")
Back to Journals » Clinical and Experimental Gastroenterology » Volume 16
Tenapanor in the Treatment of Irritable Bowel Syndrome with Constipation: Discovery, Efficacy, and Role in Management
Authors Herekar A, Shimoga D, Jehangir A, Shahsavari D, Yan Y, Karunaratne TB , Sharma A
Received 14 December 2022
Accepted for publication 29 May 2023
Published 7 June 2023 Volume 2023:16 Pages 79—85
DOI https://doi.org/10.2147/CEG.S384251
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Santosh Shenoy
Anam Herekar, Dhanush Shimoga, Asad Jehangir, Dariush Shahsavari, Yun Yan, Tennekoon Buddhika Karunaratne, Amol Sharma
Department of Medicine, Augusta University, Augusta, GA, USA
Correspondence: Amol Sharma, Medical College of Georgia, Augusta University, 1120 15th Street, AD 2226, Augusta, GA, 30912, USA, Email [email protected]
Abstract: Irritable bowel syndrome (IBS) is a common disorder of gut–brain interaction (DGBI). IBS significantly impacts the quality of life of patients. Since its pathogenesis is unclear and can be multifactorial, it highlights the need for new and improved pharmaceutical drugs that not only improve bowel symptoms, but also address global IBS symptoms, such as abdominal pain. Tenapanor, a recently Food & Drug Administration (FDA)-approved medication for IBS with constipation (IBS-C), is a small molecule inhibitor of the sodium/hydrogen exchanger isoform 3 (NHE3) that inhibits the absorption of sodium and phosphate in the gastrointestinal tract, resulting in fluid retention and softer stool. Furthermore, tenapanor reduces intestinal permeability to improve visceral hypersensitivity and abdominal pain. Due to its recent approval, tenapanor was not included in the recent IBS guidelines, however, it may be considered for IBS-C patients failing first-line treatment of soluble fiber. In this review article, we aim to provide in-depth information to the reader regarding the design of tenapanor, its development through Phase I, II and III randomized clinical trials, and its role in the treatment of IBS-C.
Keywords: irritable bowel syndrome, irritable bowel syndrome with constipation, IBS, IBS-C, constipation, tenapanor
Introduction
Irritable bowel syndrome (IBS) is a prevalent disorder of gut–brain interaction (DGBI). DGBIs were formerly known as functional gastrointestinal disorders (FGID). IBS is abdominal pain occurring at least once a week over the prior 3 months associated with change in stool frequency, stool form and/or relief or worsening of pain related to defecation occurring for more than 6 months according to the updated Rome IV international consensus criteria.1 Rome IV criteria transitioned from the vague terminology of “abdominal discomfort” to “abdominal pain” in its updated definition for IBS. The worldwide prevalence of IBS is 10.1% when the Rome III criteria are used, however, falls to 3.8% when Rome IV criteria are used.2 Nonetheless, IBS significantly impacts the quality of life of patients, rates of absenteeism, and work productivity strongly correlates to GI-specific anxiety.3 IBS is associated with significant economic burden, the direct cost per-patient ranging from $1562 to $7547 per year.4 IBS makes up 5% of the referrals to gastroenterologists in the US, UK, and Canada.5 For unclear reasons, IBS more frequently affects women and patients younger than 50 years old.5 In patients with IBS with constipation (IBS-C), more than a quarter of stools must be consistent with constipation (Bristol stool scale [BSS] type 1 or 2).1
The last decade has seen many therapeutic advancements in the treatment of IBS-C. Nonetheless, there are limited pharmacological treatment options for IBS-C patients refractory to secretagogues. Tegaserod, a 5-HT4 agonist, may be considered in a select population of women younger than 65 years with minimal cardiovascular risk factors and recommendations for its use are based on low quality of evidence.6 However, recently the manufacturer withdrew the New Drug Application (NDA) for tegaserod, making it unavailable for IBS-C patients in the United States. A new pharmacological agent, tenapanor, has shown promise for patients with IBS-C. The aim of this review article is to understand the discovery, drug development, mechanism of action, and role in management for IBS-C patients.
Drug Design and Development of Tenapanor
Tenapanor is a small molecule inhibitor of the sodium/hydrogen exchanger isoform 3 (NHE3), which is expressed on the apical surface of the small intestine and colon.7 NHE3 facilitates the absorption of sodium and phosphate in the gastrointestinal tract. Inhibition of NHE3 by tenapanor promotes colonic fluid retention and softer stool (Figure 1). This contrasts with secretagogues, which promote colonic fluid secretion. Tenapanor has minimal systemic availability. Tenapanor was originally developed to treat hyperphosphatemia in patients on hemodialysis. In a Phase 3 randomized controlled trial (RCT) designed to assess safety and tolerability of tenapanor in dialysis patients with hyperphosphatemia, the most common adverse event was diarrhea in 39.4% of subjects. In all subjects, mean bowel movement weekly frequency increased by 2.8 from baseline, revealing tenapanor’s benefit to constipated dialysis subjects.8
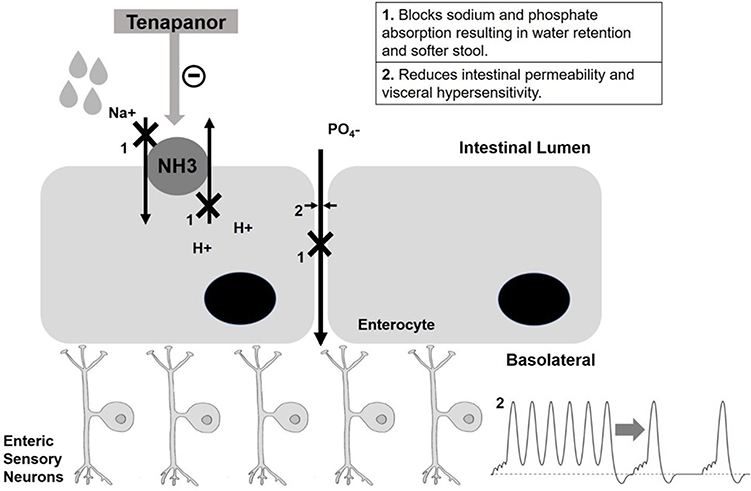 |
Figure 1 Tenapanor’s mechanism of action. Tenapanor inhibits NH3 that results in sodium retention in intestinal lumen. It also blocks phosphate absorption resulting in water retention and softer stools. It reduces visceral hypersensitivity. Na+, sodium ions; H+, hydrogen ions; PO4 –, phosphate; NH3, sodium/hydrogen ion exchanger isoform-3. |
The safety, tolerability, pharmacodynamics, and pharmacokinetics of tenapanor for hyperphosphatemia in dialysis patients were studied in a Phase 1, double-blind, randomized, placebo-controlled trial conducted in healthy Japanese volunteers and some Caucasians.9 The participants were either given 180 mg as a single dose or one of four doses (15, 30, 60, 90mg) twice daily over 7 days and compared to placebo. The Caucasian group was assigned to the 90 mg twice daily versus placebo. Tenapanor was well-tolerated with only 16 of 68 study participants (4 of them in placebo) reporting mild symptoms of nausea, abdominal pain, headache and diarrhea. The 30, 60 and 90mg treatment arms of tenapanor had mean daily stool sodium excretion of 30 mmol, compared with 4 mmol/day for placebo. Tenapanor also resulted in an increase in stool phosphorus excretion of 0.8–8.0 mmol/day and decrease in urinary phosphate excretion of 6.1–10.2 mmol/day compared to placebo.
Translational in vivo rodent experiments of human small intestinal stem cell–derived enteroid monolayers demonstrate that tenapanor reduces intestinal phosphate absorption by modulating tight junctions. This, in turn, increases transepithelial electrical resistance (TEER) and reduces intestinal permeability (Figure 1). An animal study using an established model of visceral sensitivity using acetic acid sensitized rats further explored the effects of tenapanor on colonic hypersensitivity in response to colorectal distension.10 Tenapanor reversed the increased visceral motor response in this animal model when compared to polyethylene glycol (PEG). Tenapanor also resulted in reversal of neuronal hyperexcitability seen in single-patch clamp experiments of colon-specific dorsal root ganglia (DRG). Furthermore, rats treated with tenapanor also had reduced DRG neuronal hyperexcitability when exposed to capsaicin, suggesting drug effect on TRPV1 (transient receptor potential vanilloid type 1) nociceptive signaling. Another study examining colonic monolayer culture from IBS-C subjects found that tenapanor also reduced TEER after exposure to TNF-a, IL-6, fecal supernatants from IBS patients, improving colonic permeability and reducing inflammation and hyperexcitability of sensory neurons.11
Phase I Study: Drug Safety and Pharmacodynamics
Two phase 1 single-center, double-blinded, randomized, dose-ranging, placebo-controlled trials were conducted in healthy volunteers between November 2010 and October 2011.12 The single ascending dose (SAD) phase of the study evaluated tenapanor with random subject assignment to one of five doses (10 mg, 50 mg, 150 mg, 450 mg and 900 mg) compared to placebo. The multiple ascending dose (MAD) study evaluated tenapanor with random subject assignment to one of four tenapanor daily doses (3 mg, 10 mg, 30 mg and 100 mg) for 7 days compared to placebo. The dose regimen study evaluated seven different dose regimens of tenapanor (15 mg b.i.d, 30 mg q.d, 30 mg b.i.d, 30 mg t.i.d, 60 mg b.i.d, escalating b.i.d. dose and 30 mg b.i.d. with psyllium).
No deaths or serious adverse events (SAE) were reported in either study. All of adverse events (AE) were either mild or moderate and GI-related. AEs were uncommon in the SAD-MAD study (14 in tenapanor and 3 in placebo). In the dose regimen study, 38 participants (30 tenapanor) experienced AEs. Twenty-five volunteers (19 tenapanor arm) had one AE that was drug related. Most commonly reported AEs were abdominal pain, discomfort, and abnormal GI sounds. Two volunteers discontinued study due to abdominal pain (both), nausea (one) and proctalgia (one).
Tenapanor was noted to cause decrease in sodium and phosphate absorption from the GI tract with increases in stool sodium and phosphate excretion and decrease in urinary sodium excretion compared to placebo. In patients with renal impairment, tenapanor may be associated with hyperkalemia. The pharmacodynamic effects were noted to be reversible as urine sodium was the same as placebo two days after a single dose of tenapanor. Twice daily dosing was noted to have a greater effect on sodium excretion compared to daily dosing. Tenapanor also resulted in increase in stool frequency and weight compared to placebo.
Phase II Study: Drug Efficacy
In a Phase 2b, doubled-blind, placebo-controlled randomized trial, 365 patients with IBS-C (mean age: 45.7 years; 86.8% women) were randomized 1:1:1:1 into 5 mg bid, 20 mg bid, 50 mg bid or placebo bid for 12 weeks.13 The primary endpoint was defined as number of patients with increase in baseline of ≥1 complete spontaneous bowel movement (CSBM)/week for ≥6/12 treatment weeks. Secondary endpoints included ≥30% score improvement in abdominal pain from baseline for ≥6/12 weeks and composite responder rate (CSBM and abdominal pain response in same week for ≥6/12 weeks). Significantly more IBS-C subjects receiving 50 mg bid tenapanor met the primary endpoint (60.7% vs. 33.7% P < 0.001), abdominal symptom endpoint (65.5% vs. 48.3% P < 0.026), and the composite endpoint (50% vs. 23.6% P < 0.001) than subjects in the placebo group. Improvements in other abdominal symptoms such as pain, bloating, cramping, fullness, and discomfort were also significantly higher in tenapanor 50 mg bid group. Diarrhea was the most frequently reported AE in both tenapanor 20 mg bid (12.4%) and tenapanor 50 mg bid (11.2%) arms.
Phase III Studies: Long-Term Efficacy and Safety
Two randomized, multicenter, double-blind, phase III trials were conducted to assess the safety and efficacy of tenapanor 50 mg bid compared to placebo in subjects (18–75y) meeting Rome III criteria of IBS-C. In T3MPO-1 trial, 629 (84.7% completed) IBS-C subjects were randomized to tenapanor or placebo for 12 weeks followed by 4-week randomized withdrawal period during which the groups were crossed over.14 In second phase T3MPO-2 trial, 620 IBS-C subjects (481 completed) were randomized to tenapanor 50 mg bid or placebo for 26 weeks to assess the long-term efficacy and safety.15 Both trials had the FDA primary responder endpoint, a reduction in average weekly worst abdominal pain of ≥30% and an increase of ≥ 1 CSBM from baseline in the same week for ≥6 out of 12-week treatment period in T3MPO-1 and ≥13 out of 26-week in T3MPO-2. Both trials had comparable mean age (T3MPO-1: 45 years T3MPO-2: 45.4 years) and proportion of women (T3MPO-1: 81.4% T3MPO-2: 82.1%). They demonstrated early onset of action by significantly improving symptoms and average weekly spontaneous bowel movements at week one compared to placebo.16 In a post hoc analysis of T3MPO-2, the average weekly symptoms of abdominal pain, discomfort, bloating, cramping and fullness decreased significantly from baseline in patients with IBS-C.17 Patients receiving tenapanor were significantly more satisfied with treatment and had greater mean change in their overall IBS-QoL score in both T3MPO-1 (16.9 vs. 13.2, p = 0.089) and T3MPO-2 trials (21.0 vs. 17.1, p = 0.011) compared to placebo.18 A significantly greater proportion of subjects in the tenapanor arm met the primary endpoint both in T3MPO-1 (27% vs. 18.7%, P = 0.020) and T3MPO-2 (36.5% vs. 23.7%; P < 0.001) compared to placebo (Figure 2). Diarrhea was reported as the most common AE in both trials resulting in study discontinuation for 19 patients receiving tenapanor and 2 patients receiving placebo.
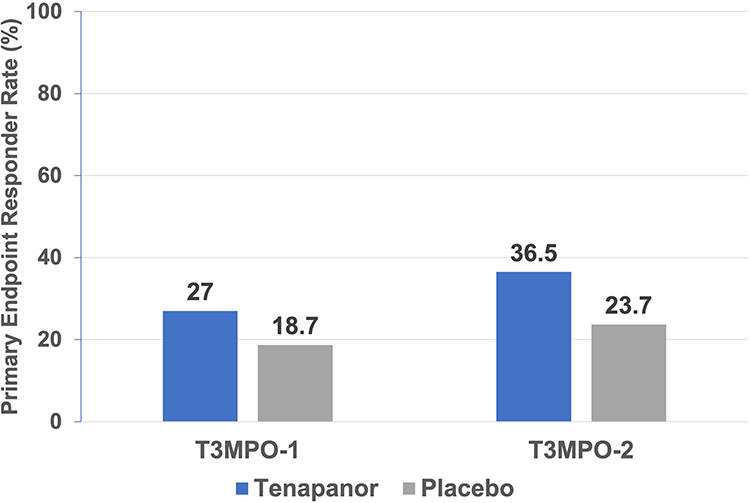 |
Figure 2 Proportions of patients with combined response for ≥6 of the 12 treatment weeks (primary efficacy variable) in T3MPO-1 and T3MPO-2 phase III trials. |
Role of Tenapanor in the Treatment of IBS-C
In clinical practice, IBS-C is diagnosed on the positive identification of symptoms in the absence of concerning alarm symptoms with minimal to no further testing. Unwarranted or repeated diagnostic testing often lead to excessive healthcare resource utilization.19 Anorectal physiology testing is recommended when patients have symptoms suggestive of pelvic floor disorders and/or are refractory to standard medical therapy.6,20,21 First-line therapy for IBS-C is soluble, viscous, poorly fermentable fiber, such as psyllium, oat bran, barley, and beans to improve stool viscosity and frequency.6 PEG is a widely available, over-the-counter, osmotic laxative extensively used in clinical practice for IBS-C. Although PEG improves stool frequency and consistency, it has not shown improvement in abdominal pain, leading to recommendation against its use to relieve global symptoms in IBS-C.6 In the last two decades, secretagogues, such as lubiprostone, linaclotide, and plecanatide, have provided effective pharmacological treatment options for IBS-C patients (Table 1).
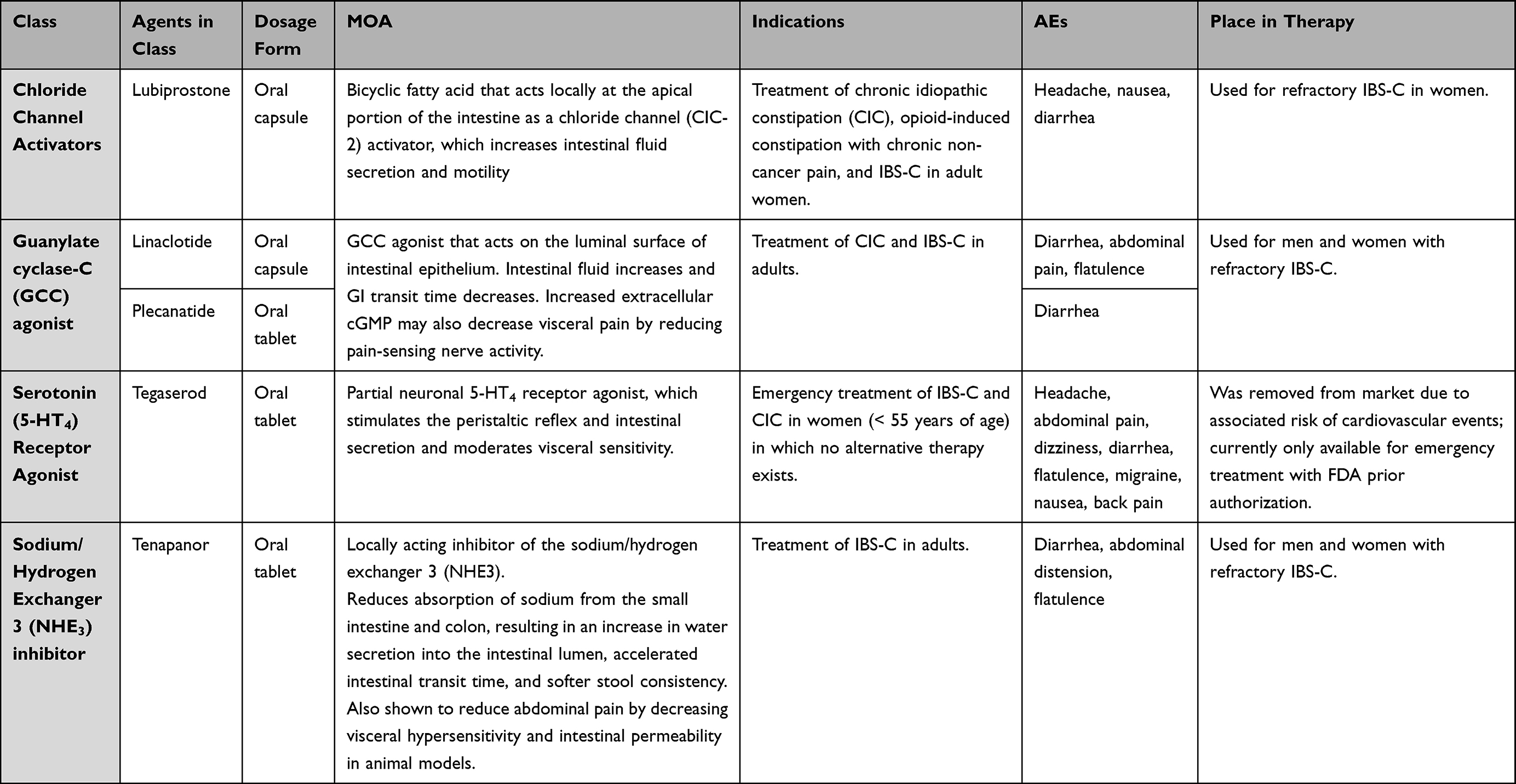 |
Table 1 Treatment Options Available for IBS-C and Their Mechanism of Action, Indications, and Adverse Effects |
In September 2019, the FDA approved tenapanor for the treatment of patients with IBS-C based on its excellent safety profile and compelling evidence of its efficacy from large-scale, Phase III, randomized, placebo-controlled trials (T3MPO1 and T3MPO2). Tenapanor can be used safely in patients with IBS-C unresponsive to soluble fiber as a first-line therapy. It has also been recommended as an efficacious second line drug for IBS-C by British Society of Gastroenterology.22 Due to its effect on colonic hypersensitivity, it can reduce abdominal bloating, second most bothersome symptom reported by patients, however, it was ranked last compared to linaclotide, lubiprostone and tegaserod in an indirect comparison.23,24 Tenapanor has minimal systemic availability, however, it is a minor substrate of CYP3A4 and therefore may decrease serum concentrations of enalapril and its active metabolites. Its use is contraindicated in children less than 6 years old and patients with mechanical bowel obstruction. Tenapanor may result in hyperkalemia in patients with renal impairment. Administration of tenapanor 5–10 minutes prior to a meal may increase stool sodium excretion and efficacy. In a pooled study including 21 trials comparing licensed drugs for IBS-C, tenapanor has the highest number of AEs resulting in withdrawal.25 Even though, Linaclotide is the only secretagogue that has been approved by European Medicines Agency, tenapanor meets a rigorous global symptoms endpoint with relief from both bowel and abdominal symptoms in IBS-C patients.26 Tenapanor provides a different mechanism of action from secretagogues for constipation and does not need to be restricted due to cardiovascular concerns as in the case of serotoninergic agents. Further studies comparing rates of AEs, especially diarrhea, and efficacy in IBS-C subjects between pharmacologic treatments are warranted. Cost dynamics of these IBS-C medications will continue to be the most important driving factor in the treatment of patients in clinical practice.
Conclusion
Tenapanor is a small molecule inhibitor of the sodium/hydrogen exchanger isoform 3 (NHE3) that inhibits the absorption of sodium and phosphate in the gastrointestinal tract, resulting in fluid retention and softer stool. Tenapanor is a proven, safe, and efficacious treatment option for IBS-C subjects. It provides global IBS symptom relief with both an increase in complete spontaneous bowel movements and improved abdominal pain. Tenapanor has minimum systemic availability and minimal adverse effects. After three double-blind, placebo-controlled RCTs, tenapanor 50 mg twice daily was approved by FDA for the treatment of patients with IBS-C and has been included as a recommendation in recent guideline.27 This dosage has shown a significantly greater reduction in abdominal pain and increase of ≥ 1 CSBM from baseline compared to placebo.Direct costs to the patient of IBS-C medications will continue to be a driving factor in clinical practice. From the provider standpoint, it is welcome to see additional treatment options become available for refractory IBS-C patients.
Disclosure
AS served on the advisory board for Phathom Pharmaceuticals, Takeda Pharmaceuticals, Salix Pharmaceuticals, and Ironwood Pharmaceuticals. He has received research funding from Vibrant Ltd, Parkinson’s Foundation, and NIDDK. The authors report no other conflicts of interest in this work.
References
1. Drossman DA, Hasler WL. Rome IV-functional GI disorders: disorders of gut-brain interaction. Gastroenterology. 2016;150(6):1257–1261. doi:10.1053/j.gastro.2016.03.035
2. Sperber AD, Bangdiwala SI, Drossman DA, et al. Worldwide prevalence and burden of functional gastrointestinal disorders, results of Rome Foundation Global Study. Gastroenterology. 2021;160(1):99–114. doi:10.1053/j.gastro.2020.04.014
3. Frändemark Å, Törnblom H, Jakobsson S, Simrén M. Work productivity and activity impairment in irritable bowel syndrome (IBS): a multifaceted problem. Am J Gastroenterol. 2018;113(10):1540–1549. doi:10.1038/s41395-018-0262-x
4. Nellesen D, Yee K, Chawla A, Lewis BE, Carson RT. A systematic review of the economic and humanistic burden of illness in irritable bowel syndrome and chronic constipation. J Manag Care Pharm. 2013;19(9):755–764. doi:10.18553/jmcp.2013.19.9.755
5. Palsson OS, Whitehead W, Tornblom H, et al. Prevalence of Rome IV functional bowel disorders among adults in the United States, Canada and United Kingdom. Gastroenterology. 2020;158(5):1262–1273. doi:10.1053/j.gastro.2019.12.021
6. Lacy BE, Pimentel M, Brenner DM, et al. ACG clinical guideline: management of irritable bowel syndrome. Am J Gastroenterol. 2021;116(1):17–44. doi:10.14309/ajg.0000000000001036
7. Spencer AG, Labonte ED, Rosenbaum DP. Intestinal inhibition of the Na+/H+ exchanger 3 prevents cardiorenal damage in rats and inhibits Na+ uptake in humans. Sci Transl Med. 2014;6(227):227ra36. doi:10.1126/scitranslmed.3007790
8. Block GA, Rosenbaum DP, Korner P, Yan A, Chertow GM. Gastrointestinal tolerability of tenapanor to treat hyperphosphatemia in patients on hemodialysis. J Am Soc Nephrol. 2017;28:373.
9. Johansson S, Rosenbaum DP, Knutsson M, Leonsson-Zachrisson M. A phase 1 study of the safety, tolerability, pharmacodynamics, and pharmacokinetics of tenapanor in healthy Japanese volunteers. Clin Exp Nephrol. 2017;21(3):407–416. doi:10.1007/s10157-016-1302-8
10. Li Q, King A, Liu L, Zhu Y, Caldwell J, Pasricha PJ. Tenapanor reduces IBS pain through inhibition of TRPV1-dependent neuronal hyperexcitability in vivo. Off J Am Coll Gastroenterol. 2017;112:S255. doi:10.14309/00000434-201710001-00484
11. Wang J, Larauche M, Siegel M, et al. Tenapanor attenuates increased macromolecule permeability in human colon monolayer cultures induced by inflammatory cytokines and human fecal supernatants. Gastroenterology. 2018;154(Suppl 1):S326. doi:10.1016/S0016-5085(18)31424-0
12. Rosenbaum DP, Yan A, Jacobs JW. Pharmacodynamics, safety, and tolerability of the NHE3 inhibitor tenapanor: two trials in healthy volunteers. Clin Drug Investig. 2018;38:341–351. doi:10.1007/s40261-017-0614-0
13. Chey WD, Lembo AJ, Rosenbaum DP. Tenapanor treatment of patients with constipation-predominant irritable bowel syndrome: a phase 2, randomized, placebo-controlled efficacy and safety trial. Am J Gastroenterol. 2017;112(5):763. doi:10.1038/ajg.2017.41
14. Chey WD, Lembo AJ, Rosenbaum DP. Efficacy of tenapanor in treating patients with irritable bowel syndrome with constipation: a 12-week, placebo-controlled phase 3 trial (T3MPO-1). Am J Gastroenterol. 2020;115(2):281–293. doi:10.14309/ajg.0000000000000516
15. Chey WD, Lembo AJ, Yang Y, Rosenbaum DP. Efficacy of tenapanor in treating patients with irritable bowel syndrome with constipation: a 26-week, placebo-controlled phase 3 trial (T3MPO-2). AmJGastroenterol. 2021;116(6):1294–1303.
16. Fogel RP, Edelstein S, Yang Y, Rosenbaum DP. Tu1375: tenapanor has early onset of action in treating symptoms of irritable bowel syndrome with constipation (IBS-C) (T3MPO-1 AND T3MPO-2 TRIALS). Gastroenterology. 2022;162(7):S–940. doi:10.1016/S0016-5085(22)62229-7
17. Lembo A, Edelstein S, Yang Y, Rosenbaum DP. Mo1396: long term treatment with Tenapanor improves abdominal pain and other abdominal symptoms associated with IBS-C. Gastroenterology. 2022;162(7):S–757. doi:10.1016/S0016-5085(22)61788-8
18. Chey WD, Edelstein S, Yang Y, Rosenbaum DP. Mo1394: effect of Tenapanor on treatment satisfaction, degrees of relief, and quality of life for patients with irritable bowel syndrome with constipation (IBS C). Gastroenterology. 2022;162(7):S–756. doi:10.1016/S0016-5085(22)61786-4
19. Ladabaum U, Boyd E, Zhao WK, et al. Diagnosis, comorbidities, and management of irritable bowel syndrome in patients in a large health maintenance organization. Clin Gastroenterol Hepatol. 2012;10(1):37–45. doi:10.1016/j.cgh.2011.08.015
20. Sharma A, Rao SS, Kearns K, Orleck KD, Waldman SA. Diagnosis, management and patient perspectives of the spectrum of constipation disorders. Aliment Pharmacol Ther. 2001;53(12):1250–1267. doi:10.1111/apt.16369
21. Sharma A, Herekar A, Yan Y, Karunaratne T, Rao SS. Dyssynergic defecation and other evacuation disorders. Gastroenterol Clin. 2022;51(1):55–69. doi:10.1016/j.gtc.2021.10.004
22. Vasant DH, Paine PA, Black CJ, et al. British Society of Gastroenterology guidelines on the management of irritable bowel syndrome. Gut. 2021;70(7):1214–1240. doi:10.1136/gutjnl-2021-324598
23. Ringel Y, Williams RE, Kalilani L, Cook SF. Prevalence, characteristics, and impact of bloating symptoms in patients with irritable bowel syndrome. Clin Gastroenterol hepatol. 2009;7(1):68–72. doi:10.1016/j.cgh.2008.07.008
24. Nelson AD, Black CJ, Houghton LA, Lugo‐Fagundo NS, Lacy BE, Ford AC. Systematic review and network meta‐analysis: efficacy of licensed drugs for abdominal bloating in irritable bowel syndrome with constipation. Aliment Pharmacol Ther. 2021;54(2):98–108. doi:10.1111/apt.16437
25. Barberio B, Savarino EV, Black CJ, Ford AC. Adverse events in trials of licensed drugs for irritable bowel syndrome with constipation or diarrhea: systematic review and meta‐analysis. Neurogastroenterol Motil. 2022;34(6):e14279. doi:10.1111/nmo.14279
26. Barbara G, Cremon C, Bellini M, et al. Italian guidelines for the management of irritable bowel syndrome: joint consensus from the Italian societies of: gastroenterology and endoscopy (SIGE), neurogastroenterology and motility (SINGEM), Hospital Gastroenterologists and Endoscopists (AIGO), Digestive Endoscopy (SIED), general medicine (simg), gastroenterology, hepatology and pediatric nutrition (SIGENP) and Pediatrics (SIP). Dig Liver Dis. 2023;55(2):187–207. doi:10.1016/j.dld.2022.11.015
27. Chang L, Sultan S, Lembo A, Verne GN, Smalley W, Heidelbaugh JJ. AGAclinical practice guideline on the pharmacological management of irritable bowel syndrome with constipation. Gastroenterology. 2022;163(1):118–136. doi:10.1053/j.gastro.2022.04.016
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.