Back to Journals » Clinical Ophthalmology » Volume 17
The Association Between Improvement of Stereoacuity and Suppression in the Treatment of Anisometropic Amblyopia
Authors Shiraishi Y, Wakayama A, Matsumoto F, Tanabe F, Kusaka S
Received 12 March 2023
Accepted for publication 24 May 2023
Published 1 June 2023 Volume 2023:17 Pages 1545—1553
DOI https://doi.org/10.2147/OPTH.S412194
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yukari Shiraishi, Akemi Wakayama, Fumiko Matsumoto, Fumi Tanabe, Shunji Kusaka
Department of Ophthalmology, Kindai University Faculty of Medicine, Osaka-sayama City, Osaka, Japan
Correspondence: Yukari Shiraishi, Department of Ophthalmology, Kindai University Faculty of Medicine, 377-2, Ohnohigashi, Osaka-sayama City, Osaka, 589-8511, Japan, Tel +81-72-366-0221 Ext 2216, Fax +81-72-368-2559, Email [email protected]
Purpose: To investigate the association between stereoacuity and suppression during occlusion therapy for patients with anisometropic amblyopia.
Design: Retrospective study.
Patients and Methods: This study included 19 patients with hyperopic anisometropic amblyopia who underwent occlusion therapy. The mean age of the patients was 5.5 ± 1.4 years. The participants were evaluated for improvement in stereoacuity and suppression before beginning occlusion therapy, when the highest amblyopic visual acuity (VA) was achieved, during tapering, at the end of occlusion therapy, and at the final visit. Stereoacuity was evaluated using the TNO test or JACO stereo test. The presence of suppression was evaluated using circle No. 1 of the Stereo Fly Test or JACO results as the optotype.
Results: Of the 19 patients, 13 (68.4%) had suppression before occlusion, eight (42.1%) when the highest VA was achieved, five (26.3%) during tapering, and none at the final visit. Of the 13 patients with suppression before occlusion, 10 (76.9%) showed further improvement in stereoacuity when suppression disappeared, and nine had foveal stereopsis of 60 arcseconds. A significant association was confirmed between foveal stereopsis and suppression when the highest VA was achieved and during the tapering period (P< 0.05, Fisher’s exact test).
Conclusion: Suppression was observed even when the VA in amblyopic eyes reached the highest score. By gradually decreasing the duration of occlusion, suppression was eliminated, leading to the acquisition of foveal stereopsis.
Keywords: amblyopic visual acuity, foveal stereopsis, occlusion therapy, suppression
Introduction
Anisometropic amblyopia is a type of visual impairment caused by the inability to form a clear image on the fovea of the more ametropic eye.1–3 Stereoacuity decreases due to the inability to see objects binocularly because the more ametropic eye has reduced visual acuity (VA) with amblyopia, and the VA does not improve even with appropriate correction.2,3 Stereoacuity is the most advanced binocular function, and its decrease can potentially impact the activities of daily living.4,5 Therefore, when evaluating the treatment for amblyopia, it is essential to assess not only the changes in VA but also the level of stereoacuity.
Occlusion therapy is used to improve VA for the treatment of anisometropic amblyopia.6–8 Some studies have reported that improvement of VA in amblyopic eyes was associated with improved stereoacuity.6–9 However, other studies failed to demonstrate this association and found that only 35.9−54% of patients achieved a stereoacuity of 60 arcseconds or better despite an improvement in the VA in amblyopic eyes.10,11 These findings indicate that in some cases it is difficult to achieve good stereoacuity by improving VA alone.
Suppression is one of the factors that affects stereoacuity in patients with unilateral amblyopia. Several studies have reported the presence of suppression in anisometropic amblyopia11–18 and its association with decreased stereoacuity.11–13,15,16 These studies suggest that the key to treating amblyopia lies not only in improving VA but also in eliminating suppression and enhancing binocular function to acquire stereoacuity. However, to date, no studies have reported on occlusion therapy for amblyopia and examined the progress of stereoacuity and suppression in detail both during and after the completion of therapy. Chen et al reported that amblyopic VA improved remarkably following 6 months of occlusion therapy, and that the depth of suppression remained the same as that before occlusion. However, they did not evaluate the course of stereoacuity.14 If changes in suppression are found to be associated with improvements in stereoacuity, it would provide a deeper understanding of the etiology of anisometropic amblyopia. Moreover, it would guide physicians on when to terminate occlusion treatment.
Therefore, in this study, we aimed to investigate the relationship between improvement and suppression of stereoacuity during occlusion therapy for patients with anisometropic amblyopia.
Patients and Methods
This retrospective study was approved by the ethics committee of the Kindai University Faculty of Medicine (No. R02-250) and adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from all patients. Among the 106 patients diagnosed with hyperopic anisometropic amblyopia at the Kindai University Hospital between January 2015 and February 2021, 98 were successfully followed up until the end of treatment. Among these 98 patients, 19 (seven males and 12 females) were eligible for evaluation of temporal changes in both stereoacuity and suppression at all treatment periods: before beginning occlusion therapy, when the highest VA in the amblyopic eye was first achieved, during the occlusion tapering period, at the end of occlusion therapy, and at the final visit. All 19 patients underwent occlusion therapy. The participants were aged 3 to 8 years (5.5 ± 1.4 years). Patients showing spherical equivalent anisometropia of <1.50 D in a refraction test using 1% atropine sulfate drops (twice daily for 7 days), those with astigmatism of ≥2.00 D in both eyes, those with manifest strabismus in the cover test, those with clear eccentric fixation in a fixation test on the visuscope, those with a history of amblyopia treatment at other medical facilities, and those with organic diseases, such as cataracts, were excluded. No criteria were set for pre-treatment VA. After refraction examination with 1% atropine sulfate drops, the patients were instructed to wear fully corrective glasses and reminded not to take the glasses off when they were awake. At every visit, the patients and their parents were asked about their wearing status, which was recorded in their medical records. We judged the wearing status based on the medical records. All 19 patients wore their glasses at all times. Occlusion therapy was performed when no further improvement was observed in the VA in the amblyopic eyes after 1−2 months of wearing glasses. The mean daily occlusion time was 6.4 ± 1.6 hours. We instructed the patients to record the number of hours of occlusion every day in a notebook and evaluated the occlusion implementation rate by confirming the notebook at every visit. In all 19 cases, the implementation rate was more than 80% of the instructed occlusion hours.
The duration of occlusion was gradually decreased in the final stage of therapy. The hours of occlusion were decreased to approximately half when the VA in the amblyopic eye improved.
The VA was measured using a standard Landolt C VA chart for all patients. Stereoacuity was evaluated using the TNO test (TNO: Laméris Ootech B.V., Netherlands) or the JACO stereo tests (JACO: T.M.I. Company, Saitama, Japan) (Figures 1a and b). Both methods used near stereoacuity test charts created using the random-dot stereogram that is less affected by monocular cues and conducted at a test distance of 40 cm. TNO red-green and JACO red-blue glasses were used for the binocular separation method. The binocular disparity consists of six steps for both TNO (480, 240, 120, 60, 30, and 15 arcseconds) and JACO (960, 480, 240, 120, 60, and 30 arcseconds). Both test charts have two figures to evaluate each binocular disparity. Thus, the disparity with which both charts were answered correctly was judged as the minimum disparity.
 |
Figure 1 Structure of JACO stereo test and evaluation decisions. (a) Overall view of the test chart. The test chart consists of four plates: plate I (disparity-free figure and 960 seconds), plate II (480 and 240 seconds), plate III (120 and 60 seconds), and plate IV (30 seconds and suppression detection figure). (b) Shapes and sizes of the three-dimensional (3D) figures. The size of the 3D figure is 4.0°. (c) Suppression detection figure. The size of the outer circle is 4.0° in visual mark size, and within it are figures that can detect suppression at 0.5° in visual mark size and 1.0° in visual mark size. The two circles in the center are the one visible to the right eye and the other one visible to the left eye. (d) Evaluation of suppression. When the red-blue glasses are worn, with the blue glass for the right eye and red glass for the left eye, the circle appears 3D without suppression if the circle with a visual mark size of 1.0° is in the center of the figure. However, when there is suppression, the circle is not in the center of the figure. If it is shifted to the right, the right eye is judged to have suppression, and if it is shifted to the left, the left eye is judged to have suppression. When the circle is not in the center but shifted to the right or left, the circle does not appear 3D. |
The central suppression test was performed using the detection figures of JACO (visual mark size: 0.5° and 1.0°) or circle No. 1 (visual mark size: 0.7°) of the Stereo Fly Test (Stereo Optical Inc., Chicago, IL, USA) to evaluate the presence or absence of suppression. The evaluation of suppression using JACO was examined as follows. The configuration of the suppression detection figure was as follows: the size of the outer circle of the figure was 4.0° in visual mark size, and there are two small figures with 0.5° and 1.0° in visual mark size within the circle that could detect suppression (Figure 1c). The binocular disparity of the suppression detection figure was 1920 seconds. At the beginning of the test, we showed the figure with a visual mark size of 1.0° and asked the patients if they can see one or two circles in the center. If the reply was “one”, we confirmed whether the circle was at the center of the figure or shifted to the right or left from the center. The evaluation of suppression is shown in Figure 1d. If no suppression was present at the visual mark size of 1.0°, the presence or absence of suppression was confirmed at a visual mark size of 0.5°. We also evaluated suppression using circle No. 1 of the Stereo Fly Test. Circle No. 1 is usually used as a stereoacuity test chart, but it can also be used to detect suppression. One circle in Circle No. 1 has a visual mark size of 0.7° and a binocular disparity of 800 seconds. Among the four circles, we evaluated whether any upper or lower circles were on a straight line. The evaluation of the suppression is shown in Figure 2.
 |
Figure 2 Evaluation of suppression using circle No. 1 of the Stereo Fly Test. When the upper and lower circles are aligned on a straight line, there is no suppression, and the lower circle appears three-dimensional. However, when there is suppression, the upper and lower circles are not aligned on a straight line, and if the lower circle is shifted to the right of the upper circle, the right eye is judged to have suppression, and if it is shifted to the left, the left eye is judged to have suppression. |
Changes in stereoacuity and suppression over time were evaluated at the following time points: before the start of occlusion therapy, when the highest VA in the amblyopic eye was first achieved, during the occlusion-tapering period, at the end of the occlusion therapy, and at the final visit.
The association between the amblyopia treatment periods and stereoacuity or suppression was analyzed using the Chi-square test for independence, whereas the association between stereoacuity and suppression was analyzed using Fisher’s exact test. A P-value <0.05 was considered statistically significant, and 4-Step Excel Statistics 4th edition (OMS Publishing, Tokyo, Japan) was used for the statistical analyses.
Results
The mean spherical equivalent values for the fellow and amblyopic eyes were +2.37 D ± 1.45 D and +5.26 D ± 1.91 D, respectively, whereas the mean anisometropia was +2.89 D ± 1.24 D (Table 1).
 |
Table 1 Characteristics of Study Patients |
Changes in the VA in the Amblyopic Eye and Suppression During Occlusion Therapy
The corrected VA of the amblyopic eye was 0.31 ± 0.17 logMAR before occlusion, which improved to ≥0.0 logMAR in all patients when the highest VA was achieved. No patient experienced any regression in the VA in the amblyopic eye at the last visit. The corrected VA of the fellow eye was −0.07 ± 0.06 logMAR before the occlusion therapy. Before occlusion, suppression of the amblyopic eye was present in 13 out of 19 patients (68.4%). This decreased to eight patients (42.1%) when the highest VA was achieved and five patients (26.3%) during the tapering period. Suppression disappeared in all patients at the final visit (Figure 3). All suppressions observed during the course of treatment were those found in the amblyopic eye. There was a significant association between the presence of suppression and each period of amblyopia therapy (P <0.01, Chi-square for independence test).
 |
Figure 3 Changes in the amblyopic visual acuity and suppression during occlusion therapy. The upper line graph shows the progression of VA in the amblyopic eye, while the lower bar graph shows changes in the ratio of patients with and without suppression. Suppression of the amblyopic eye was found in 42.1% of patients, even at the highest VA (≥0.0 logMAR) but disappeared in all the patients at the final visit. Abbreviation: VA, visual acuity. |
Progression of Stereoacuity During Occlusion Therapy
We examined the progression of stereoacuity in 13 patients who experienced suppression before therapy (Figure 4). Prior to occlusion therapy, five of the 13 patients (38.5%) had no stereoacuity, five (38.5%) had stereoacuity ranging from 960 to 240 arcseconds, and three had stereoacuity of 120 arcseconds (23.1%). At the time when the highest VA was achieved, a stereoacuity of 120 arcseconds or better was observed in nine patients (69.2%), which improved further during both the tapering period and at the end of occlusion therapy. At the end of the occlusion therapy and at the last visit, stereoacuity was 120 arcseconds or better in 12 patients (92.3%), among whom nine had an initial value of 60 arcseconds. There was a significant association between the acquisition of stereopsis better than 120 arcseconds during each treatment period (P <0.01, Chi-square for independence test), indicating that stereopsis improved over the course of therapy.
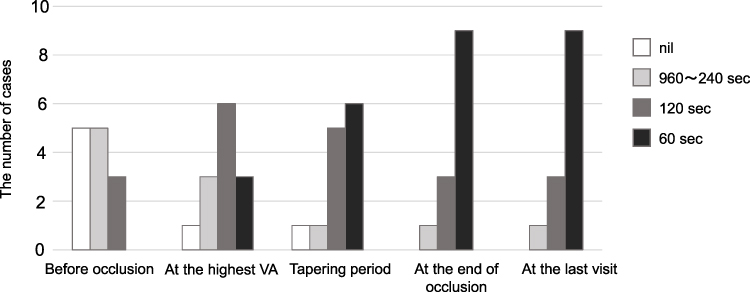 |
Figure 4 Progression of stereoacuity during occlusion therapy. More patients achieved a favorable stereoacuity of 120 arcseconds or better at the end of occlusion therapy than at the time of the highest VA. Abbreviations: sec, seconds of arc; VA, visual acuity; nil, no stereoacuity. |
The duration of treatment was 3.3 ± 3.2 (range: 1−11) months from the pre-occlusion period to the time when the highest VA was achieved, 3.4 ± 0.7 (range: 3−5) months from the time when the highest VA was achieved to the end of occlusion therapy, and 5.0 ± 4.0 (range: 1−14) months from the end of occlusion therapy to the final visit.
Association Between Stereoacuity and Suppression in Occlusion Therapy
Figure 5 shows the acquisition rate of favorable foveal stereopsis better than 60 arcseconds and the changes in suppression over time in the 13 patients who had suppression before starting occlusion therapy. When suppression disappeared, 10 patients (76.9%) experienced a further improvement in stereoacuity, and nine achieved foveal stereopsis. Regardless of the length of treatment, foveal stereopsis was not observed in patients with suppression. A significant correlation was found between foveal stereopsis and suppression at the time of reaching the highest VA and during the tapering period (P <0.05, Fisher’s exact test).
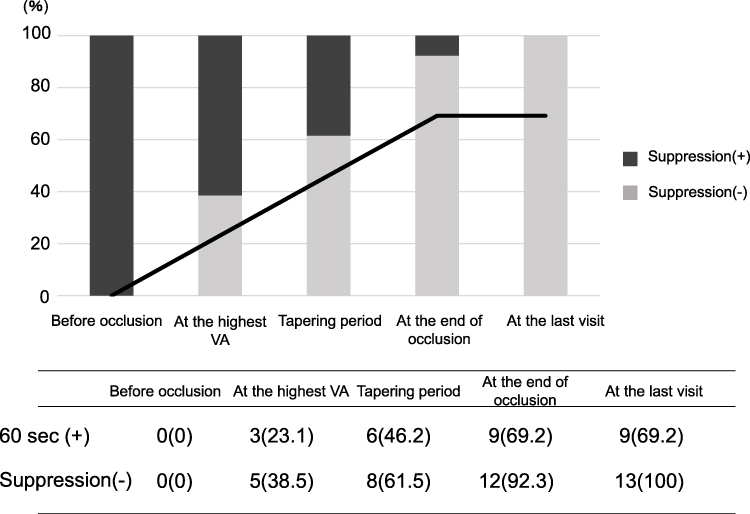 |
Figure 5 The association between the acquisition of foveal stereopsis and suppression in occlusion therapy. The upper line graph shows the percentage of patients who achieved 60 arcseconds of foveal stereopsis. The lower table shows the number of patients who achieved 60 arcseconds of foveal stereopsis and those who did not show suppression at each treatment period. Foveal stereopsis of 60 arcseconds was achieved after the suppression disappeared. Abbreviations: sec, seconds of arc; VA, visual acuity. |
Discussion
This study demonstrated that patients with anisometropic amblyopia experienced suppression of amblyopic eyes through occlusion therapy even when the VA in the amblyopic eye reached the highest score of ≥0.0 logMAR. Suppression of amblyopic eyes disappeared as the occlusion hours gradually decreased and stereoacuity improved further. These findings indicate that although the fellow eye remained superior under binocular vision conditions even after VA was equivalent in both eyes, suppression was eliminated by gradually releasing both eyes, which led to the acquisition of foveal stereopsis.
Regarding suppression of anisometropic amblyopia in our study, although the VA in the amblyopic eye improved to over 0.0 logMAR in all patients after occlusion therapy, suppression of the amblyopic eye was observed even when the highest VA was achieved; this is consistent with the findings of a previous study.11 In addition, Nakamura and Araki et al reported that there were cases in which the VA in the amblyopic eye improved to ≥0.0 logMAR under monocular conditions but decreased under binocular conditions. They concluded that it was due to the suppression applied to the amblyopic eye from the fellow eye.19,20 These results indicate that even if the VA in the amblyopic eye improves, the fellow eye remains superior because the amblyopic eye is suppressed.
It is known that stereoacuity in patients with unilateral amblyopia cannot be obtained when the difference in VA between the two eyes is large at the beginning of the amblyopia treatment,21 but it improves as the VA in the amblyopic eye improves.6–9 However, in our study, the highest stereoacuity was not achieved even when the VA in the amblyopic eye was ≥0.0 logMAR, but stereoacuity showed further improvement when the amblyopic eye was no longer suppressed. In particular, we found that the reduction of suppression of the amblyopic eye was associated with the acquisition of foveal stereopsis. Regarding the differences in suppression in each treatment stage, we believe that the suppression before reaching 0.0 logMAR reflects poor visual development due to an unclear image formed on the fovea of the amblyopic eye. Moreover, the suppression after reaching 0.0 logMAR indicates that suppression still remains in the amblyopic eye because the superiority of the fellow eye is too strong for both eyes to be used equally when they are open and to be free from suppression, even if VA measured by one eye after another is equal between the fellow and amblyopic eyes. Therefore, it is difficult to acquire foveal stereopsis for 60 seconds if the suppression of the amblyopic eye remains. These findings suggest that to acquire foveal stereopsis, the superiority of the fellow eye must disappear after the improvement of VA under binocular conditions, and the suppression of the amblyopic eye must be eliminated by the interaction of both eyes.
Based on the course of occlusion therapy, we found that suppression of the amblyopic eye, which persisted even after the improvement in VA, could be reduced by gradually decreasing the duration of occlusion, thereby stabilizing the amblyopic eye. This gradual reduction plays a significant role not only in preventing the regression of VA in the amblyopic eye22 but also in eliminating suppression and improving subsequent stereoacuity. We believe that suppression of the amblyopic eye can be eliminated when, by gradually decreasing the duration of occlusion, the amblyopic eye becomes actively involved in the binocular function, and the activity of the amblyopic eye becomes equivalent to that of the fellow eye. Based on these findings, we believe that it is essential to focus on the state of the amblyopic eye under binocular vision in the final stage of occlusion therapy and encourage the amblyopic eye to function as well as the fellow eye under everyday visual conditions by decreasing the duration of occlusion.
Moreover, one possible reason why suppression was reduced by gradually decreasing the duration of occlusion could be due to the therapeutic effect of refractive correction. It takes approximately 3–4 months for refractive correction to show improvement in VA.23,24 However, in the present study, the maximum treatment period of wearing glasses before the start of the occlusion therapy was only 2 months. Refractive correction not only reduces blurring of retinal images in both eyes, but also reduces the interocular refractive imbalances. Therefore, refractive adaptation may have reduced suppression. Yap et al conducted electrophysiological evaluations and showed that interocular suppression can be reduced by correcting glasses alone.25,26 Thus, we believe that it is important to gradually decrease the duration of occlusion in the final stage of occlusion therapy.
There are some limitations to this study. First, the sample size of our study was small due to the retrospective nature of the study. Several studies have shown that suppression of amblyopic eyes decreases stereoacuity11–13,15,16 and Webber et al27 reported that suppression affected stereoacuity more than VA. However, no other studies have investigated the relationship between VA, suppression, and stereoacuity during the course of amblyopia treatment, even in a limited number of patients. Thus, we believe our study is clinically significant in that we revealed changes in suppression caused by occlusion therapy. We believe that the results of this study will help clinicians make clear decisions regarding when to terminate the occlusion therapy based not only on the VA in the amblyopic eye but also on suppression. In the future, we hope to conduct a prospective study involving a large number of patients to evaluate stereoacuity and suppression at each visit to consider the optimal timing to end occlusion therapy as well as develop appropriate treatment plans. In addition, we are planning to observe in detail the changes in the size and depth of suppression caused by the amblyopia treatment. Second, confirmation of the implementation of occlusion was self-reported. Moreover, previous studies using occlusion dose monitors reported poor compliance with occlusion therapy.28 We explained the need for occlusion in detail to patients and their parents to increase compliance. However, we believe that treatment by correcting glasses alone should be considered when compliance is extremely poor.
Conclusion
Suppression of the amblyopic eye was observed even when the highest VA in the amblyopic eye was achieved, but it could be reduced by gradually decreasing the duration of occlusion. Reduction of suppression was found to be associated with the acquisition of foveal stereopsis.
Funding
There is no funding to report.
Disclosure
The authors report no conflict of interest.
References
1. Von Noorden GK. Factors involved in the production of amblyopia. Br J Ophthalmol. 1974;58(3):158–164. doi:10.1136/bjo.58.3.158
2. Von Noorden GK. Classification of amblyopia. Am J Ophthalmol. 1967;63(2):238–244. doi:10.1016/0002-9394(67)91543-7
3. Bradfield YS. Identification and treatment of amblyopia. Am Fam Phys. 2013;87(5):348–352.
4. Webber AL, Wood JM, Gole GA, Brown B. The effect of amblyopia on fine motor skills in children. Invest Ophthalmol Vis Sci. 2008;49(2):594–603. doi:10.1167/iovs.07-0869
5. O’Connor AR, Birch EE, Anderson S, Draper H. The functional significance of stereopsis. Invest Ophthalmol Vis Sci. 2010;51(4):2019–2023. doi:10.1167/iovs.09-4434
6. Lee SY, Isenberg SJ. The relationship between stereopsis and visual acuity after occlusion therapy for amblyopia. Ophthalmology. 2003;110(11):2088–2092. doi:10.1016/S0161-6420(03)00865-0
7. Awadein A, Fakhry MA. Changes in binocular function in anisometropic nonstrabismic children with optical correction and occlusion therapy. J AAPOS. 2011;15(6):545–550. doi:10.1016/j.jaapos.2011.07.008
8. Sen DK. Results of treatment of anisohypermetropic amblyopia without strabismus. Br J Ophthalmol. 1982;66(10):680–684. doi:10.1136/bjo.66.10.680
9. Chung YW, Park SH, Shin SY. Distant stereoacuity in children with anisometropic amblyopia. Jpn J Ophthalmol. 2017;61(5):402–407. doi:10.1007/s10384-017-0518-9
10. Wallace DK, Lazar EL, Melia M, et al. Stereoacuity in children with anisometropic amblyopia. J AAPOS. 2011;15(5):455–461. doi:10.1016/j.jaapos.2011.06.007
11. Yagasaki T, Suzuki M, Matsuura H, et al. Binocular function in anisometropic amblyopia. Jpn Rev Clin Ophthalmol. 2011;97(5):377–382.
12. Li J, Thompson B, Lam CS, et al. The role of suppression in amblyopia. Invest Ophthalmol Vis Sci. 2011;52(7):4169–4176. doi:10.1167/iovs.11-7233
13. Firth AY, Stevenson C. Depth of suppression in anisometropic amblyopia (with or without microtropia). Binocul Vis Strabolog Q Simms Romano. 2012;27(3):187–194.
14. Chen Y, He Z, Mao Y, Chen H, Zhou J, Hess RF. Patching and suppression in amblyopia: one mechanism or two? Front Neurosci. 2019;13:1364. doi:10.3389/fnins.2019.01364
15. Sehgal S, Satgunam P. Quantifying suppression in anisometropic amblyopia with VTS4 (Vision therapy system 4). Transl Vis Sci Technol. 2020;9(12):24. doi:10.1167/tvst.9.12.24
16. Li J, Hess RF, Chan LY, et al. Quantitative measurement of interocular suppression in anisometropic amblyopia: a case-control study. Ophthalmology. 2013;120(8):1672–1680. doi:10.1016/j.ophtha.2013.01.048
17. Philipp W, Mayer W. Investigation of visual field defects in strabismic and anisometropic amblyopes with the Octopus program G1. Graefes Arch Clin Exp Ophthalmol. 1989;227(5):448–454. doi:10.1007/BF02172897
18. Li J, Li J, Chen Z, et al. Spatial and global sensory suppression mapping encompassing the central 10° field in anisometropic amblyopia. Invest Ophthalmol Vis Sci. 2017;58(1):481–491. doi:10.1167/iovs.16-20298
19. Nakamura H, Ohno E, Matsumoto F, et al. Usefulness of occlusion partielle in the amblyopia treatment at the last stage of occlusion therapy. Jpn Orthopt J. 1990;18:116–119. doi:10.4263/jorthoptic.18.116
20. Araki S, Miki A, Goto K, et al. Visual acuity of amblyopic eye under binocular condition and stereopsis in anisometropic amblyopia. Kawasaki Med J. 2020;46:21–25.
21. Hirai Y, Awaya S. Studies on visual acuity and stereoacuity. Folia Ophthalmol Jpn. 1985;36(8):1524–1531.
22. Holmes JM, Beck RW, Kraker RT, et al. Risk of amblyopia recurrence after cessation of treatment. J AAPOS. 2004;8(5):420–428.
23. Cotter SA; Pediatric Eye Disease Investigator Group. Treatment of anisometropic amblyopia in children with refractive correction. Ophthalmology. 2006;113(6):895–903. doi:10.1016/j.ophtha.2006.01.068
24. Stewart CE, Moseley MJ, Fielder AR, Stephens DA. Refractive adaptation in amblyopia: quantification of effect and implications for practice. Br J Ophthalmol. 2004;88:1552–1556. doi:10.1136/bjo.2004.044214
25. Yap TP, Boon MY. Electrodiagnosis and treatment monitoring of children with refractive amblyopia. Adv Ophthalmol Optom. 2020;5:1–24. doi:10.1016/j.yaoo.2020.04.001
26. Yap TP, Luu CD, Suttle C, Chia A, Boon MY. Effect of stimulus orientation on visual function in children with refractive amblyopia. Invest Ophthalmol Vis Sci. 2020;61(5):1–12. doi:10.1167/iovs.61.5.5
27. Webber AL, Schmid KL, Baldwin AS, Hess RF. Suppression rather than visual loss limits stereoacuity in amblyopia. Invest Ophthalmol Vis Sci. 2020;61(6):1–8. doi:10.1167/iovs.61.6.50
28. Awan M, Proudlock FA, Gottlob I. A randomized controlled trial of unilateral strabismic and mixed amblyopia using occlusion dose monitors to record compliance. Invest Ophthalmol Vis Sci. 2005;46(4):1435–1439. doi:10.1167/iovs.04-0971
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.