Back to Journals » Cancer Management and Research » Volume 14
The Application of Liquid Biopsy Techniques in High-Risk Population for Hepatocellular Carcinoma
Received 3 May 2022
Accepted for publication 27 August 2022
Published 15 September 2022 Volume 2022:14 Pages 2735—2748
DOI https://doi.org/10.2147/CMAR.S373165
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Seema Singh
Jingnuo Ding, Weifeng Zhao
Department of Infectious Diseases, The First Affiliated Hospital of Soochow University, Suzhou, JiangSu Province, 215000, People’s Republic of China
Correspondence: Weifeng Zhao, Department of Infectious Diseases, The First Affiliated Hospital of Soochow University, 188 Shizi Street, Gusu District, Suzhou, JiangSu Province, 215000, People’s Republic of China, Tel +86 13360518767, Email [email protected]
Abstract: Hepatocellular carcinoma (HCC) is one of the most common malignant tumors of the digestive system and has a 5-year overall survival rate of 14.1%. Many HCC patients are diagnosed at an advanced stage, and thus early screening is essential for reducing the mortality of HCC. In addition to commonly used detection indicators such as serum alpha-fetoprotein (AFP), lens culinaris agglutinin-reactive fraction of alpha-fetoprotein (AFP-L3) and abnormal prothrombin (protein induced by vitamin K absence II, PIVKA-II), liquid biopsy techniques have been demonstrated to have diagnostic value in HCC detection. Compared with invasive procedures, liquid biopsy can detect circulatory metabolites of malignant neoplasms. Liquid biopsy techniques can detect circulating tumor cells, circulating tumor DNA, circulating RNA and exosomes and have been used in the early screening, diagnosis and prognostic evaluation of HCC. This paper reviews the molecular biological characteristics and application of different liquid biopsy techniques, and aim to highlight promising biomarkers that may be feasible options for early-stage HCC evaluation to improve early screening in populations at high risk for HCC.
Keywords: liquid biopsy techniques, hepatocellular carcinoma, high-risk population
Introduction
Hepatocellular carcinoma (HCC) is a common malignant digestive tumor that ranks sixth among new cases of malignancies in both males and females.1 Worldwide, liver cancer is the third leading cause of cancer mortality after lung and colorectal cancers and accounts for 8.3% of all cancer-related deaths.1 The prognosis of HCC is closely related to the stage at the time of diagnosis. The poor survival rate of HCC is mainly due to factors such as intrahepatic metastasis, portal vein tumor thrombosis and distant metastasis, which preclude resection; moreover, patients already have many of these features at the time of diagnosis.
According to the diagnosis and treatment guidelines, major risk factors for HCC include cirrhosis, chronic hepatitis B virus (HBV) or hepatitis C virus (HCV) infection, alcoholic fatty liver disease, and nonalcoholic fatty liver disease (NAFLD).2 In addition, the consumption of aflatoxin-contaminated food, schistosomiasis, other causes of cirrhosis, a family history of liver cancer, diabetes, obesity, smoking and drug-induced liver damage are also risk factors for HCC. Regular physical examination should be performed for high-risk populations aged 35 and 45 years. Early screening is a vital strategy for early treatment to improve the overall survival rate of HCC patients.
Biomarkers such as AFP, AFP-L3 and PIVKA-II are recommended indicators for early screening of HCC.3,4 In recent years, novel molecular markers such as proteins, exosome nucleic acids and tumor cells released by tumors into the bloodstream, based on liquid biopsy techniques have shown encouraging results in early diagnosis and treatment evaluation.5,6 Substantial progress has been made in liquid biopsy for HCC, which may have higher sensitivity and specificity than frequently used serum markers such as AFP (Table 1).
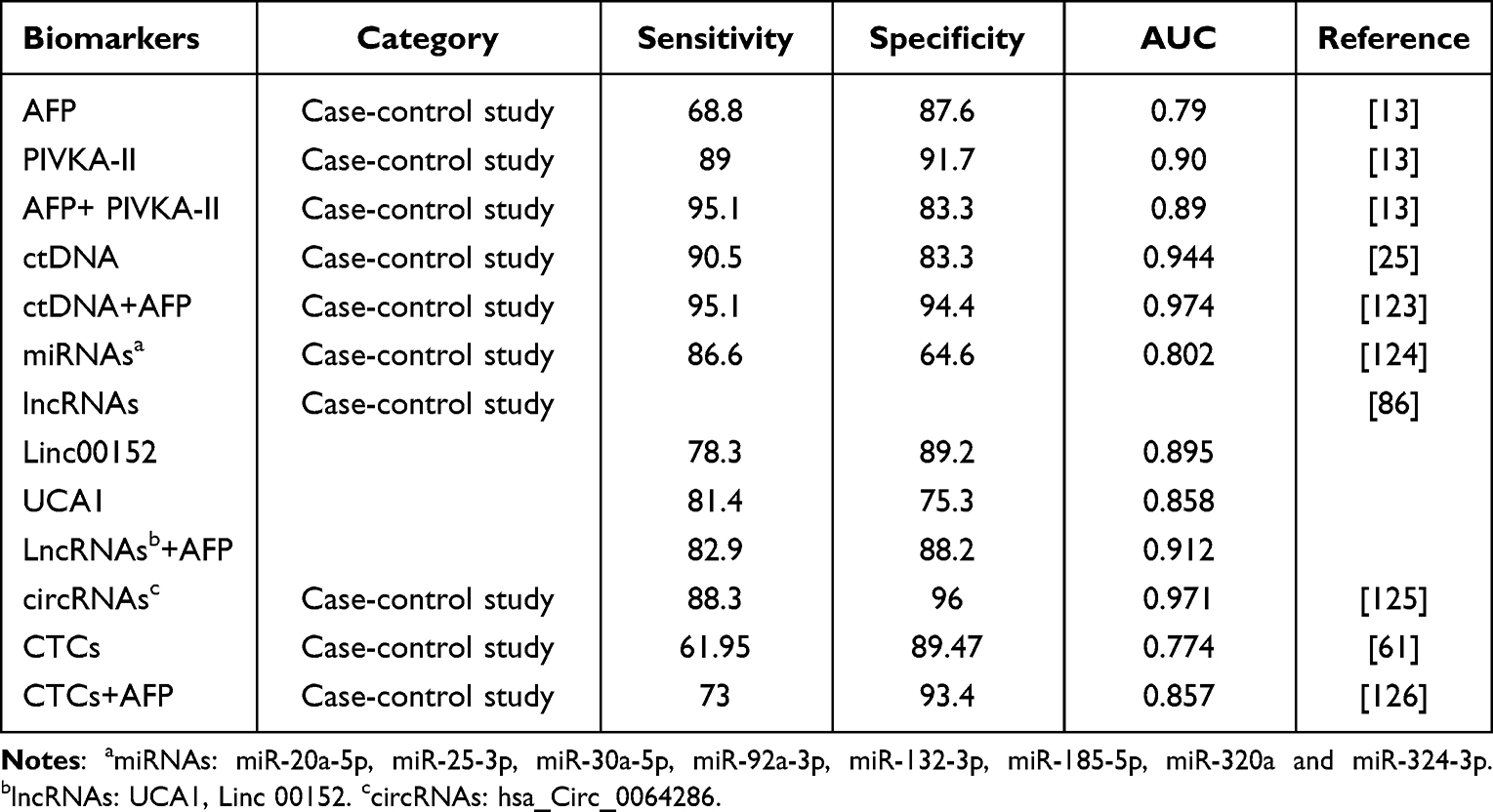 |
Table 1 The Comparison of Different Serum Biomarkers in the Diagnostic Value of HCC |
AFP is a commonly tested biomarker in HCC, is currently the most well-studied biomarker and is widely used in early screening, diagnosis, and disease evaluation. Consistently elevated AFP levels are believed to be a risk factor for HCC progression.7,8 With the development of ultrasound and computed tomography technologies, the detection rate of small hepatocellular carcinoma (sHCC) is increasing, and AFP has been found to be particularly insensitive for the detection of sHCC in clinical practice. According to a retrospective multicenter study,9 AFP positivity was found in 46% (616/1338) of HCC cases and in 23.4% (150/641) of sHCC cases. In addition, AFP is also increased in patients with chronic liver disease and cirrhosis.10 Therefore, the screening effect of AFP for sHCC is limited.11 According to the Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma, AFP is not recommended as a confirmatory test for sHCC.12 Clinical evidence suggests that PIVKA-II is superior to AFP in the management of HCC and that the combination of PIVKA-II and AFP has improved diagnostic value in HCC.13 Compared with tissue biopsy, liquid biopsy primarily detects tumor-related metabolites in body fluids (blood, saliva, pleural fluid, cerebrospinal fluid or urine) and is less tissue-invasive.14 In addition, liquid biopsy can reflect malignant characteristics, which are not manifested in the primary tumor tissue.15 Liquid biopsy is not yet a routine test for all types of tumors in clinical practice, but its diagnostic potential for cancer is drawing the attention of oncologists.16 Liquid biopsy can detect circulating tumor cells (CTCs), circulating tumor DNA (ctDNA), circulating free RNA(cfRNA) and exosomes. In this paper, we will discuss the characteristics, functions and application of different liquid biopsy techniques in the early screening of individuals at high risk for HCC.
Circulating Tumor DNA
Molecular Biological Characteristics of Circulating Tumor DNA
In 1948, Mandel et al first described cell-free DNA (cfDNA) in blood samples from healthy subjects.17 cfDNA is a free DNA fragment of approximately 160–180 bp, that is mainly derived from lymphocytes and bone marrow cells. ctDNA is a specific mutant DNA fragment released from tumor cells into the peripheral blood, that represents the genomic information of oncogenesis after certain pathophysiological processes, including necrosis, apoptosis and excretion of tumor cells. The proportion of ctDNA in all cfDNA varies tremendously depending on the tumor type, and the length of the ctDNA fragment is reported to be generally less than 167 bp.18 A study by Underhill showed that ctDNA segments are generally shortened in length compared with normal cfDNA derived from healthy cells.19 Compared with healthy individuals, the overall length of cfDNA fragments in the blood of tumor patients is shorter, thus, cfDNA can be used as an indicator in early tumor screening. Enrichment of a specific subset of cfDNA fragment lengths can improve the detection of ctDNA associated with nonmetastatic solid tumors. Studies have shown that ctDNA is detectable in over 75% of cases of advanced pancreatic, colorectal, bladder, gastroesophageal, liver, ovarian, breast, melanoma, head and neck cancers.20,21 However, the quantity of ctDNA in blood varies depending on tumor localization.22 In the study of Bettegowda, patients with colorectal cancer, breast cancer, liver cancer, lung cancer and prostate cancer were found to have higher quantities of ctDNA in their blood than those with other cancers. In contrast, patients with oral, pancreatic, gastric cancer and gliomas have lower concentrations of ctDNA in their blood.21
Since ctDNA contains the same genetic mutations as primary tumor cells, ctDNA can be used to identify heterogeneous tumor-specific mutations and epigenetic changes, including methylation, hydroxymethylation, single nucleotide variants and copy number variations.23
Epigenetic Alterations in Circulating Tumor DNA
Methylation and Hydroxymethylation
DNA methylation is one of the most common epigenetic alterations that results in gene suppression. Compared with normal cells, tumor cells show variations in the overall methylation level of the genome, especially the methylation of tumor suppressor genes that can be identified early, which suggests that DNA methylation changes may be an indicator used in the early detection of oncogenesis. HCC-related tumor suppressor genes can be inactivated by promoter methylation, which can drive oncogenesis.24 DNA methylation is an ideal marker for the early diagnosis of tumors because of its tissue specificity, feasibility of detection, and it is not influenced by age. In additions, DNA methylation is more abundant compared with somatic mutation, as more target regions exist and multiple altered CpG sites are in each targeted genomic region.25 Except for the number of multiple CpG sites, a large number of independent hypermethylated gene sites in ctDNA collected from HCC patients have been identified, such as DBX2, THY1, MT1M, INK4A, VIM, FBLN1 and RGS10.26 Xu et al compared cfDNA samples from 1098 HCC patients and 835 healthy controls, and found that HCC-related genes were highly correlated with the methylation characteristics of corresponding matched plasma ctDNA.25 According to a laboratory analysis, a forecast model comprising 10 methylation markers was established, and the sensitivity and specificity of the model were 85.7% and 94.3% respectively, moreover, these markers were highly correlated with tumor load, tumor stage and treatment response. These results indicate the promising prospects of using ctDNA methylation markers in the diagnosis, monitoring and prognosis of HCC. In a methylation model comprised of three abnormally methylated genes (APC, COX2, RASSF1A) and one miRNA (miR203) introduced by Lu et al,27 the sensitivity and specificity of the model for HBV-related HCC diagnosis were both as high as 80%. Moreover, 75% of undiagnosed HCC patients with AFP levels of 20 ng/mL could be detected by this model. The Ras-associated domain family protein 1A (RASSF1A) gene is a major repetitive DNA sequence in the human genome. Araújo et al concluded that hypermethylation of the RASSF1A promoter could be a valuable biomarker for early HCC screening and a potential molecular target for epigenetic therapy.28 In one study, serum RASSF1A promoter hypermethylation was detected in 73.3% of HCC patients.29 Long interspersed nucleotide element 1(LINE-1) is another highly active mediator of retrotransposition. LINE-1 hypomethylation was found in the DNA of 66.7% of HCC serum samples, and was associated with early recurrence and poor survival after radical resection.29 Hypermethylation is a common genetic process and plays a distinct role in cirrhosis and HCC.30 In contrast, hydroxymethylation is a demethylation process that induces the reactivation and expression of genes, and the detection of 5-hydroxymethylcytosine (5-hmC) products from this process can be used for tumor identification. Methylation and hydroxymethylation of ctDNA are associated with oncogenesis, and may facilitate early screening for HCC. In a study including 2554 subjects,31 genome-wide 5-hmC was detected in cfDNA samples, and a 32-gene diagnostic model was established by comparing 5-hmC sequences in HCC patients with those in high-risk populations such as patients with chronic liver disease and cirrhosis. The model was superior to AFP in distinguishing HCC from nonneoplastic tissue.
Mutations
Mutations in the coding region may result in transcriptional abnormalities, which may lead to changes in protein sequence and eventually cancer. Single nucleotide variants are important genomic markers for early screening of tumors because of their high tissue reliability and high tumor and tissue specificity. Among a large number of HCC-related studies that used next-generation sequencing (NGS) to sequence exons and the entire cancer genome, commonly mutated somatic genes, such as TP53 and CTNNB1, were identified and several novel genes including ARID1A, MLL, IRF2, ATM, CDKN2A, FGF19, PIK3CA, RPS6KA3 and JAK1 were found to exhibit moderate mutation frequency. Mutant gene function analysis suggests that alterations in chromatin remodeling, Wnt/β-catenin and JAK/STAT signal transduction, the P53-cell cycle pathway, epigenetic modifiers, oxidative stress pathways, the PI3K/AKT/MTOR pathway and the RAS/RAF/MAPK kinase pathway play crucial roles in HCC oncogenesis.32,33 In a study in which tumor-associated mutations were detected, Huang et al found that the frequency of tumor-associated mutations dependent on ctDNA was 19.5%, and the specificity was 90%.34 In addition, patients who experienced vascular invasion were more likely to have ctDNA mutations (P=0.041) and shorter recurrence-free survival (P<0.001). Another common driver gene for HCC is TP53, which has a mutation frequency of more than 30%. Studies have shown that the frequency of mutated TP53 in ctDNA in blood and urine is between 5% and 60%.35 The study by Johann found that the mutation profile of ctDNA in advanced HCC showed similar mutation frequencies to the profile of early-stage HCC, including mutations in the TERT promoter (51%), TP53 (32%), CTNNB1 (17%), PTEN (8%), AXIN1, ARID2, KMT2D, and TSC2 (each 6%).36 The oncogene β-catenin (CTNNB1) plays an important role in the Wnt signaling pathway. The transcriptional coactivator CTNNB1 can help promote gene expression, which may lead to cell proliferation, apoptosis suppression and angiogenesis. CTNNB1 can also cooperate with TERT to induce hepatocyte transformation.33 The TERT promoter is a common mutation site in several solid tumors. TERT alterations, which are some of the earliest genetic alterations in the malignant transformation of HCC, may lead to telomerase reactivation in cirrhotic hepatocytes and may promote proliferation and prevent senescence.33–37 TERT promoter mutations are reported to occur at a frequency of 59–90% in patients with hyperplastic hepatic nodules and early stages of HCC and are associated with survival rate.38
Copy Number Alteration
Copy number alteration (CNA) is an important subtype of somatic mutations. Studies have shown that broad and focal CNA loading is a genomic feature, that is able to predict tumor immune infiltration and exclusion in several cancer types.39 Active infiltration signals, high cytolytic activity, high inflammation, and genetic markers associated with antigen presentation in HCC were found in low broad CNA burden after analyzing single-nucleotide polymorphism-array data of 477 subjects. In contrast, chromosomally unstable tumors with high broad CNA loads exhibit immune rejection characteristics and are associated with proliferation, DNA repair, and TP53 dysfunction. Xu et al showed that the CNA score in the HCC group was higher than that in the chronic liver disease group.40 Using single-cell whole-genome sequencing, CNAs were found to occur early in hepatocarcinogenesis and to remain relatively stable during tumor progression.41 Chung et al found that cfDNA levels were significantly higher in HCC patients and that genome-wide CNAs in cfDNA were important independent prognostic indicators in HCC patients treated with sorafenib.42 Compared with those with smaller CNA burden, patients with larger CNA burden are more likely to experience disease progression and mortality. Oellerich et al found that copy number instability (CNI) scores could be used in evaluating the CNAs of cfDNA in cancer patients. And they pointed that CNI scores were significantly higher in advanced cancers patients than controls, and it could assess the response of patients to systemic chemotherapy and immunotherapy.43 These results suggest that CNAs detected in liquid biopsy samples can serve as prognostic indicators in patients with advanced HCC who are receiving systematic treatment.
Application of Circulating Tumor DNA in HCC
Currently, the techniques used to detect ctDNA can be divided into targeted and untargeted methods. Briefly, targeted methods, such as digital polymerase chain reaction (dPCR), BEAMing digital PCR, amplification-refractory mutation system-PCR, Capp-Seq and Tam-Seq, which have high sensitivity for the predefined genes. Untargeted methods, such as whole-genome sequencing and NGS, provide a comprehensive view of the entire genomic landscape.44 Compared with the targeted panel, whole-genome-wide sequencing can detect not only point mutations and indels but also rearrangements and copy number variants. In a systematic review that included 112 studies that evaluated the accuracy of liquid biopsy, the authors concluded that detection of CTCs and cfDNA was precise approach to predict prognosis and that both CTCs and cfDNA were good indicators that can be used to dynamically monitor HCC.45 Furthermore, cfDNA analysis may be more useful in the detection of HCC. Yan et al showed that cfDNA was significantly higher in plasma from HCC patients than plasma from liver fibrosis patients and healthy controls. ctDNA is expected to be a better screening marker for early HCC than AFP.46 In a prospective study,47 liquid biopsy to detect cfDNA and proteins in a community population showed a sensitivity of 85% and a specificity of 93% in differentiating HCC patients from non-HCC patients. Then in the follow-up of 331 patients with normal ultrasound combined with AFP negativity, the sensitivity and specificity of cfDNA for the diagnosis of HCC were 100% and 94% respectively, and thus ctDNA could detect HCC in asymptomatic HBsAg-seropositive individuals. High frequency (92.5%) of RASSF1A promoter hypermethylation was detected in HCC patients in the study of Yeo48. And Xu et al established a diagnostic model for HCC prediction with specific methylation marker panel, for which the specificity and sensitivity were 90.5% and 83.3% respectively, this panel could distinguish HCC patients from those with other liver diseases and was superior to AFP. They also found that normal controls with positive detection were likely to have risk factors for HCC, such as HBV infection or a history of alcohol consumption.25 We speculate that high risk factors for HCC may promote cfDNA hypermethylation and then HCC progression, hence, cfDNA may play a key role in screening of high-risk populations. Cai et al summarized the comprehensive ctDNA mutation profiles and proposed a reliable strategy for assessing tumor burden in patients.49 This strategy could identify oncogenesis an average of 4.6 months before imaging changes, and showed superior diagnostic efficacy over the serum biomarkers AFP, AFP-L3 and PIVKA-II. The diagnostic value of ctDNA detection was demonstrated when imaging assessment was unavailable, and thus, ctDNA detection has value for diagnosis of early HCC in high-risk individuals. Recently, scholars used NGS technology to analyze 3204 clinical samples and multidimensional gene variation indicators in cfDNA (including 5-hydroxymethylcytosine, 5’ end motif, fragmentation, nucleosome footprint, HIFI).50 After repeated verification by three independent training, validation and test sets, the HIFI model was shown to be stable and reliable in distinguishing HCC from the non-HCC population with a sensitivity of 95.79% and 95.42%, and a specificity of 95.00% and 97.83% for HCC in the validation and test sets. The diagnostic value of the HIFI method for distinguishing HCC vs cirrhosis was superior to that of AFP. In addition, ctDNA was also associated with surgical management. By detecting the preoperative serum ctDNA content of HCC patients, Atsushi et al found that the recurrence and extrahepatic metastasis rates of the ctDNA positive group were significantly higher than those of the ctDNA-negative group, and that ctDNA content was significantly correlated with tumor progression.51 As a highly sensitive biomarker, ctDNA can predict the vascular invasion capacity of HCC. Wang et al performed whole-genome sequencing in 46 patients with HCC, and a multivariate analysis showed that the ctDNA variant allele frequency had a cutoff value of 0.83% for microvascular invasion, with a sensitivity of 89.7% and a specificity of 80.0%.52 ctDNA can be used serve as an independent risk factor for microvascular invasion in resectable HCC, which suggests that ctDNA may help to establish optimal therapeutic modalities. In summary, ctDNA is fully involved in the occurrence and development of HCC and can used for early screening, surgical evaluation, disease monitoring.
Circulating Tumor Cells
Molecular Biological Characteristics of Circulating Tumor Cells
CTCs are malignant cells derived from either the primary tumor or metastases that migrate into the circulation. Tumor cells secrete matrix metalloproteinases (MMPs) which can degrade the basement membrane, thus allowing the tumor cells to gain direct access to blood and lymphatic vessels. However, most CTCs are rapidly eliminated by anoikis, immune attacks, or shear stress.53 Epithelial to mesenchymal transition (EMT) enables CTCs to easily detach from the primary tumor tissue, invade capillaries and gain a significantly improved ability for survival, metastasis, invasiveness and drug resistance. Studies have revealed a profound heterogeneity between different tumor cells in primary metastatic tumors. Therefore, analysis of CTCs may lead to a comprehensive understanding of tumor cell heterogeneity.54
Specific markers of HCC-related CTCs include Glypican-3 (GPC3), Asialoglycoprotein receptor (ASGPR), epithelial cell adhesion molecule (EpCAM), and stem cell-related markers such as CD44, CD90,55 and intercellular adhesion molecule 1 (ICAM1).56 The marker GPC3 is a cell membrane-anchored protein used in the clinic for HCC pathological analysis and characterization.57 GPC3 expression is more commonly detected in moderately to poorly differentiated HCC tumor cells, which could facilitate extrahepatic migration; moreover, the presence of GPC3+ CTCs suggests metastatic HCC.58 ASGPR is a transmembrane protein expressed only on the surface of liver cells, and is highly expressed in well-differentiated HCC. EpCAM is one of the most commonly used membrane-associated proteins for capturing CTCs. EpCAM has been identified as a surface marker of HCC cells with stem cell characteristics,59 which are correlated with various clinicopathological features of HCC, such as vascular infiltration, evaluted AFP level, and more advanced Barcelona clinic liver cancer (BCLC) stage.60 CTCs with an EMT phenotype have highly metastatic properties.54 The EMT process in CTCs can promote HCC metastasis. The expression of EMT markers such as vimentin, twist, zinc finger E-box-binding (ZEB)1, ZEB2, snail, slug, and E-cadherin has been studied in liver-derived CTCs from HCC patients.58 In the study by Cheng,61 the CanPatrolTM system was used to stratify CTCs into three phenotypic subgroups according to the predominantly expressed markers: epithelial phenotype (EpCAM, CK8/18/19), mesenchymal phenotype (vimentin, twist), and mixed phenotype. Total CTCs had a superior diagnostic value over AFP in differentiating HCC from nonmalignant liver disease among 176 patients. The AUC values for total CTCs, AFP, and the combined use of total CTCs and AFP were 0.774 (95% CI, 0.704–0.834), 0.669 (95% CI, 0.587–0.750), and 0.821 (95% CI, 0.756–0.886), respectively. EMT-based classification of CTCs could predict the diagnosis, early recurrence, metastases, and shorter overall in HCC.
Application of Circulating Tumor Cells in HCC
Currently, CTC detection methods include physical methods and biological methods. The physical methods are commonly called biophysical property-based enrichment, and mainly depend on the physical characteristics of CTCs, such as size, density, electric charge, migratory capacity and deformability. Based on different physical properties, there are various technologies such as filtration- based system, dielectrophoresis and so on.The latter is also called immunoaffinity-based enrichment and mainly depends on antigen-antibody binding, as this method uses antibodies against tumor-specific biomarkers, such as EpCAM, ASGPR, human epidermal growth factor receptor 2 (HER2), prostate-specific antigen (PSA), human pancytokeratin (P-CK), and carbamoyl phosphate synthetase1(CPS1).62 Another type known as an enrichment-free methods, uses flow cytometry to distinguish CTCs from leukocytes based on a higher karyoplasmic ratio and size. Currently, the only FDA-approved test for detecting CTCs is the Cell-Search™ system, which utilizes EpCAM cell surface markers. However, combined markers-based CTC detection could increase the positivity rate.54 A mixture of antibodies against ASGPR and CPS1 achieved a CTC detection rate of 91% in HCC patients.63 Zhang et al used a CTC-Chip with antibodies against ASGPR, P-CK and CPS1, and differentiated HCC patients from those with benign liver disease or non-HCC cancer at a rate of 100%.64 A study by Wang detected EpCAM+ CTCs in 60% of 42 HCC patients and found significant correlations between both the positivity rate and the number of CTCs with TNM stage.65 Guo et al found that a CTC-derived PCR score was elevated in 125/171 (73%) patients whose AFP level was <20 ng/mL with a sensitivity of 72.5% and a specificity of 95.0%, compared with 57.0% and 90.0% for AFP at a cutoff 20 ng/mL.66 The combination of AFP and CTCs may improve HCC detection.45 It is believed that CTCs have an advantage over AFP in early screening of groups at high-risk for HCC. Therefore, for population with positive CTCs who are at high-risk for HCC, CTC examination should be routinely combined with ultrasound and AFP detection. However, CTCs are considered to be an important predictor of tumor metastasis and recurrence, CTC detection is not independently recommended as diagnostic tool.62 Thus CTCs may serve as better prognostic biomarker than other currently used markers. Zhou et al found that patients with elevated numbers of EpCAM+ CTCs and regulatory T cells showed a higher risk of developing HCC recurrence, than those with low numbers of CTCs, with a recurrence ratio of 66.7% vs 10.3% (P < 0.001).67 A similar study was reported by Zhong et al.68 In addition, Qi found that 101 of 112 patients (90.81%) with HCC, including those with early-stage disease, were positive for CTCs and that very small HCC nodules were detected after 3 to 5 months of follow-up. They also detected CTCs in 12 patients with chronic HBV infection and found that of 2 patients who were positive for CTCs, both had small HCC tumors detected within 5 months.69 Therefore, CTCs could be used to predict HCC,70 but may be able to be used more routinely as a prognostic biomarker.
Circulating Free RNA
Molecular Biological Characteristics of Circulating Free RNA
Similar to cfDNA, cfRNA is released into the circulations via various systems. These molecules in peripheral blood represent the cancer tissue of origin. Compared with markers tested by noninvasive approaches, cfRNAs are more dynamically regulated, tissue specific, and abundant in extracellular environments.71 The significance and diagnostic value of microRNAs (miRNAs) in HCC have been reported in many studies. miRNAs are endogenous, noncoding (ncRNAs) that regulate various molecular biological activities by suppressing the translation of target messenger RNAs (mRNAs). miRNAs are located within exosome-encapsulated, apoptotic bodies, but they can also bind stably to serum proteins and lipids in peripheral blood and can be used to evaluate HCC. miRNAs are involved in liver regeneration, lipid metabolism, apoptosis, inflammation and HCC development.72 Oncogenic miRNAs such as miR-21, miR-155, and miR-221 are well-known in HCC. Specifically miR-21 plays a key role in collagen synthesis in the extracellular matrix and in fibrosis and contributes to hepatocarcinogenesis by activating hematopoietic stem cells.72,73 Tumor suppressor miRNAs in HCC includes miRNA-122, miRNA-29, the Let-7 family and the miRNA-15 family. The Let-7 family consists of multiple tumor suppressor miRNAs that target the RAS family. The miR-15 family includes miR-15a, miR-15b, miR-16, miR-195, and miR-497, which have complementary sequences targeting specific mRNAs. In addition, long noncoding RNAs (lncRNAs) and circular RNAs (circRNAs) are also important in early screening for HCC. LncRNAs, which are the broadest class of ncRNAs, include mRNA-like ncRNAs, and contribute to the pathogenesis of numerous human diseases. LncRNAs act as regulators in the liver microenvironment and chronic liver diseases.74 CircRNAs are also a class of ncRNAs that have multiple functions in the regulation of gene expression. Recently, circRNAs have been considered a diagnostic tool for HCC.
Application of Circulating Free RNA in HCC
Circulating free RNA has remarkable stability, including resistance to temperature, pH, and RNases, and thus isolation of cfRNA from the peripheral blood is less tedious with standard RNA purification techniques. The most commonly technologies include NGS, microarray, and RT-qPCR. NGS allows the measurement of genome-wide miRNA. However, this method is expensive and the analysis is not standardized. In contrast, RT-qPCR is inexpensive, rapidly amplifies nucleic acids, and has many advantages such as high sensitivity, better accuracy, a wide dynamic range and the need for less sample input. Microarrays are another method used to detect miRNA, and are based on the sensitive and specific hybridization of the target miRNA to complementary DNA probes,75 but analysis of microarray data is time-consuming.
It has been reported that circulating miR-122 and Let-7 have potential utility in the diagnosis of early-stage HCC in high-risk populations and these markers showed considerable sensitivity to AFP in patients with HBV-related precancerous nodules and patients with early-stage HCC.76 Tsai et al found that Let-7 family members (miR-92, miR-122, miR-125b, mir-143, miR-192, miR-16, miR-126, and miR-199a/b) can predict HCC risk in chronic hepatitis C patients. The Let-7 family could be an effective surrogate biomarker for predicting HCC development in chronic hepatitis C -related high-risk populations.77 miR-122 has high diagnostic accuracy in the detection of early HCC in patients with cirrhosis.78 Serum circulating miR-107 has also been evaluated in early-stage HCC,79 and shows good potential in high-risk populations. Zhou et al reported that a microRNA panel (miR-122, miR-192, miR-21, miR-223, miR-26a, miR-27a and miR-801) could discriminate HCC from chronic hepatitis B (CHB) and cirrhosis, with sensitivities of 79.1% and 75%, and specificities of 76.4% and 91.1% respectively.80 In HBV-related HCC, scholars found that miR150 levels were significantly reduced compared with the levels in chronic HBV patients without HCC (sensitivity 79.1% and specificity 76.5%).81 The same was observed for the miRNA 101.82 Wu et al found that the expression of miR-224 in HCC was elevated compared with that in healthy controls, and the subgroup analysis showed that patients with HBV-related HCC had higher levels.83 In a multicenter clinical study which contained different groups such as healthy population, inactive HBsAg carriers, patients with CHB, CHB-related cirrhosis and HCC, an miRNA classifier containing seven differentially expressed miRNAs that could detect HCC from different control cohorts was identified; this panel was significantly superior to AFP in early screening of a high-risk population with an AUC that ranged from 0.817–0.818.84 Yu et al also confirmed the presence of some deregulated miRNAs in an independent cohort of HCC, CHB patients and healthy control volunteers. They found that four miRNAs (miR-1972, miR-193a-5p, miR-214-3p and miR-365a-3p) could distinguish patients with HCC from those without HCC. Five upregulated miRNAs (miR-122-5p, miR-125b-5p, miR-885-5p, miR-100-5p and miR-148a-3p) were considered to be potential biomarkers for HBV infection among HCC, cirrhosis, and CHB, while especially, miR-34a-5p could be biomarker for cirrhosis,85 and may be a potential biomarker for early HCC screening of high-risk populations. Highly-upregulated in liver cancer (HULC) is the most studied lncRNA in HCC. Other studies have shown that circulating HULC in HCC patients can be used as a diagnostic marker, as this lncRNA is highly upregulated in HCC patients compared with healthy individuals.71,86 Among other lnRNAs, LINC00152 is considered to be the best diagnostic lncRNA as the AUC, sensitivity and specificity values are high.86 In one study, the expression level of LINC00152 in peripheral blood gradually increased from normal healthy controls to patients with CHB and those with cirrhosis, and finally, was the highest in HCC. Studies on the expression of circSMARCA5 in the plasma of HCC patients demonstrated progressive downregulation from hepatitis to cirrhosis and HCC in precancerous lesions.87 ROC curve analysis confirmed the potential of these circRNAs in distinguishing patients with hepatitis or cirrhosis from those with HCC, especially those with AFP levels below 200ng /mL. Additionally, Zhu analyzed 13,617 circRNAs in plasma samples from patients with HBV-related HCC and confirmed that six circRNAs were differently expressed in HCC and HBV-related cirrhosis, which suggests that circRNAs may be useful markers for early screening of high-risk populations, such as those with cirrhosis.88
Exosomes
Molecular Biological Characteristics of Exosomes
Exosomes are membranous vesicles with a diameter ranging from 40 nm – 160 nm that are released into the extracellular matrix after the fusion of multiple intracellular vesicles with the cell membrane. They contain many active components, including lipids, proteins, RNA, and DNA, and play a key role in the communication between cells, including HCC cells and non-HCC cells.89,90 Exosomes regulate the progression of HCC by activating fibroblasts and hepatic stellate cells, immune cells, normal liver cells, and HCC cells.91 In the tumor microenvironment, tumor cells produce a large number of exosomes, which are transferred from cancer cells to immature cells, these cells in turn, participate in oncogenesis, degradation and cell signal transduction.92 Studies have shown that exosomes can transfer oncogenes to normal cells during pathological processes, which may be one of the mechanisms of tumor invasion and metastasis.93 The role of exosomes in cancer progression may be dynamic and specific to cancer type, genetics, and stage.89 Exosomes can be internalized by adjacent or distant cells to regulate multiple target genes in recipient cells, they can participate in intercellular communication, and cell microenvironment interactions, and they can mediate cell signaling and metabolism.94 The characteristics and dynamic changes of exosome cargo molecules directly reflect those of the parental tumor cells,95 which constitutes the foundation for applying exosomes in cancer diagnosis and prognosis as well as for predicting an individual’s response to antitumor therapy.96
The Composition and Application of Exosomes in HCC
Traditional laboratory methods for isolating and analyzing exosomes are complex, multi-step, and time-consuming, and include ultracentrifugation, filtration, size-exclusion chromatography, immunoaffinity purification, western blotting, enzyme-linked immunosorbent assay (ELISA), PCR, and flow cytometry.97 Recently, miniaturized systems and lab-on-a-chip platforms using micro/nanotechnologies have been widely developed for rapid, convenient and on-site exosome separation. Nanoparticle tracking analysis (NTA) is a widely used method for characterizing the size and concentration of exosomes, and involves techniques such as magnetic nanoparticles, and polyhydroxyalkanoate. Microfluidics and electrochemical methods can also rapidly detect exosomes with high yield.
Exosomal proteins are important markers in the diagnosis of HCC. In the Arbelaiz study,98 RasGAP SH3 domain binding protein (G3BP) and polymeric immunoglobulin receptor (PIGR) were significantly elevated in HCC-derived exosomes, and the prediction efficacy of the combination of the two proteins was superior to that of AFP. Iron overload is an important factor that promotes the occurrence and development of HCC. Tseng reported that hepcidin may play a critical role in HCC resistance.99 The copy number of the hepcidin mRNA variant in serum-derived exosomes from HCC patients was significantly higher than that of their healthy counterparts, which indicates that hepcidin may be a novel diagnostic biomarker for HCC.100 14-3-3ζ proteins in exosomes produced by HCC can reduce the activation, proliferation and differentiation of T cells and can induce the transformation of T cells into regulatory T cells, which leads to T cell depletion.101 This pathway has been confirmed by several studies investigating tumor evasion of immune surveillance,102 which can promote HCC oncogenesis.
In addition to the presence of cfRNA in plasma or serum, RNA-enriched exosomes can be used for noninvasive real-time staging in early tumor screening and to determine tumor evolution and response to therapy. The serum levels of exosomal miRNA-21 were 2.21-fold higher in the HCC group than in the CHBgroup, and 5.57-fold higher in HCC group than in the healthy population.103 In the study by Wang, exosomes were significantly increased in patients with HCC compared those with liver cirrhosis, and the AUC values for discriminating patients with early TNM stage I and II from those with cirrhosis were 0.83 (95% CI 0.74–0.93) and 0.94 (95% CI 0.88–1.00), respectively.104 Recent findings have already clarified the involvement of specific exosome cargo molecules in regulating HCC tumorigenesis and progression.105 The expression of miR-221, miR-103, miR-181c, miR-181a, miR-93 and miR-26a is consistent in the serum of HCC patients, and is associated with corresponding levels in tissue and in the circulation.106,107 MiR21 can promote the proliferation and metastasis of HCC cells by inhibiting the expression PTEN, PDCD4, and RECK, and the level of miR21 is much higher in HCC patients than in healthy controls and patients with CHB.102 LncRNAs have potential diagnostic value in HCC. Studies have revealed that the level of LINC00161, LINC000635, and lncRNA-activated by transforming growth factor-β significantly higher in serum-derived exosomes from HCC patients than in patients without HCC, and that these lncRNAs are closely correlated with TNM stage and tumor volume.108–110 Conigliaro et al found that CD90+ exosomes express high levels of lncRNAH19, which significantly increase vascular endothelial growth factor (VEGF) release and receptor VEGF-R1 production, thereby stimulating angiogenesis.93 CircRNAs are another type of exosomal ncRNAs that are well-expressed at low but stable levels in different species, circRNAs also show specificity in cell type, tissue type, developmental stage and regulatory potency.111 circRNAs are diagnostic biomarkers for early and minimally invasive cancer.112 Recent clinical trials have shown that the sensitivity and specificity of single miRNAs in predicting HCC are less than ideal. Therefore, comprehensive detection using multiple assays (such as miR-122 and miR-48a in combination with AFP) could improve the identification of early HCC and the distinction of HCC from cirrhosis.100
Conclusion and Future Perspectives
Patients with CHB and cirrhosis are the most common high-risk populations for HCC. For high-risk populations, cost-effective, HCC risk-based surveillance strategies should be established after achieving sustained virologic response, and early screening is the key for improving the diagnosis and treatment of HCC, which has a high cost-effective ratio2 The traditional early screening method for cancer has many limitations, no effective early screening method has been established for most cancer types, and compliance is generally low. Compared with the traditional early screening method, liquid biopsy technology has obvious advantages: convenient sampling, pan-cancer detection, reproducible sampling, and effective response to tumor heterogeneity. Considering the cost-effectiveness of techniques relevant to liquid biopsy, the application of these techniques in HCC screening has not been routinely tested. Despite advances in precise detection at the molecular level, liquid biopsy demands a high cost to detect HCC in target patients, and therefore, its extensive use has been limited compared with specific imaging procedures, such as ultrasonography and magnetic resonance imaging.113,114 However, a previous study suggested that liquid biopsy showed effective advantages in quality-adjusted life years (QALYs).115 The superiority of liquid biopsy was also elucidated in early gastric cancer and nasopharyngeal carcinoma.116,117 The current view is that liquid biopsy could serve as a supplement to serum biomarkers and radiological screening in tumor detection and diagnosis.117,118
According to the current literatures, liquid biopsy techniques have shown significantly higher sensitivity and specificity in the early screening of populations at-risk for HCC. Regardless of the types of liquid biopsy, it can distinguish HCC from high-risk populations without HCC, which provides evidence that early screening is important since differences between the high-risk population and the healthy population are apparent. ctDNA could be applied to HCC detection since it has a short half-life, thus any variation in tumor-derived ctDNA can provide specific evidence for tumor progression in real time, especially for small tumors. A high ctDNA level suggests cancer development and dissemination, and is an early indicator of progression and recurrence. Moreover, patients may receive individualized treatment along with subsequent surveillance depending on the ctDNA result.119 The specific methylation sites can be a superior marker over AFP in the early identification of HCC and cirrhosis nodules. High ctDNA levels imply microvascular infiltration as well as postoperative recurrence and metastasis in cases of resectable HCC. Copy number alteration is associated with survival of HCC patients. It can be speculated that ctDNA assessment could be involved in the whole management of HCC and that ctDNA can serve as an effective indicator of treatment modulation. Markers based on specific gene mutations in ctDNA have been accepted by clinical guidelines to predict efficacy and monitor resistance. ctDNA detection may be the most useful liquid biopsy tool for early screening. CTCs also play a critical role in the early screening of individuals at high risk for HCC. Different markers of HCC-related CTCs exhibit specific value in the oncogenesis, development and recurrence of liver cancer. As membranous vesicles, exosomes participate in communication between cells, especially HCC cells. Circulating miRNAs are stable in blood, and thus could be more useful for early screening for HCC. Exosomal proteins and RNA-enriched exosomes have been gradually discovered, and the prediction efficacy of HCC has also been demonstrated. Interestingly, the different causes of HCC may also be associated with different mutation, and therefore, we could choose different biomarkers for early screen according to different HCC etiologies.120
However, current liquid biopsy techniques are challenging in terms of stability and they cannot be independently performed for early screening or monitoring of HCC, but they can still complement individualized screening and diagnosis.121 As a form of liquid biopsy, the detection of ctDNA, CTCs, cfRNA and exosomes in combination with detection of AFP or PIVKA-II and imaging examinations demonstrates good application prospects for early diagnosis and prognosis for HCC. However, the exact mechanism by which ctDNA is released into the blood remains to be clarified. Clarifying the main biological characteristics of ctDNA could promote its use as a marker. The small amounts of ctDNA in circulation and the precise requirements for sample processing are challenges in the clinical adoption of ctDNA detection in HCC. In addition, genetic mutations lack specific characteristics to determine exact oncogenic factors. Due to multiple genetic mutations and somatic variants are also presented in normal tissues, gene mutations found in liquid biopsies may be of limited use in early screening of HCC.122 The limitation of clearly defined useful genetic targets and biomarkers, which can help distinguish ctDNA from nontumor DNA is the most important challenge in the use of ctDNA, Additionally, the heterogeneity of HCC-related CTCs and the EMT process of metastasis, lead to a lack of highly sensitive and specific markers for the detection of CTCs. Only living cells with metastatic potential can be detected, and the optimal combination of CTCs-enriched markers is unclear. Isolation of CTCs for culture and evaluation of their mutational profile is also challenging. Due to problems in the identification, isolation and purification of exosomes, their specific molecular mechanism is still unknown, Previous studies of exosomes and the mechanism of HCC oncogenesis are not sufficiently thorough, and the way in which miRNA, lncRNA and proteins are sorted into exosomes, and whether exosome uptake is a type-specific process are not well-known. The use of exosomes in the diagnosis and treatment of HCC is still in the preclinical experimental stage. The lack of standardization of liquid biopsy procedures such as the types of tubes used for blood collection, blood collection volume, sample storage and detection, isolation, and enrichment, due to varying practices in different medical centers may preclude their use in routine clinical practice. It is still necessary to further explore the effectiveness of liquid biopsy in the early screening, diagnosis, efficacy evaluation and prognosis of HCC, especially for high-risk populations. The liquid biopsy techniques have great potential and are expected to be extensively used for HCC in clinical practice in the near future.
Ethical Approval
This article does not contain any studies with human participants performed by any of the authors.
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. General Office of National Health Commission. Standard for diagnosis and treatment of primary liver cancer (2022 edition)[J]. J Clin Hepatol, 2022, 38(2): 288-303. doi:10.3969/j.issn.1001-5256.2022.02.009
3. Zhou J, Sun H, Wang Z, et al. Guidelines for the diagnosis and treatment of hepatocellular carcinoma (2019 edition). Liver Cancer. 2020;9(6):682–720. doi:10.1159/000509424
4. Kokudo N, Takemura N, Hasegawa K, et al. Clinical practice guidelines for hepatocellular carcinoma: the Japan Society of Hepatology 2017 (4th JSH-HCC guidelines) 2019 update. Hepatol Res. 2019;49(10):1109–1113. doi:10.1111/hepr.13411
5. Barrera-Saldana HA, Fernandez-Garza LE, Barrera-Barrera SA. Liquid biopsy in chronic liver disease. Ann Hepatol. 2021;20:100197. doi:10.1016/j.aohep.2020.03.008
6. Tay TKY, Tan PH. Liquid biopsy in breast cancer: a focused review. Arch Pathol Lab Med. 2021;145(6):678–686. doi:10.5858/arpa.2019-0559-RA
7. Kanwal F, Singal AG. Surveillance for hepatocellular carcinoma: current best practice and future direction. Gastroenterology. 2019;157(1):54–64. doi:10.1053/j.gastro.2019.02.049
8. European Association For The Study Of The L, European Organisation For R, Treatment Of C. EASL-EORTC clinical practice guidelines: management of hepatocellular carcinoma. J Hepatol. 2012;56(4):908–943. doi:10.1016/j.jhep.2011.12.001
9. Zhang G, Ha SA, Kim HK, et al. Combined analysis of AFP and HCCR-1 as an useful serological marker for small hepatocellular carcinoma: a prospective cohort study. Dis Markers. 2012;32(4):265–271. doi:10.3233/DMA-2011-0878
10. Chen S, Chen H, Gao S, et al. Differential expression of plasma microRNA-125b in hepatitis B virus-related liver diseases and diagnostic potential for hepatitis B virus-induced hepatocellular carcinoma. Hepatol Res. 2017;47(4):312–320. doi:10.1111/hepr.12739
11. Galle PR, Foerster F, Kudo M, et al. Biology and significance of alpha-fetoprotein in hepatocellular carcinoma. Liver Int. 2019;39(12):2214–2229. doi:10.1111/liv.14223
12. Omata M, Cheng AL, Kokudo N, et al. Asia-Pacific clinical practice guidelines on the management of hepatocellular carcinoma: a 2017 update. Hepatol Int. 2017;11(4):317–370. doi:10.1007/s12072-017-9799-9
13. Xu F, Zhang L, He W, et al. The diagnostic value of serum PIVKA-II alone or in combination with AFP in Chinese hepatocellular carcinoma patients. Dis Markers. 2021;2021:8868370. doi:10.1155/2021/8868370
14. Durin L, Pradines A, Basset C, et al. Liquid biopsy of non-plasma body fluids in non-small cell lung cancer: look closer to the tumor! Cells. 2020;9(11). doi:10.3390/cells9112486
15. Mader S, Pantel K. Liquid biopsy: current status and future perspectives. Oncol Res Treat. 2017;40(7–8):404–408. doi:10.1159/000478018
16. Palmirotta R, Lovero D, Cafforio P, et al. Liquid biopsy of cancer: a multimodal diagnostic tool in clinical oncology. Ther Adv Med Oncol. 2018;10:1758835918794630. doi:10.1177/1758835918794630
17. Mandel P, Metais P. Nuclear acids in human blood plasma. C R Seances Soc Biol Fil. 1948;142(3–4):241–243.
18. Mouliere F, Chandrananda D, Piskorz AM, et al. Enhanced detection of circulating tumor DNA by fragment size analysis. Sci Transl Med. 2018;10:466. doi:10.1126/scitranslmed.aat4921
19. Underhill HR, Kitzman JO, Hellwig S, et al. Fragment length of circulating tumor DNA. PLoS Genet. 2016;12(7):e1006162. doi:10.1371/journal.pgen.1006162
20. Cheng F, Su L, Qian C. Circulating tumor DNA: a promising biomarker in the liquid biopsy of cancer. Oncotarget. 2016;7(30):48832–48841. doi:10.18632/oncotarget.9453
21. Bettegowda C, Sausen M, Leary RJ, et al. Detection of circulating tumor DNA in early- and late-stage human malignancies. Sci Transl Med. 2014;6(224):224ra24. doi:10.1126/scitranslmed.3007094
22. Mehes G. Liquid biopsy for predictive mutational profiling of solid cancer: the pathologist’s perspective. J Biotechnol. 2019;297:66–70. doi:10.1016/j.jbiotec.2019.04.002
23. Lenaerts L, Tuveri S, Jatsenko T, et al. Detection of incipient tumours by screening of circulating plasma DNA: hype or hope? Acta Clin Belg. 2020;75(1):9–18. doi:10.1080/17843286.2019.1671653
24. Nishida N. Impact of hepatitis virus and aging on DNA methylation in human hepatocarcinogenesis. Histol Histopathol. 2010;25(5):647–654. doi:10.14670/HH-25.647
25. Xu RH, Wei W, Krawczyk M, et al. Circulating tumour DNA methylation markers for diagnosis and prognosis of hepatocellular carcinoma. Nat Mater. 2017;16(11):1155–1161. doi:10.1038/nmat4997
26. Wu X, Li J, Gassa A, et al. Circulating tumor DNA as an emerging liquid biopsy biomarker for early diagnosis and therapeutic monitoring in hepatocellular carcinoma. Int J Biol Sci. 2020;16(9):1551–1562. doi:10.7150/ijbs.44024
27. Lu CY, Chen SY, Peng HL, et al. Cell-free methylation markers with diagnostic and prognostic potential in hepatocellular carcinoma. Oncotarget. 2017;8(4):6406–6418. doi:10.18632/oncotarget.14115
28. Araujo OC, Rosa AS, Fernandes A, et al. RASSF1A and DOK1 promoter methylation levels in hepatocellular carcinoma, cirrhotic and non-cirrhotic liver, and correlation with liver cancer in Brazilian patients. PLoS One. 2016;11(4):e0153796. doi:10.1371/journal.pone.0153796
29. Liu ZJ, Huang Y, Wei L, et al. Combination of LINE-1 hypomethylation and RASSF1A promoter hypermethylation in serum DNA is a non-invasion prognostic biomarker for early recurrence of hepatocellular carcinoma after curative resection. Neoplasma. 2017;64(5):795–802. doi:10.4149/neo_2017_519
30. Hlady RA, Sathyanarayan A, Thompson JJ, et al. Integrating the Epigenome to Identify Drivers of Hepatocellular Carcinoma. Hepatology. 2019;69(2):639–652. doi:10.1002/hep.30211
31. Cai J, Chen L, Zhang Z, et al. Genome-wide mapping of 5-hydroxymethylcytosines in circulating cell-free DNA as a non-invasive approach for early detection of hepatocellular carcinoma. Gut. 2019;68(12):2195–2205. doi:10.1136/gutjnl-2019-318882
32. Gu DL, Chen YH, Shih JH, et al. Target genes discovery through copy number alteration analysis in human hepatocellular carcinoma. World J Gastroenterol. 2013;19(47):8873–8879. doi:10.3748/wjg.v19.i47.8873
33. Zucman-Rossi J, Villanueva A, Nault JC, et al. Genetic landscape and biomarkers of hepatocellular carcinoma. Gastroenterology. 2015;149(5):1226–39 e4. doi:10.1053/j.gastro.2015.05.061
34. Huang A, Zhang X, Zhou SL, et al. Detecting circulating tumor DNA in hepatocellular carcinoma patients using droplet digital PCR is feasible and reflects intratumoral heterogeneity. J Cancer. 2016;7(13):1907–1914. doi:10.7150/jca.15823
35. Dhayat SA, Yang Z. Impact of circulating tumor DNA in hepatocellular and pancreatic carcinomas. J Cancer Res Clin Oncol. 2020;146(7):1625–1645. doi:10.1007/s00432-020-03219-5
36. von Felden J, Craig AJ, Garcia-Lezana T, et al. Mutations in circulating tumor DNA predict primary resistance to systemic therapies in advanced hepatocellular carcinoma. Oncogene. 2021;40(1):140–151. doi:10.1038/s41388-020-01519-1
37. Khemlina G, Ikeda S, Kurzrock R. The biology of Hepatocellular carcinoma: implications for genomic and immune therapies. Mol Cancer. 2017;16(1):149. doi:10.1186/s12943-017-0712-x
38. Bell RJ, Rube HT, Xavier-Magalhaes A, et al. Understanding TERT promoter mutations: a common path to immortality. Mol Cancer Res. 2016;14(4):315–323. doi:10.1158/1541-7786.MCR-16-0003
39. Bassaganyas L, Pinyol R, Esteban-Fabro R, et al. Copy-number alteration burden differentially impacts immune profiles and molecular features of hepatocellular carcinoma. Clin Cancer Res. 2020;26(23):6350–6361. doi:10.1158/1078-0432.CCR-20-1497
40. Xu H, Zhu X, Xu Z, et al. Non-invasive analysis of genomic copy number variation in patients with hepatocellular carcinoma by next generation DNA sequencing. J Cancer. 2015;6(3):247–253. doi:10.7150/jca.10747
41. Duan M, Hao J, Cui S, et al. Diverse modes of clonal evolution in HBV-related hepatocellular carcinoma revealed by single-cell genome sequencing. Cell Res. 2018;28(3):359–373. doi:10.1038/cr.2018.11
42. Oh CR, Kong SY, Im HS, et al. Genome-wide copy number alteration and VEGFA amplification of circulating cell-free DNA as a biomarker in advanced hepatocellular carcinoma patients treated with Sorafenib. BMC Cancer. 2019;19(1):292. doi:10.1186/s12885-019-5483-x
43. Oellerich M, Schutz E, Beck J, et al. Using circulating cell-free DNA to monitor personalized cancer therapy. Crit Rev Clin Lab Sci. 2017;54(3):205–218. doi:10.1080/10408363.2017.1299683
44. Zhang Y, Liu Z, Ji K, et al. Clinical application value of circulating cell-free DNA in hepatocellular carcinoma. Front Mol Biosci. 2021;8:736330. doi:10.3389/fmolb.2021.736330
45. Chen VL, Xu D, Wicha MS, et al. Utility of liquid biopsy analysis in detection of hepatocellular carcinoma, determination of prognosis, and disease monitoring: a systematic review. Clin Gastroenterol Hepatol. 2020;18(13):2879–902 e9. doi:10.1016/j.cgh.2020.04.019
46. Yan L, Chen Y, Zhou J, et al. Diagnostic value of circulating cell-free DNA levels for hepatocellular carcinoma. Int J Infect Dis. 2018;67:92–97. doi:10.1016/j.ijid.2017.12.002
47. Qu C, Wang Y, Wang P, et al. Detection of early-stage hepatocellular carcinoma in asymptomatic HBsAg-seropositive individuals by liquid biopsy. Proc Natl Acad Sci U S A. 2019;116(13):6308–6312. doi:10.1073/pnas.1819799116
48. Yeo W, Wong N, Wong WL, et al. High frequency of promoter hypermethylation of RASSF1A in tumor and plasma of patients with hepatocellular carcinoma. Liver Int. 2005;25(2):266–272. doi:10.1111/j.1478-3231.2005.01084.x
49. Cai Z, Chen G, Zeng Y, et al. Comprehensive liquid profiling of circulating tumor DNA and protein biomarkers in long-term follow-up patients with hepatocellular carcinoma. Clin Cancer Res. 2019;25(17):5284–5294. doi:10.1158/1078-0432.CCR-18-3477
50. Chen L, Abou-Alfa GK, Zheng B, et al. Genome-scale profiling of circulating cell-free DNA signatures for early detection of hepatocellular carcinoma in cirrhotic patients. Cell Res. 2021;31(5):589–592. doi:10.1038/s41422-020-00457-7
51. Ono A, Fujimoto A, Yamamoto Y, et al. Circulating tumor DNA analysis for liver cancers and its usefulness as a liquid biopsy. Cell Mol Gastroenterol Hepatol. 2015;1(5):516–534. doi:10.1016/j.jcmgh.2015.06.009
52. Wang D, Xu Y, Goldstein JB, et al. Preoperative evaluation of microvascular invasion with circulating tumour DNA in operable hepatocellular carcinoma. Liver Int. 2020;40(8):1997–2007. doi:10.1111/liv.14463
53. Miller MC, Doyle GV, Terstappen LW. Significance of circulating tumor cells detected by the cellsearch system in patients with metastatic breast colorectal and prostate cancer. J Oncol. 2010;2010:617421. doi:10.1155/2010/617421
54. Ahn JC, Teng PC, Chen PJ, et al. Detection of circulating tumor cells and their implications as a biomarker for diagnosis, prognostication, and therapeutic monitoring in hepatocellular carcinoma. Hepatology. 2021;73(1):422–436. doi:10.1002/hep.31165
55. Yang ZF, Ho DW, Ng MN, et al. Significance of CD90+ cancer stem cells in human liver cancer. Cancer Cell. 2008;13(2):153–166. doi:10.1016/j.ccr.2008.01.013
56. Liu S, Li N, Yu X, et al. Expression of intercellular adhesion molecule 1 by hepatocellular carcinoma stem cells and circulating tumor cells. Gastroenterology. 2013;144(5):1031–41e10. doi:10.1053/j.gastro.2013.01.046
57. Tsuchiya N, Sawada Y, Endo I, et al. Biomarkers for the early diagnosis of hepatocellular carcinoma. World J Gastroenterol. 2015;21(37):10573–10583. doi:10.3748/wjg.v21.i37.10573
58. Espejo-Cruz ML, Gonzalez-Rubio S, Zamora-Olaya J, et al. Circulating tumor cells in hepatocellular carcinoma: a comprehensive review and critical appraisal. Int J Mol Sci. 2021;22(23). doi:10.3390/ijms222313073
59. Terris B, Cavard C, Perret C. EpCAM, a new marker for cancer stem cells in hepatocellular carcinoma. J Hepatol. 2010;52(2):280–281. doi:10.1016/j.jhep.2009.10.026
60. Kelley RK, Magbanua MJ, Butler TM, et al. Circulating tumor cells in hepatocellular carcinoma: a pilot study of detection, enumeration, and next-generation sequencing in cases and controls. BMC Cancer. 2015;15:206. doi:10.1186/s12885-015-1195-z
61. Cheng Y, Luo L, Zhang J, et al. Diagnostic value of different phenotype circulating tumor cells in hepatocellular carcinoma. J Gastrointest Surg. 2019;23(12):2354–2361. doi:10.1007/s11605-018-04067-y
62. Ye Q, Ling S, Zheng S, et al. Liquid biopsy in hepatocellular carcinoma: circulating tumor cells and circulating tumor DNA. Mol Cancer. 2019;18(1):114. doi:10.1186/s12943-019-1043-x
63. Liu HY, Qian HH, Zhang XF, et al. Improved method increases sensitivity for circulating hepatocellular carcinoma cells. World J Gastroenterol. 2015;21(10):2918–2925. doi:10.3748/wjg.v21.i10.2918
64. Zhang Y, Zhang X, Zhang J, et al. Microfluidic chip for isolation of viable circulating tumor cells of hepatocellular carcinoma for their culture and drug sensitivity assay. Cancer Biol Ther. 2016;17(11):1177–1187. doi:10.1080/15384047.2016.1235665
65. Wang S, Zhang C, Wang G, et al. Aptamer-mediated transparent-biocompatible nanostructured surfaces for hepatocellular circulating tumor cells enrichment. Theranostics. 2016;6(11):1877–1886. doi:10.7150/thno.15284
66. Guo W, Sun YF, Shen MN, et al. Circulating tumor cells with stem-like phenotypes for diagnosis, prognosis, and therapeutic response evaluation in hepatocellular carcinoma. Clin Cancer Res. 2018;24(9):2203–2213. doi:10.1158/1078-0432.CCR-17-1753
67. Zhou Y, Wang B, Wu J, et al. Association of preoperative EpCAM circulating tumor cells and peripheral Treg cell levels with early recurrence of hepatocellular carcinoma following radical hepatic resection. BMC Cancer. 2016;16:506. doi:10.1186/s12885-016-2526-4
68. Wang Z, Luo L, Cheng Y, et al. Correlation between postoperative early recurrence of hepatocellular carcinoma and mesenchymal circulating tumor cells in peripheral blood. J Gastrointest Surg. 2018;22(4):633–639. doi:10.1007/s11605-017-3619-3
69. Qi LN, Xiang BD, Wu FX, et al. Circulating tumor cells undergoing EMT provide a metric for diagnosis and prognosis of patients with hepatocellular carcinoma. Cancer Res. 2018;78(16):4731–4744. doi:10.1158/0008-5472.CAN-17-2459
70. Zhang Q, Rong Y, Yi K, et al. Circulating tumor cells in hepatocellular carcinoma: single-cell based analysis, preclinical models, and clinical applications. Theranostics. 2020;10(26):12060–12071. doi:10.7150/thno.48918
71. Sukowati CHC, Cabral LKD, Tiribelli C, et al. Circulating long and circular noncoding RNA as non-invasive diagnostic tools of hepatocellular carcinoma. Biomedicines. 2021;9(1). doi:10.3390/biomedicines9010090
72. Oura K, Morishita A, Masaki T. Molecular and functional roles of MicroRNAs in the progression of hepatocellular carcinoma-a review. Int J Mol Sci. 2020;21:21. doi:10.3390/ijms21218362
73. Wei J, Feng L, Li Z, et al. MicroRNA-21 activates hepatic stellate cells via PTEN/Akt signaling. Biomed Pharmacother. 2013;67(5):387–392. doi:10.1016/j.biopha.2013.03.014
74. Huang Z, Zhou JK, Peng Y, et al. The role of long noncoding RNAs in hepatocellular carcinoma. Mol Cancer. 2020;19(1):77. doi:10.1186/s12943-020-01188-4
75. Soda N, Rehm BHA, Sonar P, et al. Advanced liquid biopsy technologies for circulating biomarker detection. J Mater Chem B. 2019;7(43):6670–6704. doi:10.1039/c9tb01490j
76. Hung CH, Hu TH, Lu SN, et al. Circulating microRNAs as biomarkers for diagnosis of early hepatocellular carcinoma associated with hepatitis B virus. Int J Cancer. 2016;138(3):714–720. doi:10.1002/ijc.29802
77. Tsai YS, Huang CI, Tsai PC, et al. Circulating Let-7 family members as non-invasive biomarkers for predicting hepatocellular carcinoma risk after antiviral treatment among chronic Hepatitis C patients. Cancers. 2022;14(8). doi:10.3390/cancers14082023
78. Zekri AN, Youssef AS, El-Desouky ED, et al. Serum microRNA panels as potential biomarkers for early detection of hepatocellular carcinoma on top of HCV infection. Tumour Biol. 2016;37(9):12273–12286. doi:10.1007/s13277-016-5097-8
79. Loosen SH, Castoldi M, Jordens MS, et al. Serum levels of circulating microRNA-107 are elevated in patients with early-stage HCC. PLoS One. 2021;16(3):e0247917. doi:10.1371/journal.pone.0247917
80. Zhou J, Yu L, Gao X, et al. Plasma microRNA panel to diagnose hepatitis B virus-related hepatocellular carcinoma. J Clin Oncol. 2011;29(36):4781–4788. doi:10.1200/JCO.2011.38.2697
81. Yu F, Lu Z, Chen B, et al. microRNA-150: a promising novel biomarker for hepatitis B virus-related hepatocellular carcinoma. Diagn Pathol. 2015;10:129. doi:10.1186/s13000-015-0369-y
82. Xie Y, Yao Q, Butt AM, et al. Expression profiling of serum microRNA-101 in HBV-associated chronic hepatitis, liver cirrhosis, and hepatocellular carcinoma. Cancer Biol Ther. 2014;15(9):1248–1255. doi:10.4161/cbt.29688
83. Wu C, Wang X, Zhang J, et al. MicroRNA-224 expression and polymorphism predict the prognosis of Hepatitis B virus-related hepatocellular carcinoma patients after liver resection. Clin Lab. 2019;65(6). doi:10.7754/Clin.Lab.2018.181025
84. Lin XJ, Chong Y, Guo ZW, et al. A serum microRNA classifier for early detection of hepatocellular carcinoma: a multicentre, retrospective, longitudinal biomarker identification study with a nested case-control study. Lancet Oncol. 2015;16(7):804–815. doi:10.1016/S1470-2045(15)00048-0
85. Jin Y, Wong YS, Goh BKP, et al. Circulating microRNAs as potential diagnostic and prognostic biomarkers in hepatocellular carcinoma. Sci Rep. 2019;9(1):10464. doi:10.1038/s41598-019-46872-8
86. Huang J, Zheng Y, Xiao X, et al. A circulating long noncoding RNA panel serves as a diagnostic marker for hepatocellular carcinoma. Dis Markers. 2020;2020:5417598. doi:10.1155/2020/5417598
87. Li Z, Zhou Y, Yang G, et al. Using circular RNA SMARCA5 as a potential novel biomarker for hepatocellular carcinoma. Clin Chim Acta. 2019;492:37–44. doi:10.1016/j.cca.2019.02.001
88. Zhu K, Zhan H, Peng Y, et al. Plasma hsa_circ_0027089 is a diagnostic biomarker for hepatitis B virus-related hepatocellular carcinoma. Carcinogenesis. 2020;41(3):296–302. doi:10.1093/carcin/bgz154
89. Kalluri R, LeBleu VS. The biology, function, and biomedical applications of exosomes. Science. 2020;367:6478. doi:10.1126/science.aau6977
90. Chen W, Mao Y, Liu C, et al. Exosome in Hepatocellular Carcinoma: an update. J Cancer. 2021;12(9):2526–2536. doi:10.7150/jca.54566
91. He R, Wang Z, Shi W, et al. Exosomes in hepatocellular carcinoma microenvironment and their potential clinical application value. Biomed Pharmacother. 2021;138:111529. doi:10.1016/j.biopha.2021.111529
92. Nabet BY, Qiu Y, Shabason JE, et al. Exosome RNA unshielding couples stromal activation to pattern recognition receptor signaling in cancer. Cell. 2017;170(2):352–66 e13. doi:10.1016/j.cell.2017.06.031
93. Conigliaro A, Costa V, Lo Dico A, et al. CD90+ liver cancer cells modulate endothelial cell phenotype through the release of exosomes containing H19 lncRNA. Mol Cancer. 2015;14:155. doi:10.1186/s12943-015-0426-x
94. Marzan AL, Nedeva C, Mathivanan S. Extracellular vesicles in metabolism and metabolic diseases. Subcell Biochem. 2021;97:393–410. doi:10.1007/978-3-030-67171-6_15
95. Moldogazieva NT, Zavadskiy SP, Terentiev AA. Genomic landscape of liquid biopsy for hepatocellular carcinoma personalized medicine. Cancer Genomics Proteomics. 2021;18(3 Suppl):369–383. doi:10.21873/cgp.20266
96. Chitti SV, Nedeva C. Extracellular vesicles contain putative cancer biomarkers. Subcell Biochem. 2021;97:363–374. doi:10.1007/978-3-030-67171-6_13
97. Suwatthanarak T, Thiodorus IA, Tanaka M, et al. Microfluidic-based capture and release of cancer-derived exosomes via peptide-nanowire hybrid interface. Lab Chip. 2021;21(3):597–607. doi:10.1039/d0lc00899k
98. Arbelaiz A, Azkargorta M, Krawczyk M, et al. Serum extracellular vesicles contain protein biomarkers for primary sclerosing cholangitis and cholangiocarcinoma. Hepatology. 2017;66(4):1125–1143. doi:10.1002/hep.29291
99. Tseng HH, Chang JG, Hwang YH, et al. Expression of hepcidin and other iron-regulatory genes in human hepatocellular carcinoma and its clinical implications. J Cancer Res Clin Oncol. 2009;135(10):1413–1420. doi:10.1007/s00432-009-0585-5
100. Sasaki K, Kohgo Y, Ohtake T. Splicing variant of hepcidin mRNA. Vitam Horm. 2019;110:131–141. doi:10.1016/bs.vh.2019.01.006
101. Wang X, Shen H, Zhangyuan G, et al. 14-3-3zeta delivered by hepatocellular carcinoma-derived exosomes impaired anti-tumor function of tumor-infiltrating T lymphocytes. Cell Death Dis. 2018;9(2):159. doi:10.1038/s41419-017-0180-7
102. Wang H, Lu Z, Zhao X. Tumorigenesis, diagnosis, and therapeutic potential of exosomes in liver cancer. J Hematol Oncol. 2019;12(1):133. doi:10.1186/s13045-019-0806-6
103. Wang H, Hou L, Li A, et al. Expression of serum exosomal microRNA-21 in human hepatocellular carcinoma. Biomed Res Int. 2014;2014:864894. doi:10.1155/2014/864894
104. Wang W, Li H, Zhou Y, et al. Peripheral blood microvesicles are potential biomarkers for hepatocellular carcinoma. Cancer Biomark. 2013;13(5):351–357. doi:10.3233/CBM-130370
105. Li W, Xue H, Li Y, et al. HIPK3 circular RNA promotes metastases of HCC through sponging miR-338-3p to induce ZEB2 expression. Dig Dis Sci. 2021;66(10):3439–3447. doi:10.1007/s10620-020-06688-3
106. Chen Y, Chen J, Liu Y, et al. Plasma miR-15b-5p, miR-338-5p, and miR-764 as biomarkers for hepatocellular carcinoma. Med Sci Monit. 2015;21:1864–1871. doi:10.12659/MSM.893082
107. Xue X, Wang X, Zhao Y, et al. Exosomal miR-93 promotes proliferation and invasion in hepatocellular carcinoma by directly inhibiting TIMP2/TP53INP1/CDKN1A. Biochem Biophys Res Commun. 2018;502(4):515–521. doi:10.1016/j.bbrc.2018.05.208
108. Sun L, Su Y, Liu X, et al. Serum and exosome long non coding RNAs as potential biomarkers for hepatocellular carcinoma. J Cancer. 2018;9(15):2631–2639. doi:10.7150/jca.24978
109. Xu H, Chen Y, Dong X, et al. Serum exosomal long noncoding RNAs ENSG00000258332.1 and LINC00635 for the diagnosis and prognosis of hepatocellular carcinoma. Cancer Epidemiol Biomarkers Prev. 2018;27(6):710–716. doi:10.1158/1055-9965.EPI-17-0770
110. Lee YR, Kim G, Tak WY, et al. Circulating exosomal noncoding RNAs as prognostic biomarkers in human hepatocellular carcinoma. Int J Cancer. 2019;144(6):1444–1452. doi:10.1002/ijc.31931
111. Li X, Yang L, Chen LL, Biogenesis T. Functions, and challenges of circular RNAs. Mol Cell. 2018;71(3):428–442. doi:10.1016/j.molcel.2018.06.034
112. Wang S, Dong Y, Gong A, et al. Exosomal circRNAs as novel cancer biomarkers: challenges and opportunities. Int J Biol Sci. 2021;17(2):562–573. doi:10.7150/ijbs.48782
113. Nahon P, Najean M, Layese R, et al. Early hepatocellular carcinoma detection using magnetic resonance imaging is cost-effective in high-risk patients with cirrhosis. JHEP Rep. 2022;4(1):100390. doi:10.1016/j.jhepr.2021.100390
114. An J. Current status and future directions of hepatocellular carcinoma surveillance test based on cost-effective analysis. Korean J Gastroenterol. 2021;78(5):255–260. doi:10.4166/kjg.2021.142
115. Englmeier F, Bleckmann A, Bruckl W, et al. Clinical benefit and cost-effectiveness analysis of liquid biopsy application in patients with advanced non-small cell lung cancer (NSCLC): a modelling approach. J Cancer Res Clin Oncol. 2022. doi:10.1007/s00432-022-04034-w
116. Izumi D, Zhu Z, Chen Y, et al. Assessment of the diagnostic efficiency of a liquid biopsy assay for early detection of gastric cancer. JAMA Netw Open. 2021;4(8):e2121129. doi:10.1001/jamanetworkopen.2021.21129
117. Wu CF, Lin L, Mao YP, et al. Liquid biopsy posttreatment surveillance in endemic nasopharyngeal carcinoma: a cost-effective strategy to integrate circulating cell-free Epstein-Barr virus DNA. BMC Med. 2021;19(1):193. doi:10.1186/s12916-021-02076-4
118. van der Poort EKJ, van Ravesteyn NT, van den Broek JJ, et al. The early detection of breast cancer using liquid biopsies: model estimates of the benefits, harms, and costs. Cancers. 2022;14(12). doi:10.3390/cancers14122951
119. Roy D, Lucci A, Ignatiadis M, et al. Cell-free circulating tumor DNA profiling in cancer management. Trends Mol Med. 2021;27(10):1014–1015. doi:10.1016/j.molmed.2021.07.001
120. Li X, Wang H, Li T, et al. Circulating tumor DNA/circulating tumor cells and the applicability in different causes induced hepatocellular carcinoma. Curr Probl Cancer. 2020;44(2):100516. doi:10.1016/j.currproblcancer.2019.100516
121. Prospective suRveillance for very Early hepatoCellular cARcinoma(PreCar) expert panel. [Expert consensus on early screening strategies for liver cancer in China]. Zhonghua Gan Zang Bing Za Zhi. 2021 Jun 20;29(6):515-522. Chinese. doi:10.3760/cma.j.cn501113-20210605-00264
122. Wu J, Hu S, Zhang L, et al. Tumor circulome in the liquid biopsies for cancer diagnosis and prognosis. Theranostics. 2020;10(10):4544–4556. doi:10.7150/thno.40532
123. Huang Z, Hua D, Hu Y, et al. Quantitation of plasma circulating DNA using quantitative PCR for the detection of hepatocellular carcinoma. Pathol Oncol Res. 2012;18(2):271–276. doi:10.1007/s12253-011-9438-z
124. Wen Y, Han J, Chen J, et al. Plasma miRNAs as early biomarkers for detecting hepatocellular carcinoma. Int J Cancer. 2015;137(7):1679–1690. doi:10.1002/ijc.29544
125. El Sharkawi FZ, Awad MS, Elagawy W, et al. Circular RNAs 0064286 and 0000475: potential diagnostic biomarkers in hepatocellular carcinoma. Asian Pac J Cancer Prev. 2021;22(9):3039–3044. doi:10.31557/APJCP.2021.22.9.3039
126. Guo W, Yang XR, Sun YF, et al. Clinical significance of EpCAM mRNA-positive circulating tumor cells in hepatocellular carcinoma by an optimized negative enrichment and qRT-PCR-based platform. Clin Cancer Res. 2014;20(18):4794–4805. doi:10.1158/1078-0432.CCR-14-0251
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.