Back to Journals » Psychology Research and Behavior Management » Volume 15
The Association Between General Self-Efficacy and Depressive Symptoms in People with Type 2 Diabetes Mellitus: The Mediating Role of Coping Styles Preference
Authors Li Q, Chen Y, Välimäki M, Long Q, Yang J, Guo J ![]()
Received 9 July 2022
Accepted for publication 1 September 2022
Published 8 September 2022 Volume 2022:15 Pages 2501—2511
DOI https://doi.org/10.2147/PRBM.S381742
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Igor Elman
Qingting Li,1,* Yao Chen,1,* Maritta Välimäki,1 Qing Long,1 Jundi Yang,2 Jia Guo1
1Xiangya School of Nursing, Central South University, Changsha, 410013, People’s Republic of China; 2School of Nursing, the University of Hong Kong, Pokfulam, 999077, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Jia Guo, Email [email protected]
Background: Depressive symptoms are prevalent in persons with type 2 diabetes mellitus and related with poor disease outcomes. Both general self-efficacy and coping style are associated with depressive symptoms. A model about proactive coping indicates that coping style plays a mediation role between general self-efficacy and depressive symptoms. But, empirical evidence is missing about this potential mediation relationship which may be a barrier of taking precise strategies for relieving depressive symptoms.
Objective: This study aims to investigate the prevalence of elevated depressive symptoms in persons with type 2 diabetes mellitus and explore whether coping style preference mediates the association between general self-efficacy and depressive symptoms.
Methods: This was a secondary data analysis of a cross-sectional survey (June–July 2017) among 721 persons with type 2 diabetes mellitus (45.4% male and 54.6% female) aged from 22 to 96 years old. Data on general self-efficacy, coping style preference and depressive symptoms were collected using validated questionnaires in hospital setting. The mediation model was tested using the bootstrapping (K=5000) in the MPlus program version 7.4. The results were reported following the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines.
Results: The prevalence of elevated depressive symptoms was 58% (n = 418) among persons with type 2 diabetes mellitus at hospital setting. A higher level of general self-efficacy was related to less depressive symptoms via positive coping preference (p < 0.01).
Discussion: About two-thirds of persons with type 2 diabetes mellitus experienced elevated depressive symptoms during hospitalization. The intervention elements, including strengthening general self-efficacy and promoting positive coping, are promising to decrease their depressive symptoms.
Keywords: type 2 diabetes mellitus, depressive symptoms, self-efficacy, coping style, mediation analysis
Plain Language Summary
What Does This Paper Contribute to the Wider Global Clinical Community?
- Nurses should screen depressive symptoms routinely among persons with type 2 diabetes mellitus, especially those in hospital setting.
- The level of general self-efficacy and coping style preference are suggested to be subsequently assessed once the elevated depressive symptoms are identified.
- Nurses should incorporate coping skills training as the key element of the interventions to relieve or prevent depressive symptoms among persons with type 2 diabetes mellitus.
Introduction
Globally, it is estimated that 537 million people have diabetes in 2021, and this number is projected to reach 783 million by 2045.1 The disease places a huge burden on individuals as well as social communities and government because of its physical and psychological comorbidities.2 Depression is a common comorbidity of type 2 diabetes mellitus (T2DM) with a prevalence of 38%.2 According to a meta-analysis that includes studies from Northern America, Europe, Asia and Latin America, persons with T2DM have a 1.41–1.43 relative risk for depression compared with the general population.3 The worldwide prevalence of elevated depressive symptoms among persons with T2DM varies from 7.5% to 44.3%,4,5 whereas it ranged from 16.8% to 53.8% among hospitalized patients due to the severity and complexity of disease.6–9 The condition of depression or elevated depressive symptoms could worsen glycaemic control which in turn may exacerbate their depressive status.10
The factors associated with depressive symptoms in persons with T2DM have received increasing attention in the literature and clinical guidelines.11,12 The development of interventions for reducing depressive symptoms will not succeed without considering comprehensively associating factors of depressive symptoms among a specific population.12 Notably, sociodemographic and clinical factors, such as older age, female and lower education level, longer diagnosis duration, depressive disorder history, higher body mass index and other diabetes complications are associated with elevated depressive symptoms in persons with T2DM.13–15 Recent studies showed that psychological factors, such as childhood adversity, negative life events, chronic stresses, negative illness perceptions, and limited social support, are recognised as risk factors of elevated depressive symptoms.15,16 In addition, other psychological factors, including low general self-efficacy and negative coping style, are associated with elevated depressive symptoms.11,12,17
General self-efficacy is a protective factor against depressive symptoms among persons with T2DM in Taiwan and Western countries.18,19 General self-efficacy is a person’s own belief in their capability to commit an action described as a self-regulatory process that affects the motivation of an individual to engage in behavioural change.20 Persons with T2DM who have a low level of general self-efficacy are less likely to undertake daily diabetes self-management behaviours, subsequently causing poor blood glucose control.18,21 In these cases, blood glucose may fluctuate more frequently, making them feel overwhelmed, frustrated and disengaged, which may be associated with elevated depressive symptoms.18
Coping styles are referred as maintenance of the response and adjustments to stress during the course of diabetes, which are also associated with depressive symptoms among persons with T2DM.22–24 The coping styles are often categorised as positive and negative coping.25 Positive coping refers to coping methods that involve assuming responsibility for managing one’s stress, which include efforts to function normally despite stress, while negative coping refers to approaches that involve turning over the responsibility of managing stress to external sources and allowing one’s life to be negatively influenced by stress.26 People can use both of the two coping styles simultaneously, but the coping style preference often predicts either positive coping or negative coping they may take under specific stress, which is widely measured by sound psychological instruments.27 A study conducted in China showed that positive coping preference was associated with less depressive symptoms among persons with T2DM (β = −0.314, p < 0.05).24 Negative coping preference was found associating with more depressive symptoms among persons with T2DM in Japan and Canada.22,23
There is evidence showing that general self-efficacy and coping style preference are correlated. In Jordan, America and China, general self-efficacy was reported positively associating with positive coping preference (adaptive coping) and negatively associated with negative coping preference (eg, maladaptive coping, avoiding) among persons with T2DM.28–31 Taken together, among persons with T2DM, general self-efficacy, coping style preference and depressive symptoms are inter-correlated.
Consistently, according to a model about proactive coping proposed in 2012, positive coping could be a partial mediator between human resources, self-efficacy, optimism and treatment outcomes (satisfaction with life and depression).32 This mediation effect has been demonstrated among persons with HIV, showing that negative coping preference links the negative association between general self-efficacy and depressive symptoms.33,34 Among persons with T2DM, stress, negative emotions or feelings related to the life-lasting disease management are widely identified, they use personally preferred coping very often.33,35 There may be similar mediating role of coping style preference existing in the relationship between general self-efficacy and depressive symptoms among persons with T2DM. However, limited empirical evidence is available about the reciprocal relationship, which may be a barrier of taking precise strategies for relieving depressive symptoms among this specific population. To fill this knowledge gap, we aimed to explore whether coping style preference is the mediator between general self-efficacy and depressive symptoms. We hypothesised that 1) general self-efficacy is negatively related to depressive symptoms, and positive coping preference is associated with lower depressive symptoms while negative coping preference is associated with higher depressive symptoms; 2) a higher level of general self-efficacy is related to lower depressive symptoms via positive coping preference.
Materials and Methods
This study involved a secondary data analysis of a cross-sectional survey to explore the associating factors of adherence of self-monitoring of blood glucose in China which has been published elsewhere.16 It was reviewed and approved by the Ethical Review Board of our university (NO.2018012). This study followed the Strengthening the Reporting of Observational studies in Epidemiology Checklist for cross-sectional studies (STROBE 2020, Supplementary File 1) guidelines which aimed to ensure quality and specification of study reporting.36
Study Participants and Recruitment
A total of 721 participants with age of 18 years and above, diagnosed with T2DM for at least three months and able to understand and communicate in Chinese were considered eligible. Persons with severe diabetes complications which caused serious bodily malfunction, such as severe diabetic nephropathy, retinopathy or cognitive impairment or dysphrenia, were excluded. More details about the participants were described elsewhere.16 The sample size of 721 provided sufficient power (0.846) to detect an effect size of 0.025 (between small and medium), which was defined as the ratio of variance explained by the addition of a single predictor divided by the error variance.
This study was conducted in two hospitals in Changsha, which is the capital city of Hunan province in China, with a population of more than 7 million, 20 tertiary hospitals (with 11 endocrinology wards) and 84 secondary hospitals (with 4 endocrinology wards). A tertiary and a secondary hospital were randomly selected in the study. Four wards from each hospital, including one endocrinology ward and three non-endocrinology wards (hepatobiliary surgery, nephrology and general survey ward; respiratory, cardiology and neurology ward), were included. To control sampling bias, we used simple random sampling to select three non-endocrinology wards in each hospital.
The participants were recruited by trained nurses who worked in the study hospitals between June and July 2017. The nurses offered a flyer that describes the study to every new patient admitted in the study wards. They also checked patients for eligibility to join the study on the basis of the inclusion and exclusion criteria. Patients who met the inclusion criteria were invited to join the study. Once they showed interest to participate, the research assistant met with the patients to provide detailed information about the study. If the patients refused to join, their demographic data were collected for the intention-to-treat analysis with informed consent.
Data Collection
The data were collected from persons with T2DM in hospitals by the research assistants. Within 24 hours after the patients agreed to participate in this survey, the online self-report validated Chinese language questionnaires (https://www.wjx.cn/jq/19820102.aspx) were administered at bedside via tablets with the help of the research assistants. The participants completed the questionnaires by themselves. The research assistant explained the questions and helped in operating the questionnaire application system when needed.
Instruments
Data were collected on sociodemographic and clinical characteristics, depressive symptoms (dependent variable), general self-efficacy (independent variable) and coping styles preference (mediation variables).
Sociodemographic and Clinical Characteristics
Demographic information about persons’ sociodemographic characteristics including age, gender, marital status, education level, personal monthly income, occupation and medical insurance were collected. Clinical characteristics included family history of diabetes, diabetes-related complications, other chronic diseases, and treatment regimen.
Depressive Symptoms
The Center for Epidemiologic Studies Depression Scale (CES-D, Chinese version)17 was used to measure the depressive symptoms. The scale includes 20 items with a total score range of 0–60, in which higher scores indicate more depressive symptoms. A cut-off score ≥21 was used to define depressive symptoms based on the optimum balance between sensitivity and specificity among people with T2DM in China. The CES-D demonstrated high internal consistency (Cronbach’s α = 0.85) for Chinese people with T2DM.17 In this data set, Cronbach’s α was 0.892.
General Self-Efficacy
The general self-efficacy scale (GSES, Chinese version)37 was used to measure self-efficacy. The scale measures the degree of self-confidence of individuals when encountering difficulties. The GSES has 10 items with a four-point Likert scale (1 = totally wrong, 4 = entirely correct). Examples of statements are “I can always manage to solve difficult problems if I try hard enough” (item 1) and “I am certain that I can accomplish my goals” (item 3). The responses on each statement are then summed up to a total score, ranging from 10 to 40, with higher scores indicating higher general self-efficacy. In this data set, Cronbach’s α was 0.932.
Coping Style Preference
The 20-item simplified coping style questionnaire (SCSQ, Chinese version)25 was used to determine coping style preference. This self-report questionnaire measures the action that people often take in daily life to manage specific internal and/or external sources of psychological stress. The questionnaire has two subscales: positive coping (12 items) and negative coping (8 items).38 All items are rated using a four-point Likert-type scale (0 = never, 1 = occasionally, 2 = sometimes, 3 = frequently). Each respondent’s coping style preference is determined based on the difference between the Z-converted standard score for positive coping and the Z-converted standard score for negative coping. If the difference score was higher than 0, the respondent has a positive coping preference; otherwise, the respondent has a negative coping preference.39 In this way, coping style preference was expressed as a dichotomous variable in this study. The SCSQ has demonstrated high internal consistency (Cronbach’s α = 0.90) and a reliability of 0.89.
Ethical Consideration
We obtained the permission from the hospitals to conduct this study. The participants were informed of the aims of the study, including predetermined analyses of psychological factors. They signed an informed consent form to indicate their willingness in participating in the study. The procedures performed were in accordance with the Declaration of Helsinki.
Data Analysis
Descriptive statistics was utilised for the demographic characteristics, general self-efficacy, coping style, and depressive symptoms of the participants. Double-entry data method was adopted to ensure the accuracy of data. Descriptive statistics on the background information were formulated to present demographic and other characteristics. Comparisons of these variables were analyzed by the Chi-squared test. To examine the relationships between general self-efficacy, coping style preference and depressive symptoms, we determined the Pearson correlations. All participants with one or more missing values on the independent variables were excluded from the multivariate analyses. Data analysis was performed using SPSS (version 22.0; SPSS Inc., Chicago, IL).
Considering that this study involved secondary analysis data, the simulation in Mplus was conducted to obtain a post-hoc power of the mediation hypothesis, as presented in the Monte Carlo study.40 An alpha of value of 0.01 rather than 0.05 was chosen to adjust for multiple tests. All study variables met the necessary assumption requirements of path analysis (multivariate normal distribution) after exploratory analysis and visual inspection of the data.40 Mediation analyses were examined to investigate indirect influences of general self-efficacy on depressive symptoms through the mediating mechanism of coping style. Variables that were statistically significant (p < 0.05) in the chi-square analyses were controlled as covariates in the mediation analysis. Bootstrapping (K = 5000) was used to examine indirect effects by using the model indirect command in the MPlus program (version 7.4)41. The goodness-of-fit indices, including the comparative fit index (CFI, >0.90), Tucker Lewis index (TLI >0.90) and root mean square error of approximation (RMSEA <0.05), were used to evaluate the model goodness of fit. We set two-tailed p values of 0.05 and used 1000 bootstrap samples to estimate direct, indirect and total effects. If zero was not included in the 95% bias-corrected bootstrap CIs, then the effect was considered significant.
Results
Demographic and Clinical Characteristics of the Participants
Among the 795 patients eligible for this study, 753 (94.5%) were willing to join, while 42 (5.5%) declined because of lack of interest. A total of 32 (4.1%) forms were left empty, leaving 721 (90.7%) completed surveys. In total, 721 met the inclusion criteria for this study. No significant difference was observed between the participants and the people who declined in terms of age, gender, educational level and treatment regime (p > 0.05). Among the 721 participants, 54.6% were female. Ages of all participants in this study ranged from 22 to 96, with a mean age of 56.94. Most participants were married (n = 627, 87.0%), and 63.1% (n = 455) finished middle school at most. Over one-third (34.5%, n = 249) were treated with diet and/or exercise therapy, 31.1% (n = 224) received oral hypoglycaemic agents and 34.4% (n = 248) received insulin therapy. In addition, 28.6% (n = 206) reported other chronic diseases such as hypertension, and 55.3% (n = 399) reported diabetes-related complications. More detailed data on the characteristics of the participants are provided in Table 1.
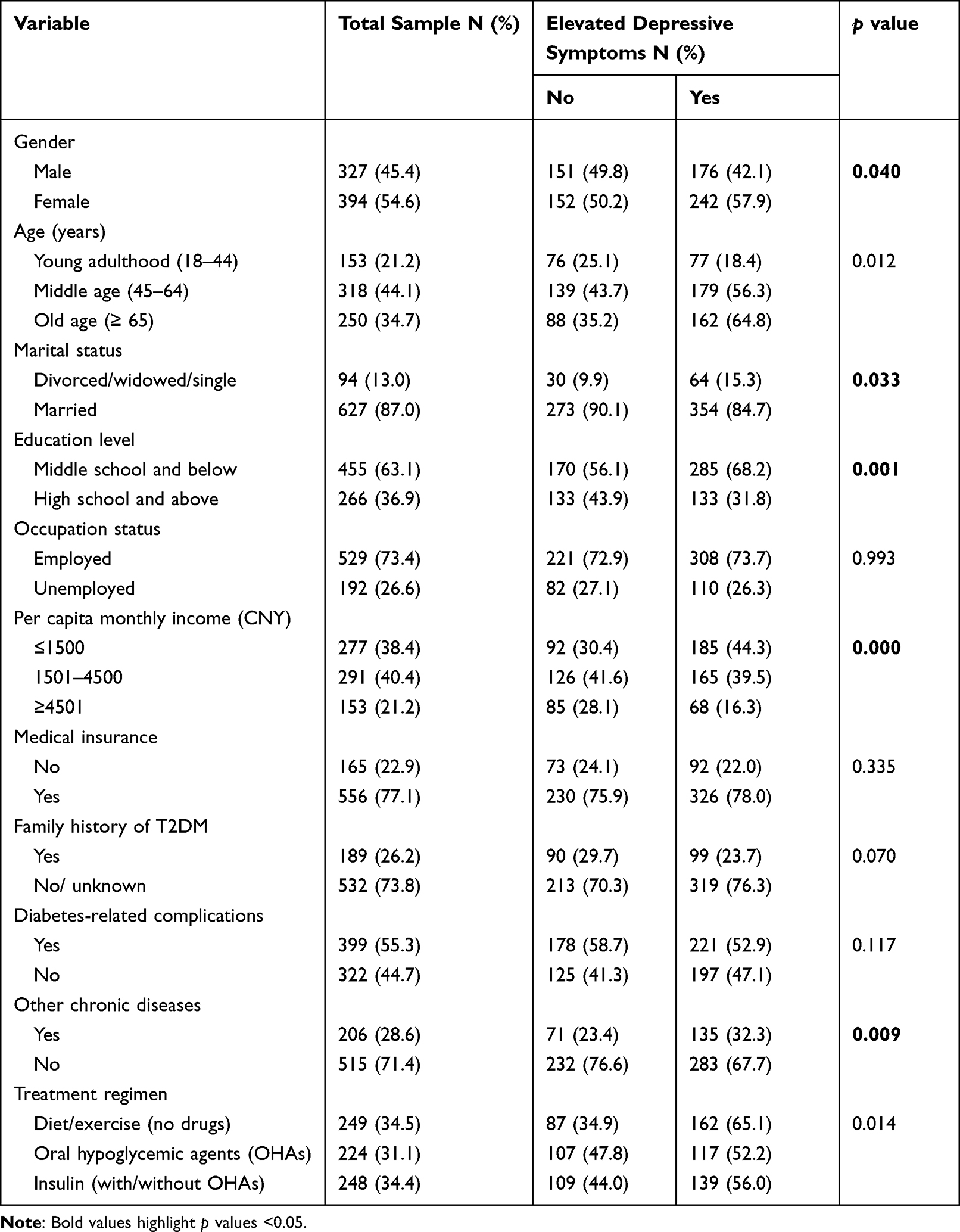 |
Table 1 Sample Demographic Characteristics (n = 721) |
Descriptive Characteristics of Depressive Symptoms, General Self-Efficacy and Coping Style Preference
The total CES-D score measuring depressive symptoms of all participants was 21.55 ± 7.76 (0–49). Based on the cut-off score ≥21, over half reported depressive symptoms (n = 418, 58.0%). The general self-efficacy score of all participants was 2.40 ± 0.59 (1–4). The mean difference of the Z-converted standard positive and negative coping score was 1.41 ± 0.49 (>0), presenting a positive coping preference. Descriptive characteristics of the actual and potential score range of the four psychosocial variables are presented in Table 2.
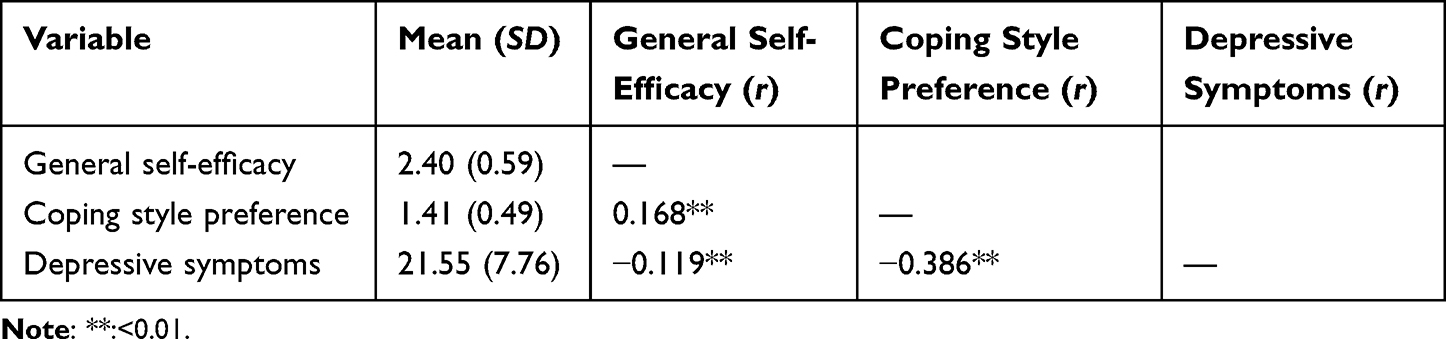 |
Table 2 Descriptive Information of General Self-Efficacy, Coping Style Preference, and Depressive Symptoms, and Pearson Correlation Analyses |
Correlations Among Depressive Symptoms, General Self-Efficacy and Coping Style Preference
The higher score of general self-efficacy was associated with less depressive symptoms (as a total score; r = –0.386, p < 0.01). The association between coping style preference and depressive symptoms was negatively significant (r = –0.119, p < 0.01). Furthermore, the association between general self-efficacy and coping style preference was positively significant (r = 0.168, p < 0.01). As coping style preference was a dichotomous variable, these results showed that positive coping preference was related to less depressive symptoms, and higher general self-efficacy was related to positive coping preference; and vice versa. No evidence of multicollinearity was observed between general self-efficacy, coping style preference and depressive symptoms (r < 0.7).
Mediating Effect of Coping Style Preference on the Association Between General Self-Efficacy and Depressive Symptoms
The structural model was based on the hypothesised relationship between general self-efficacy, coping style preference and depressive symptoms. The data has met a good fit of the model (CFI = 1.000, TLI = 1.000 and RMSEA = 0.000; Figure 1). After controlling for gender, marital status, education level, per capita monthly income (CNY), and other chronic diseases, the regression coefficients from general self-efficacy to coping style preference were positively significant (β = 0.0339; 95% CI, 0.186~0.484; p < 0.01). The path coefficients from coping style preference to depressive symptoms were negatively significant (β = –0.481; 95% CI, −0.559~-0.387; p < 0.01). As with the correlation analysis, these results showed that higher general self-efficacy was related to positive coping preference, and then was associated with less depressive symptoms; and vice versa.
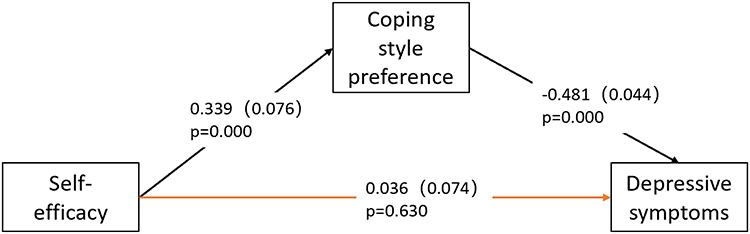 |
Figure 1 Mediation model for the effect of coping style preference on the relationships between general self-efficacy and depressive symptoms. Standardized coefficients and errors terms for the path is provided. Black lines indicate indirect effect. |
The analysis also showed that the total effect of general self-efficacy on depressive symptoms was not significant (β = −0. 127; 95% CI, −0.264~0.008; p > 0.05). The direct effect from general self-efficacy to depressive symptoms was not significant (β = 0.036; 95% CI, −0.114~0.178; p > 0.05). Therefore, the association between general self-efficacy and depressive symptoms was not statistically significant when coping style preference was controlled. However, higher general self-efficacy could indirectly and negatively influence depressive symptoms via coping style preference (β = −0.163; 95% CI, −0.245~-0.088; p < 0.05), showing that higher general self-efficacy was related to less depressive symptoms via positive coping preference, and vice versa. The results demonstrate that coping style preference completely mediated the association between general self-efficacy and depressive symptoms. The detailed information is shown in Table 3.
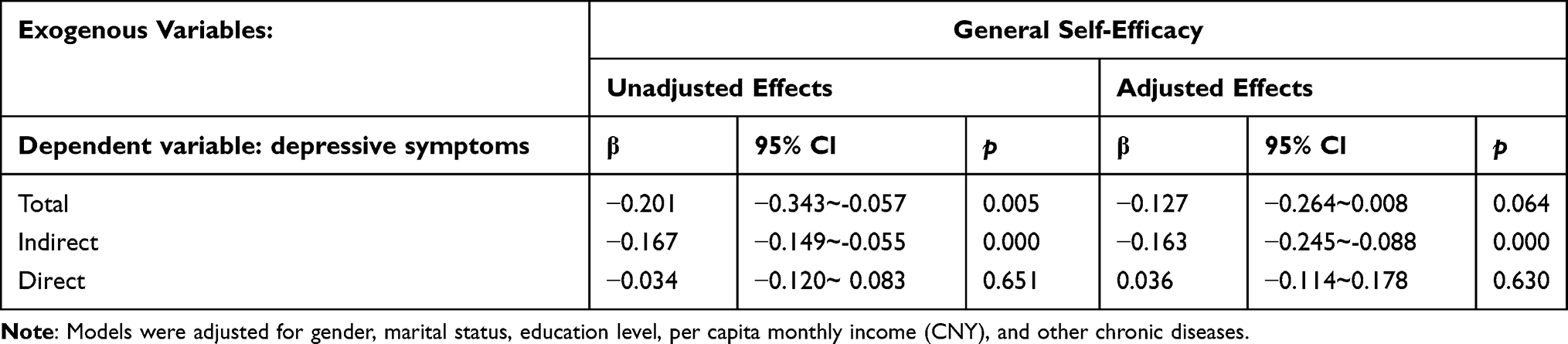 |
Table 3 Summary of Total, Indirect, and Direct Effects of General Self-Efficacy, Coping Style Preference, and Depressive Symptoms in a Mediation Model |
Discussion
We found that about 58% participants (N = 418) reported elevated depressive symptoms, which was similar to a study in Nanjing, China (51%)6 and Saudi Arabia (53.8%),9 but higher than the findings in the US (23.0%),42 Germany (23.0%)7 and Japan (16.8%)8 among persons with T2DM at hospital settings. The variety of the proportion could be explained by the diabetes care practice gap across health-care systems. To the best of our knowledge, this study first reported the empirical findings that higher level of general self-efficacy was related to less depressive symptoms via positive coping preference. Our findings highlight that if intervention elements on elevated depressive symptoms only involve improving general self-efficacy but not considering coping style preference, the effectiveness may not be satisfied. This result provides evidence to the proactive coping theory and extends scholarly and practical understanding on this mediation relationship among persons with T2DM.
In our study, persons with higher level of general self-efficacy preferred to use positive coping, which was consistent with the results of studies in Australia and Finland.43,44 Persons with higher self-efficacy often have the feeling of being effective in overcoming challenges and achieving desired goals.45 When surrounded with stressful events, they are more confident or motivated to relieve stress through adopting positive coping style, such as active coping, planning, positive revaluation and seeking emotional support.38
In this study, we found that positive coping preference was related to less depressive symptoms among persons with T2DM. It was consistent with a study which showed positive coping preference was protective factors of depressive symptoms among adults with diabetes.44 It can be interpreted from the perspectives of behaviours and personality. In terms of behaviours, persons who have positive coping preference may be more motivated and strive to seek help for solutions or communicate with others to release negative emotion.46,47 In terms of personality, persons who have positive coping preference are often optimistic and outgoing.48 They are more likely to offset the harm when setbacks and frustrations occur;46,49 subsequently, psychological problems such as depressive symptoms do not develop easily.50 Taken together, stress may be relieved by deploying positive coping, which could retard depressive symptoms.46,49
For persons who have preference to use negative coping, they may easily experience depressive symptoms. Indeed, previous studies among persons with T2DM have indicated that negative coping styles such as denial, self-blame, drinking and smoking might be associated with depressive symptoms.35,51 They may be less likely to seek help for their health problems and avoid medical visits, especially if medical visits made them feel overwhelmed or frustrated.33,52 They may ignore their disease condition and use relief what they can manage themselves such as alcohol or other substances.53 Overall, negative coping preference may accumulate failure and exacerbate stressful events, which will further trigger negative emotions, even depressive symptoms.46,49
Based on our results, a precise model of depressive symptoms management may be promising for persons with T2DM in clinical practice. First, in terms of the high prevalence of depressive symptoms among this population in a hospital setting, depressive symptoms should be routinely screened as recommended by the guideline of the American Diabetes Association.54 Second, the level of general self-efficacy and coping style preference should be assessed once elevated depressive symptoms are identified, with a purpose to specify the level of general self-efficacy and coping style preference to customize precise intervention elements. Finally, regarding the intervention elements of elevated depressive symptoms, for persons with a low level of general self-efficacy, health professionals could apply strategies to enhance general self-efficacy, and to encourage positive coping is recommended.55 Evidence showed that coping skills training could encourage more positive coping and promote better general self-efficacy which may be promising among persons with T2DM.56 This study also has some research implications: the need for additional research to identify strategies for increasing level of general self-efficacy and use of positive coping among persons with T2DM; future researches should seek to explore other potential mediators, such as social and family support, and psychological resilience.
This study has several limitations. First, participants were recruited from hospital setting, and the set-up may be different from patients in the community, thus limiting the generalisability of the results. Second, although we controlled the confounders, we were unable to include all the associating variables in a single study, such as diabetes distress or self-management. Hence, additional research is needed to examine the mediator and moderator variables in different cultural contexts. Third, this was a secondary data analysis, which limited the data available. Fourth, diabetes-specific self-efficacy was not measured, because the specific instrument of a Chinese version was not available. Fifth, self-report questionnaires may result in recall and reporting bias. Lastly, correlational study design did not equate to causation. The future studies need to determine causations.
Conclusion
About two-thirds of the people with T2DM at a hospital setting in China reported elevated depressive symptoms, which address the significant attention on psychological health during diabetes care practice. This study highlighted the mediating role of coping style preference between general self-efficacy and depressive symptoms among persons with T2DM, which was limited before. This finding suggests a promising approach to decrease depressive symptoms among persons with T2DM, including encouraging positive coping and enhancing general self-efficacy.
Abbreviation
T2DM, type 2 diabetes mellitus.
Data Sharing Statement
The datasets generated and analysed during the current study are not publicly available due to the confidentiality agreement with the participants. The data is however available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Ethical Review Board of Xiangya School of Nursing Central South University (NO.2018012). The procedures performed were in accordance with the Declaration of Helsinki. Potential participants were all informed about the study in writing and orally. The information described the purpose and process of the study, the method used and publication plans. The information also included confidentiality assurance, the principles for voluntary participation and included contact information to the researcher and organization behind the study. The written information also included a form for obtaining a written informed consent. All the participants signed and returned the written informed consent prior to participation.
Acknowledgments
We thank Sinocare Diabetes Foundation for improving public cognition of diabetes mellitus.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Innovation Project of Graduate Students of Central South University in 2021 (Number: 2021zzts1023).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. International Diabetes Federation. IDF Diabetes Atlas.
2. Lotfaliany M, Bowe SJ, Kowal P, Orellana L, Berk M, Mohebbi M. Depression and chronic diseases: co-occurrence and communality of risk factors. J Affect Disord. 2018;241:461–468. doi:10.1016/j.jad.2018.08.011
3. Yu M, Zhang X, Lu F, Fang L. Depression and risk for diabetes: a meta-analysis. Can J Diabetes. 2015;39(4):266–272. doi:10.1016/j.jcjd.2014.11.006
4. Bąk E, Marcisz-Dyla E, Młynarska A, Sternal D, Kadłubowska M, Marcisz C. Prevalence of depressive symptoms in patients with type 1 and 2 diabetes mellitus. Patient Prefer Adherence. 2020;14:443–454. doi:10.2147/ppa.S237767
5. Liu Y, Maier M, Hao Y, Chen Y, Qin Y, Huo R. Factors related to quality of life for patients with type 2 diabetes with or without depressive symptoms - results from a community-based study in China. J Clin Nurs. 2013;22(1–2):80–88. doi:10.1111/jocn.12010
6. Zhang JB, Bi Y, Shen S, Tong G, Cui S, Yu W, Zhu D. Dalong prevalence of depression and its risk factors in type 2 diabetes mellitus. Chin J Endocrinol Metab. 2011;27(10):4.
7. Herder C, Schmitt A, Budden F, et al. Longitudinal associations between biomarkers of inflammation and changes in depressive symptoms in patients with type 1 and type 2 diabetes. Psychoneuroendocrinology. 2018;91:216–225. doi:10.1016/j.psyneuen.2018.02.032
8. Furukawa S, Sakai T, Niiya T, et al. Nocturia and prevalence of depressive symptoms in Japanese adult patients with type 2 diabetes mellitus: the dogo study. Can J Diabetes. 2018;42(1):51–55. doi:10.1016/j.jcjd.2017.03.002
9. AlBekairy A, AbuRuz S, Alsabani B, et al. Exploring factors associated with depression and anxiety among hospitalized patients with type 2 diabetes mellitus. Med Princ Pract. 2017;26(6):547–553. doi:10.1159/000484929
10. Engidaw NA, Wubetu AD, Basha EA. Prevalence of depression and its associated factors among patients with diabetes mellitus at Tirunesh-Beijing general hospital, Addis Ababa, Ethiopia. BMC Public Health. 2020;20(1):266. doi:10.1186/s12889-020-8360-2
11. Cherrington A, Wallston KA, Rothman RL. Exploring the relationship between diabetes self-efficacy, depressive symptoms, and glycemic control among men and women with type 2 diabetes. J Behav Med. 2010;33(1):81–89. doi:10.1007/s10865-009-9233-4
12. Groh CJ, Moran K Depression and diabetes in a primarily African American female population. Issues Ment Health Nurs. 2016;37(2):106–112. doi:10.3109/01612840.2015.1087605
13. Bo A, Pouwer F, Juul L, Nicolaisen SK, Maindal HT. Prevalence and correlates of diabetes distress, perceived stress and depressive symptoms among adults with early-onset Type 2 diabetes: cross-sectional survey results from the Danish DD2 study. Diabet Med. 2020;37(10):1679–1687. doi:10.1111/dme.14087
14. An JH, Han KD, Jung JH, et al. High bodyweight variability increases depression risk in patients with type 2 diabetes mellitus: a nationwide cohort study in Korea. Front Psychiatry. 2021;12:765129. doi:10.3389/fpsyt.2021.765129
15. Nouwen A, Adriaanse MC, van Dam K, et al. Longitudinal associations between depression and diabetes complications: a systematic review and meta-analysis. Diabet Med. 2019;36(12):1562–1572. doi:10.1111/dme.14054
16. Wang X, Luo JF, Qi L, Long Q, Guo J, Wang HH. Adherence to self-monitoring of blood glucose in Chinese patients with type 2 diabetes: current status and influential factors based on electronic questionnaires. Patient Prefer Adherence. 2019;13:1269–1282. doi:10.2147/PPA.S211668
17. Zhang Y, Ting RZ, Lam MH, et al. Measuring depression with CES-D in Chinese patients with type 2 diabetes: the validity and its comparison to PHQ-9. BMC Psychiatry. 2015;15:198. doi:10.1186/s12888-015-0580-0
18. Wu SF, Huang YC, Lee MC, Wang TJ, Tung HH, Wu MP. Self-efficacy, self-care behavior, anxiety, and depression in Taiwanese with type 2 diabetes: a cross-sectional survey. Nurs Health Sci. 2013;15(2):213–219. doi:10.1111/nhs.12022
19. Khalid A, Dawood S. Social support, self-efficacy, cognitive coping and psychological distress in infertile women. Arch Gynecol Obstet. 2020;302(2):423–430. doi:10.1007/s00404-020-05614-2
20. Bandura A. Self-efficacy: toward a unifying theory of behavioral change. Psychol Rev. 1977;84(2):191–215. doi:10.1037//0033-295x.84.2.191
21. Al-Khawaldeh OA, Al-Hassan MA, Froelicher ES. Self-efficacy, self-management, and glycemic control in adults with type 2 diabetes mellitus. J Diabetes Complications. 2012;26(1):10–16. doi:10.1016/j.jdiacomp.2011.11.002
22. Burns RJ, Deschênes SS, Schmitz N. Associations between coping strategies and mental health in individuals with type 2 diabetes: prospective analyses. Health Psychol. 2016;35(1):78–86. doi:10.1037/hea0000250
23. Shayeghian Z, Aguilar-Vafaie ME, Besharat MA, et al. Self-care activities and glycated haemoglobin in Iranian patients with type 2 diabetes: can coping styles and social support have a buffering role? Psychol Health. 2015;30(2):153–164. doi:10.1080/08870446.2014.951651
24. Kong LN, Zhu WF, He S, Yao Y, Yang L. Relationships among social support, coping strategy, and depressive symptoms in older adults with diabetes. J Gerontol Nurs. 2019;45(4):40–46. doi:10.3928/00989134-20190305-03
25. Xie Y. Validity and reliability of Simplified Coping Style Questionnaire. Chin J Clin Psychol. 1998;2:3–5.
26. Brown GK, Nicassio PM. Development of a questionnaire for the assessment of active and passive coping strategies in chronic pain patients. Pain. 1987;31(1):53–64. doi:10.1016/0304-3959(87)90006-6
27. Wang X, Zhang Q. Chain mediating effect of cognitive appraisal and dispositional coping on family resilience and posttraumatic growth of hemodialysis patients in a hospital in Tianjin. Med Soc. 2022;35(1):5.
28. Al-Amer R, Ramjan L, Glew P, Randall S, Salamonson Y. Self-efficacy, depression, and self-care activities in adult Jordanians with type 2 diabetes: the role of illness perception. Issues Ment Health Nurs. 2016;37(10):744–755. doi:10.1080/01612840.2016.1208692
29. He QZ, Liu F, Guo Y, Shen H, Ou Y-N, Xian M. Mediating effect of coping styles on the relationship between self-efficacy and self-management among young patients with type 2 diabetes. J Nurs Adm. 2018;18(04):263–267.
30. Xiaojia YZZ, Yang Q, Liu X. Self-efficacy as a mediator between illness perception and coping style in elderly diabetic patients. J Nurs Sci. 2013;29(01):21–23.
31. Samuel-Hodge CD, Watkins DC, Rowell KL, Hooten EG. Coping styles, well-being, and self-care behaviors among African Americans with type 2 diabetes. Diabetes Educ. 2008;34(3):501–510. doi:10.1177/0145721708316946
32. Stanojevi D, Krsti M, Jaredi B, Dimitrijevi B. Proactive coping as a mediator between resources and outcomes: a structural equations modeling analysis. Appl Res Qual Life. 2014;9(4):871–885. doi:10.1007/s11482-013-9274-2
33. Cherenack EM, Sikkema KJ, Watt MH, Hansen NB, Wilson PA. Avoidant coping mediates the relationship between self-efficacy for HIV disclosure and depression symptoms among men who have sex with men newly diagnosed with HIV. AIDS Behav. 2018;22(10):3130–3140. doi:10.1007/s10461-018-2036-2
34. Frydenberg EE. Beyond Coping: Meeting Goals, Visions, and Challenges. Oxford University Press; 2002.
35. Yasui-Furukori N, Murakami H, Otaka H, et al. Coping behaviors and depressive status in individuals with type 2 diabetes mellitus. Ann Gen Psychiatry. 2019;18:11. doi:10.1186/s12991-019-0235-5
36. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP; STROBE Initiative. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. J Clin Epidemiol. 2008;61(4):344-349.
37. Cheung SK, Sun SY. Assessment of optimistic self-beliefs: further validation of the Chinese version of the General Self-Efficacy Scale. Psychol Rep. 1999;85(3 Pt 2):1221–1224. doi:10.2466/pr0.1999.85.3f.1221
38. Zhou H, Peng J, Wang D, et al. Mediating effect of coping styles on the association between psychological capital and psychological distress among Chinese nurses: a cross-sectional study. J Psychiatr Ment Health Nurs. 2017;24(2–3):114–122. doi:10.1111/jpm.12350
39. Li X, Guan L, Chang H, Zhang B, Courvoisier DS. Core self-evaluation and burnout among nurses: the mediating role of coping styles. PLoS One. 2014;9(12):e115799. doi:10.1371/journal.pone.0115799
40. Faul F, Erdfelder E, Buchner A, Lang AG. Statistical power analyses using G*Power 3.1: tests for correlation and regression analyses. Behav Res Methods. 2009;41(4):1149–1160. doi:10.3758/brm.41.4.1149
41. Efron B, Tibshirani TJ. An Introduction to the Bootstrap. New York: Chapman & Hall; 1993.
42. Shin N, Hill-Briggs F, Langan S, Payne JL, Lyketsos C, Golden SH. The association of minor and major depression with health problem-solving and diabetes self-care activities in a clinic-based population of adults with type 2 diabetes mellitus. J Diabetes Complications. 2017;31(5):880–885. doi:10.1016/j.jdiacomp.2017.01.026
43. Bodys-Cupak I, Majda A, Zalewska-Puchała J, Kamińska A. The impact of a sense of self-efficacy on the level of stress and the ways of coping with difficult situations in Polish nursing students. Nurse Educ Today. 2016;45:102–107. doi:10.1016/j.nedt.2016.07.004
44. Knowles SR, Apputhurai P, O’Brien CL, Ski CF, Thompson DR, Castle DJ. Exploring the relationships between illness perceptions, self-efficacy, coping strategies, psychological distress and quality of life in a cohort of adults with diabetes mellitus. Psychol Health Med. 2020;25(2):214–228. doi:10.1080/13548506.2019.1695865
45. Kav S, Yilmaz AA, Bulut Y, Dogan N. Self-efficacy, depression and self-care activities of people with type 2 diabetes in Turkey. Collegian. 2017;24(1):27–35. doi:10.1016/j.colegn.2015.09.005
46. Sun P, Sun Y, Jiang H, Jia R, Li Z. Gratitude as a protective factor against anxiety and depression among Chinese adolescents: the mediating role of coping flexibility. Asian J Psychol. 2020;23(4):447–456. doi:10.1111/ajsp.12419
47. Du S, Hu L, Bai Y, et al. The influence of self-efficacy, fear-avoidance belief, and coping styles on quality of life for Chinese patients with chronic nonspecific low back pain: a multisite cross-sectional study. Pain Pract. 2018;18(6):736–747. doi:10.1111/papr.12660
48. Schneider R, Schneider R. Social optimism as generalized expectancy of a positive outcome. Pers Individ Dif. 1997;22:317–325. doi:10.1016/S0191-8869(96)00219-X
49. Féki I, Turki M, Zitoun I, Sellami R, Baati I, Masmoudi J. Dépression et stratégies de coping chez les sujets âgés atteints de diabète de type 2 [Depression and coping strategies in the elderly with type 2 diabetes]. Encephale. 2019;45(4):320–326. doi:10.1016/j.encep.2019.01.005
50. Shing EZ, Jayawickreme E, Waugh CE. Contextual positive coping as a factor contributing to resilience after disasters. J Clin Psychol. 2016;72(12):1287–1306. doi:10.1002/jclp.22327
51. Huang CY, Lai HL, Lu YC, et al. Risk factors and coping style affect health outcomes in adults with type 2 diabetes. Biol Res Nurs. 2016;18(1):82–89. doi:10.1177/1099800415569845
52. Miles SR, Khambaty T, Petersen NJ, Naik AD, Cully JA. The role of affect and coping in diabetes self-management in rural adults with uncontrolled diabetes and depressive symptoms. J Clin Psychol Med Settings. 2018;25(1):55–65. doi:10.1007/s10880-017-9527-6
53. Doron J, Trouillet R, Maneveau A, Ninot G, Neveu D. Coping profiles, perceived stress and health-related behaviors: a cluster analysis approach. Health Promot Int. 2015;30(1):88–100. doi:10.1093/heapro/dau090
54. Young-Hyman D, de Groot M, Hill-Briggs F, Gonzalez JS, Hood K, Peyrot M. Psychosocial care for people with diabetes: a position statement of the American Diabetes Association. Diabetes Care. 2016;39(12):2126–2140. doi:10.2337/dc16-2053
55. Young HM, Miyamoto S, Dharmar M, Tang-Feldman Y. Nurse coaching and mobile health compared with usual care to improve diabetes self-efficacy for persons with type 2 diabetes: randomized controlled trial. JMIR mHealth uHealth. 2020;8(3):e16665. doi:10.2196/16665
56. D’Eramo Melkus G, Chyun D, Vorderstrasse A, Newlin K, Jefferson V, Langerman S. The effect of a diabetes education, coping skills training, and care intervention on physiological and psychosocial outcomes in black women with type 2 diabetes. Biol Res Nurs. 2010;12(1):7–19. doi:10.1177/1099800410369825
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.