Back to Journals » Cancer Management and Research » Volume 12
The Accuracy of Three-Dimensional Planned Bone Tumor Resection Using Patient-Specific Instrument
Authors Müller DA ![]() , Stutz Y
, Stutz Y ![]() , Vlachopoulos L, Farshad M
, Vlachopoulos L, Farshad M ![]() , Fürnstahl P
, Fürnstahl P ![]()
Received 20 August 2019
Accepted for publication 23 June 2020
Published 29 July 2020 Volume 2020:12 Pages 6533—6540
DOI https://doi.org/10.2147/CMAR.S228038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chien-Feng Li
Daniel A Müller,1 Yannik Stutz,1 Lazaros Vlachopoulos,1 Mazda Farshad,1 Philipp Fürnstahl2
1Department of Orthopedic Surgery, Balgrist University Hospital, Zürich 8008, Switzerland; 2Computer Assisted Research & Development Group, Balgrist University Hospital, Zürich 8008, Switzerland
Correspondence: Daniel A Müller
Balgrist University Hospital, Forchstrasse 340, Zürich CH-8008, Switzerland
Tel +41 44 386 11 11
Fax +41 44 386 11 09
Email [email protected]
Introduction: Although treatment of bone tumors is multidisciplinary, the complete surgical resection of bone tumors remains the mainstay of the treatment. Patient-specific instruments (PSI) are personalized tools, which help the surgeon to perform tumor resections accurately. The aim of this study is to evaluate how precise the planned resection can be intraoperatively executed with the use of PSI.
Patients and Methods: Eleven patients who underwent a resection of bone tumor using PSI were analyzed. A preoperative model of the tumor and the affected bone was created from acquired CT scans and MRI. After defining the resection planes, PSI were produced by a 3D printer. The resected piece of bone was scanned and imported in the original planning model enabling the assessment of the distance between the planned resection plane and the realized osteotomy in every direction.
Results: In overall, the combined error of an osteotomy ranges from 0.74 ± 0.96 mm to 3.60 ± 2.46 mm. The average errors observed in situations with one resection plane (simple osteotomy) are lower than in complex curved osteotomies with multiple planes, in which we also found a greater variance.
Conclusion: 3D planned bone tumor resections using PSI show promising results for precise resection at different anatomical regions. Even if the found error range in this series is slightly higher than reported, PSI remain a valuable tool to facilitate complex bone tumor resections.
Keywords: bone tumor, patient-specific instruments, 3D resection, surgical guide, limb salvage surgery
Introduction
Although the treatment of primary bone tumors is often multidisciplinary, the complete surgical resection of the tumor remains the mainstay of the treatment. In malignant bone tumors, a wide resection with safe tumor margins is the most prognostic factor for a successful outcome. However, excessive resection may alter or reduce reconstructive options and may lead to negative functional outcomes.1 Whenever possible, joints, a normal bone stock, and important ligaments and tendons should be preserved to enable satisfying postoperative function of the salvaged limb. Thus, an accurate planning and a high precision in the surgical procedure is mandatory. But even experienced surgeons do not achieve a satisfactory accuracy with freehand osteotomies, especially around complex anatomical sites such as the pelvis.2 Several techniques have been described for helping the surgeon to perform bone tumor resections more precisely, such as computer-assisted surgical navigation, robot-assisted surgery and use of patient-specific instruments.3–7 Patient-specific instruments (PSI) are personalized tools that guide the saw, chisel or drill in a specific, pre-designed cutting path. The first clinical applications of PSI in the treatment of bone tumors have been reported recently and the preliminary results are promising.8–12 However, present case studies focus mainly on the description of the technique and its surgical feasibility. Reliable information about in vivo accuracy is lacking completely.
The aim of this study is to evaluate how precise the planned resection can be intraoperatively executed with the use of PSI.
Patients and Methods
Study Population
We introduced the concept of PSI for tumor resections in the beginning of 2015 in our institution. For reasons of internal quality control, we have planned to closely monitor the first 10 cases. In this prospective cohort study, all patients diagnosed of primary bone tumor from March 2015 to September 2017, in whom the resection was performed by PSI in our institution (Balgrist University Hospital Zurich, Switzerland), were included. During this period, the previously defined minimum number of at least 10 patients were reached. Since several patients were treated simultaneously towards the end, the total number of patients included was 12. The inclusion criteria were met if there was a primary bone tumor for which resection by freehand osteotomy was considered difficult. Patients who were treated with curettage or had unpretentious tumor localizations, such as diaphyseal tumors, were not considered for PSI and therefore excluded from this study. The included 12 patients gave written consent for participation in the present study. Furthermore, we obtained the approval from our local ethical board (BASEC-Nr. 2017–01810).
The histological diagnosis was verified by a preoperative core needle biopsy and the treatment protocol was defined individually by an interdisciplinary sarcoma board.
An overview of the patient characteristics is shown in Table 1. The mean age of the patients was 44.9 years (12 to 65 years). For further analysis, the patients were divided into two groups according to the complexity of the planned resection. We assigned the patient to group A if there was a simple resection plane necessitating only one PSI. If there was more than one PSI necessary enabling a complex curved osteotomy with several resection planes, the patient was included in group B.
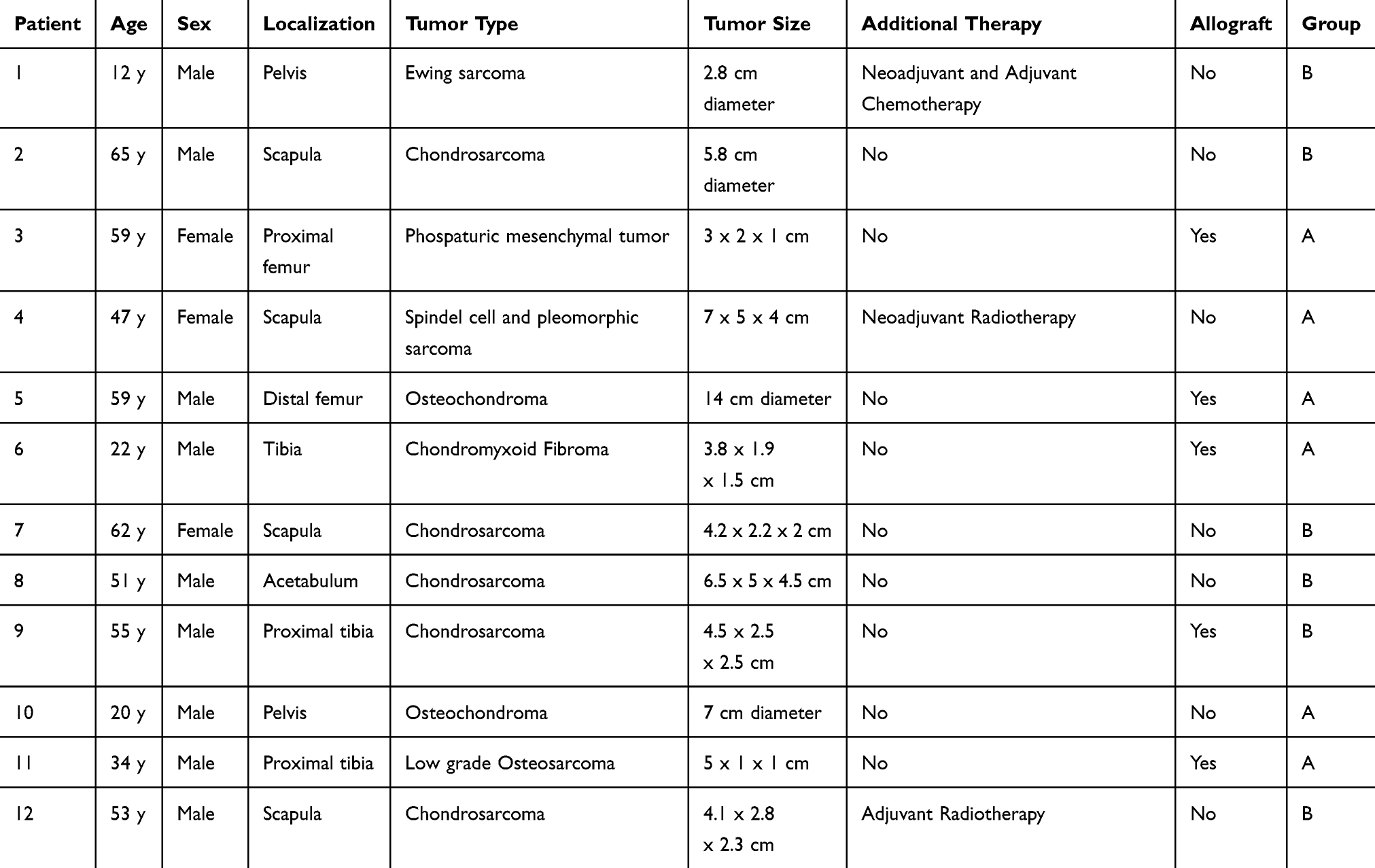 |
Table 1 Patient Characteristics |
Preoperative Planning
Computer tomography (CT; axial resolution 1–1.25mm) and magnetic resonance imaging (MRI; axial resolution 0.9–4.5 mm) scans of the affected bone were acquired using clinical standard protocols. The axial resolution was chosen depending on the anatomical region. The bone models are extracted from CT scans using the segmentation functionality. The pathological bone was segmented by using the global thresholding and region growing functionality of the Mimics software (Materialise, Leuven, Belgium)13 to obtain a three-dimensional (3D) model of the bone (Figure 1A and B). The bone was pre-segmented by the software and then edited manually to achieve highest possible precision. The tumor was identified and segmented in the MRI data for better visualization of the extraosseous spreading. To this end, the tumor outline was manually masked slice by slice. A Marching Cube algorithm was applied to the segmented data to generate 3D triangular surface models of the bone and the tumor.
 |
Figure 1 Preoperative Planning. Preoperative planning of patient Nr 6: Chondromyxoid Fibroma. (A) Preoperative segmented bone from CT scan. (B) Fusion of the segmented bone and the segmented tumor. (C) Planned resection planes. (D) Creation of a cutting guide, so drill holes correspond to the resection planes. (E) The osteotomy is performed by drilling. Therefore two corresponding guides with a small offset of the drilling holes are needed to enable a complete cut through the bone. (F) Allograft bone (purple) aligned on the host bone (green). (G) Resection guide for trimming the allograft bone. |
Next, we imported the models into the preoperative planning software CASPA (Balgrist CARD AG, Zurich, Switzerland) to plan the surgery on the computer. This software was developed in our institution and has already been evaluated and published for 3D planning in orthopedic surgery.13–17 The surgeon defined the resection planes by specifying consecutive line segments on the bone surface. The line segments were automatically extruded to create the corresponding 3D osteotomy planes of 2 mm thickness (Figure 1C). According to the complexity of the surgery, either one planar resection plane (group A) or a compound plane consisting of several combined planes (group B) were created. After the exact resection was determined, the reconstruction with a massive bone allograft was also planned if needed. For this purpose, a 3D model of the allograft was obtained by CT acquisition and segmentation and imported into the preoperative planning software. The allograft model was superimposed with the pathological bone as accurate as possible (Figure 1F). The same osteotomy planes as for the resection were now applied to the allograft such that it fitted perfectly in the bony defect (Figure 1G).
Patient-Specific Instruments
PSI have been described as an intraoperative aid to support the surgeon in a more precise surgical execution of the resection planning.8–12 The PSI concept offers unique advantages because it is highly flexible and can be modified according to the individual patient conditions.
PSI were created based on the 3D resection planes. We used a technique in which complex osteotomy planes can be performed by perforating the bone with consecutive drills of instead of saw blade (a detailed description of the technique has been published before15). Dependent on the case we used either 2.0 mm or 2.5 mm drill bits, modelled by cylinder objects in the preoperative planning. PSI with drill sleeves corresponding to the cylinders were designed to define the exact position, direction and depth of the drill holes. These sleeves were combined in a guide body, whose undersurface was molded as a negative of the bone surface (Figure 1D). The anatomy-specific undersurface helped the surgeon in the operation to precisely determine the correct position of the PSI. In long bones, the exact positioning of PSI guides may be difficult sometimes. If there was a doubt of the correct positioning intraoperatively, distances from the guides to clear anatomical landmarks were measured and compared to the preoperative planning. Each PSI was produced twice with slightly offset drill holes to achieve a dense perforation of the bone (Figure 1E). The PSI were manufactured by the company Medacta (Castel San Pietro, Switzerland) using a selective laser sintering device (Formiga P100, EOS GmbH, Germany). Biocompatible polyamide (PA2200) was used as raw material.11,13
Postoperative Evaluation
A CT scan of the resection specimen was acquired before sending to the histological evaluation (Figure 2A). In two patients we decided not to perform these CT scans, because the histological analysis was time sensitive (patient nr 1 and 11). Instead, we performed postoperative CT scans of the affected bones in these cases. (Figure 2F).
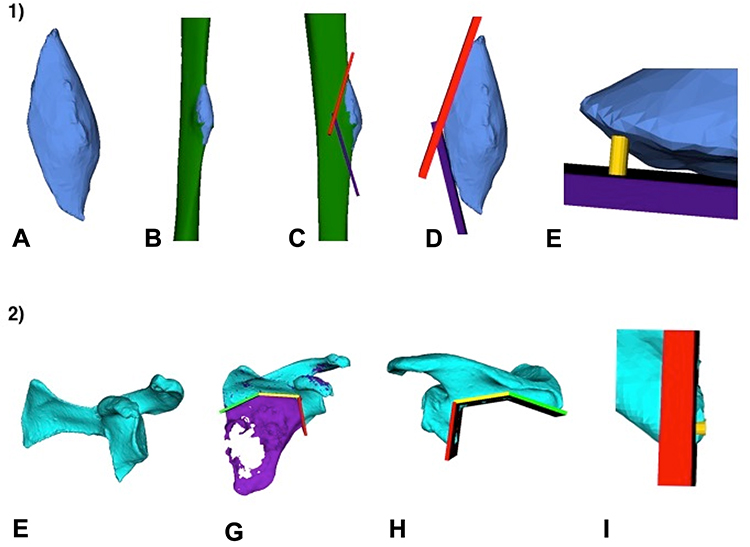 |
Figure 2 Postoperative analysis. First row (1): The accuracy analysis was performed based on the resection specimen. (A) 3D model of the resection specimen gained from CT scan. (B) Resected part aligned on the preoperatively segmented bone. (C) The previous planned cutting planes displayed in the model. (D) The original bone is hidden for simplification of the measurement. (E) Cylindrical body between planned and performed resection to evaluate the distance. Second row (2): The accuracy analysis was performed based on the residual bone. Case in which remaining bone in the patient was segmented. (F) 3D model of the residual bone gained from a CT scan after the resection. (G) Postoperative result aligned with the preoperative planning and the corresponding resection planes. (H) Postoperative residual bone in comparison to the planned resection planes. (I) Cylindrical body between planned and performed resection to evaluate the distance. |
Segmentation and 3D model generation was performed in the same way as for the preoperative CT scans. The postoperative 3D models were approximately aligned with the preoperative planning in a manual fashion, followed by an automatic alignment correction using the iterative closest point (ICP) registration functionality of CASPA (Figure 2B and G). In the end, manual fine-tuning was executed if the models were not aligned perfectly. After alignment, the difference between planned and executed osteotomies could be measured (Figure 2C, D and H). The maximum distances between the osteotomy planes and the postoperative model were measured as follows: first, compound planes were divided into sections of straight single planes. Next cylindrical bodies were inserted between the postoperative model and the section plane. The base of the cylinder was placed exactly on the executed cutting plane. The length was then continuously increased vertically until the surface of the cylinder touched the planned cutting plane for the first time (Figure 2E and I).
The deviations were analyzed on both sides for all section planes in order to calculate the average “inside error” and the average “outside error” for each patient.
In order to judge the accuracy independently of the direction, we have added the absolute values of inside and outside errors and calculated the average from them. We defined this value, consisting of the average of all errors added, as a combined error.
Results
One patient had to be excluded from analysis (patient nr. 12) because of an unexpected tumor progress compared to the preoperative imaging. In the other eleven cases, the surgery could be performed as planned. There were no surgical complications and during a mean follow-up of 17.4 months (range: 4 to 32 months) no local recurrence occurred. As the osteotomy plane was divided in several single planes both inside and outside errors were found in the same assessed osteotomy (Figure 3). All measured deviations are shown in Table 2. The biggest errors found in a subdivision plane range from +7.7 mm (inside error) to −6.4 mm (outside error). Considering all subsections of the osteotomy together, the largest mean inside error was +3.34 ± 2.74 mm and the largest mean outside error −3.86 ± 2.12 mm, respectively. On the other hand, the smallest mean inside error was +0.16 ± 0.25 mm and the smallest mean outside error was −0.70 ± 0.70 mm. Overall, the combined error of osteotomy ranged from 0.74 ± 0.96 mm to 3.60 ± 2.46 mm. Again, for the combined error the absolute amounts of inside and outside deviations were added together, to prevent the errors from being cancelled out due to the different directions.
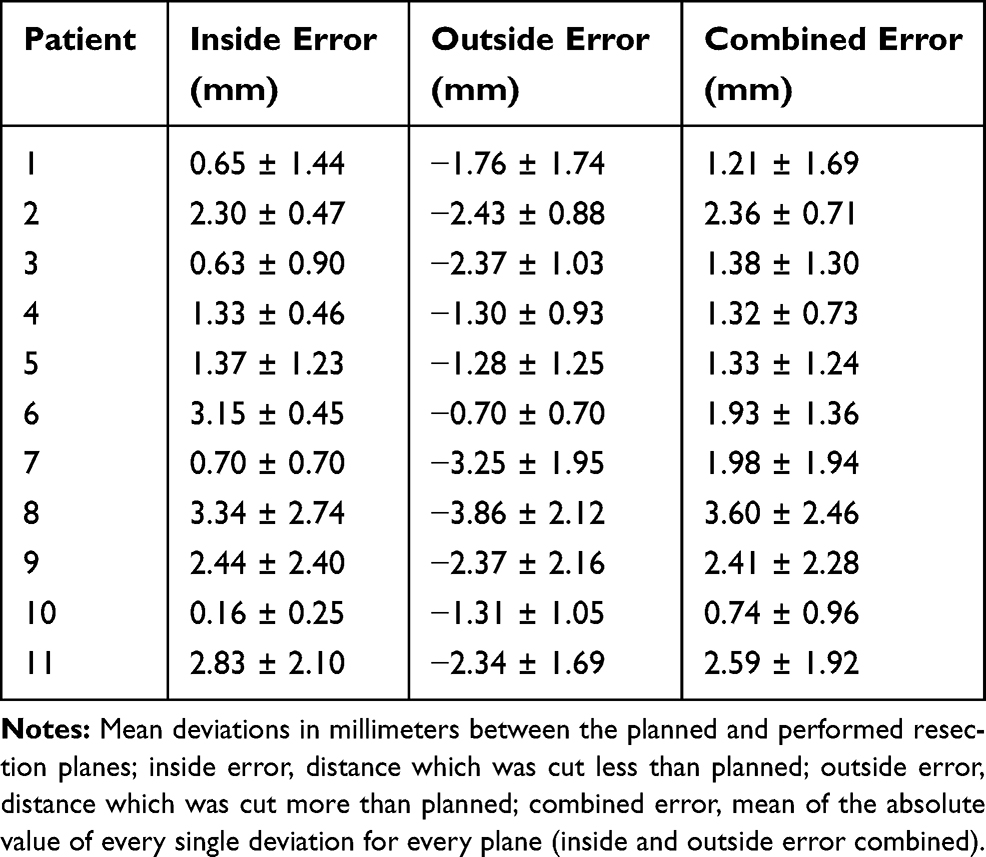 |
Table 2 Resection Errors |
 |
Figure 3 Assessment of curved plains. (A) Example of a curved resection plane. (B) The curved plane was divided into several adjacent straight planes. The distance between the planned and performed resection plane was measured for every section. |
Table 3 highlights the difference between the two patient groups. As expected, the average inside and outside errors observed in group A are both lower than in group B. In group B we also found a greater variance of the deviations. Because of the small sample size, the differences were not statistically significant.
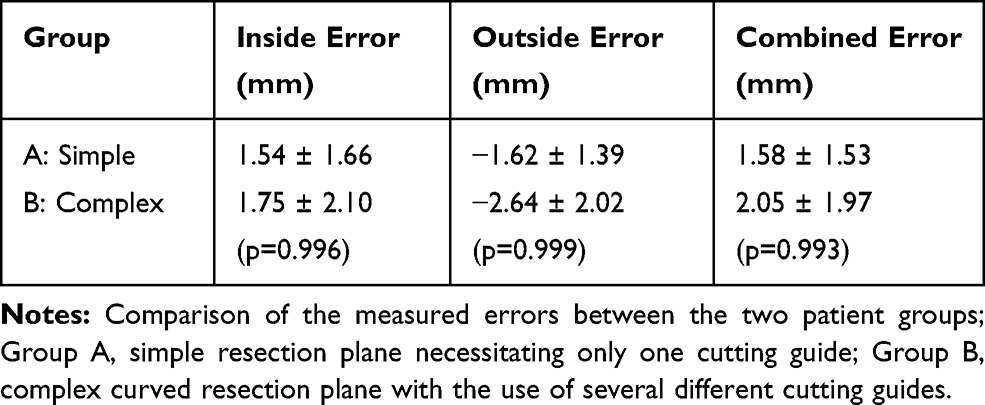 |
Table 3 Differences Between Simple and Complex Resections |
The histological laboratory tests revealed tumor free margins (R0 resection) in all patients except for patient nr. 5. In this case microscopic cartilaginous tissue was found at the osteotomy plane (R1 resection). As the diagnosis was a benign osteochondroma with no signs of secondary dedifferentiation, the resection was planned very close and no further treatment was needed after the surgery.
Discussion
Executing a preoperative plan as accurately as possible is crucial in orthopaedic tumor surgery to achieve negative surgical margins and thus decrease the likelihood of local recurrence. However, resecting significantly more tissue than planned, out of concern to leaving a positive margin, can compromise patient function and successful reconstruction.7
Since there have been no attempts to measure and quantify the in vivo accuracy of PSI guided resections, we had to develop a measurement method from scratch. We searched for an analytical procedure that already worked in another setting. The here presented type of measurements have been used to verify the accuracy of bone malunion correction in orthopaedic surgery.18,19
So far, there is only one experimental study directly comparing the accuracy between PSI and optical navigation with respect to bone tumor surgery: While both achieved acceptable accuracy, surgeons described intra-operative use of PSI as simpler. Moreover, the average time required for resection was significantly lower in the PSI group.5 Another advantage of PSI lies in the navigation of allograft trimming into the shape of the osseous defect when a biological reconstruction with a massive bone allograft has to be performed.
While the previous reports agree on the surgical advantages of PSI, the information on the intraoperative precision of the technique remains very sparse. The scientific community considers this information as crucial in order to know the limits of the technique. The aim of our study was therefore to quantify exactly the difference between planned and executed resection and to identify possible difficulties. Overall, we found a mean error up to 3.60 ± 2.46 mm. Regarding small subsections of the osteotomy plane, the deviations can even be almost twice as high at certain points (up to 7.7mm).
To the best of our knowledge, only one study exists that has measured the in vivo accuracy of PSI for tumor resections.12 The authors retrospectively reviewed 12 patients, who underwent limb salvage surgery using a 3D‐printed guide at a single institution. They compared the actual and planned distances between the cutting surface and tumor, which were reported in the final pathological report. A maximum error of 3 mm is reported. Their published accuracy of the resection varies between 0 and 3mm. In their study no postoperative 3D model was generated to compare to the previous-planned resection. Park et al compared their planned margins to the reported histological margins. This is an easy and good feasible concept but compares two completely different measuring techniques. The methods used in our study may provide additional information for calculating errors in planned and executed resection. The reason for our slightly higher resection error in implementing intraoperatively the planning can have various causes. The difference can be based on the different measurement techniques or on the complexity of the cases. Not unexpectedly, we were able to show that complex osteotomies with several PSI show a greater variance of errors with higher outliers than simple resections with one PSI. Looking only at the patient group A who underwent a quite straightforward surgery, the results are even better than reported in the previous study.
In all but one patient tumor-free resections margins were achieved. However, it should be mentioned that a benign osteochondroma was diagnosed in the only patient with microscopic incomplete resection. Thus, a very close resection was planned to protect the surrounding tissue. The patient did not need any further treatment.
Overall no surgical complication related to the use of PSI occurred. However, a known disadvantage of the presented technique was also confirmed in this study. The overall 3D planning including bone segmentation and the design of the PSI is time consuming. On average, these steps take one to two days. Additionally, a production time of 2 week has to be respected. One patient showed a relevant local progression of the tumor during this time. Therefore, the PSI could not be used during the surgery and a conventional free hand osteotomy had to be performed. The planning time can be further reduced with software improvement and increasing experience, but the production time will remain a critical point in the future.
The findings of this study should be interpreted with due consideration of some limitations. First, the rarity of bone tumors unavoidably leads to a heterogenous study and impedes a good matching control group. Secondly, the follow up period was too short to definitely evaluate the local recurrence rate and the overall prognosis.
We are convinced that the integration of the resection specimen into the 3D computer model allows a very accurate and thorough evaluation. Our measurement shows that the results so far probably overestimate the accuracy of the resections with PSI. There is always a deviation in two directions because too much or too little bone can be removed by mistake. For this purpose, we calculated the combined error consisting of the addition of the absolute values of all directional deviations. This is the first time as such considerations were taken into account in analyzing the errors. As there are no previous experiences or descriptions of the used methodology in tumor surgery, further validation of our reported values is needed in the future.
Conclusion
3D planned bone tumor resections using PSI are safe and show promising results for precise resection at different anatomical regions. The found error range is still very small and PSI therefore remain a valuable tool to facilitate complex bone tumor resections.
Ethical Approval
The presented study was approved by the local ethical board (BASEC-Nr. 2017- 01810)
Disclosure
Prof. Dr. Mazda Farshad reports grants from Medacta, during the conduct of the study. The Patient-Specific Instrumentation has been largely developed at Balgrist University Hospital in a cooperation of the CARD research team and the CARD company (Balgrist Company). Latter has recently been sold to Medacta international. Dr Philipp Fürnstahl reports grants from University Hospital Balgrist, during the conduct of the study. The authors report no other conflicts of interest in this work.
References
1. Han I, Lee YM, Cho HS, Oh JH, Lee SH, Kim HS. Outcome after surgical treatment of pelvic sarcomas. Clin Orthop Relat Res. 2010;2(3):160–166. doi:10.4055/cios.2010.2.3.160
2. Cartiaux O, Docquier P-L, Paul L, et al. Surgical inaccuracy of tumor resection and reconstruction within the pelvis: an experimental study. Acta Orthop. 2008;79(5):695–702. doi:10.1080/17453670810016731
3. Wong K-C, Niu X, Xu H, Li Y, Kumta S. Computer navigation in orthopaedic tumour surgery. Adv Exp Med Biol. 2018;1093(3):315–326. doi:10.1007/978-981-13-1396-7_24
4. Jeys L, Matharu GS, Nandra RS, Grimer RJ. Can computer navigation-assisted surgery reduce the risk of an intralesional margin and reduce the rate of local recurrence in patients with a tumour of the pelvis or sacrum? Bone Joint J. 2013;95-B(10):1417–1424. doi:10.1302/0301-620X.95B10.31734
5. Wong K-C, Sze K-Y, Wong IO-L, Wong C-M, Kumta S-M. Patient-specific instrument can achieve same accuracy with less resection time than navigation assistance in periacetabular pelvic tumor surgery: a cadaveric study. Int J CARS. 2016;11(2):307–316. doi:10.1007/s11548-015-1250-x
6. Cartiaux O, Paul L, Docquier P-L, Raucent B, Dombre E, Banse X. Computer-assisted and robot-assisted technologies to improve bone-cutting accuracy when integrated with a freehand process using an oscillating saw. J Bone Joint Surg. 2010;92(11):2076–2082. doi:10.2106/JBJS.I.00457
7. Khan F, Pearle A, Lightcap C, Boland PJ, Healey JH. Haptic robot-assisted surgery improves accuracy of wide resection of bone tumors: a pilot study. Clin Orthop Relat Res. 2013;471(3):851–859. doi:10.1007/s11999-012-2529-7
8. Bellanova L, Paul L, Docquier P-L. Surgical guides (patient-specific instruments) for pediatric tibial bone sarcoma resection and allograft reconstruction. Sarcoma. 2013;2013(4):1–7. doi:10.1155/2013/787653
9. Gouin F, Paul L, Odri GA, Cartiaux O. Computer-assisted planning and patient-specific instruments for bone tumor resection within the pelvis: a series of 11 patients. Sarcoma. 2014;2014(270):1–9. doi:10.1155/2014/842709
10. Ma L, Zhou Y, Zhu Y, et al. 3D-printed guiding templates for improved osteosarcoma resection. Sci Rep. 2016;6(1):E959. doi:10.1038/srep23335
11. Jentzsch T, Vlachopoulos L, Fürnstahl P, Müller DA, Fuchs B. Tumor resection at the pelvis using three-dimensional planning and patient-specific instruments: a case series. World J Surg Oncol. 2016;14(1):14. doi:10.1186/s12957-016-1006-2
12. Park J-W, Kang HG, Lim KM, Park DW, Kim JH, Kim HS. Bone tumor resection guide using three-dimensional printing for limb salvage surgery. J Surg Oncol. 2018;118(6):898–905. doi:10.1002/jso.25236
13. Fürnstahl P, Vlachopoulos L, Schweizer A, Fucentese SF, Koch PP. Complex osteotomies of tibial plateau malunions using computer-assisted planning and patient-specific surgical guides. J Orthop Trauma. 2015;29(8):e270–e276. doi:10.1097/BOT.0000000000000301
14. Vlachopoulos L, Schweizer A, Meyer DC, Gerber C, Fürnstahl P. Three-dimensional corrective osteotomies of complex malunited humeral fractures using patient-specific guides. J Shoulder Elbow Surg. 2016;25(12):2040–2047. doi:10.1016/j.jse.2016.04.038
15. Schweizer A, Fürnstahl P, Nagy L. Three-dimensional correction of distal radius intra-articular malunions using patient-specific drill guides. J Hand Surg Am. 2013;38(12):2339–2347. doi:10.1016/j.jhsa.2013.09.023
16. Weigelt L, Fürnstahl P, Hirsiger S, Vlachopoulos L, Espinosa N, Wirth SH. Three-dimensional correction of complex ankle deformities with computer-assisted planning and patient-specific surgical guides. J Foot Ankle Surg. 2017;56(6):1158–1164. doi:10.1053/j.jfas.2017.05.025
17. Vlachopoulos L, Schweizer A, Meyer DC, Gerber C, Fürnstahl P. Computer-assisted planning and patient-specific guides for the treatment of midshaft clavicle malunions. J Shoulder Elbow Surg. 2017;26(8):1367–1373. doi:10.1016/j.jse.2017.02.011
18. Roner S, Vlachopoulos L, Nagy L, Schweizer A, Fürnstahl P. Accuracy and early clinical outcome of 3-dimensional planned and guided single-cut osteotomies of malunited forearm bones. J Hand Surg Am. 2017;42(12):
19. Hirsiger S, Schweizer A, Miyake J, Nagy L, Fürnstahl P. Corrective osteotomies of phalangeal and metacarpal malunions using patient-specific guides: CT-based evaluation of the reduction accuracy. Hand. 2018;13(6):627–636. doi:10.1177/1558944717726135
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.