Back to Journals » International Medical Case Reports Journal » Volume 19
Temporary Rhythm Control with Flecainide in Atrial Fibrillation-Related Conversion Pauses Prior to Catheter Ablation: A Case of Successful Pharmacological Bridging
Authors Skakun O ![]() , Varunkiv O, Symchych A
, Varunkiv O, Symchych A ![]() , Symchych K
, Symchych K ![]() , Vandzhura I, Vandzhura Y, Denina R
, Vandzhura I, Vandzhura Y, Denina R ![]() , Zvonar P, Rudnyk V
, Zvonar P, Rudnyk V ![]()
Received 23 February 2026
Accepted for publication 1 July 2026
Published 9 July 2026 Volume 2026:19 604692
DOI https://doi.org/10.2147/IMCRJ.S604692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Thomas E Hutson
Video abstract of “Rhythm Control with Flecainide in Conversion Pauses” [604692].
Views: 7
Oleksii Skakun,1 Oleksandr Varunkiv,2 Anton Symchych,3 Khrystyna Symchych,4 Ihor Vandzhura,5 Yaroslava Vandzhura,5 Roksolana Denina,5 Pavlo Zvonar,5 Viktoriia Rudnyk4
1Cardiological Department, St. Luke’s Clinic, Ivano-Frankivsk, Ukraine; 2Department of Phthisiology and Pulmonology with the Course of Occupational Diseases, Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine; 3Department of General and Vascular Surgery, Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine; 4Department of Therapy, Family, and Emergency Medicine of Postgraduate Education, Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine; 5Department of Internal Medicine No. 2 and Nursing, Ivano-Frankivsk National Medical University, Ivano-Frankivsk, Ukraine
Correspondence: Oleksii Skakun, Cardiological Department, St. Luke’s Clinic, Sofron Mydryi, 26 street, Ivano-Frankivsk, Ivano-Frankivsk Region, Ukraine, Tel +380502293269, Email [email protected]
Abstract: The management of paroxysmal atrial fibrillation with conversion pauses remains challenging, with catheter ablation and permanent pacemaker implantation representing the main therapeutic strategies. Catheter ablation may eliminate atrial fibrillation paroxysms and prevent conversion pauses, whereas pacemaker implantation combined with antiarrhythmic therapy for rhythm control is another accepted option. We report a case of successful management of paroxysmal atrial fibrillation with conversion pauses using antiarrhythmic agents for rhythm control prior to catheter ablation. A 61-year-old woman had episodes of palpitations, dizziness, and presyncope. Ambulatory 12-lead 24-hour ECG monitoring showed 51 episodes of atrial fibrillation and atrial flutter with conversion pauses after each of them; the longest pause was 7460 ms. Atrial fibrillation lasted for 46.9% of the total monitoring time. When ambulatory 24-hour monitoring was performed, the patient was highly symptomatic (complaints of palpitations and fear of death were predominant, but dizziness episodes were also noted). Catheter ablation was unavailable in the short-term period and permanent pacemaker implantation was not accepted by the patient. Thus, flecainide at a dose of 100 mg BID under close supervision for rhythm control was administered. Also, anticoagulation with edoxaban was provided. The patient remained asymptomatic until ablation was performed. Pulmonary vein isolation with pulsed field ablation and cavotricuspid isthmus ablation was performed 10 days after ambulatory ECG monitoring. There were no paroxysms of atrial fibrillation after ablation. Antiarrhythmic agents in patients with conversion pauses may worsen sinus node function but may also eliminate atrial fibrillation paroxysms preventing conversion pauses. Thus, catheter ablation may be an option for a patient presenting with atrial fibrillation and conversion pauses to avoid unnecessary permanent pacemaker implantation. Short-term pharmacological bridging with flecainide under close supervision may be used in patients with atrial fibrillation and conversion pauses without other signs of sinus node dysfunction, providing effective rhythm control.
Keywords: antiarrhythmic agents, ambulatory ECG monitoring, symptomatic pauses, post-atrial fibrillation pauses, pulsed field ablation
Introduction
Conversion pauses are transient pauses occurring after termination of atrial fibrillation or atrial flutter due to delayed recovery of sinus node automaticity. Prolonged sinus pauses after paroxysms of atrial fibrillation may result from depression of sinus node function1 and are considered to be a distinct type of sinus node dysfunction.2 When the sinus node is suppressed by the overdrive effect of an atrial fibrillation episode, its recovery after abrupt termination of the atrial fibrillation episode may be delayed, and the timing of sinus rate normalization cannot be reliably predicted.3 Conversion pauses may lead to dizziness and syncope.4 Conversion pauses are often the only manifestation of sinus node dysfunction and may occur in the absence of classic forms of sinus node dysfunction, such as sinus arrest, sinus exit block, sinus bradycardia, or chronotropic incompetence.
Although pharmacological cardioversion is not recommended in patients with sinus node dysfunction unless risks of bradycardia have been carefully considered,5 there are no clear recommendations regarding antiarrhythmic agents for maintenance of sinus rhythm for patients with paroxysmal atrial fibrillation with conversion pauses. Use of antiarrhythmic agents in patients with atrial fibrillation and conversion pauses may, on the one hand, prevent atrial fibrillation paroxysms and thereby completely eliminate conversion pauses, while, on the other hand, suppress sinus node function and prolong the pauses. However, no studies have evaluated the use of antiarrhythmic agents in patients with paroxysmal atrial fibrillation and conversion pauses. Catheter ablation may be used in selected patients with symptoms due to prolonged pauses upon atrial fibrillation termination to avoid unnecessary pacemaker implantation.5
Additionally, atrial fibrillation poses a certain risk of stroke and proper anticoagulation is required.5
Case Report
A 61-year-old woman visited a cardiologist for episodes of palpitations, dizziness, and presyncope. Symptoms occurred every second to third day. Atrial fibrillation was diagnosed 7 months ago. The patient also had hypertension and hypercholesterolemia. The patient received propafenone 150 mg BID, edoxaban 30 mg OD, moxonidine 0.3 mg OD, rosuvastatin 20 mg, valsartan 80 mg OD, and metoprolol 12.5 mg OD. Resting ECG showed normal sinus rhythm. Ambulatory 24-hour ECG monitoring was performed. There were 51 episodes of atrial fibrillation with conversion pauses after each of them. There were episodes of transformation from atrial fibrillation to atrial flutter. The longest RR interval was 7460 ms (Figure 1). Significant sinus bradycardia and frequent single and coupled premature atrial complexes appeared for a short period after sinus rhythm restoration (Figure 2A). Some pauses were terminated by junctional escape beats (Figure 2B). Also, there were episodes of micro-atrial fibrillation (Figure 2C). Atrial fibrillation lasted for 46.9% of the total monitoring time. Additionally, there were 426 premature atrial complexes, 28 atrial couplets, and 7 episodes of supraventricular tachycardia (presumed focal atrial tachycardia) lasting from 4 to 7 complexes. When ambulatory 24-hour ECG monitoring was performed, the patient was highly symptomatic (complaints of palpitations and fear of death were predominant, but dizziness during atrial fibrillation episodes was also noted). Echocardiography revealed normal values (including a left atrial volume of 36 mL and a left atrial volume index of 18.9 mL/m2). Considering the clinical condition, especially the fact that all pauses were associated with atrial fibrillation, the absence of the possibility of performing ablation in the short term, and the fact that ambulatory ECG monitoring was performed while the patient was taking a beta-blocker, it was decided to cancel metoprolol and moxonidine. Also, the patient was switched from propafenone to flecainide at a dose of 100 mg BID. Considering normal GFR (86 mL/min/1.73m2), the dose of edoxaban was increased to 60 mg. All other drugs remained unchanged. The ECG was normal on the second day after initiation of flecainide therapy. There were no symptoms until ablation was performed. Pulmonary vein isolation with pulsed field ablation and ablation of the cavotricuspid isthmus was performed 10 days after ambulatory ECG monitoring. Flecainide at a dose of 100 mg BID and edoxaban 60 mg OD were continued; rosuvastatin and valsartan were also continued.
 |
Figure 1 Termination of atrial flutter with a conversion pause lasting 7460 ms, followed by sinus bradycardia with single and coupled premature atrial complexes. Abbreviations: AF, QRS complexes during atrial flutter; J, junctional escape complex; L, QRS complexes followed by an RR interval > 2000 ms; N, normal QRS complexes; S, supraventricular complexes. |
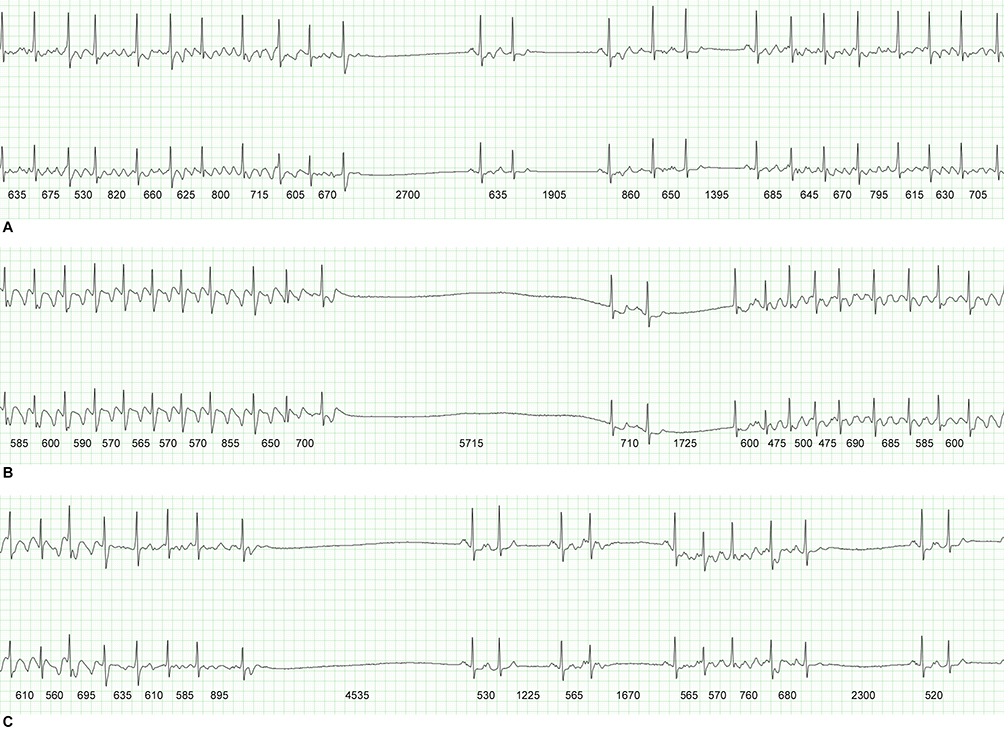 |
Figure 2 Conversion pauses: atrial fibrillation paroxysm termination with a conversion pause lasting 2700 ms followed by sinus rhythm with single and coupled premature atrial complexes with subsequent initiation of a new atrial fibrillation episode (A); atrial flutter episode termination with a conversion pause lasting 5715 ms followed by junctional escape complexes and a single premature atrial contraction with subsequent initiation of a new atrial flutter episode (B); atrial flutter with transformation to atrial fibrillation followed by a conversion pause lasting 4535 ms with subsequent sinus rhythm with single premature atrial complexes and one episode of “micro-atrial fibrillation” lasting 4 complexes (C). |
One month after ablation, 24-hour ambulatory ECG monitoring was repeated. There were 5 episodes of sinus exit block (Figure 3) with the longest RR interval of 1990 ms and 2 premature atrial contractions. The patient remained asymptomatic. The dose of flecainide was reduced to 50 mg BID, and 24-hour ambulatory ECG monitoring was repeated. There were 19 premature atrial contractions and 30 premature ventricular contractions. The maximum RR interval was 1355 ms. There were no signs of sinus node dysfunction. Flecainide was continued at a dose of 50 mg BID for up to 3 months after ablation. Edoxaban, rosuvastatin, and valsartan were continued as well. The patient remained asymptomatic.
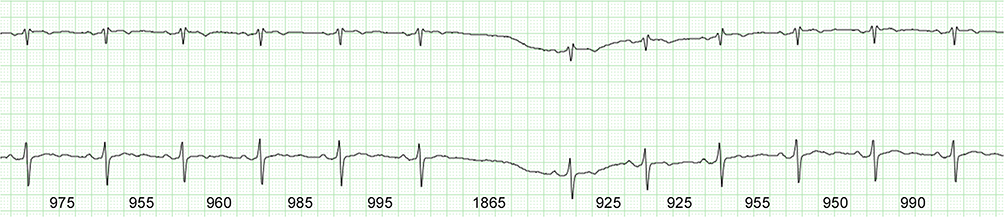 |
Figure 3 Sinus exit block. |
Discussion
Despite the fact that the patient had symptomatic pauses, permanent pacemaker was not implanted. The strategy of rhythm control with catheter ablation was prioritized for the patient. According to the 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy, ablation for atrial fibrillation should be considered as a strategy to avoid pacemaker implantation in patients with symptomatic pauses after atrial fibrillation conversion.2 If catheter ablation had not been performed, permanent pacing would be indicated for this patient. Meta-analysis performed by Su L. et al (2024) showed that ablation for atrial fibrillation can effectively reduce the risk of all-cause mortality, thromboembolism, stroke, heart failure, progression to persistent atrial fibrillation, and the need for permanent pacemaker implantation in patients with tachycardia–bradycardia syndrome.6 However, long pause on termination of atrial fibrillation predicts the need for permanent pacemaker implantation.7 Chen Y.W. et al (2014) showed that in patients with prolonged symptomatic sinus pauses on atrial fibrillation termination, atrial fibrillation ablation appears to be superior to a strategy of pacing plus antiarrhythmic drugs and pacemaker implantation can be avoided after a successful ablation in the 95.3% of patients.8
Reduced need for long-term use of antiarrhythmic agents is another benefit of catheter ablation.6 Moreover, there is evidence that the sinus node function after ablation for atrial fibrillation improves, suggesting reverse remodeling of the sinus node.1 Atrial fibrillation ablation may result in significant increase in minimum heart rate and the disappearance of pauses >2.0 seconds.9 Restoration of the sinus rhythm, whether by ablation or cardioversion, in patients with persistent atrial fibrillation leads to increase in atrial effective refractory period, improvement of sinus node function, and increase in atria conduction velocity.10
Catheter ablation was unavailable immediately after the diagnosis of conversion pauses were made in the reported patient. It was an option in 1–2 weeks. However, the patient was highly symptomatic. Therefore, prevention of atrial fibrillation episodes and conversion pauses with antiarrhythmic agents was chosen. There is limited evidence for administration of antiarrhythmic agents in patients with concomitant sinus node dysfunction. This is explained by the fact that all antiarrhythmic agents may worsen sinus node function.11 However, there is a potential beneficial effect of antiarrhythmic agents when pauses or bradycardia episodes are related to atrial fibrillation. There is evidence that dronedarone at a dose of 400 mg BID was administered to patient with sinus bradycardia and concomitant atrial fibrillation.12 There is evidence that flecainide increases the corrected sinus node recovery time and the sinoatrial conduction time.13 However, we successfully used flecainide under meticulous supervision as pharmacological bridging, and there were no side effects. Moreover, the patient was completely asymptomatic for 10 days.
Flecainide was preferred in this case as it has no beta-blocking effect compared to other antiarrhythmic agents such as propafenone,14 amiodarone,15 dronedarone,16 and sotalol.17 Such pharmacological bridging may be important for maintaining rhythm control during the days or weeks before ablation when the procedure is temporarily unavailable. Careful monitoring for side effects of flecainide should be maintained. Widening of the QRS complex by >25% from the baseline value or appearance of a bundle branch block is contraindication for flecainide continuation.5 As flecainide without a concomitant beta-blocker may lead to transformation from atrial fibrillation to atrial flutter with a high ventricular rate,5 careful bedside ECG monitoring for the first few days after flecainide initiation is required. Also, monitoring of other signs of sinus node dysfunction such as sinus arrest and sinus exit block should be provided. In this case, flecainide was prescribed based on the principle: “No atrial fibrillation – no conversion pauses”.
The antiarrhythmic agent was prescribed for 3 months after ablation according to 2023 ACC/AHA/ACCP/HRS Guideline for the Diagnosis and Management of Atrial Fibrillation.18 There is evidence that in patients free of atrial fibrillation at the end of 3 months of post-ablation blanking period, continued use of antiarrhythmic agents significantly reduces the recurrence of atrial tachyarrhythmia in the first year after pulmonary vein isolation.19
Such a strategy cannot be applied to patients with conversion pauses and episodes of sinus arrest, symptomatic sinus bradycardia, atrial fibrillation refractory to antiarrhythmic agents, or contraindications to antiarrhythmic agents.
Conclusion
Catheter ablation for atrial fibrillation may be an option for patients presenting with atrial fibrillation and conversion pauses to avoid unnecessary permanent pacemaker implantation. Pharmacological bridging with flecainide may be used in patients with atrial fibrillation and conversion pauses without other signs of sinus node dysfunction for a short period, providing effective rhythm control under close supervision.
Abbreviations
ACC, American College of Cardiology; ACCP, American College of Clinical Pharmacy; AHA, American Heart Association; BID, bis in die (twice a day); ECG, electrocardiogram; ESC, European Society of Cardiology; HRS, Heart Rhythm Society; OD, omni die (once a day).
Patient Consent and Institution Approval
The written consent for this case publication preserving the patient’s anonymity was obtained from the patient. The institutional approval for the case report is not required according to local guidelines.
Funding
The authors declare that this study has not received any funding sources.
Disclosure
There is no conflicts of interest to declare.
References
1. Hocini M, Sanders P, Deisenhofer I, et al. Reverse remodeling of sinus node function after catheter ablation of atrial fibrillation in patients with prolonged sinus pauses. Circulation. 2003;108(10):1172–6. doi:10.1161/01.CIR.0000090685.13169.07
2. Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021;42(35):3427–3520. doi:10.1093/eurheartj/ehab364
3. Poçi D, Abrahamsson BM, Edvardsson N, Bergfeldt L. Sinus bradycardia and sinus pauses immediately after electrical cardioversion of persistent atrial fibrillation--what do they mean? Ann Noninvasive Electrocardiol. 2013;18(3):281–287. doi:10.1111/anec.12033
4. Tsiachris D, Stabola S, Kordalis A, Stefanadis C. Interrupting the natural history of atrial fibrillation. Image from the future. J Atr Fibrillation. 2018;10(5):1793. doi:10.4022/jafib.1793
5. Van Gelder IC, Rienstra M, Bunting KV, et al. 2024 ESC guidelines for the management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2024;45(36):3314–3414. doi:10.1093/eurheartj/ehae176
6. Su L, Wang X, Kang F, Gong C, Chen D. Atrial fibrillation ablation compared to pacemaker therapy in patients with tachycardia-bradycardia syndrome: a systematic review and updated meta-analysis. Medicine. 2024;103(16):e37543. doi:10.1097/MD.0000000000037543
7. Kim DH, Choi JI, Lee KN, et al. Long-term clinical outcomes of catheter ablation in patients with atrial fibrillation predisposing to tachycardia-bradycardia syndrome: a long pause predicts implantation of a permanent pacemaker. BMC Cardiovasc Disord. 2018;18(1):106. doi:10.1186/s12872-018-0834-0
8. Chen YW, Bai R, Lin T, et al. Pacing or ablation: which is better for paroxysmal atrial fibrillation-related tachycardia-bradycardia syndrome? Pacing Clin Electrophysiol. 2014;37(4):403–411. doi:10.1111/pace.12340
9. Ohkubo K, Watanabe I, Okumura Y, et al. Pulmonary vein isolation for atrial fibrillation in patients with paroxysmal atrial fibrillation and prolonged sinus pause. Int Heart J. 2007;48(2):247–252. doi:10.1536/ihj.48.247
10. Raitt MH, Kusumoto W, Giraud G, McAnulty JH. Reversal of electrical remodeling after cardioversion of persistent atrial fibrillation. J Cardiovasc Electrophysiol. 2004;15(5):507–512. doi:10.1046/j.1540-8167.2004.03217.x
11. Bai J, Lu Y, Zhang H. In silico study of the effects of anti-arrhythmic drug treatment on sinoatrial node function for patients with atrial fibrillation. Sci Rep. 2020;10(1):305. doi:10.1038/s41598-019-57246-5
12. Zhang Q, Shi F, Song B, Bao Y, Cao Y. Safety observation of antiarrhythmic drug use in a patient with sinus bradycardia following atrial fibrillation radiofrequency ablation combined with cardiac neural ablation: a case report. Pan Afr Med J. 2024;48:63. doi:10.11604/pamj.2024.48.63.43881
13. Andrikopoulos GK, Pastromas S, Tzeis S. Flecainide: current status and perspectives in arrhythmia management. World J Cardiol. 2015;7(2):76–85. doi:10.4330/wjc.v7.i2.76
14. Lombardi F, Torzillo D, Sandrone G, et al. Beta-blocking effect of propafenone based on spectral analysis of heart rate variability. Am J Cardiol. 1992;70(11):1028–1034. doi:10.1016/0002-9149(92)90355-3
15. Heijman J, Dobrev D. Pleiotropic actions of amiodarone: still puzzling after half a century. Naunyn-Schmiedeberg’s Arch Pharmacol. 2013;386:571–574. doi:10.1007/s00210-013-0865-0
16. Cha JJ. Pleiotropic effect of dronedarone beyond antiarrhythmic agent: reduction of hypertrophy. Korean Circ J. 2024;54(4):187–188. doi:10.4070/kcj.2024.0067
17. Antonaccio MJ, Gomoll A. Pharmacologic basis of the antiarrhythmic and hemodynamic effects of sotalol. Am J Cardiol. 1993;72(4):27A–37A. doi:10.1016/0002-9149(93)90022-5
18. Joglar JA, Chung MK, Armbruster AL, et al. 2023 ACC/AHA/ACCP/HRS guideline for the diagnosis and management of atrial fibrillation. J Am Coll Cardiol. 2023;83(1):109–279. doi:10.1016/j.jacc.2023.08.017
19. Duytschaever M, Demolder A, Phlips T, et al. PulmOnary vein isolation with vs. without continued antiarrhythmic Drug trEatment in subjects with Recurrent Atrial Fibrillation (POWDER AF): results from a multicentre randomized trial. Eur Heart J. 2018;39(16):1429–1437. doi:10.1093/eurheartj/ehx666
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.