Common Method Bias
The Harman single-factor test identified 14 factors with eigenvalues exceeding 1. The first factor accounted for 17.82% of the variance, falling below the critical threshold of 40%. This suggests minimal influence of common method bias in the study.
Participants Characteristic
Among the 307 study participants, 179 (58.3%) were male and 128 (43.7%) were female, with a mean age of (69.41±10.90) years. The average IP score was (45.64±6.53), indicating a moderate level, while REA scored an average of (54.83±9.32), also at a moderate level. The mean frailty score was (4.59±2.14), FC scored (6.82±2.44), and nutrition scored (9.79±2.67). Additional participant characteristics are detailed in Table 1. Gender, marital status, living arrangement, hukou, and number of medications emerged as statistically significant predictors of REA through univariate analysis.
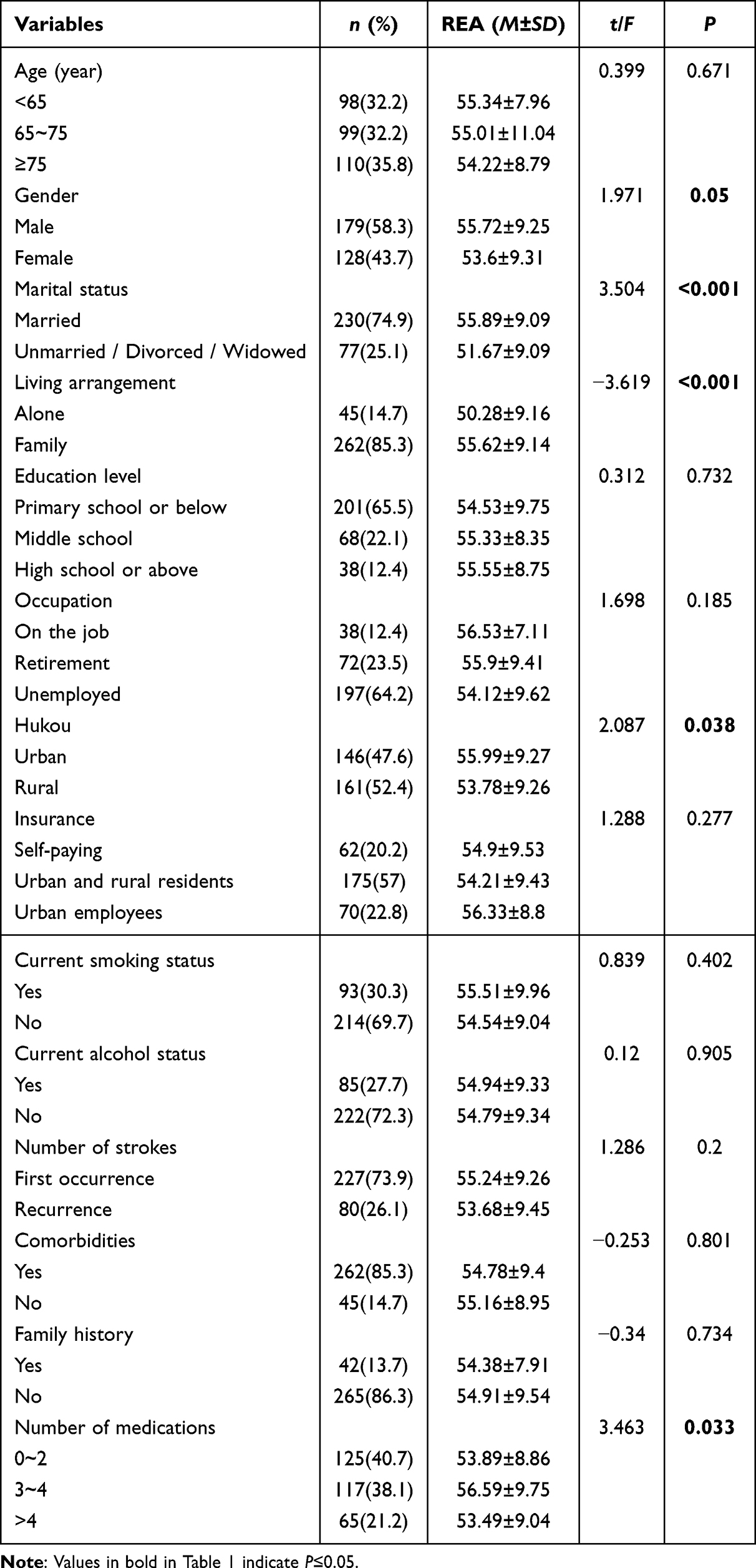 |
Table 1 Univariate Analysis of Different Baseline Characteristics on Rehabilitation Exercise Adherence |
Correlation Analysis
Pearson correlation analysis revealed a positive association between IP and frailty (r = 0.625, P < 0.01), and negative correlations with FC (r = −0.640, P < 0.01) and REA (r = −0.532, P < 0.01). Moreover, REA showed positive correlations with FC (r = 0.630, P < 0.01) and nutrition (r = 0.414, P < 0.01), while displaying a negative correlation with frailty (r = −0.612, P < 0.01) (Table 2).
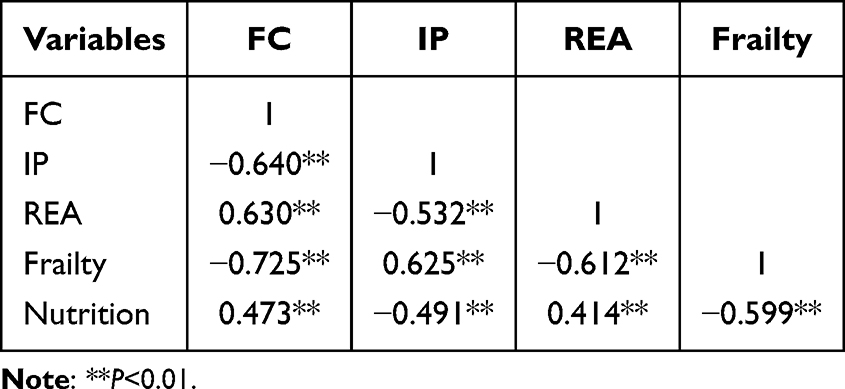 |
Table 2 Correlation Analysis Among Variables |
Mediation Effect Analysis
Standardization of all variables was performed within Model 6 of the PROCESS macro, employing 5000 bootstrap samples. Control variables encompassed gender, marital status, hukou, living arrangement, and number of medications. A chain mediation model was formulated, with the outcomes of the mediation effect analysis detailed in Table 3. IP exerted a significant negative effect on REA (β = −0.165, P < 0.01), each one-SD increase in IP corresponded to a 0.165-SD decrease in REA. The mediating analysis revealed that frailty and FC act as chain mediators in the relationship between IP and REA. The direct impact of IP on REA is 31.55%. In addition, three indirect pathways were identified: Path 1: IP → exacerbates frailty → reduces REA, with a mediating effect of 32.50%; Path 2: IP → weakens FC → reduces REA, with a mediating effect of 19.31%; Path 3: IP → exacerbates frailty → weakens FC → reduces REA, with a chain mediating effect of 16.63%. The Bootstrap test results showed that the 95% confidence intervals (CIs) for all paths did not include zero, indicating significant mediation effects. Frailty and FC independently mediated the relationship between IP and REA, while also acting as a chain mediation. The proportions of these mediation effects are detailed in Table 4.
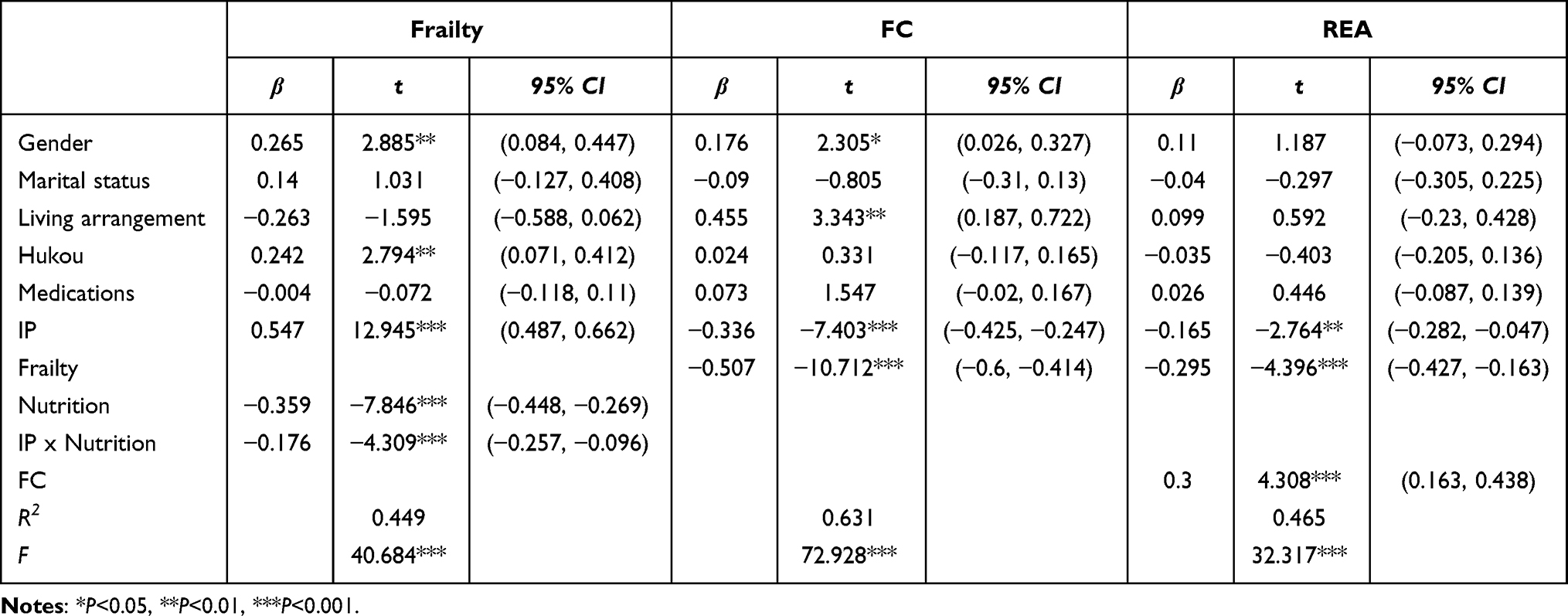 |
Table 3 Regression Analysis Results for the Moderated Chain Mediation Model |
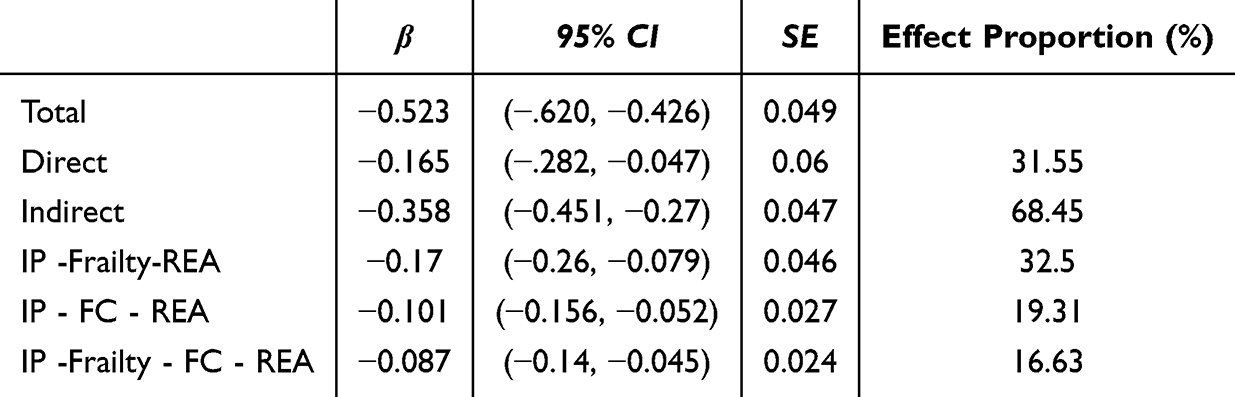 |
Table 4 The Bootstrap 95% Confidence Interval Results for the Effect of Illness Perception on Rehabilitation Exercise Adherence |
Moderation Effect Analysis
In this study, Model 83 of the PROCESS macro was employed to examine the moderating impact of nutrition. Results revealed that the interaction between IP and nutrition has significantly negatively impacted on frailty (β = −0.176, P < 0.001). It demonstrated that a one-SD rise in IP combined with a one-SD decline in nutritional status increased frailty scores by 0.176 SD. Nutrition levels were classified as high, medium, and low based on the criteria of one SD above and below the (M±1SD). Subsequent simple slope analyses were performed (Figure 2). At a high level of nutrition (M + 1SD), IP significantly exerted a significant positive effect on frailty (β = 0.226, P < 0.001), and this relationship persisted even at a low nutrition level (M - 1SD) (β = 0.578, P < 0.001). However, as nutrition levels increased, the positive association between IP and frailty progressively weakened. Moreover, the chain mediation effect of frailty and FC remained significant at various nutrition levels, with a more prominent effect observed at lower nutrition levels.
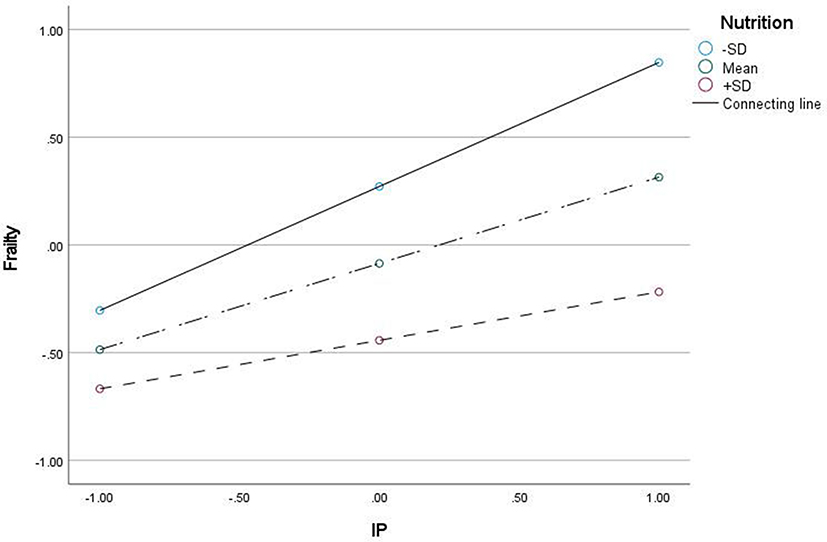 |
Figure 2 Nutritional status moderates the relationship between IP and frailty. |
Discussion
Illness Perception Was Negatively Associated with Rehabilitation Exercise Adherence
By utilizing moderated mediation analysis, this study revealed how IP influences REA in patients with ischemic stroke. Studies have shown that IP was significantly negatively associated with REA. This discovery reinforces and broadens existing research suggesting that stroke patients’ perceptions of the disease, often shaped by their pre-existing environment, are significantly constrained. Influenced by cultural beliefs, the elevated prevalence and fatality rates of stroke prompt patients to perceive disease advancement with pessimism.20–22 The Self-Regulation Model of IP posits that negative IP and emotions can lead patients who perceive a health threat to engage in negative behaviors, reducing treatment adherence and hindering disease recovery. Therefore, guiding patients to establish accurate IPs is of significant importance for patients to actively confront their illness and enhance adherence to treatment and rehabilitation.
Frailty Mediates the Relationship Between Illness Perception and Rehabilitation Exercise Adherence
This study revealed that frailty serves as a mediator between IP and REA. Studies have shown that patients’ IP is associated with a variety of factors, including a strong sense of identification with the illness, the acute or chronic nature of the disease course, periodicity of time, and serious consequences.53 These factors may result in negative emotional reactions in patients, such as anxiety, depression, and rumination. Adverse emotional responses may result in negative IP, impacting patients’ mental health and indirectly contributing to frailty development, thus affecting adherence to rehabilitation exercises.54,55 Post-stroke frailty is linked not only to physiological decline but also to impairments in limb function, mental well-being, and social involvement.56 Negative IP can trigger or exacerbate patients’ psychological burden, undermining their confidence and initiative in rehabilitation, thereby affecting the recovery of limb function and activities of daily living. Moreover, it can decrease patients’ engagement in social activities, resulting in a decline in social functioning. The interaction among physical, psychological, and social functional impairments contributes to the development of frailty. Existing studies have confirmed a direct correlation between the severity of negative IP and the likelihood of frailty. Furthermore, negative IP and frailty mutually influence each other, establishing a bidirectional causal relationship.31,33 Frail patients, facing physical and psychological challenges, frequently encounter difficulties in maintaining adherence to extended rehabilitation regimens. One study found that negative IP can lead to skepticism toward rehabilitation treatment plans among stroke patients, diminishing their confidence in recovery.33 Frailty, in turn, affects the sustainability of REA.
Family Care Mediates the Relationship Between Illness Perception and Rehabilitation Exercise Adherence
This study discovered that FC mediates the relationship between IP and REA. IP is a process that encompasses patients’ cognitive and emotional responses to their illness, reflecting the psychological impact of their physiological burden. Patients experiencing negative IP typically turn to family members for emotional support and guidance in selecting effective coping strategies. Relevant studies have shown that high levels of FC have been demonstrated to enhance the psychological well-being of stroke patients, mitigate negative IP, lessen the self-perceived burden of the disease, and consequently enhance both their physical and mental health. Moreover, positive FC can effectively enhance treatment adherence and quality of life among patients with chronic diseases.57 Positive FC plays a crucial role in assisting patients in dealing with negative events, facilitating increased emotional support, enhancing perceptions of disease adversity, and fostering positive behaviors for illness management.
However, the generalizability of the finding to populations beyond mainland China is constrained by the distinct cultural beliefs and family interaction patterns that characterize the Chinese context. Rooted in Confucian collectivism, filial piety, and hierarchical family roles,12,13 this cultural milieu not only shapes the cognitive schemata through which illness is interpreted and managed but also predetermines the gendered distribution of caregiving labor, with female relatives assuming primary responsibility while male involvement remains limited—thereby directly constraining both the quantity and quality of FC that patients ultimately perceive. Consequently, the patient’s IP is not constructed in isolation; rather, it is continuously negotiated within an asymmetrical power structure in which the relative discursive authority of individual family members mediates the final illness narrative. Given these culture-specific contingencies, results derived from a Chinese sample may not extrapolate to societies whose value systems, family configurations, or interactional norms diverge substantially; replication across culturally heterogeneous settings is therefore required before any broader generalization is warranted.
Frailty and Family Care Mediate the Relationship Between Illness Perception and Rehabilitation Exercise Adherence in a Chain Mediation Model
Additionally, studies have also found that frailty and FC play a chain mediating role between IP and REA. Specifically, the stronger a patient’s perception of disease threat, the less confident they feel in self-control, and the more likely they are to engage in negative ruminative thinking, leading to emotional responses such as restlessness and depression, which increase the risk of frailty. Consistent with Pearlin’s caregiver stress process model,58 escalating frailty intensifies functional dependence, which abruptly elevates caregiving burden and depletes family members’ physical, financial, and emotional resources. In the context of Confucian filial piety,59,60 this burden is disproportionately shouldered by female relatives who must simultaneously negotiate the conflicting roles of caregiver and breadwinner; such role strain accelerates physiological and psychological exhaustion, thereby undermining the sustainability of FC. Within this mechanistic framework, reliable and compassionate family support can supply patients with both practical and emotional aid, diminishing unfavorable illness beliefs and possibly reversing frailty, ultimately assisting patients in establishing favorable exercise routines for rehabilitation. Conversely, if patients have high levels of negative IP and have already developed frailty, and if family members fail to provide sufficient FC, then IP and frailty can produce a boomerang effect, weakening patients’ perception of FC, which in turn is associated with lower REA.
Nutrition Moderates the Relationship Between Illness Perception and Frailty
This study concludes that nutrition plays a significant role in moderating the association between IP and frailty. Under high nutritional status, the positive influence of IP on frailty is diminished in comparison to low nutritional status. This could be attributed to stroke exacerbating the decline in systemic physiological reserve functions, which can lead to homeostatic imbalance or physical frailty. The formation of a vicious cycle is a result of patients’ lack of accurate IP, which leads to the accumulation of negative emotions and exacerbates psychological frailty. The trajectory of frailty is closely associated with nutritional status in this process.61–63 The physiological impact of stroke can lead to decreased appetite and food intake. Patients’ negative perception of the disease can compound this effect, causing unintentional weight loss, a prevalent occurrence among hospitalized patients. The lack of equilibrium between protein supply and demand, coupled with the disruption in the balance between muscle protein synthesis and degradation, results in the ongoing reduction of skeletal muscle mass and impaired muscle function. This, in turn, further exacerbates patients’ functional impairments and reduces treatment adherence. However, our study revealed that nutritional status can significantly moderate the association between IP and frailty, irrespective of the level. As nutritional status improves, the association between IP and frailty progressively weakens. This finding underscores the necessity of closely monitoring the nutritional status of stroke patients. Malnutrition can exacerbate negative IP, which in turn intensifies the occurrence of frailty and ultimately reduces patients’ REA. Thus, enhancing the nutritional management of stroke patients can improve their physiological condition and positively impact their psychological well-being, thereby providing robust support for recovery.
Limitations
This study offers new insights into REA among patients with ischemic stroke, albeit with certain limitations. The data were obtained from a single region, potentially restricting the generalizability and applicability of the findings to stroke populations in regions with different socioeconomic conditions, healthcare resources, or cultural norms. Subsequent studies could expand their scope to encompass additional regions and populations. Given that all research data are self-reported by patients, there may be a recall bias leading to information bias. This study employed a cross-sectional design; therefore, the directionality of the observed associations remains undetermined, and causal relationships cannot be inferred. Subsequent research may investigate these relationships using a longitudinal design approach.
Conclusion
IP has the potential to lower REA among ischemic stroke patients by heightening frailty and compromising FC giving. In addition, nutrition may moderate the link between IP and frailty, strengthening the negative impact of IP on frailty, especially when nutritional status is low. To improve REA among stroke survivors, healthcare providers should integrate routine screening for both nutritional and frailty risks. For patients exhibiting low mood, concurrent psychological care and structured health education should be provided to establish accurate IP for both patients and their families. Additionally, caregivers should receive targeted guidance on delivering precise multidimensional support, encompassing diet, emotional encouragement, and functional exercise to facilitate comprehensive recovery.
Data Sharing Statement
Correspondence to the first author or corresponding author for further information. First author to: Qingwen Long, Nursing Department, Affiliated Hospital of North Sichuan Medical College, Nanchong, 637000, China; emails: [email protected].
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare financial support was received for the research, authorship, and publication of this article. This work was supported by the Nanchong Science and Technology Program (23JCYJPT0046).
Disclosure
The authors declare that they have no competing interests.
References
1. Hankey GJ. Stroke. Lancet. 2017;389(10069):641–654. doi:10.1016/S0140-6736(16)30962-X
2. Ma Q, Li R, Wang L, et al. Temporal trend and attributable risk factors of stroke burden in China, 1990-2019: an analysis for the global burden of disease study 2019. Lancet Public Health. 2021;6(12):e897–e906. doi:10.1016/S2468-2667(21)00228-0
3. Longde W; Report on Stroke Prevention and Treatment in China Writing Group. Brief report on stroke prevention and treatment in China, 2021. Chin J Cerebrovasc Dis. 2023;20(11):783–793.
4. Longde W; Group ROSCICW. Brief report on stroke center in China,2022. Chin J Cerebrovasc Dis. 2024;21(8):565–576.
5. Chinese Medical Association Neurology Branch, Neurorehabilitation Group of the Chinese Medical Association Neurology Branch, Cerebrovascular Disease Group of the Chinese Medical Association Neurology Branch. Chinese guidelines for early rehabilitation in stroke patients. Chin J Neurol. 2017;50(6):405–412. doi:10.3760/cma.j.issn.1006-7876.2017.06.002
6. Yetiş A, Canli M, Yildiz NT, et al. Investigation of the validity, reliability and psychometric properties of the turkish version of the Ottawa sitting scale in patients with Parkinson’s disease. Sci Rep. 2025;15(1):2628. doi:10.1038/s41598-025-87006-7
7. Coleman ER, Moudgal R, Lang K, et al. Early rehabilitation after stroke: a narrative review. Curr Atherosclerosis Rep. 2017;19(12):59. doi:10.1007/s11883-017-0686-6
8. Zeiler SR. Should we care about early post-stroke rehabilitation? Not yet, but soon. Curr Neurol Neurosci Rep. 2019;19(3):13. doi:10.1007/s11910-019-0927-x
9. Haijuan L, Meiqi Y, Jinhua C, Xuhui S. Status and correlation analysis of stroke patients’ family function and rehabilitation exercise compliance. Chin J Modern Nursing. 2019;25(27):3474–3479. doi:10.3760/cma.j.issn.1674-2907.2019.27.009
10. Han S, Shengwen S, Huiqin W, Meiqi Y, Jinhua C. A study on the rehabilitation exercise compliance curve in stroke patients. Chin J Nurs. 2016;51(6):712–715.
11. Broadbent E, Petrie KJ, Main J, Weinman J. The brief illness perception questionnaire. J Psychosom Res. 2006;60(6):631–637. doi:10.1016/j.jpsychores.2005.10.020
12. Gu C, Li Z. The confucian ideal of filial piety and its impact on Chinese family governance.
13. Li Y. Confucian philosophy of family: interpretation or justification? Asian Philosophy. 2022;32(2):152–163. doi:10.1080/09552367.2022.2024346
14. Hu R, Wang X, Liu Z, et al. Stigma, depression, and post-traumatic growth among Chinese stroke survivors: a longitudinal study examining patterns and correlations. Top Stroke Rehabil. 2022;29(1):16–29. doi:10.1080/10749357.2020.1864965
15. Liu HY, Liu QH, Li ZR, Deng CS, Zhang XP, Wan LH. The cognitive appraisal path of stroke knowledge, coping traits, family functioning and stigma among stroke patients: a moderated parallel mediation model. J Clin Nurs. 2024;33(3):1048–1061. doi:10.1111/jocn.16909
16. Lu Q, Wang D, Fu L, et al. The effect of stigma on social participation in community-dwelling Chinese patients with stroke sequelae: a cross-sectional study. Clin Rehabil. 2022;36(3):407–414. doi:10.1177/02692155211050558
17. Yucheng G, Rui Y, Wenyue Z, Shiwei L, Yumei L. Trajectories of disease perception and decision tree analysis of core influencing factors in stroke patients. J Nursing. 2022;37(3):20–24.
18. Groeneveld IF, van der Pas SL, Meesters JJL, et al. Illness perceptions of stroke survivors: predictors and changes over time - a 1 year follow-up study. J Psychosom Res. 2019;116:54–61. doi:10.1016/j.jpsychores.2018.10.019
19. Yumei L, Yucheng G, Yuqiu Z. Research on the developmental trajectory of rehabilitation exercise adherence and its potential classes predictors in stroke patients. Chin J Nurs. 2023;58(17):2103–2111.
20. Jinwen W, Lingbo L, Hui Y. Status quo and influencing factors of functional exercise compliance in stroke patients with hemiplegia. Chin Nurs Res. 2024;38(8):1478–1484.
21. Tsai SJ, Li CC, Tsai SM, Kao SC, Chen HM, Pai HC. Illness representation and self-efficacy: an exploration of fatigue factors in middle-aged stroke survivors. Clin Nurs Res. 2021;30(7):1030–1037. doi:10.1177/1054773821997134
22. Thomson P, Rushworth GF, Andreis F, Angus NJ, Mohan AR, Leslie SJ. Longitudinal study of the relationship between patients’ medication adherence and quality of life outcomes and illness perceptions and beliefs about cardiac rehabilitation. BMC Cardiovasc Disord. 2020;20(1):71. doi:10.1186/s12872-020-01378-4
23. Sováriová Soósová M, Suchanová R, Parová V, Ulbrichtová A, Kopčová O, Rimárová K. Association between illness perception and adherence to treatment in Slovak patients with hypertension: a cross-sectional study. J Cardiovasc Nurs. 2023;38(5):433–442. doi:10.1097/JCN.0000000000000913
24. Hamza MA, Ullah S, Ahsan H, Ali W, Masud M, Ahmed A. Health literacy, illness perception, and their association with medication adherence in end-stage renal disease. Int Urol Nephrol. 2025;57(9):2979–2994. doi:10.1007/s11255-025-04472-8
25. Lan M, Zhang L, Zhang Y, Yan J. The relationship among illness perception, coping and functional exercise adherence in Chinese breast cancer survivors. J Adv Nurs. 2019;75(1):75–84. doi:10.1111/jan.13832
26. Shakya R, Shrestha S, Gautam R, et al. Perceived illness and treatment adherence to hypertension among patients attending a tertiary hospital in Kathmandu, Nepal. Patient Prefer Adherence. 2020;14:2287–2300. doi:10.2147/PPA.S270786
27. Taylor SE, Stanton AL. Coping resources, coping processes, and mental health. Annu Rev Clin Psychol. 2007;3(1):377–401. doi:10.1146/annurev.clinpsy.3.022806.091520
28. Evans NR, Todd OM, Minhas JS, et al. Frailty and cerebrovascular disease: concepts and clinical implications for stroke medicine. Int J Stroke. 2022;17(3):251–259. doi:10.1177/17474930211034331
29. Evans NR, Wall J, To B, Wallis SJ, Romero-Ortuno R, Warburton EA. Clinical frailty independently predicts early mortality after ischaemic stroke. Age Ageing. 2020;49(4):588–591. doi:10.1093/ageing/afaa004
30. Tan BYQ, Ho JSY, Leow AS, et al. Effect of frailty on outcomes of endovascular treatment for acute ischaemic stroke in older patients. Age Ageing. 2022;51(4):afac096. doi:10.1093/ageing/afac096
31. Xueqi G, Huiju H, Qiqun T, Jiao Y, Tianshu S, Qian W. Factors influencing disease perception in elderly patients with coronary heart disease in nursing homes. Nursing Res. 2023;37(4):608–613.
32. Xu X, Chen X, Wang T, Qiu C, Li M. Relationship between illness perception and family resilience in gynecologic cancer patients: the mediating role of couple illness communication. Support Care Cancer. 2023;31(9):522. doi:10.1007/s00520-023-07992-0
33. Gu X, Shen X, Chu JH, Fang TT, Jiang L. Frailty, illness perception and lung functional exercise adherence in lung cancer patients after thoracoscopic surgery. Patient Prefer Adherence. 2023;17:2773–2787. doi:10.2147/PPA.S435944
34. Oliveira J, Sousa H, Bártolo A, Figueiredo D, Ribeiro O. Illness perception and treatment adherence in haemodialysis: a systematic review. Psychol Health Med. 2023;28(7):1641–1655. doi:10.1080/13548506.2022.2099559
35. Liu YR, Wang Y, Wang J, Wang X. Association between illness perception and adherence to inhaler therapy in elderly Chinese patients with chronic obstructive pulmonary disease. Chron Respir Dis. 2024;21:14799731241286837. doi:10.1177/14799731241286837
36. Pobrotyn P, Pasieczna A, Diakowska D, et al. Evaluation of frailty syndrome and adherence to recommendations in elderly patients with hypertension. J Clin Med. 2021;10(17):3771. doi:10.3390/jcm10173771
37. Uchmanowicz B, Chudiak A, Uchmanowicz I, Mazur G. How may coexisting frailty influence adherence to treatment in elderly hypertensive patients? Int J Hypertens. 2019;2019:5245184. doi:10.1155/2019/5245184
38. Lapi F, Marconi E, Aprile PL, et al. Frailty, comorbidity, and multimorbidity and their relation with medications adherence in primary care older adults. Eur Geriatr Med. 2025;16(2):583–603. doi:10.1007/s41999-024-01098-4
39. Rui L, Hong S, Chunyan Z, Liming G, Wenjuan C, Yifan L. The effect of family functioning on exercise adherence in elderly patients with postoperative vertebral compression fractures and adjacent vertebral re-fractures. Chin J Nurs. 2025;60(10):1164–1170.
40. Lingqin H, Xiaohua W, Yili R, Jun W. Construction of a nomogram for predicting malnutrition risk in elderly patients with pharyngeal dysphagia after stroke. Chin J Gen Pract. 2025;23(4):551–554. doi:10.16766/j.cnki.issn.1674-4152.003947
41. Nan L, Hua A, Geng Y, Xiaonan Z, Rongjun Z. Risk factors for malnutrition and nursing interventions in elderly stroke patients during the recovery period: a review. Chin Med Guide. 2025;23(12):67–70. doi:10.15912/j.issn.1671-8194.2025.12.018
42. Chinese Society of Neurology, Chinese Stroke Society. Diagnostic criteria of cerebrovascular diseases in China (version 2019). Chin J Neurol. 2019;52(9):710–715. doi:10.3760/cma.j.issn.10067876.2019.09.003
43. Cohen J. Statistical Power Analysis for the Behavioral Sciences.
44. Yaqi M, Huiping L, Yajuan Y, et al. Validation of the Chinese version of the brief illness perception questionnaire in female breast cancer patients. J Nursing. 2015;22(24):11–14. doi:10.16460/j.issn1008-9969.2015.24.011
45. Gobbens RJ, van Assen MA, Luijkx KG, Schols JM. Testing an integral conceptual model of frailty. J Adv Nurs. 2012;68(9):2047–2060. doi:10.1111/j.1365-2648.2011.05896.x
46. Xing X, Guifang G, Jing S. Reliability and validity of the Chinese version of the Tilburg frailty indicator. J Nursing. 2013;20(16):1–5. doi:10.16460/j.issn1008-9969.2013.16.006
47. Fei L, Huisong L, Longxiao Z, Bo H, Jingfang L, Xiuli Z. Reliability and validity testing of the Chinese version of Tiburg Frailty Indicator. J Nurs Sci. 2017;32(7):18–20,27.
48. Bellón Saameño JA, Delgado Sánchez A, Luna Del Castillo JD, Lardelli Claret P. Validity and reliability of the family apgar family function test. Aten Primaria. 1996;18(6):289–296.
49. Fan L, Yuan G. Family APGAR questionnaire and its clinical application. Int Med J. 1995;(2):56–59.
50. Beilei L, Zhenxiang Z, Yumei S, Yongxia M, Junfang X, Yaqi Z. Development and validation of a scale for exercise adherence in community-dwelling stroke patients. Chin J Rehabil Med. 2013;28(6):574–578.
51. Rubenstein LZ, Harker JO, Salvà A, Guigoz Y, Vellas B. Screening for undernutrition in geriatric practice: developing the short-form mini-nutritional assessment (MNA-SF). J Gerontol a Biol Sci Med Sci. 2001;56(6):M366–372. doi:10.1093/gerona/56.6.m366
52. Yan Z, Lixian W, Xiaohua L, Hongmei L, Zhengping Z. Application of mini nutritional assessment-short form in nutrition screening inelderly inpatients with chronic diseases. Chin J Multiple Organ Dis Elderly. 2019;18(2):107–111.
53. Pai HC, Li CC, Tsai SM, Pai YC. Association between illness representation and psychological distress in stroke patients: a systematic review and meta-analysis. Int J Nurs Stud. 2019;94:42–50. doi:10.1016/j.ijnurstu.2019.01.015
54. Cheiloudaki E, Alexopoulos EC. Adherence to treatment in stroke patients. Int J Environ Res Public Health. 2019;16(2):196. doi:10.3390/ijerph16020196
55. Khoshbakht Pishkhani M, Dalvandi A, Ebadi A, Hosseini M. Factors affecting adherence to rehabilitation in iranian stroke patients: a qualitative study. J Vasc Nurs. 2019;37(4):264–271. doi:10.1016/j.jvn.2019.07.001
56. Qiao X, Ji L, Jin Y, et al. Effectiveness of a theory-underpinning exercise intervention among community-dwelling (pre)frail older adults: a stepped-wedge cluster-randomized trial. Int J Nurs Stud. 2025;161:104933. doi:10.1016/j.ijnurstu.2024.104933
57. Deek H, Hamilton S, Brown N, et al. Family-centred approaches to healthcare interventions in chronic diseases in adults: a quantitative systematic review. J Adv Nurs. 2016;72(5):968–979. doi:10.1111/jan.12885
58. Pearlin LI, Mullan JT, Semple SJ, Skaff MM. Caregiving and the stress process: an overview of concepts and their measures. Gerontologist. 1990;30(5):583–594. doi:10.1093/geront/30.5.583
59. Hu A. Providing more but receiving less: daughters in intergenerational exchange in mainland China. J Marriage Family. 2017;79(3):739–757. doi:10.1111/jomf.12391
60. Li S, Feldman MW, Jin X. Children, marriage form, and family support for the elderly in contemporary rural China: the case of songzi. Res Aging. 2004;26(3):352–384. doi:10.1177/0164027503262477
61. Zupo R, Castellana F, Bortone I, et al. Nutritional domains in frailty tools: working towards an operational definition of nutritional frailty. Ageing Res Rev. 2020;64:101148. doi:10.1016/j.arr.2020.101148
62. Zupo R, Donghia R, Castellana F, et al. Ultra-processed food consumption and nutritional frailty in older age. GeroScience. 2023;45(4):2229–2243. doi:10.1007/s11357-023-00753-1
63. Zupo R, Castellana F, Guerra V, et al. Associations between nutritional frailty and 8-year all-cause mortality in older adults: the Salus in Apulia study. J Intern Med. 2021;290(5):1071–1082. doi:10.1111/joim.13384
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Frailty, Illness Perception and Lung Functional Exercise Adherence in Lung Cancer Patients After Thoracoscopic Surgery
Gu X, Shen X, Chu JH, Fang TT, Jiang L
Patient Preference and Adherence 2023, 17:2773-2787
Published Date: 2 November 2023
Multidimensional Analysis of Frailty and Its Influencing Factors in Hospitalized Elderly Stroke Patients
Zhou H, Han Y, Xie D, Zheng K, Zhu H, Zhou Z, Ji Y
Clinical Interventions in Aging 2025, 20:1741-1755
Published Date: 11 October 2025